Education & knowledge through people & facts - Cancerworld
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

cw6_copertina3 22-04-2005 14:14 Pagina 1
CancerWorld 6
Education & knowledge through people & facts
MAY-JUNE 2005
Number 6, May-June 2005
José Baselga
➜ José Baselga: playing to Europe’s strengths ➜ Why patients are still dying
needlessly ➜ US War on Cancer: DeVita says “I got it right" ➜ Neoadjuvant
treatment gets a mixed report ➜ Rising to the challenge in developing countries
Contents
3 Editorial
Balancing safety against need
Editor
4 Cover Story
Kathy Redmond José Baselga: playing to Europe’s strengths
Assistant Editor
Anna Wagstaff
14 Grand Round
Editorial Assistant
Mariarita Cassese They could be alive today
Editorial Board
Mariano Barbacid, Franco Cavalli
Alberto Costa (chair)
24 Drug Watch
Lev Demidov, Mario Dicato
Gordon McVie, Nicolas Pavlidis
What do animal experiments really tell us?
Hans-Jörg Senn, Antonella Surbone
Board of Advisors 30 Regulatory Digest
Jan Betka, Jacques Bernier
Vincent T. DeVita, Lex Eggermont EPO rules on contested gene patent
Jan Foubert, Lynn Faulds Wood
Neel Mittra, Santiago Pavlovsky
Bob Pinedo, Mike Richards 32 Inside Track
Maurice Schneider, Tom Voûte
Umberto Veronesi (chair) Tackling cancer: the view from Brussels
Contributing Writers
Marc Beishon, Raphaël Brenner,
Raphael Catane, Nathan Cherny, 38 Masterpiece
Christine Haran, Peter McIntyre,
Emma Mason, Alex Mathieson, Vince DeVita: the view from the top
Robert Matthews, Anna Wagstaff
Publishing Advisors
Gillian Griffith, Fedele Gubitosi 44 Spotlight on...
Website Liaison
Rising to the challenge in the developing world
Chatrina Melcher Does your hospital pass the palliative care test?
Project Designer
Andrea Mattone
54 Impact Factor
Graphic and Layout Designers
Pier Paolo Puxeddu+Francesca Vitale Neoadjuvant studies offer mixed messages
Production Manager Cancer vaccine for CML shows promise
Gianfranco Bangone
Published by
Editoriale Darwin srl
62 e-World
Piazza Antonio Mancini, 4 - 00196 Rome Symptom management at the touch of a button
Printed by
IGER Istituto Grafico
Editoriale Romano s.r.l. 66 Bookcase
Viale C.T. Odescalchi, 67 - 00147 Rome
Cover photograph
Eligio Paoni / Contrasto 70 Focus
Registrazione Tribunale di Roma
Who pays the piper...
Decreto n. 436 del 8.11.2004
Direttore responsabile
Emanuele Bevilacqua
All enquiries about Cancer World
should be made to:
ESO Editorial Office
Viale Beatrice D’Este 37
20122 Milan, Italy
e-mail: magazine@esoncology.org
Fax: +39 02 8546 4545
Cancer World is published six times per year by the European School of Oncology
with an average print run of 10,000 copies. It is distributed at major conferences,
Copyright ©2005 European School of Oncology. mailed to subscribers and to European opinion leaders, and is available on-line at
All rights reserved www.cancerworld.org
CANCER WORLD ■ MAY-JUNE 2005 ■ 1
Editorial
Balancing safety
against need
➜ Kathy Redmond ■ EDITOR
W hen Pfizer followed
Merck & co in with-
drawing one of their
COX-2 inhibitors from the market owing to
increased risks of cardiovascular complica-
tions, it provided a timely reminder that
patients and other stakeholders is essential
in order to get the balance right. This is
because risks are experienced and inter-
preted very differently depending on the
perspective of the observer, and the way
risks are perceived can also vary signifi-
medicines are not without their risks. We cantly depending on the situation. Once a
have known about the potential harm asso- medicine reaches the market its safety
ciated with medicines for centuries. Almost should be continuously monitored and
500 years ago Paracelsus wrote: Dosis facit efforts made to ensure that it is used appro-
venenum (the dose makes the poison) – in priately in clinical practice. Additional clin-
other words, the higher the dose of any par- ical trials need to be carried out to clarify
ticular chemical, the greater its toxic effect the effect of exposure to the medicine in
on living organisms. Beneficial medicines ‘real life’ situations and to define new indi-
can turn poisonous if you take too much – cations. Better mechanisms are needed for
low-dose aspirin can reduce heart disease reporting adverse drug reactions and we
but higher doses can kill. need to raise professional and public
Ideally, we should protect patients from awareness about potential safety concerns.
harm, but in reality, when most novel med- In its recent ‘Road Map to 2010’ the
icines are approved it is impossible to know European Medicines Agency has made a
enough about their long-term effects to commitment to ensure that patients suffer-
enable us to do so. Gathering sufficient ing from life-threatening conditions will
information prior to approval could delay gain timely access to safe and effective
access to potentially useful therapies for medicines. The Agency also aims to intro-
patients with no other options – a delay duce more proactive approaches to phar-
some cancer patients cannot afford. The macovigilance across the EU. These devel-
introduction of innovative medicines opments are welcome, for it would be a
requires that regulators strike the right bal- tragedy if ill-informed risk-benefit analyses
ance between risk and benefit. With life- hindered the approval of innovative cancer
threatening diseases it is more acceptable drugs that could benefit thousands of
to take risks with safety because so much European patients, or if effective medi-
more is at stake. Communication between cines have to be withdrawn because we did
pharmaceutical companies, regulators, not get the monitoring right.
All correspondence should be sent to the Editor at editor@esoncology.org
CANCER WORLD ■ MAY-JUNE 2005 ■ 3
CoverStory
José Baselga:
playing
to Europe’s strengths
➜ Marc Beishon
It took José Baselga just a few years to build the oncology department at Barcelona’s Vall
d’Hebron hospital from a few shabby consulting rooms to a leading centre for research into
targeted therapies. Europe has the edge in this type of research because we are better at
working together, says Baselga. But we still have a lot to learn from the US.
T
he European oncology community what happens in the US but play to our
had better get its act together – or strengths, in particular our capacity for coopera-
suffer more years of fragmentation, tion and partnership. But we need to become far
underfunding and overburdensome more professional in our organisation, training
regulation. It’s a strong message and fundraising.”
delivered by the quietly spoken José Baselga, All of those factors have been promoted by
head of oncology at the Vall d’Hebron hospital in Baselga in the nine years he has been in
Barcelona, and professor of medicine at the Barcelona. Half his time is taken up with the
associated medical school at the Universidad ongoing transformation of what was a tiny oncol-
Autonoma de Barcelona. ogy effort into a major cancer treatment base for
He speaks from a position of considerable the province of Catalonia, such that 40% of all
strength and experience. Not only did he spend breast cancer patients in the region, for exam-
more formative years than most immersed in ple, are now seen at the hospital.
one of the top facilities in the US, but he has The other half of his work is translational
also put Vall d’Hebron on the map as one of the clinical and pre-clinical science – probably the
major translational research and cancer treat- area of cancer research that is weakest in gener-
ment centres in Europe – from a standing start. al wherever you go. “We have a huge effort here
“We must realise that medical oncology is on early clinical development of targeted thera-
still a new field – it is not even recognised as a peutics,” he says. “We do a lot of pre-clinical and
speciality in countries such as the UK,” he says. phase I trials on new compounds and we have
“It is no good pretending we are strong when we been blessed to have been involved with a large
actually lack strength at the European level number that are now on the market.”
compared to the US. But a lot of top oncology It all suggests that Baselga is well plugged in
work is European in origin. I don’t want to copy to both the many organisational issues that go
4 ■ CANCER WORLD ■ MAY-JUNE 2005
CoverStory
ELIGIO PAOLI / CONTRASTO
“I don’t want to copy what happens in the US but
play to our strengths – our capacity for cooperation”
CANCER WORLD ■ MAY-JUNE 2005 ■ 5
CoverStory
With his mentor into running a cancer centre, and the clinical the Memorial Sloan-Kettering Cancer Center in
John Mendelsohn research areas most likely to yield promising New York, which I’d never heard of.”
(left), at the MD results. There’s always a certain degree of good Initially he was accepted only for a three-
Anderson Cancer fortune involved, but what is clear is that he has month rotation, which confirmed his feeling
Center, Houston, been able to marry the scientific work he built that oncology was a fascinating subject and one
Texas, last June, up from his time in the US with the advantages he wanted to pursue. To do so in the US,
where Baselga of working in a public health system in Spain. however, he had to work his way back through
was awarded Baselga went to medical school at Vall internal medicine via internship and residency
the 2004 Waun-Ki d’Hebron – his background at the university positions elsewhere in New York, his Spanish
Hong Visiting hospital was one factor in his eventual return. “I qualification not being accepted. He then
Professorship absolutely fell in love with internal medicine and applied for a three year medical oncology and
began to be attracted to oncology.” Like many, haematology fellowship at Sloan-Kettering and
he saw cancer as a huge challenge. “But the was successful.
early 1980s were fascinating times – oncogenes “In the second year of the fellowship I had
were just being discovered and for the first time to choose a mentor and was very lucky to have
we had the promise that the molecular basis of John Mendelsohn, then chair of medicine – he
cancer was going to be found.” had produced the first anti-epidermal growth
His curiosity led to a request for an ‘elective’ factor receptor (EGFR) antibodies. I became
to a cancer centre, which was granted and involved in laboratory studies on EGFR antibod-
Baselga duly asked what would be a good place ies, and gained grants and ran clinical trials.”
to go to. “They said ‘America,’ and I went off to What happened next was the kind of break
6 ■ CANCER WORLD ■ MAY-JUNE 2005
CoverStory
that Baselga would now consider essential for development of EGFR and HER2 antibodies
any aspiring medical oncologist. He was offered and was giving up a lot. But there were frustra-
a faculty position at Sloan-Kettering, but tions in New York about the capacity to do good
because of visa restrictions he was unable to translational clinical science. It was extremely
take up the post until a waiver was arranged. difficult to enrol patients in clinical trials
This took about two years. “In the meantime I because of the regulatory atmosphere, and
had no licence to treat patients and that was tremendous difficulty in getting funding.”
wonderful because I spent all my time in the There were also, adds Baselga, difficulties in
lab. What happens with medical oncologists is simply getting people to work together at Sloan-
we get pushed all too soon into clinical duties – Kettering. “It was very hard for me to have, for
which is what we like and what we do best – but example, a good working relationship with the
it’s important to work in the lab too.” Today at pathology department. I did try very hard to run
Vall d’Hebron, he won’t give clinical jobs to peo- biopsy driven studies to look for biomarkers of
ple unless they have spent at least two years in activity in tumours – but I couldn’t do it.”
the laboratory. He puts this down to the professional and
“I did feel frustrated that I couldn’t see cultural structures in the US – “Still the same
patients like all my peers – but looking back it today I hear” – and says that team working is
was great because I was so productive in the lab. much better at Barcelona and indeed in other
At the time the HER2 antibodies had come out parts of Europe. “So I came here not only to
He won’t give clinical jobs to people unless
they have spent at least two years in the laboratory
and John Mendelsohn had received Herceptin build the oncology effort but also because I was
[trastuzumab] from Genentech to study. It was convinced I could do superb translational sci-
fascinating to see its effect on breast cancer ence here – and that’s been true. If you look at
cells and we became involved in the phase I and my CV you’ll see that my best translational work
II trials of Herceptin, and I was principal inves- has been done at Vall d’Hebron. I don’t feel
tigator on the phase II single agent trial where deprived of new compounds here – quite the
we saw the first sign of activity.” reverse. Just look at the number of trials we are
After his visa waiver came through Baselga doing here.”
took up his faculty post, continuing his joint lab In fact, no fewer than 55 trials were running
and breast service work. “I’d done the hard part in early 2005, including 15 phase I trials. This
and got my qualifications, green card and facul- level of activity has not been possible in the US,
ty job and I thought I’d now stay in the US. I was which has been the subject of much soul
publishing well and the research was exciting.” searching. While European trials involvement is
But by then he’d met and married his wife also patchy, Baselga’s experience indicates that
Silvia, a Spanish economist and also from the barriers here are more easily overcome.
Barcelona. They’d had their first child and she Baselga does, however, recognise the enor-
wanted to return home, and fortuitously Baselga mous advantages the US has in basic science
was sounded out for the opportunity to head the and cancer care, albeit marked by a big social
development of the new oncology centre at Vall divide driven by the medical insurance system.
d’Hebron. At first, it seemed like a hard decision “Memorial is full of excellence – they have many
for him. “I was involved in leading the clinical superb research scientists working there. They
CANCER WORLD ■ MAY-JUNE 2005 ■ 7
CoverStory
for which I’m very grateful to Genentech. I met
with the faculty and said I’d started the phase III
Herceptin trial at Sloan-Kettering and we had
an opportunity to translate the protocol here –
an opportunity that will very seldom come along.
It took many months and we were far behind –
but we entered more patients in the trial than
Memorial did.
“From the start we built a clinical trials
effort in pursuit of excellence and it sent a sig-
nal to the oncology community, although we
were lucky that the first results were positive
and so we got extra visibility – we were co-
authors on the New England Journal of Medicine
papers on Herceptin.
“The other thing I did was try to instil a
At home with have huge funding and vision and also many sense of pride in the staff who had been there
his family physicians working in clinical care. Overall, the for years. We had some great professionals who
US model has heavily influenced my career and had little self-esteem – they were just pushing
that of many others in Europe.” chemotherapy. I said to them: ‘This is medical
The authorities at Vall d’Hebron were fortu- oncology, this is the future and you’re good and
nate to find Baselga before he became too we have to do a good job’ – and they began to
entrenched in the American research commu- join societies and I helped them design trials of
nity, although he was young for such a move – their own and get published.”
just 37. “There’s a point of no return once you At the same time Baselga was working on
are on the career path to full professor and your obtaining more resources and funding – and the
family is settled over there,” he says. “Apart rapid ramp-up of trials work was a key factor. “In
from the timing, I also had the advantages that 1996, we were number 23 of all the research
I knew the hospital well, having been a student groups at Vall d’Hebron in terms of impact [i.e.
here, and am from Barcelona. But many times papers and citations]; by 2002 we were number
people come back to Spain from the US and one and were given more resources. It’s been a
other parts of Europe and have failed. If I’d huge victory – and now we are also the largest
have come back with a US mentality I would oncology trials site in Spain by far.”
have failed too.” Between 15% and 20% of patients are now
Certainly, he knew that the oncology depart- in trials – “It’s easier to do research in a public
ment at Vall d’Hebron was the Cinderella of the health system, and Spaniards are interested in
hospital – relegated to a few shabby consulting participating. We also make sure that patients in
rooms in an old part of the large complex, which trials are very well taken care of – they get the
is located on the edge of Barcelona. “First I set best nurses and superb physicians.” With
out to recruit my closest collaborators – people approval and budget restrictions, enrolling in tri-
who shared my vision and were prepared to roll als is also the only way that some patients can
up their sleeves, such as the head of research at access treatments such as taxanes, he adds.
the oncology department, Joaquin Arribas, who Essentially, Baselga has continued his work
was also at Sloan-Kettering. He was brave on molecular targeted therapies and signal path-
enough to come here to build the first oncology ways at Vall d’Hebron. “When I started here the
lab.” only agents available were anti-EGFRs and
Next, Baselga created a clinical trials pro- Herceptin, but then came the tyrosine kinase
gramme. “We set out to get involved in some inhibitors and we jumped on them, doing a lot of
important phase III trials, such as for Herceptin, studies on selecting the best dose and patient
8 ■ CANCER WORLD ■ MAY-JUNE 2005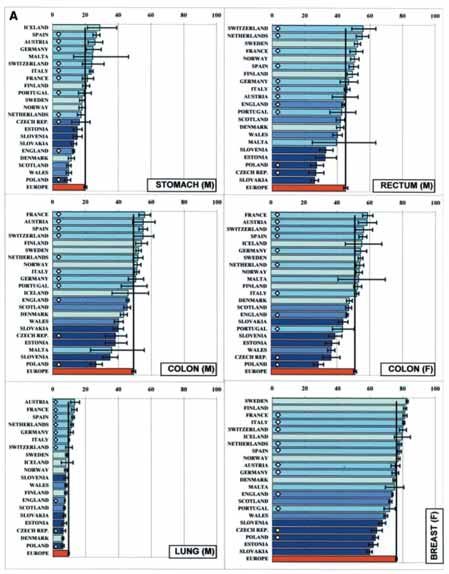
CoverStory
populations.” His recent and current work now tumour-focused multidisciplinary teams.” Breast
read like a roll call of new agents – trastuzumab, is a good place to start, he says, as many patients
cetuximab, gefitinib, erlotinib, EMD 72000, Ras need chemotherapy prior to surgery, and pathol-
inhibitors and a variety of anti-angiogenic agents ogists, radiologists and genetic counsellors are
– and his team has pioneered combined molec- all also involved – “So it is obvious we all have to
ular blockades, for example anti-EGFR and work together.” (And, pragmatically, it is also a
small molecules. cancer with a strong advocate community and
“We now only get involved in phase I trials fundraising potential, he notes.)
where we are part of the science – I’m not inter- If all this sounds like a smooth progression,
ested in pushing drugs and seeing whether they Baselga notes that in the early days many basic
are tolerated or not, which is the classic model problems had to be sorted out. They included
of phase I development. I think our obligation is convincing the hospital to upgrade the oncology
to understand why an agent is working and facilities from one of the worst to among the
selecting the right patients for treatment.” best; being open with patients about their con-
Facilities at Vall d’Hebron now include six dition, and not allowing families and consultants
labs and a refurbished and expanded oncology to hide the truth; and abolishing waiting lists (no
department. Baselga says he has strong patholo- mean feat given there are 3,000 new patients
gy and diagnostic departments and the key visits each year and 30,000 follow-ups).
differentiator compared to other translational Another issue familiar to many around
“It’s easier to do research in a public health system,
and Spaniards are interested in participating”
centres is multidisciplinary integration. It’s a far Europe has been persuading surgeons to spe-
cry from when he started – medical oncology cialise only in particular tumours – that’s been
was merely a referral point for chemotherapy. agreed at Vall d’Hebron, but is not the case yet
Now every tumour case is discussed in multidis- in outlying hospitals in Catalonia.
ciplinary teams with oncology playing the cen- Motivating the medical oncology staff has
tral role. also not been easy. “For example, I’ve had to
A new breast cancer centre will open next force people to learn English so they can travel
year – as he is a breast specialist it is natural that and participate in international forums, and
this has been a focus for expansion, but as he internal sessions are also conducted in the can-
points out research is now much more targeting cer community’s lingua franca.” Baselga is a
the molecular features of cancer and not its site. great advocate of networking and personal bond-
“I don’t feel restricted to one tumour type. Yes, ing with European colleagues. With funding
we do a lot of trials on breast cancer, which is from a Spanish bank he’s also inviting experts to
my main area, but also on colon, lung, and head come to Barcelona to give talks, but is equally
and neck cancers – wherever we see an oppor- keen that staff get to know them over lunch and
tunity we will try and adapt to that disease.” dinner.
The new breast centre, he adds, will be a It’s part of his drive to make the most of
“paradigm and laboratory” for future expansion. opportunities for co-operation within Europe.
“If it is successful we will open centres for gas- Outside of individual centres, Europeans can
trointestinal, prostate and other cancers – the often organise trials on large patient popula-
future for big academic hospitals is to create tions much quicker than counterparts in the US
CANCER WORLD ■ MAY-JUNE 2005 ■ 9
CoverStory
– studies on adjuvant Herceptin being a case produce educational materials, and is funding
in point, he notes. But the agenda for medical career development – as well as running a great
oncology is much broader and more journal and annual meeting. Given that Europe
challenging. has twice the population of the US, we should
The community needs to lobby for medical have a society of at least the same size and
oncology to be recognised across Europe as a influence as ASCO, especially to bring on the
key discipline, feels Baselga – medical oncolo- new generation of medical oncologists.” The
gists must be the pivotal players in multidisci- good news, he adds, is that ASCO does also
plinary teams. As he points out, only doctors operate as a global organisation, and would be
with a background in internal medicine can “very happy to help the European cancer
hope to understand the molecular basis of can- community”.
cer and in what combinations, settings and pop- Training of oncologists is an especially
ulation groups to administer treatment. “The important topic for Baselga, who is currently
quality of cancer care relates directly to the chair of ESMO’s young medical oncologists
strength of medical oncology in any centre – working group. Just as cancer care is far from
there’s no question of that. If you look around uniform across Europe, training also varies
Europe, there is a tremendous imbalance of greatly, which can only delay the establishment
quality of care – because we don’t have a strong of medical oncology as a specialism and the
speciality.” emergence of oncology leaders – of whom there
It is an opposite view from the one some- is a dearth, according to Baselga. “Are we taking
times heard from surgeons – that medical oncol- care of our young doctors and providing enough
ogy has become very powerful because it gets so funding for training? No – but the Americans
heavily funded by pharmaceutical companies. are.” He does currently have an Italian investi-
ESMO (the European Society for Medical gator under his wing funded by an ESMO award
Oncology), they argue, already has one of the – “She is a superb oncologist” – but there are
biggest European meetings. “But compare few such positions in Europe.
ESMO to ASCO [the American Society of So what other kind of changes does he
Clinical Oncology], which has 28,000 attendees envisage? “I don’t want another ASCO – let’s
at its conference – and just look at how many play to our strengths and be the champions of
presentations they have from Europe. I love multidisciplinary work. The European Breast
ASCO – it’s been fundamental to my career, it Cancer Conference is a good model for a meet-
gave me a young investigator award, a career ing, at least. We currently have two journals in
development award, and I’m a board member, Europe – the European Journal of Cancer and
but we are not doing our job here if most of our the Annals of Oncology – we should instead have
major papers go to them.” one strong publication to rival the American
It may surprise some to learn that ASCO Journal of Clinical Oncology [JCO]. The careers
has grown from about 15 employees to close on of young oncologists depend on publication, so I
300 since 1996 (and Baselga recalls that when can’t fault them for sending papers to JCO –
it was small he once got a call from the executive they have to look after themselves.”
director chasing him for a grant application). Lobbying at European and national level will
Those days are long gone. “Now ASCO has be critical to addressing resourcing gaps – and
tremendous lobbying power and capacity to Baselga isn’t alone in wanting a professional lob-
“The quality of cancer care relates directly
to the strength of medical oncology in any centre”
10 ■ CANCER WORLD ■ MAY-JUNE 2005CoverStory
Speaking
at a conference
attended by Spain’s
Queen Sofia
at the Real
Academia
de Medecina
in Barcelona,
October 2004
bying and fundraising operation. “We need mini- breast cancer by 45%. If these aren’t break-
mum standards for cancer care agreed by law and throughs, what are?”
to create a European movement against cancer.” Americans are rather more gung ho. “The
In Catalonia, Baselga is playing his part – dinner Breast Cancer Foundation has a powerful logo,
with the president of the region helped cement the MD Anderson Cancer Center’s logo is
12 million euros for his new research laborato- ‘Making Cancer History’. Memorial Sloan-
ries, and he’s a regular on TV, including a Kettering says it has the ‘best cancer care any-
‘telethon’ fundraising programme that involved where’.” That’s the kind of branding he’d like to
patients speaking up about their treatment. He see more widely applied, and with the “phenom-
has also set up a research foundation (Fundació enal progress” being made with the many new
Privada d’Estudis i Recerca Oncològica – compounds he’s involved with, there is no short-
FERO), through which the breast centre and a age of achievements to trumpet.
new head and neck cancer lab are being funded, With so much to work on he’s probably glad
and he hopes to set up scholarships and young of the distractions of home life. He’s now a
investigator awards. father of four children aged 12 and under – and
Medical oncologists also need to speak out they sound like an outward bound family; “My
more about their achievements. Baselga often wife and I are mad on skiing, hiking and biking.”
talks of breakthroughs in clinical research – Family life should keep him in Barcelona for the
again, this is something to learn from the US. foreseeable future – but he gets plenty of big job
“There is a psychological issue here with the way offers from other cancer centres, especially in
medical oncologists communicate – we are mak- the US, who want the best person to lead their
ing breakthroughs all the time. Breast cancer clinical research, so the attractions of Europe
mortality is dropping 2–3% a year. Colon cancer may not be enough to keep him for ever.
response rates used to be 12–15% with available When he’s not reading medical papers,
chemotherapy – and now with new agents the Baselga likes to pursue his keen interest in mod-
response to metastatic disease is 84%. ern history. One senses that, at just 45, Baselga
Herceptin increases survival of HER2 positive has every chance of making a history of his own.
CANCER WORLD ■ MAY-JUNE 2005 ■ 11GrandRound
They could be alive
today
➜ Anna Wagstaff
Every year thousands of people die unnecessarily from cancer because their
care is sub-optimal or arrives too late. Europe has known where the problems
are for more than a decade and has the knowledge to improve matters. It is
the political will that is lacking.
D
uring the 1990s, a series ices, with an emphasis on reducing would be horrified to know how fre-
of reports emanating waiting times and ensuring equal quently this happens.
from the EuroCare access to specialist care. Denmark Take breast cancer. Pathologists
project revealed signifi- also took measures to improve the were once simply required to define
cant differences bet- quality of its cancer care. the extent and type of tumour
ween survival rates for a wide variety of Many lessons were learnt. But through examining its morphology;
cancers in European countries. there is plenty of evidence to show today, they have to characterise the
Five years after being diagnosed, that patients are continuing to die cancer in far greater detail. They
a stomach cancer patient in Iceland across Europe because available report on how many lymph nodes are
was around three times more likely to knowledge and techniques are not involved and evaluate the tumour for
be alive than a similar patient in being used to best effect. Indeed, oestrogen, progesterone and HER2
Slovakia, the UK, Denmark, or some experts believe that the situa- expression. On the basis of these
Poland. The differences were not just tion is likely to get worse. reports, fundamental decisions are
about resources, because Denmark made such as whether the patient
and the UK are relatively affluent KNOW YOUR DISEASE requires adjuvant chemo- and/or
with access to the latest drugs and up Oncologists need to know an increas- radiotherapy, whether hormonal ther-
to date equipment. Many factors may ing amount about the pathology of the apy is sufficient, or whether the
have skewed the results, but it was disease. If the tumour has been incor- patient can safely forego adjuvant
hard to avoid the conclusion that rectly defined or wrongly staged, the therapy following surgery.
some patients were dying because treatment will be sub-optimal. Viale says that confidence in
their cancer care was not up to Guiseppe Viale, professor of patholo- these reports is often misplaced. “We
scratch. gy at the University of Milan – know that 20–25% of patients who
The EuroCare statistics shocked European Institute of Oncology have been assessed as node-negative
the UK into overhauling cancer serv- (EIO), believes that most oncologists have disease recurrence and will
14 ■ CANCER WORLD ■ MAY-JUNE 2005CANCER WORLD ■ MAY-JUNE 2005 ■
15
GrandRound
JOSE LUIS PELAEZ, INC. / CORBIS / CONTRASTOGrandRound
eventually die of the disease. If we go
back to those regional lymph nodes
and examine more sections, we will
find metastases in the large majority
of these patients. The risk to these
patients was not assessed correctly in
the beginning.”
The story on endocrine response
status is hardly more encouraging.
Quality control in the UK has estab-
lished that the false-negative result
for oestrogen and progesterone recep-
tors lies somewhere between 15%
and 25%; the picture in Germany is a Source: M P Coleman, G Gatta, A Verdecchia et al. EUROCARE-3 summary: cancer survival in Europe
little better (11–24%). Many at the end of the 20th century. Annals of Oncology (2003) vol 14 (Suppl 5): v128–v149. Reprinted with permission
European countries have no quality of Oxford University Press
control procedures, and the results
coming out of their labs could be even
more unreliable. Viale estimates the learnt only after he left his job in a medical oncology training is very sim-
false-negative figures in Italy to be general hospital. “I thought I knew ilar to that in Western Europe and
closer to 20–25%. breast cancer, but when I started that money is available for cancer
There are also problems with working at the EIO, I changed my drugs. However, clinicians cannot
HER2 evaluation. False-positive approach completely. I started to always treat patients effectively
rates of up to 30% are common and realise, for instance, that saying ‘10% because they are unable to charac-
this is true whether the assay is done progesterone positive’ is completely terise the disease.
by immunohistochemistry or using different to saying ‘80% positive’ in There are no immunohistochem-
the FISH (phosphorescence in situ) terms of treatment – it’s not just a istry testing facilities outside the main
procedure. The problem, says Viale, question of saying ‘negative’ or ‘posi- cancer centres in Bucharest and Cluj,
lies with the pathologist rather than tive’. Once you realise that, you are and these centres do not offer servic-
the test. ready to spend the necessary time to es to smaller hospitals. Access to
“You can see that a large fraction make an accurate evaluation.” imaging techniques such as bone
of breast cancer patients are not One way to help pathologists scan, CT and MRI is also extremely
treated properly… it makes you a bit become more aware of the signifi- limited. The ultrasound equipment is
nervous about what is happening cance of their role would be to make 20 years old, and unreliable.
around you.” funding available for pathologists “There must be some way to
Problems are more evident in from centres participating in clinical organise the system to work better
breast cancer, because we know more trials to attend coordinating meetings. with the money we have,” says
about subtypes and the implications They should also receive feedback on Udrea. “We are spending money for
for treatment than for many other the quality of their evaluations in real expensive drugs, but we don’t know
cancers. But differentiation and tai- time, rather than several years later what we need to know in order to use
lored treatment is the future for most after the trial has closed. them effectively.”
cancers, giving the role of the pathol- In some countries poor access to The problem is not confined to
ogy labs even greater importance. the latest diagnostic and imaging central and eastern European coun-
Viale believes that pathologists techniques is an obstacle to accurate- tries. In Italy, for instance, though
who are not working as part of a mul- ly defining the disease. costly trastuzumab prescriptions are
tidisciplinary team are not aware of Adrian Udrea, who works in the reimbursed by the national health
how their conclusions determine chemotherapy department at the system, the HER2 test that indicates
treatment. Oncological Institute of Cluj, whether the tumour might respond to
This is something Viale himself Romania, says that the standard of the drug is not.
16 ■ CANCER WORLD ■ MAY-JUNE 2005GrandRound
Comparative index
of 5-year relative
survival (%) by
country for adults
diagnosed in the
period 1990–1994,
followed up to
1999. These were
the graphs that
shamed the UK into
improving cancer
services
15 rectal or 15 oesophageal or 15 pan-
creatic or 15 gastric cancers a year, you
shouldn’t do any at all, because you are
automatically associated with worse
outcomes.”
This principle has been recognised
in Europe for 20 years, and many
countries encourage regional or
national specialisation – but bad
practice still continues. Eggermont
says that there is a need for a new
referral culture, where different units
work collaboratively rather than
competing for patients, and agree a
rational way to divide specialist services.
Even in the Netherlands, with its
excellent referral culture and commit-
ment to regional specialisation, it is
proving hard to stop a few errant
small hospitals carrying out low
volumes of oesophageal or pancreatic
operations. The situation is probably
KNOW YOUR PROCEDURE Expert surgery is also associated with far worse in other countries, particu-
SURGERY far lower local recurrence rates – larly those with weaker public health
Since the 1980s, studies have shown between five and ten times lower in sectors and poorly coordinated cancer
that referring a patient to a specialist the case of rectal surgery. treatment delivery, and in poorer and
centre for difficult procedures to Lex Eggermont, head of surgical more rural areas.
excise pancreatic, gastric and rectal oncology at the Erasmus University The public have little access to
cancers significantly lowers their risk Medical Centre in Rotterdam, says information about volume. However,
of dying from postoperative complica- observing simple principles will min- www.corriere.it/sportello-cancro, a
tions. The latest figures from the imise unnecessary deaths from poor website supported by the leading
Netherlands show patients operated surgery. “First you must be well Italian daily the Corriere della Sera and
for pancreatic cancer in small hospitals trained. Second, there is a direct vol- the Umberto Veronesi Foundation,
are ten times more likely to die than ume effect – the more you do, the bet- provides a fascinating insight into how
those treated in the larger centres. ter you are. If you don’t do more than surgical procedures are divided
CANCER WORLD ■ MAY-JUNE 2005 ■ 17GrandRound
with new cancers up to 20 cancers and the arena in which major
years later and there is some advances are expected. Unfortunately,
evidence to show that high- it is also least amenable to quality
dose radiotherapy to treat control.
Hodgkin’s lymphoma or In the 1980s and ’90s, huge varia-
breast cancer can damage tions in the way patients were being
the heart. treated led to much greater emphasis
Intensity modulated radio- on evidence-based medicine. The idea
therapy allows for more was to educate all oncologists to act
aggressive and effective according to the best available evi-
treatment, concentrating dence rather than relying on empirical
firepower on the tumour and knowledge or on the established policy
sparing normal tissue to a in their departments.
greater extent. However, if Recently published studies show
mistakes are made, the dam- that following guidelines has an
age can be all the greater. impact on survival. However, the key
Jacques Bernier of the to success lies in how guidelines and
Oncology Institute of evidence is applied to each patient.
Southern Switzerland in Aron Goldhirsch of the
Bellinzona, says, “We have to Department of Medicine at the
The Italian website www.corriere.it/sportello-cancro. have much stricter controls European Institute of Oncology, wor-
For the best chance of survival, click the relevant part before irradiating, because if ries that too many medical oncologists
of the body to find out which hospitals in your region the plan calculation and the use guidelines uncritically and pre-
have the greatest experience in dealing with your type delivery don’t correspond, scriptively.
of cancer – and which hospitals to avoid you can give two, “Every patient is absolutely
three or four times the dose unique, but part of a population.
you calculated.” Statistics and epidemiology have
between major centres and peripheral Gross errors are rare however. brought medicine away from individ-
hospitals across Italy. It shows that One UK study of almost 2000 patients ual patients, so that what is said is
around 230 hospitals are carrying out treated with 95,000 individual actually ‘on average’. It’s like ‘one-size-
surgical procedures for cancers of the doses showed an error rate of 0.18%, fits-all’. If we don’t recognise patterns
digestive tract even though their all of minor clinical significance. of diversity from one individual to
annual case load is less than the Of greater concern, is the under- another, and we take an average
recommended 15. When the figures investment in latest equipment and answer as a good answer for everyone,
are broken down to surgery on the software, leading to increased waiting we are likely sometimes to be wrong.”
oesophagus or rectum, the number of time or treatment using outdated Statistics in cancer medicine is
hospitals carrying out between 1 and methods. Radiotherapy now forms a typically used to group people into
15 procedures is very much higher. part of the treatment of more than wider populations in order to analyse
50% of all cancer patients, but outcome and factors that influence
RADIOTHERAPY according to the European Society for response to treatment. Goldhirsch’s
Of all cancer treatments, radiotherapy Therapeutic Radiology and Oncology concern is that no-one is teaching the
is the easiest to systematise. It is con- (ESTRO), the services in many coun- methodology of applying those statis-
centrated in larger centres, with fewer tries cannot cope with this level of tics to the individual patient.
problems associated with low volumes demand, and access to treatment is Goldhirsch is involved in the
of treatment. Decades of quality con- now a major problem. MINDACT breast cancer trial
trol prevents most easily identifiable (MIcro-array for Node negative
mistakes, but controversy remains KNOW YOUR PATIENT Disease may Avoid ChemoTherapy),
over long-term effects. Radiation for Medical oncology has emerged as the which seeks to find out how respons-
testicular cancer has been associated defining mode of treatment for most es to therapies vary according to the
18 ■ CANCER WORLD ■ MAY-JUNE 2005GrandRound
specific genetic and pathologic char- morbidities such as heart conditions MULTIDISCIPLINARY TREATMENT
acteristics of subgroups of node nega- or diabetes. They may be taking other Top quality pathology, medical oncolo-
tive breast cancer. medicines and their organs may not gy, surgery and radiotherapy are all
He says that, while breast cancer be functioning normally. Pinedo feels essential to save every patient who can
is ahead of the field in defining sub- young oncologists are not being be saved. But each mode of treatment
types and identifying oncogenes, the taught to take this into account when becomes significantly more effective
same process is now happening else- they prescribe medication, and some in the presence of the vital ingredient:
where, and all cancers will require patients are being put at risk as a multidisciplinary collaboration.
ever more precise treatments. The result. “You need to know what is The majority of treatments
trouble is that as much of the evidence going on with the patient. You need to involve two or three types of therapy,
that oncologists currently use repre- do a lot of research making use of often interlinked. Almost 90% of all
sents only an average response, some their tissues and blood to understand radiotherapy now takes place within a
tumour subgroups will respond better the biology, to understand their phar- multidisciplinary framework.
than the average, and others may not macodynamics. It’s not just a ques- Effective multidisciplinary work-
respond at all. tion of measuring drugs, you need to ing makes it possible to select the
A wise oncologist, says know the effects of your drugs on the most effective treatments with the
Goldhirsch, does not apply evidence organs.” least damage to the patient.
unquestioningly, especially when Knowing your patient also means Supportive care is also essential.
detailed information is not available. knowing who is at extra risk of cancer. Nutrition, for instance, can make the
‘Average’ data are just not precise Pinedo is frustrated at lack of effec- difference between surviving or dying
enough. “Doubt is very important. tive monitoring for people known to for very ill patients. Monitoring and
When you don’t have anything else, be at very high risk. dealing promptly with life-threatening
evidence-based is by far the best, but He wants to see women who have side-effects such as thrombocytopae-
you must use it critically or you end a family history of BRCA positive nia and neutropaenia is essential; the
up stagnating knowledge.” breast cancer routinely screened by involvement of expert cancer nurses
Encouraging oncology depart- MRI, to detect disease earlier than by in the multidisciplinary teams can
ments to participate in well-struc- mammography. make a difference here.
tured clinical trials that apply tailored People with familial colon cancer Such a multidisciplinary approach
treatments, would be one of the most also need more effective screening he is impractical outside of larger hospi-
effective ways to improve their says. Studies coming out of the US tals or networks of collaborating cen-
methodological approach, he says. and the Netherlands have shown that tres. Where cancer patients make up
Bob Pinedo, director of the VUmc only half of the patients in whom ade- only a small proportion of a surgeon’s
Cancer Centre at Vreie Universiteit nomatous polyps had been indenti- or pathologist’s work, they will not be
hospital in Amsterdam, emphasises fied by colonoscopy show positive for able to organise their timetables
the diversity of patients, as well as the colon cancer using the faecal occult around multidisciplinary meetings,
diversity of tumour types and believes blood (FOB) test. So why, asks which would in any event happen too
that young oncologists need more Pinedo, are we still relying on this infrequently for them to build a rela-
training in internal medicine to allow method of detection for people tionship or to understand the roles
them to tailor treatment to their known to be at high risk? “I foresee a and problems of other specialists.
patient. big problem here. We will get angry It is the combination of specialist
Medical oncologists give toxic people who have been screened with surgery and multidisciplinary working
drugs to people who may not only be the FOB test and they get cancer, and that has been credited with signifi-
weakened by cancer, but have co- they will say why did this happen?” cant differences in survival rates
If we don’t recognise patterns of diversity from
one individual to another, we will make mistakes
CANCER WORLD ■ MAY-JUNE 2005 ■ 19GrandRound
Involving pathologists, cancer nurses and dieticians
in the team can make a difference to survival
between larger centres and peripheral very few EU countries have sufficient you accept an operation within eight
hospitals in a number of studies, linear accelerators and trained staff to weeks. I just cannot work that way. I
notably in Scotland in the early provide an adequate service, and that find it horrible, because we don’t tell
1990s. Finding a way to deliver spe- a high proportion of patients are treat- our patients the risks.”
cialist multidisciplinary treatment to ed outside clinically acceptable time
all patients, no matter where they limits. WHAT NEXT?
live, is one of the logistical challenges Where waiting lists are long, All over Europe, patients who could
for good cancer care. radiotherapy departments systemati- have been saved are dying because
cally treat patients when they know it they did not get high-quality treat-
TEACHING CANCER is too late, and doctors have to choose ment when they needed it. We know
Decades after the multidisciplinary which patient will receive the best a lot about the training and systems of
approach was recognised as effective, care today, and which will have to care delivery needed to avoid unnec-
it is still rarely taught as a concept in wait – or be assigned to palliative essary deaths. We need now to know
medical schools. treatment simply because their how to get there from here.
Franco Cavalli of the Oncology chance of a cure is below the thresh-
Institute of Southern Switzerland, old that makes them a priority within PATIENT POWER
Bellinzona, says the fragmented way an overstretched system. Many argue that patients hold the
in which cancer is taught lies at the Pinedo believes there is also a key, through exercising informed
heart of many problems. “There is no critical shortage of oncology special- choice over where they are treated.
overall teaching in oncology. You will ists across Europe that will become Eggermont says the most effective
have the internist, who will talk a lit- more acute as more patients survive thing to do is “bombard” patients with
tle bit about cancer, the surgeon, who longer. “We know that the prognosis advice to ask their hospital the crucial
will talk a little bit about cancer, the for colorectal cancer improves if you questions: “How often are these pro-
pathologist and so on. Most universi- do secondary surgery. But if you have cedures performed here? What is your
ties do not have well-structured a waiting list of months for a primary track record? What are your mortality
teaching on cancer, and because of colon cancer, you are not going to figures?” And if the answer is not reas-
that most physicians, when they fin- take a patient with a little metastasis suring, they should go elsewhere.
ish their training, do not know and put them on the list.” Pinedo still Patient groups have been advocat-
enough about cancer.” goes to multidisciplinary meetings ing this approach for years, but they
and argues for that surgery to be have precious little information to go
WAITING TO DIE done, but he is aware of the pressure. on; the Sportello Cancro website is an
The best cancer services are under- “You know the surgeon is already very exception. Eggermont would like to
mined if patients do not receive a upset because of his waiting list. I see similar statistics on volume and
diagnosis and treatment when they know I’m asking them something I track record available in all countries.
need it. Evidence shows that in some shouldn’t ask, because there are cer- “That would force the system to
tumours, making patients wait weeks, tain things you just cannot ask these reform.”
sometimes months, for radiotherapy days, even though you know it is the In the Netherlands, the Breast
reduces their chance of a cure, allow- best for the patient.” Cancer Patients Association is setting
ing the tumour to grow beyond a ‘cur- He worries that the medical pro- its own agenda. It has drawn up qual-
ative size’ or to metastasise. ESTRO, fession seems to accept delays as a ity guidelines, covering issues such as
the professional body for European fact of life. “If 30 years ago you would waiting lists, expertise and choices
radiologists and radiotherapists, says say, ‘operate within four weeks’, now between different interventions, and
20 ■ CANCER WORLD ■ MAY-JUNE 2005GrandRound
has set a deadline of January 1 2007 ulation with access to specialist facili- tion. If, for instance, hospitals are
for treatment centres to comply or ties. This is the system that has kept obliged to contract out specialist
face a boycott by patients. Sweden, Finland and the Netherlands pathology services, there is no way
A Europe-wide accreditation sys- at the top of the cancer survival that pathologists will be able to work
tem for specialist breast cancer units, league. It is now being emulated by within a multidisciplinary team.
developed and operated by the countries like the UK, Ireland and Health budgets are generally stat-
European Society of Mastology, is in France, which can build on a strong ic or shrinking, because of pressure to
the pipeline. This will set standards base of 20 regional cancer centres. limit public spending. He says there
for specialist centres in breast cancer Building new state of the art can- is a danger of developing the two-tier
care, and will offer an important cer centres is not always the issue. The health system that exists in the US –
marker for patients deciding where to Netherlands, for instance, is develop- a highly sophisticated system for
go for treatment. ing a structure designed to achieve those who can afford it, and a funda-
But directing patients to the best top-quality treatment in smaller hospi- mentally inadequate one for those
treatment centres creates its own tals that agree to specialise and coordi- who cannot.
waiting list problems. Patients may nate their work. It does, however, Cavalli points out that life
have to choose between waiting eight require a system in which there is no expectancy in Russia has decreased
weeks for top-quality treatment, or big financial loss in referring a patient by around seven years since the col-
immediate treatment at a hospital elsewhere. It is also easier in more lapse of state-led systems, some of
with less expertise. In the end, says concentrated populations, although which can be attributed to the col-
Pinedo, pressure on centres of excel- Sweden pioneered this system, and lapse of the health system. He says
lence can compromise the quality of distances there can be great. there is no reason to believe that min-
care they can offer. The French national cancer plan, imising the public sector and encour-
The European Court of Justice introduced in 2003, represents a wel- aging private provision in eastern
believes that patients should be able come attempt to address all aspects of Europe will provide an effective can-
to use their power. In three landmark cancer care: training and continual cer service for more than a tiny part of
cases between 1998 and 2003, it medical education, equal access, a the population.
ruled that patients have the right to mandatory multidisciplinary approach
be reimbursed for treatment in another and patient information. Importantly, MONITOR THE SYSTEM
Member State if they cannot get the it also supports the work of the French Funding for the EuroCare project
treatment they need from their own cancer registries, which should pro- has dried up, and as a result many
health system within a reasonable vide information that can be used to national or regional registries have
time. further improve the system. lost their sense of dynamism and
This is not a solution, since it Despite these encouraging signs, purpose. Many registers have also
does not create any new resources in Cavalli cautions that France has been hit by privacy legislation,
the offending state, but it establishes always believed in a strong state, and though some people argue this is
the legal principle that timely treat- is probably an exception. He argues more of a problem of political will or
ment is a right that health services that the current European economic legal interpretation.
cannot ignore. and political climate is driving the Jan Willem Coebergh, of the
organisation of public services Eindhoven Cancer Registry in the
PLAN AHEAD towards greater liberalisation, which Netherlands, says he is worried by
In the end, the answer lies in net- may be counterproductive since can- this apparent retreat from the
works of adequately resourced centres cer care needs well-planned systems approach that taught us much of what
that can provide all sectors of the pop- driven by collaboration not competi- we now know about unnecessary can-
Very few EU countries are able to provide
an adequate radiotherapy service
CANCER WORLD ■ MAY-JUNE 2005 ■ 21GrandRound
cer deaths. His concern is that, with-
10 ways to prevent
out effective registries, we will no
longer be able to tell which systems or
procedures are working and which are
unnecessary deaths
not. Ian Kunkler, who analysed reg-
istries for the Scottish cancer plan,
agrees. “A cancer service without can-
cer registration is like a clinical trial
without a statistician.”
Norway is swimming against the
1
Training. Teach oncology in a holis-
tic way instead of splitting it
between disciplines and organ spe-
6
Multidisciplinary working.
Ensure that all cancer treatment
takes place within a multidiscipli-
tide. The government is investing cialties. Teach the importance of nary setting, either within one hos-
heavily in upgrading its registry early detection, multidisciplinary pital or by co-ordinating specialists
system to include detailed pathologi- treatment and comorbidity issues. from different hospitals.
cal and clinical data. Surgical proce-
dures, radiotherapy and medical
treatment will be recorded as well as
instances of recurrences and metas-
tases. This huge project requires
2
Pathology. Raise awareness among
pathologists of the key role they play.
Involve pathologists in planning and
7
Networks. Organise well-struc-
tured networks of specialist centres.
close cooperation between registries executing clinical trials. Introduce Encourage a culture of referral
and clinicians, but the government is greater quality control, and feedback where hospitals collaborate rather
convinced that the information it results quickly. than compete for patients.
yields about variations in survival will
be worth it.
But there is also plenty that could
be learnt from less ambitious projects
that analyse smaller populations. The
3
Surgery. Ensure that surgeons carry-
ing out complex procedures do at least
15 such cases a year. Make relevant
8
Registries. Monitor effectiveness
by collating and analysing data on
European Network of Cancer information available on the Internet diagnosis, treatment and survival.
Registries has recently regrouped and and encourage patients to choose
is looking to promote these sorts of
studies throughout Europe.
WINNING THE ARGUMENT
People will continue to die from can-
carefully where they go for treatment.
4
Radiotherapy. Ensure rigorous
quality control of high-dose modern
9
Waiting time. Delays can cost
lives. Define acceptable time frames
for imaging, pathology and specialist
cer under any system. However, dying procedures. Conduct long-term stud- treatment of different cancers, and
because your health system let you ies to monitor possible late side- provide sufficient resources and
down, you live in the wrong country effects such as heart problems in effective systems to keep delays
or even in the wrong part of the coun- breast cancer and Hodgkin’s patients, within those limits. Educate
try, is not inevitable and should be or new tumours that may emerge patients to demand treatment with-
considered unacceptable. decades after treatment. in that time frame.
When the compelling voice of
patients and their families joins with
the medical profession and is backed
by firm evidence, it is possible to cap-
ture the media and political agenda.
5
Medical oncology. Promote the
use of evidence-based guidelines
and encourage oncology depart-
10
Cancer plans. Organise national
and regional cancer plans, covering
That is what is needed to force gov- ments to participate in trials. training, resource allocation, loca-
ernments to address the inequities Improve training in interpreting sta- tion of specialist services, profes-
revealed by the EuroCare data, and tistical evidence to tailor treatment sional guidelines, quality control,
ensure that every cancer patient is to individual patients. and evaluation.
given the best chance of life.
22 ■ CANCER WORLD ■ MAY-JUNE 2005You can also read