Effective Parenting Interventions to Reduce Youth Substance Use: A Systematic Review
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Effective Parenting Interventions
to Reduce Youth Substance
Use: A Systematic Review
Michele L. Allen, MD, MS,a Diego Garcia-Huidobro, MD,b,c Carolyn Porta, PhD, MPH, RN,d Dorothy
Curran, BS,b Roma Patel, MPH,a Jonathan Miller, MURP,e Iris Borowsky, MD, PhDb
CONTEXT: Parenting interventions may prevent adolescent substance use; however, questions abstract
remain regarding the effectiveness of interventions across substances and delivery qualities
contributing to successful intervention outcomes.
OBJECTIVE: To describe the effectiveness of parent-focused interventions in reducing or
preventing adolescent tobacco, alcohol, and illicit substance use and to identify optimal
intervention targeted participants, dosage, settings, and delivery methods.
DATA SOURCES: PubMed, PsycINFO, ERIC, and CINAHL.
STUDY SELECTION: Randomized controlled trials reporting adolescent substance use outcomes,
focusing on imparting parenting knowledge, skills, practices, or behaviors.
DATA EXTRACTION: Trained researchers extracted data from each article using a standardized,
prepiloted form. Because of study heterogeneity, a qualitative technique known as harvest
plots was used to summarize findings.
RESULTS: A total of 42 studies represented by 66 articles met inclusion criteria. Results
indicate that parenting interventions are effective at preventing and decreasing adolescent
tobacco, alcohol, and illicit substance use over the short and long term. The majority
of effective interventions required ≤12 contact hours and were implemented through
in-person sessions including parents and youth. Evidence for computer-based delivery was
strong only for alcohol use prevention. Few interventions were delivered outside of school or
home settings.
LIMITATIONS: Overall risk of bias is high.
CONCLUSIONS: This review suggests that relatively low-intensity group parenting interventions
are effective at reducing or preventing adolescent substance use and that protection may
persist for multiple years. There is a need for additional evidence in clinical and other
community settings using an expanded set of delivery methods.
NIH
Departments of aFamily Medicine and Community Health, and bPediatrics, University of Minnesota Medical School, Minneapolis, Minnesota; cSchool of Medicine, Pontificia Universidad
Catolica de Chile, Santiago, Chile; and dDepartment of Population Health and Systems, School of Nursing, and eDivision of Epidemiology and Community Health, School of Public Health,
University of Minnesota, Minneapolis, Minnesota
Dr Allen conceptualized the study, led study design, contributed to data extraction, and wrote the initial draft of the manuscript; Dr Garcia-Huidobro contributed
to study design, led data extraction, and reviewed and revised the manuscript; Dr Porta contributed to study design and reviewed and revised early drafts of the
manuscript; Ms Curran and Ms Patel contributed to data extraction and study design and reviewed and revised early drafts of the manuscript; Mr Miller contributed
To cite: Allen ML, Garcia-Huidobro D, Porta C, et al. Effective Parenting Interventions to Reduce Youth Substance Use: A Systematic Review. Pediatrics.
2016;138(2):e20154425
Downloaded from www.aappublications.org/news by guest on July 13, 2021
PEDIATRICS Volume 138, number 2, August 2016:e20154425 REVIEW ARTICLEDespite recent encouraging from the perspective of future METHODS
trends, youth tobacco, alcohol, and implementers include the following:
other illicit drug use continue to Who needs to be involved, for how Search Strategy
represent a considerable source of long, in what settings, and through
youth morbidity and mortality and what means? However, to the best As reported in the review protocol
establish behavioral patterns that of our knowledge, no reviews have (PROSPERO systematic review
have detrimental health outcomes comprehensively examined the registry number CRD42014013069),
into adulthood.1,2 There is therefore a state of the evidence regarding we searched PubMed, PsycINFO,
need to identify effective prevention targeted participants (parents ERIC, and CINAHL for studies
strategies and to better understand only vs both parents and youth), investigating parent-focused
the delivery qualities contributing to minimal dosages required to achieve interventions designed to reduce
successful intervention outcomes. outcomes, ideal delivery settings substance use in adolescents. Search
(schools, community organizations, terms are presented in Table 1. The
One approach to adolescent
clinics, homes), and optimal delivery search included all dates available by
substance use prevention builds on
modalities. The lack of evidence respective online databases up to the
the recognition that parents play
regarding success of implementation date of March 1, 2015.
a key role in promoting healthy
within clinics is problematic at a time
adolescent behaviors and therefore
when prevention and integrated Eligibility Criteria
focuses on strengthening parenting
services are emerging as pediatric
skills.2 The influence that parents
primary care targets within the This review included studies
have on their adolescent children
Affordable Care Act.8 In addition, published in any language
has been substantiated by numerous
although multiple modalities of meeting the following criteria:
studies linking a well-defined set of
program delivery are known to (1) intervention studies focused
parenting practices (ie, monitoring,
appeal to parents and increasing on adolescents (mean age of
discipline, communication)
evidence supports the use of online participating youth between 10
and qualities of parent-youth
prevention programming, few and 19 years), (2) reported youth
relationships (ie, warmth, support,
reviews have examined the state smoking, alcohol, or illicit substance
acceptance, attachment) to
of the literature across delivery outcomes (intention, initiation, or
adolescent behavioral outcomes
methods for parenting interventions use), and (3) involved parent training
including substance use.3,4 Parenting
focused on adolescent substance use with focus on imparting parenting
interventions for parents of
prevention.7,9 knowledge, skills, practices, or
adolescents broadly focus on building
parent self-efficacy in implementing behaviors.
This systematic review therefore
skills and engaging with their
aims to assess the effectiveness of Exclusion criteria were (1) design
children in a manner encouraging
parenting interventions over the not a randomized controlled trial, (2)
health-protective and preventing risk
short and long term on reducing adolescents were the participating
behaviors. Previous reviews suggest
adolescent tobacco, alcohol, and illicit parents, (3) intervention focused
that parent-focused interventions
substance use and, secondarily, to on specific populations (eg, parents
directed at adolescent substance use
describe effectiveness in relation to of children with cystic fibrosis or
are effective; however, to the best of
intervention characteristics (targeted other medical conditions), (4) study
our knowledge, no systematic review
participants, intervention dosage, compared 2 parenting interventions
of parenting interventions delivered
delivery settings, and delivery without a usual care condition,
during adolescence has looked across
method), using visual depictions of and (5) individual family therapy
multiple substances,3,5,6 nor has any
qualitative data summaries called interventions distinguished from
considered intervention delivery
harvest plots. These plots represent parenting-skills interventions in their
modalities or contexts.
a novel approach to synthesizing focus on changing behaviors though
With increasing focus on evidence- the findings of systematic therapeutic rather than curricular
based adolescent health promotion, reviews focused on complex and approaches.
and given that poor reach is a known heterogeneous interventions that
challenge for parenting interventions, cannot be combined into a meta- Two independent reviewers (DGH
consideration of evidence analysis.10 Results of this review will and RP) screened titles, abstracts,
regarding how to most effectively inform the development, tailoring, and full texts of potential articles.
and efficiently reach families of and delivery of parent-focused A third reviewer (MLA) resolved
adolescents becomes important.7 interventions to improve adolescent disagreements regarding inclusion of
Practical questions of interest health. a study.
Downloaded from www.aappublications.org/news by guest on July 13, 2021
2 ALLEN et alTABLE 1 Search Terms Used to Search for Articles in PubMed, ERIC, CINAHL, and PsycInfo
(“Family”[Mesh] OR Famil* OR Parent*) AND “Adolescent”[Mesh] AND (“Clinical Trial” [Publication Type] OR “Clinical Trials as
PubMed Topic”[Mesh]) AND (“Alcohol Drinking”[Mesh] OR “Smoking”[Mesh] OR “Substance-Related Disorders”[Mesh] OR smok* OR
substance* OR alcohol* OR marijuana* OR cocaine* OR amphetamine* OR heroine*)
(parent* OR famil*) AND (“Clinical Trials+” OR Randomized OR “Parenting Education” OR “parent education”) AND (Adol* OR
ERIC teen* OR youth*) AND (tobacco or smok* or alcohol OR substance or marijuana or cocaine or heroin or methamphetamine or
amphetamine or prescription or drug*)
(parent* OR famil*) AND (“Clinical Trials+” OR Randomized OR “Parenting Education” OR “parent education”) AND (Adol* OR
CINAHL teen* OR youth*) AND (tobacco or smok* or alcohol OR substance or marijuana or cocaine or heroin or methamphetamine or
amphetamine or prescription or drug*)
(adolescent or teen or youth or adolescents or teens or youths or adolescence) AND (exp family/ or exp Parents/ or exp Parenting
Skills/ or exp Family Relations/ or exp Parenting/ or exp Parent Child Relations/) AND (exp Parent Training/ or exp clinical
PSYCINFO
trials/ or exp Family Intervention/ or exp Intervention/) AND (exp Alcohols/ OR exp Drugs/ or drug.mp OR exp Tobacco Smoking/
OR smoking.mp OR tobacco.mp)
Data Extraction and Risk of Bias recommendations,12 if insufficient ethnicity that comprised >75%
Assessments information was presented to permit of the participants or as diverse
judgment, the risk was scored as populations if no one race/ethnicity
All manuscripts were grouped by “unclear.” To confirm unclear scores, comprised >75% of the participants.
study and assigned a study number. study protocols were searched,
Trained researchers (D.G.H., D.C., and and authors were contacted asking Data Synthesis
J.M.) extracted data from each article additional information on each We used harvest plots to graphically
using a standardized, prepiloted source of bias. Two independent synthesize the findings for the study
form. For studies with multiple arms, coders (D.G.H. and J.M.) reviewed aims.10 In these plots, each study
data were only extracted for the arms each article, study protocol, and or study arm for those evaluating
that had a parent focus. Extracted authors’ response to determine multiple interventions is represented
outcomes were adolescent smoking, the risk of bias of each study. by a bar, and the properties of the bar
alcohol, other illicit substance, and Disagreement between coders was represent features of the study. The
polysubstance intention to use; resolved by consensus. height presents the study risk of bias;
initiation of use; and use. Results
Intervention characteristics extracted taller bars represent studies with
were documented as either reduced,
included “targeted participants,” fewer sources of bias. Because some
no change, or increased when
classified as parents only, parents studies did not achieve low risk of
compared with control groups at the
and youth, and multilevel (targeted bias on any criteria and thus received
P < .05 level of significance. Time to
teachers, medical providers, or a count of zero, the heights on the
follow-up for all reported outcomes
others). “Intervention dosage” harvest plots represent the raw
were grouped by time from baseline
was calculated as the amount of counts plus 1. The location within a
as ≤12 months, 12.1 to 24 months,
time parents were intended to column represents the study results
24.1 to 48 months, and >48 months.
participate in the intervention classified as detrimental effect, no
If 2 time points fell within a grouping,
and was classified into low (≤12 difference, or positive effect using
the longest time point presented was
parent-hours), moderate (12.1–24 an α of .05. The bar’s color or fill and
presented.
parent-hours), and high (>24 location within a row represent the
Risk of bias was evaluated using the parent-hours). “Delivery setting” analyses of interest.
Cochrane Risk of Bias Assessment was defined as the primary location For the first aim, to assess the efficacy
Tool, a widely used and validated of intervention, classified as home, of the parenting interventions (see
tool.11 Sources of study bias assessed school, community agency, or Fig 2), we included all adolescent
were a) random sequence generation, combination. The primary “method smoking, alcohol, and illicit substance
b) allocation concealment, c) blinding of intervention delivery” was use outcomes for all reported time
of study personnel and outcome categorized as in-person, typically points within each study. The bar
assessment, d) incomplete outcome group sessions with a professional; color indicates whether substance
data, and e) selective outcome workbook based; computer based; or use (black), substance use initiation
reporting. Risk of bias was judged a combination. Additional extracted (gray), or substance use intention
as low, high, or unclear. A summary data included youth age described as (white) was reported in the study.
with the criteria for low risk of bias in a range in years or grade level and When >1 outcome was reported for a
each of the domains is presented as sex as percent female. Participant substance, we presented 1 outcome
a footnote in the Supplemental Table race/ethnicity was classified as based on the following hierarchy:
3. As per Cochrane systematic review reported by authors or by the race/ use, initiation, and intention. The
Downloaded from www.aappublications.org/news by guest on July 13, 2021
PEDIATRICS Volume 138, number 2, August 2016 3bar’s location within rows represent
the follow-up times that the
study reported. The 4 studies
reporting only polysubstance use
outcomes are not included in the
harvest plots.
For the second aim, to determine
the interventions’ characteristics
associated with efficacy (see Figs
3–5), harvest plots synthesize dose
intensity, delivery setting, and
delivery method for each substance.
Only studies reporting these
characteristics were included in the
plots. In these harvest plots, the bar
pattern indicates the longest time
point of follow-up for each study;
white = ≤12 months, dotted = 12.1 to
24 months, horizontal stripes =
24.1 to 48 months, black = >48
months. The bar’s location within
rows represents the characteristic
of the intervention in each study.
Participant types (eg, parents vs
parents and youth) were
not presented in harvest plots
because of a lack of variability.
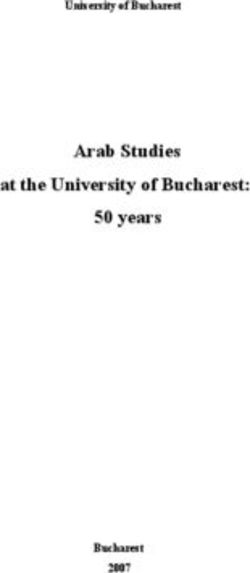
Because comparing counts between FIGURE 1
the number of studies with positive Study flow diagram. From Moher D, Liberati A, Tetzlaff J, Altman DG; The PRISMA Group. Preferred
Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann Intern Med.
and null results based on the study’s
2009;151(4):264–269.
P value for the difference between
intervention and control groups
effective outcomes is greater than not a target of the intervention (n =
might be misleading,13 we conducted
what would have been found by 2), (2) the study targeted a population
a binomial test of proportions for
chance.13 Using this same formula, with a specific medical problem (n =
each outcome of interest, using the
we calculated the number of studies 2), (3) youth substance use outcomes
following formula:
that would need to be null to change were not reported (n = 3), or (4) study
X score = [H - Kp / Kp(1-p) 1/2], the conclusions of the review in any did not meet methodological inclusion
given category. criteria (n = 4).
where H is the number of positive
studies, K is the number of total The final 66 manuscripts included
studies with the characteristic of RESULTS in the review represented 42
interest, and p is the criterion for unique studies (Table 2); 6 of
positivity by a 2-sided test (0.05 / Of the 1883 studies identified, 1721 these studies included multiple
2 = 0.025).13 P values were calculated unique articles were screened (Fig parent-focused arms. Studies and
from a normal distribution. We 1). A total of 1644 articles were associated citations will hereafter
defined a “positive” study as one excluded, largely because they did not be referred to by the study number
reporting results with P values ≤.05 evaluate family skills interventions, in Table 2 with letter subscripts
or lower; under the null hypothesis, did not focus on substance use, or indicating arms for multiarmed
1 in 20 studies would be expected were not randomized controlled studies (eg, 9[a], 9[b]). Some
to meet this criterion. A significant trials. The remaining 77 articles were manuscripts reported combined
Xscore suggests that there is sufficient screened in full, and 11 additional data from multiple studies and
evidence to conclude that the articles (representing 7 studies) were are therefore presented in Table 2
proportion of studies showing excluded because (1) parents were multiple times.
Downloaded from www.aappublications.org/news by guest on July 13, 2021
4 ALLEN et alTABLE 2 Summary of Studies Using Parent-Focused Interventions to Reduce Youth Substance Use
Number Low Risk of Bias
Study ID Authors Youth Demographics Intervention Description Control Description Outcomes Measured Resultsa (P < .05) Criteriab
1 Bauman et al N = 1326; Female NA; Race 4 booklets + 4 follow-up calls No intervention Smoking initiation; 12 mo: no difference smoking 1
(2001)14 NA; 12–14 y (parent) alcohol use and use or alcohol use
initiation
2 Brody et al N = 332; 53.6% Female; 7 sessions (youth + parents) 3 leaflets Alcohol use and 3 mo: reduced alcohol initiation/ 3
(2006)15 African American; 11–13.5 intention use; 29 mo: reduced alcohol
y initiation/use
3 Brody et al N = 667; Female (NA); African 5 sessions (youth + parents) 3 leaflets Alcohol use and 29 mo: reduced alcohol use; 65 2
(2010)16 American; 10.8 y initiation mo: reduced alcohol use
4 Brody et al N = 502; 51% Female; African 5 sessions (youth + parents) 5 sessions on nutrition Smoking, alcohol, 22 mo: reduced polysubstance 1
(2012)17 American; Age 16 y (10th (youth + parents) substance and use
PEDIATRICS Volume 138, number 2, August 2016
grade) polysubstance use
5 Connell et al N = 998; 47.3% Female; 6 sessions (youth) + 3 family No intervention Smoking, alcohol, 72 mo: reduced smoking use, 4
(2006,18 2007)19 Diverse population; checkups + elective family substance alcohol use, and substance
11–17 y intervention (youth + use
parents)
6 Curry et al N = 4026; 52% Female; 1 handbook + 2 counseling Standard care Smoking intention 6 mo: no difference smoking 1
(2003)20 Primarily white; 10–12 y calls + 1 newsletter (parent) and use intention, or use; 12 mo: no
difference smoking intention,
or use; 20 mo: no difference
smoking intention, or use
7 DeGarmo et al N = 361; 51% Female; 6 sessions (youth + parent) No intervention Smoking, alcohol, and 60 mo: reduced smoking 4
(2009)21 European American; + recess games (youth + substance use and and alcohol initiation, no
5th–12th grade teacher) + 7 phone calls initiation difference substance initiation
(parent) + newsletters
(teacher + parent)
8 Dembo et al N = 315; 44% Female; Diverse 30 home visits (youth + parent) Phone contacts with Alcohol use 36 mo: no difference alcohol use 1
(2002)22 population; 14.5 y staff and referrals if
necessary
9(a) Dishion & N = 65; 47.5% Female; 90% 12 sessions + 6 newsletter No intervention Smoking and 4 mo: no change smoking use; 16 1
Andrews Caucasian; 10–14 y (parents) substance use mo: no change smoking use
(1995)23
9(b) Dishion & N = 70; 47.5% Female; 90% 12 sessions + 6 newsletter No intervention Smoking and 4 mo: increased smoking use; 16 1
Andrews Caucasian; 10–14 y (youth + parents) substance use mo: increased smoking use
Downloaded from www.aappublications.org/news by guest on July 13, 2021
(1995)23
10 Fang L, et al N = 108; 100% Female; Asian 9 online sessions (youth + No treatment Smoking and alcohol 6.25 mo: no difference smoking 4
(2010)24 American; 10–14 y parent) use; substance use use, reduced alcohol
and intention use, substance use, and
polysubstance intention
11 Forman SG et al N = 279; Female (NA); White; 10 youth sessions + 1 booster 10 sessions + 2 booster Smoking, alcohol and 12 mo: no difference smoking 2
(1990)25 14.72 y + 5 parent sessions (youth on peer support, substance use use or alcohol use, reduced
+ parent) increase substance substance use
knowledge (youth
only)
56
TABLE 2 Continued
Number Low Risk of Bias
Study ID Authors Youth Demographics Intervention Description Control Description Outcomes Measured Resultsa (P < .05) Criteriab
12 Gonzales et al N = 516; 50.8% Female; 9 sessions + 2 home visits 1 workshop on school Smoking, alcohol, 12 mo: reduced polysubstance 4
(2012)26 Mexican American; 12.3 y (youth + parent) resources/ school substance and use
success (youth + polysubstance use
parent)
13 Guilamo-Ramos N = 1386; 50.4% Female; 2 youth sessions + 2 parent 2 youth sessions + Smoking use 15 mo: reduced smoking use 4
et al (2010)27 Diverse population; 12.1 y sessions + 2 booster calls parent class on high
(youth + parent) school selection
14(a) Haggerty et al N = 213; 48.7% Female; 50.8% Intervention 1: self- No treatment Smoking initiation; 24 mo: no change in tobacco, 1
(2007)28 Caucasian, 49.2% African administered video + alcohol, substance alcohol, substance or poly
American; 13.7 y (8th workbook program (parent) and polysubstance substance initiation
grade) use and initiation
14(b) Haggerty et al N = 224; 48.7% Female; Intervention 2: 7 Group video + No treatment Smoking initiation; 24 mo: no change in tobacco, 1
(2007)28 50.8%; Caucasian, 49.2% workbook sessions (youth alcohol, substance alcohol, substance or
African American; 13.7 y + parent) and polysubstance polysubstance initiation
(8th grade) use and initiation
15 Komro et al N = 5812; 50% Female; Youth: 25 sessions + 9.5 peer Standard care Alcohol intention; 36 mo: no difference alcohol 2
(2006,29 2008)30 Diverse population; 11.8 y leaderships training + alcohol and intention, alcohol or
(6th grade) community service project. polysubstance use polysubstance use
Youth + parent: 12 at
home booklets+ 2 family
fun events + 13 parent
postcards (youth + parent)
16(a) Koning (2009,31 N = 1736; 49% Female; Dutch; Intervention 1: 1 presentation No intervention Alcohol use 10 mo: no difference alcohol use; 3
2011,32 2013)33 12.6 y + 1 parent consensus 22 mo: no difference alcohol
meeting for rule making + 1 use; 34 mo: no difference
information leaflet (parent) alcohol use; 50 mo: no
difference alcohol use
16(b) Koning (2009,31 N = 1747; 49% Female; Dutch; Intervention 2: 1 presentation No intervention Alcohol use 10 mo: reduced alcohol use; 22 3
2011,32 2013)33 12.6 y + 1 parent consensus mo: reduced alcohol use; 34
meeting for rule making + 1 mo: reduced alcohol use; 50
information leaflet (parent) mo: reduced alcohol use
+ 4 lessons + 1 booster
session (youth)
Downloaded from www.aappublications.org/news by guest on July 13, 2021
17 Loveland-Cherry N = 892; 54% Female; 3 home sessions + phone calls No intervention Alcohol use and 60 mo: reduced alcohol use 1
et al (1999)34 European American; 9 y + newsletter initiation
(4th grade)
18 Martinez et al N = 73; 44% Female; Latino; 12 sessions + 12 notebook No project-related Smoking, alcohol 5.61 mo: reduced smoking 1
(2005)35 12.74 y (middle school) exercises (parent) intervention and substance intention, marginally reduced
intention substance intention, no
difference alcohol intention
19 Milburn et al N = 151; 66.2% Female; 5 sessions (youth + parent) Standard care Alcohol, substance 12 mo: reduced alcohol use, 3
(2012)36 Diverse population; 14.8 y and polysubstance increased marijuana use,
use reduced hard substance use
ALLEN et alTABLE 2 Continued
Number Low Risk of Bias
Study ID Authors Youth Demographics Intervention Description Control Description Outcomes Measured Resultsa (P < .05) Criteriab
20(a) O’Donnell et al N = 268; 100% Female; Intervention 1: 4 audio CDs No materials Alcohol use 12 mo: reduced alcohol use 1
(2010)37 Diverse population; (youth + parent)
11–13 y
20(b) O’Donnell et al N = 268; 100% Female; Intervention 2: 4 booklets No materials Alcohol use 12 mo: no change in alcohol use 1
(2010)37 Diverse population; (youth + parent)
11–13 y
21 Pantin et al N = 213; 36% Female; 9 group sessions +10 family 3 individual and Smoking, alcohol, 30 mo: reduced polysubstance 3
(2009)38 Hispanic; 13.8 y (8th visits + 4 booster sessions family referrals to substance and use
grade) (youth + parent) agencies that serve polysubstance use
delinquent youth
PEDIATRICS Volume 138, number 2, August 2016
22 Perry et al N = 2351; 48.7% Female; 94% Project Northland: classroom Standard care Smoking, alcohol,8
TABLE 2 Continued
Number Low Risk of Bias
Study ID Authors Youth Demographics Intervention Description Control Description Outcomes Measured Resultsa (P < .05) Criteriab
26 Schinke et al N = 325; 51.4% Female; 10 online sessions (youth) + 1 No intervention Smoking, alcohol andTABLE 2 Continued
Number Low Risk of Bias
Study ID Authors Youth Demographics Intervention Description Control Description Outcomes Measured Resultsa (P < .05) Criteriab
33 Spoth et al N = 429; 52% Female; 99% Preparing for Drug Free Years 4 leaflets on adolescent Smoking, alcohol, 12 mo: no change in smoking, 3
(1999,54 Caucasian; 6th grade (PDFY): 4 sessions (parent) development substance and alcohol, substance or
2001,55 + 1 session (youth + parent) (parent) polysubstance use polysubstance initiation or
2004,56 and intention use; 24 mo: reduced smoking,
2006,57 alcohol, substance and
2006,58 polysubstance initiation/use;
2008)59, 48 mo: reduced, alcohol use,
Park et al marginally reduced smoking,
(2000)60, alcohol, substance initiation,
Mason et al no change in tobacco or
PEDIATRICS Volume 138, number 2, August 2016
(2003)61, Guyll substance use; 6 y: reduced
et al (2004)62 smoking initiation & use,
no change in alcohol or
substance initiation or use; 10
y: marginally reduced misuse
of prescription drugs
34 Spoth et al N = 446; 52% Female; 99% Intervention: Iowa 4 leaflets on adolescent Smoking, alcohol, 12 mo: Reduced alcohol initiation 3
(1999,54 Caucasian; 6th grade Strengthening Families development substance and no change in smoking,
1999,63 Program (ISFP): 7 sessions (parent) polysubstance use substance or polysubstance
2001,55 (youth + parent) and intention initiation or use or alcohol
2004,56 use; 24 mo: reduced smoking,
2006,57 alcohol, substance and
2006,58 polysubstance initiation and
2008,59 marginally reduced smoking,
2009,64 alcohol, substance and
2012)65, polysubstance use; 48 mo:
Guyll et al reduced smoking, alcohol,
(2004)62 substance and polysubstance
initiation, reduced tobacco
and alcohol use no change in
substance use; 6 y: reduced
smoking, alcohol, substance
and polysubstance initiation,
Downloaded from www.aappublications.org/news by guest on July 13, 2021
reduced alcohol, substance
and polysubstance use,
no change in tobacco use;
10 y: reduced misuse of
prescription drugs
910
TABLE 2 Continued
Number Low Risk of Bias
Study ID Authors Youth Demographics Intervention Description Control Description Outcomes Measured Resultsa (P < .05) Criteriab
35 Spoth et al N = 1664; 47% female; 7 sessions (youth + parent) 4 leaflets on adolescent Smoking, alcohol, 12 mo: no difference smoking 3
(2002,66 Caucasian; 7th grade development substance and initiation; reduced alcohol
2005,67 (parent) polysubstance initiation, substance initiation,
2008)68, use; alcohol and poly substance initiation;
Spoth et al and substance 2.5 y: reduced poly substance
(2006,57,58 initiation initiation; no change
2008)59 substance use; 5.5 y: reduced
describes smoking initiation/use,
2 studies alcohol initiation, substance
(including use, and poly substance
this 1) initiation/use; no change
alcohol use or substance
initiation
36 Spoth et al N = 11 931; 51% Female; 85% Year 1: Strengthening Families No project support Smoking, alcohol 12 mo: reduced substance 1
(2007,69 Caucasian; 6th grade at Program (10–14 y): 7 and substance initiation and use, reduced
2011,70 baseline sessions (youth + parent). use, initiation poly-substance initiation,
2013)71, Year 2: in-class lessons on and intention; marginally reduced tobacco
Redmond substance avoidance (youth) polysubstance use and initiation, no change
et al (2009)72 initiation and in alcohol use or initiation; 2
intention y: no difference polysubstance
intention; 4 y: reduced
smoking, alcohol, substance
and polysubstance initiation;
reduced substance use;
marginally reduced tobacco
use; no change in alcohol use;
6 y: reduced smoking and
substance use; no change in
alcohol use
37(a) Stanton et al N = 579; 58% Female; 100% Intervention 1: Intervention 1 + 8 youth sessions alone Smoking, alcohol and 24 mo: reduced smoking use; no 2
(2004)73 African American; 13–16 y 1 video (youth + parent) substance use change alcohol use; marginal
change in substance use
37(b) Stanton B, et al N = 559; 58% Female; 100% Intervention 2: Intervention 1 8 youth sessions alone Smoking, alcohol and 24 mo: reduced smoking use; no 2
Downloaded from www.aappublications.org/news by guest on July 13, 2021
(2004)73 African American; 13-16 + 4 booster sessions (youth substance use change alcohol use; marginal
+ parent) change in substance use
38 Stormshak, et al N = 593; 48.6% Female; 3 sessions (youth + parent) School as usual Smoking, alcohol and 24 mo: reduced smoking use, 4
(2011)74 Van Diverse population; 11.88 substance use reduced alcohol use, reduced
Ryzin, et al (6th grade) substance use; 36 mo:
(2012)75 reduced alcohol use
39 Werch, CE et al N = 211; 49.8% Female; 85% 1 consultation (youth)+ 1 letter Booklet on alcohol Alcohol use initiation 1 mo: no change alcohol use; 12 2
(1998)76 African American; 12.1 + 2-9 workbooks (youth + (youth) and intention mo: no change alcohol use
(6th grade) parent)
ALLEN et alNumber Low Risk of Bias
Studies varied in operationalization,
measurement of substance use
Criteriab
outcomes, which included tobacco,
alcohol, and illicit substance
intention to use, initiation, and
current use, as well as polysubstance
2
1
3
3
use. Twenty studies (48%) reported
3 substance use outcomes, 3 (7%)
6 y: no change in polysubstance
6 y: no change in polysubstance
2 y: reduced alcohol use; 3 y: no
intention, no change alcohol
reported 2 substance use outcomes,
Resultsa (P < .05)
15 (36%) reported 1 substance use
12 mo: reduced alcohol
change alcohol use
outcome, and 4 (9%) reported only
use or initiation
poly-substance use. Outcomes are
noted in Table 2 in the “Intervention
Description” column. Control
use
use
conditions were most often standard
care, leaflets, or no intervention. All
and polysubstance
and polysubstance
Outcomes Measured
but 2 studies were conducted in the
Alcohol use initiation
Alcohol, substance
Alcohol, substance
United States. Eleven studies (29%)
and intention
Alcohol use and
included a majority of participants of
intention
white/Caucasian/European origin,
use
use
11 studies (29%) focused on other
specific race/ethnic groups (5 on
African American, 1 on Asian, and 5
adjustment (parent)
adjustment (parent)
standard nationally
Control Description
Books on postdivorce
Books on postdivorce
on Latino youth), 16 (38%) included
Booklet on alcohol
(curriculum is
diverse youth populations, and 4 did
Control schools
in Croatia)
not report race/ethnicity.
(youth)
Risk of Bias
parent-child communication
individual sessions (parent)
individual sessions (parent)
Northland) (youth + parent)
Of the 42 included studies,
consultation (youth) + 10
Intervention Description
1 consultation + 1 follow-up
and peer communication
Intervention 1: 11 group + 2
Intervention 2: 11 group + 2
postcards +4 workbooks
approximately half described how
Intervention encourages
the randomization sequences
+ 11 youth sessions
(based on Project
(youth + parent)
were generated (n = 22, 52.4%),
approximately a third described
how these were concealed (n = 13,
31.0%), and few reported blinding
outcome evaluators (n = 9, 21.4%).
Many had high attrition rates and
N = 650; 46% female; Diverse
Primarily Caucasian; 10.8
Primarily Caucasian; 10.8
were selective in the outcomes
Croatian; 6th–8th grade
Youth Demographics
that were reported in published
population; 11.4 (6th
N = 1981; Female (NA);
N = 159; 51.8% female;
b Number of Cochran Criteria indicating low risk of bias from 0 to 5.
N = 157; 49% Female;
a Reduction, no difference, or increase in substance use outcome.
manuscripts (n = 16, 38.1% for both
domains). Summary counts of the
y at baseline
at baseline
risk of bias assessment is presented
grade)
in Table 2 in the “Number of Low
Risk of Bias Criteria” column and
ranged from 0 (higher risk of bias,
West et al (2008)78
1 study) to 4 (lower risk of bias, 7
Authors
studies) with an average number of
Wolchik et al
Wolchik et al
Werch et al
(2003)77
(2002)79
(2002)79
low risk of bias criteria of 2.3 ± 1.1
of a maximum score of 5. Because all
TABLE 2 Continued
of the included studies had at least
NA, not available.
1 feature that either was unclear or
posed high risk of bias to the study
42(b)
42(a)
40
41
Study ID
findings (see Supplemental Table 3
for scoring on each criteria for each
Downloaded from www.aappublications.org/news by guest on July 13, 2021
PEDIATRICS Volume 138, number 2, August 2016 11FIGURE 2
Tobacco, alcohol, and illicit substance use, initiation, and intention outcomes according to length of participant follow-up. Black, substance use; gray,
substance use initiation; white, substance use intention. Taller columns represent studies with lower risk of bias. Numbers indicate study ID. Xscore,
number of studies needed to be null (NNN).
study), the overall risk of bias of this what would be expected by chance. earlier time periods. The Xscores were
systematic review is high, suggesting However, the number of studies that significant at all time points. In this
results must be interpreted with would need to be null to change this case, the number of studies needed
caution.11 conclusion was much lower at the to be null to change this conclusion
48 months27 reported
so are presented in Table 2 but not other illicit substance outcomes
no significant intervention effect at
in harvest plots. Of these, 3 were (Fig 2, column 3), primarily use.
earlier time periods reinforces this
effective at outcome end points The Xscores were again significant at
trend. There was variation in the
ranging from 12 to 30 months.4,12,80 all time points. Similar to alcohol,
risk of bias in studies but no pattern
the number of studies needed to be
For smoking, 26 unique studies indicting that studies with greater
null to change this conclusion was
assessed outcomes across the 4 risk of bias were either more or less
highest at the early time points.
time periods (Fig 2, column 1). effective than those with less risk of
Again, there was variability in risk of
The majority of studies reported bias.
bias across effective and ineffective
smoking as opposed to intent or
interventions.
initiation; after 12 months, all but Thirty-four studies reported alcohol
1 study81 reported smoking as the outcomes (Fig 2, column 2), primarily Across all 3 substances (Fig 2, all
outcome. The Xscores were significant use as opposed to intent or initiation. columns), few studies reported
at all time points, indicating that Effective studies at >24 months efficacy across multiple substance
the proportion of studies showing either did not report early outcomes use outcomes. Three studies
effective outcomes was greater than or also indicated effectiveness at indicated significant effects for
Downloaded from www.aappublications.org/news by guest on July 13, 2021
12 ALLEN et alFIGURE 3
Tobacco use at the longest follow-up time according to dose of intervention, setting, primary delivery method, and program duration. White columns, ≤12
months of follow-up; dotted columns, 12.1–24 months of follow-up; horizontal stripe columns, 24.1–48 months of follow-up; black, >48 months of follow-up.
Taller columns represent studies with lower risk of bias. Numbers indicate study ID. Xscore, number of studies needed to be null (NNN).
preventing or reducing use of 2 Only 1 of these reported significant or computer-based approaches
substances at 48 For the 26 studies reporting alcohol outcomes, 65% reported
months.7,18 In terms of preventing all smoking outcomes, 69% reported the intervention dosage, 85%
3 substances, 1 study showed efficacy information that allowed calculating reported delivery setting, and 94%
at 48 months.
reported delivery method (Fig 3). 1), the majority of effective studies
In terms of dosage, (Fig 3, column reportedFIGURE 4
Alcohol use at the longest follow-up time according to dose of intervention, setting, primary delivery method, and program duration. White columns, ≤12
months of follow-up; dotted columns, 12.1–24 months of follow-up; horizontal stripe columns, 24.1–48 months of follow-up; black columns, >48 months of
follow-up. Taller columns represent studies with lower risk of bias. Numbers indicate study ID. Xscore, number of studies needed to be null (NNN).
included ≤24 hours of training, interventions may generate a On the encouraging side, our
although Xscores were significant reduction on youth substance use findings indicate that relatively
for all dosages. There was a variety over the short and long term. low-intensity interventions with
of effective delivery settings for a dosage of a manageable ≥12
illicit substances (Fig 5, column 2); Despite the existence of multiple parent contact hours achieve
most occurred in schools or in a effective programs, prevention outcomes. Although the dosage is
combination of settings. The majority researchers have noted that uptake manageable, the delivery modality
of these studies used sessions with of evidence-based programming has may be problematic. The finding
a professional as their delivery been limited.81 Common challenges that group sessions were the most
method (Fig 5, column 3). Xscores were for translation of evidence-based common means for delivering
significant for all delivery methods interventions to nonresearch settings these interventions to parents
except for computer based. include intervention intensity, a and youth may pose barriers for
discrepancy between skills needed some community settings. When
to implement the interventions implemented well, in-person group
DISCUSSION and those available with current sessions may be powerful because
Results of this systematic review staff, and intervention relevance (to of social support and shared
indicate that parenting interventions population or setting).2 Maximal learning among the participants;
could be effective at preventing reach of interventions in this review however, high-quality sessions
and decreasing adolescent tobacco, would be achieved if evidence existed require dedicated staff with content
alcohol, and illicit substance use for a broad menu of minimally expertise, strong facilitation skills,
but that the substance of focus burdensome delivery modalities that and high-intensity training on
and delivery characteristics are could be easily accessed by families intervention implementation. The
important. The finding that Xscores across a variety of settings and costs and staff requirements may
were highly significant for all impact multiple outcomes, yet our be beyond the means of community
outcomes at all time periods supports results suggest a relatively limited set organizations, particularly those
the conclusion that parent-focused of options. in resource-limited settings where
Downloaded from www.aappublications.org/news by guest on July 13, 2021
14 ALLEN et alFIGURE 5
Illicit substance use at the longest follow-up time according to dose of intervention, setting, primary delivery method, and program duration. White
columns, ≤12 months of follow-up; dotted columns, 12.1–24 months of follow-up; horizontal stripes, 24.1–48 months of follow-up; black columns, >48
months of follow-up. Taller columns represent studies with lower risk of bias. Numbers indicate study ID. Xscore, number of studies needed to be null (NNN).
highest at-risk youth are often served Overall, many studies were delivered patient-centered health care homes.8
and reside. In this review, alcohol use in a combination of settings, largely This approach has shown positive
was unique among the substances schools and home. Few studies results with newborns86; more
in that multiple effective studies occurred in nonschool community research is needed to understand
used computer-based delivery agencies, such as health clinics. which delivery modalities are
modalities. The success of these There is evidence that parenting most appropriate for the clinic
interventions can be successfully environment and how policies and
interventions suggests that this may
implemented in health care clinical procedures can best sustain
be an effective and presumably less
settings, yet few studies have these effective programs with
costly approach to reaching a larger
made use of clinics as locations for adolescents.
group of parents of youth. An added
implementation of family-based
benefit of computer-based delivery Finally, given limited resources
substance use prevention.84,85 As
is that content may be tailored to a available for prevention
schools become overburdened with
particular family’s needs or cultural programming and competing
initiatives focusing on academic demands within delivery agencies,
preferences, increasing the likelihood
achievement, it is important to parent-focused interventions would
of relevance and effectiveness.83
consider clinics and community ideally effectively target multiple
In sum, although group sessions agencies as alternative settings to substance use outcomes; however,
represent the most common and promote, sustain, and fund parent few studies were effective at reducing
evidence-based delivery modality training programming. This is adolescent use of multiple substances
for tobacco and illicit substance use particularly true with the increased over the long term. Future research
prevention in particular, there is focus on “moving prevention to should investigate common core
need for additional studies using the mainstream of health,” clinical- principles, content, and delivery
alternative approaches, including community and public health modalities that contribute to study
social/online media, to develop a partnerships promoted through outcomes for a given substance use
broader set of options for translation the Affordable Care Act,82 and to enhance programming in a manner
of effective programs. integrated care within family- and that will increase the likelihood of
Downloaded from www.aappublications.org/news by guest on July 13, 2021
PEDIATRICS Volume 138, number 2, August 2016 15interventions being efficacious across of our review. In addition, because With the increased move to
substances. of the heterogeneity of intervention translate effective interventions
components, contexts, samples, into broad use and the call for
This study has notable strengths, methods, outcomes, and measures, collaboration between clinic
including use of broad inclusion we did not perform a meta-analysis and public health initiatives to
criteria to identify all relevant and instead used harvest plots to promote disease-preventing
intervention studies, but given summarize the study findings and programming, there is need to
that the majority of studies had explore the effects of intervention identify effective interventions that
risk of bias based on available delivery methods on tobacco, prevent adolescent substance use
data, the overall conclusions must alcohol, and substance use outcomes. across multiple delivery modalities
be interpreted with caution.11 Although this approach does not and settings, including clinics.
Conclusions were limited by the provide effect estimate summaries as Parent training interventions are
degree to which authors adhered in meta-analyses, it is an alternative an effective means to promote
to the CONSORT (Consolidated that visually represents different public health goals for adolescents,
Standards of Reporting Trials) aspects of intervention complexity.80 and an opportunity remains to
guidelines for behavioral In addition, using the binomial test extrapolate what works to varied
interventions when reporting study of proportions to complement the community settings in a manner that
design and findings, particularly harvest plots allowed us to estimate prevents adolescent use of multiple
in the areas of randomization probabilities of observing the substances.
sequence generation and blinding of presented patterns of results, which
data collection processes.87 Better produced quantitative evidence ACKNOWLEDGMENTS
reporting of risk of bias outcomes supporting the qualitative summary. The authors acknowledge the
within articles would potentially The high number of studies needed to substantial contribution of Nicole
have increased the strength of our be null to change study conclusions Hassig in formatting the harvest
recommendations but not the results support the findings of our review. plots.
to data extraction and reviewed and revised drafts of the manuscript; Dr Borowsky contributed to conceptualization of the study and reviewed and revised drafts
of the manuscript; and all authors approved the final manuscript as submitted.
This trial has been registered at the PROSPERO systematic review registry (identifier CRD42014013069).
DOI: 10.1542/peds.2015-4425
Accepted for publication May 11, 2016
Address correspondence to Michele Allen, MD, MS, University of Minnesota Department of Family Medicine and Community Health, Program in Health Disparities
Research, 717 Delaware St SE, Minneapolis, MN 55414. E-mail: miallen@umn.edu
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2016 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Dr Garcia-Huidobro was supported by National Research Service Award in Primary Medical Care, grant. T32HP22239 (principal investigator: Dr
I Borowsky), Health Resources and Services Administration (HRSA), US Department of Health and Human Services (HHS). This information or content and
conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or
the US government. Funded by the National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Johnston LD, O’Malley PM, Miech Emotional, and Behavioral Disorders components associated
RA, Bachman JG, Schulenberg JE. Among Young People: Progress and with parent training program
Monitoring the Future national survey Possibilities. Washington, DC: The effectiveness. J Abnorm
results on drug use: 1975–2014: National Academies Press; 2009 Child Psychol. 2008;36(4):
Overview, key findings on adolescent 567–589
3. Kumpfer KL, Alvarado R. Family-
drug use. Ann Arbor, MI: Institute
strengthening approaches for the
for Social Research, University of 5. Petrie J, Bunn F, Byrne G. Parenting
prevention of youth problem behaviors.
Michigan; 2015 programmes for preventing tobacco,
Am Psychol. 2003;58(6–7):457–465
alcohol or drugs misuse in children
2. National Research Council and Institute 4. Kaminski JW, Valle LA, Filene JH,6. Thomas RE, Baker PRA, Thomas alcohol use. J Consult Clin Psychol. substance use. Psychol Addict Behav.
BC, Lorenzetti DL. Family-based 2010;78(2):281–285 1990;4(2):67–76
programmes for preventing smoking 26. Gonzales NA, Dumka LE, Millsap RE,
17. Brody GH, Chen YF, Kogan SM, et al.
by children and adolescents. Cochrane et al. Randomized trial of a broad
Family-centered program deters
Database Syst Rev. 2015;(2):CD004493 preventive intervention for Mexican
substance use, conduct problems,
7. Metzler CW, Sanders MR, Rusby and depressive symptoms in American adolescents. J Consult Clin
JC, Crowley RN. Using consumer black adolescents. Pediatrics. Psychol. 2012;80(1):1–16
preference information to increase 2012;129(1):108–115 27. Guilamo-Ramos V, Jaccard J, Dittus
the reach and impact of media-based P, Gonzalez B, Bouris A, Banspach
parenting interventions in a public 18. Connell AM, Dishion TJ. Deater-Deckard
K. Variable- and person-centered S; GuilamoRamos V. The Linking
health approach to parenting support. Lives health education program:
Behav Ther. 2012;43(2):257–270 approaches to the analysis of early
adolescent substance use: linking peer, a randomized clinical trial of a
8. Bultas MW, McMillin SE, Broom MA, family, and intervention effects with parent-based tobacco use prevention
Zand DH. Brief, rapid response, developmental trajectories. Merrill- program for African American and
parenting interventions within primary Palmer Q. 2006;52(3):421–448 Latino youths. Am J Public Health.
care settings. J Behav Health Serv Res. 2010;100(9):1641–1647
2015;(Aug):20 19. Connell AM, Dishion TJ, Yasui M,
28. Haggerty KP, Skinner ML, MacKenzie
Kavanagh K. An adaptive approach
9. Portnoy DB, Scott-Sheldon LA, Johnson EP, Catalano RF. A randomized trial
to family intervention: linking
BT, Carey MP. Computer-delivered of Parents Who Care: effects on key
engagement in family-centered
interventions for health promotion outcomes at 24-month follow-up. Prev
intervention to reductions in
and behavioral risk reduction: a Sci. 2007;8(4):249–260
adolescent problem behavior. J Consult
meta-analysis of 75 randomized 29. Komro KA, Perry CL, Veblen-Mortenson
Clin Psychol. 2007;75(4):568–579
controlled trials, 1988-2007. Prev Med. S, et al. Cross-cultural adaptation
2008;47(1):3–16 20. Curry SJ, Hollis J, Bush T, et al. A and evaluation of a home-based
10. Ogilvie D, Fayter D, Petticrew M, et randomized trial of a family-based program for alcohol use prevention
al. The harvest plot: a method for smoking prevention intervention in among urban youth: the “Slick Tracy
synthesising evidence about the managed care. Prev Med. 2003;37(6 Pt Home Team Program.” J Prim Prev.
differential effects of interventions. 1):617–626 2006;27(2):135–154
BMC Med Res Methodol. 2008;8:8 21. DeGarmo DS, Eddy JM, Reid JB, Fetrow 30. Komro KA, Perry CL, Veblen-
11. Higgins JP, Altman DG, Gøtzsche PC, RA. Evaluating mediators of the Mortenson S, et al. Outcomes from a
et al; Cochrane Bias Methods Group; impact of the Linking the Interests randomized controlled trial of a multi-
Cochrane Statistical Methods Group. of Families and Teachers (LIFT) component alcohol use preventive
The Cochrane Collaboration’s tool for multimodal preventive intervention intervention for urban youth: project
assessing risk of bias in randomised on substance use initiation and northland Chicago. Addiction.
trials. BMJ. 2011;343:d5928 growth across adolescence. Prev Sci. 2008;103(4):606–618
2009;10(3):208–220
12. Higgins JP, Green S, eds. Cochrane 31. Koning IM, Vollebergh WA, Smit
Handbook for Systematic Reviews 22. Dembo R, Wothke W, Livingston S, F, et al. Preventing heavy alcohol
of Interventions. Chichester, United Schmeidler J. The impact of a family use in adolescents (PAS): cluster
Kingdom: Wiley-Blackwell; 2008 empowerment intervention on juvenile randomized trial of a parent and
offender heavy drinking: a latent student intervention offered separately
13. Rothman KJ, Greenland S, Lash TL.
growth model analysis. Subst Use and simultaneously. Addiction.
Modern Epidemiology. Philadelphia, PA:
Misuse. 2002;37(11):1359–1390 2009;104(10):1669–1678
Lippincott Williams & Wilkins; 2008
23. Dishion TJAD, Andrews DW. 32. Koning IM, van den Eijnden RJ,
14. Bauman KE, Foshee VA, Ennett ST, et al.
Preventing escalation in problem Verdurmen JE, Engels RC, Vollebergh
The influence of a family program on
behaviors with high-risk young WA. Long-term effects of a parent and
adolescent tobacco and alcohol use.
adolescents: immediate and 1-year student intervention on alcohol use
Am J Public Health. 2001;91(4):604–610
outcomes. J Consult Clin Psychol. in adolescents: a cluster randomized
15. Brody GH, Murry VM, Kogan SM, et al. 1995;63(4):538–548 controlled trial. Am J Prev Med.
The Strong African American Families 2011;40(5):541–547
Program: a cluster-randomized 24. Fang L, Schinke SP, Cole KC. Preventing
33. Koning IM, van den Eijnden RJ,
prevention trial of long-term effects substance use among early Asian-
Verdurmen JE, Engels RC, Vollebergh
and a mediational model. J Consult American adolescent girls: initial
WA. A cluster randomized trial on
Clin Psychol. 2006;74(2):356–366 evaluation of a Web-based, mother-
the effects of a parent and student
daughter program. J Adolesc Health.
16. Brody GH, Chen YF, Kogan SM, Murry intervention on alcohol use in
2010;47(5):529–532
VM, Brown AC. Long-term effects adolescents four years after baseline;
of the strong African American 25. Forman SFJLMB. Effects of coping skills no evidence of catching-up behavior.
families program on youths’ training on adolescents at risk for Addict Behav. 2013;38(4):2032–2039
Downloaded from www.aappublications.org/news by guest on July 13, 2021
PEDIATRICS Volume 138, number 2, August 2016 1734. Loveland-Cherry CJ, Ross LT, Kaufman interaction effects by parental stress alcohol-positive adolescents treated in
SR. Effects of a home-based family and social support. Drug Alcohol an emergency department: results of a
intervention on adolescent alcohol Depend. 2012;125(suppl 1):S18–25 randomized clinical trial. Arch Pediatr
use and misuse. J Stud Alcohol Suppl. 44. Riesch SK, Brown RL, Anderson LS, Adolesc Med. 2011;165(3):269–274
1999;13:94–102 Wang K, Canty-Mitchell J, Johnson DL. 54. Spoth R, Lopez Reyes M, Redmond
35. Martinez CR Jr, Eddy JM. Effects of Strengthening families program (10- C, Shin C. Assessing a public
culturally adapted parent management 14): effects on the family environment. health approach to delay onset
training on Latino youth behavioral West J Nurs Res. 2012;34(3):340–376 and progression of adolescent
health outcomes. J Consult Clin 45. Schinke SP, Schwinn TM, Di Noia J, Cole substance use: latent transition and
Psychol. 2005;73(5):841–851 KC. Reducing the risks of alcohol use log-linear analyses of longitudinal
36. Milburn NG, Iribarren FJ, Rice E, et among urban youth: three-year effects family preventive intervention
al A family intervention to reduce of a computer-based intervention with outcomes. J Consult Clin Psychol.
sexual risk behavior, substance and without parent involvement. J Stud 1999;67(5):619–630
use, and delinquency among newly Alcohol . 2004;65(4):443–449
55. Spoth RL, Redmond C, Shin C.
homeless youth. J Adolesc Health. 46. Schinke SP, Schwinn TM, Fang L. Randomized trial of brief family
2012;50(4):358–364 Longitudinal outcomes of an alcohol interventions for general populations:
37. O’Donnell L, Myint-U A, Duran R, Stueve abuse prevention program for adolescent substance use outcomes 4
A. Especially for daughters: parent urban adolescents. J Adolesc Health. years following baseline. J Consult Clin
education to address alcohol and sex- 2010;46(5):451–457 Psychol. 2001;69(4):627–642
related risk taking among urban young 47. Schwinn TM, Schinke SP. Preventing 56. Spoth R, Redmond C, Shin C, Azevedo
adolescent girls. Health Promot Pract. alcohol use among late adolescent K. Brief family intervention effects
2010;11(suppl 3):70S–78S urban youth: 6-year results from a on adolescent substance initiation:
38. Pantin H, Prado G, Lopez B, et al. A computer-based intervention. J Stud school-level growth curve analyses 6
randomized controlled trial of Familias Alcohol. 2010;71(4):535–538 years following baseline. J Consult Clin
Unidas for Hispanic adolescents with 48. Schinke SP, Cole KCA, Fang L. Gender- Psychol. 2004;72(3):535–542
behavior problems. Psychosom Med. specific intervention to reduce
2009;71(9):987–995 57. Spoth R, Shin C, Guyll M, Redmond C,
underage drinking among early
Azevedo K. Universality of effects: an
39. Perry CLWC, Williams CL, Veblen- adolescent girls: A test of a computer-
examination of the comparability of
Mortenson S, et al. Project Northland: mediated, mother-daughter program. J
long-term family intervention effects
outcomes of a communitywide alcohol Stud Alcohol. 2009;70(1):70–77
on substance use across risk-related
use prevention program during early 49. Schinke SP, Fang L, Cole KC. Computer- subgroups. Prev Sci. 2006;7(2):209–224
adolescence. Am J Public Health. delivered, parent-involvement
1996;86(7):956–965 intervention to prevent substance use 58. Spoth RL, Clair S, Shin C, Redmond
among adolescent girls. Prev Med. C. Long-term effects of universal
40. Perry CLWC, Williams CL, Komro KA,
2009;49(5):429–435 preventive interventions on
et al. Project Northland: long-term
methamphetamine use among
outcomes of community action to 50. Schinke SP, Fang L, Cole KC. Preventing adolescents. Arch Pediatr Adolesc
reduce adolescent alcohol use. Health substance use among adolescent girls: Med. 2006;160(9):876–882
Educ Res. 2002;17(1):117–132 1-year outcomes of a computerized,
41. Williams CL, Perry CL, Farbakhsh mother-daughter program. Addict 59. Spoth R, Trudeau L, Shin C, Redmond
K, Veblen-Mortenson S. Project Behav. 2009;34(12):1060–1064 C. Long-term effects of universal
Northland: comprehensive alcohol preventive interventions on
51. Schinke SP, Fang L, Cole KC, Cohen-
use prevention for young adolescents, prescription drug misuse. Addiction.
Cutler S. Preventing substance
their parents, schools, peers and 2008;103(7):1160–1168
use among Black and Hispanic
communities. J Stud Alcohol Suppl. adolescent girls: results from a 60. Park J, Kosterman R, Hawkins JD, et al.
1999;13:112–124 computer-delivered, mother-daughter Effects of the “Preparing for the Drug
42. Prado G, Pantin H, Briones E, et intervention approach. Subst Use Free Years” curriculum on growth
al. A randomized controlled trial Misuse. 2011;46(1):35–45 in alcohol use and risk for alcohol
of a parent-centered intervention 52. Simons-Morton B, Haynie D, Saylor use in early adolescence. Prev Sci.
in preventing substance use and K, Crump AD, Chen R. The effects 2000;1(3):125–138
HIV risk behaviors in Hispanic of the going places program on 61. Mason WA, Kosterman R, Hawkins
adolescents. J Consult Clin Psychol. early adolescent substance use JD, Haggerty KP, Spoth RL. Reducing
2007;75(6):914–926 and antisocial behavior. Prev Sci. adolescents’ growth in substance
43. Prado G, Cordova D, Huang S, et al The 2005;6(3):187–197 use and delinquency: randomized
efficacy of Familias Unidas on drug 53. Spirito A, Sindelar-Manning H, Colby trial effects of a parent-training
and alcohol outcomes for Hispanic SM, et al. Individual and family prevention intervention. Prev Sci.
delinquent youth: main effects and motivational interventions for 2003;4(3):203–212
Downloaded from www.aappublications.org/news by guest on July 13, 2021
18 ALLEN et alYou can also read