Emergency Department Medical Officer's Orientation Manual - MEd from ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
SOUTH EASTERN SYDNEY ILLAWARRA AREA HEALTH SERVICE
SHOALHAVEN DISTRICT MEMORIAL HOSPITAL
Emergency
Department
Medical Officer’s
Orientation Manual
SECTION 1
Welcome and Orientation
Roles and Rostering
General department policies
Education
SECTION 2
Investigations
SECTION 3
Support Services
SECTION 4
Admission policies and procedures
Transfers and Retrievals
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin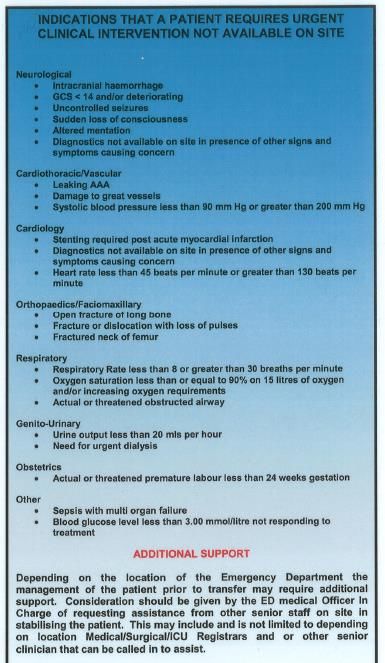
SECTION 1
WELCOME & ORIENTATION
Welcome to Shoalhaven Emergency Department!
Please feel free to ask for the in-charge MO or RN to give you an orientation
to the department on your arrival to your shift.
This manual is to guide you in the general workings of the department.
Much of the information may also be found on the Departmental Internet site –
“Med from the SHED”.
http://www.medfromtheshed.com.au/
This is accessible from any kiosk computer and may be found with the
following icon
MEd from the SHED
- MEd from the SHED (2).url
Please try to familiarise yourself with it as much as you can but don’t hesitate
to ask staff at any time if there are any questions.
The Department
Contact phone numbers -
Main Desk (Communications Clerk) - 0244239262
Triage Clerk 0244239365
Nurse in Charge 0244239312
NUM 0244239328
Director 0244239400
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin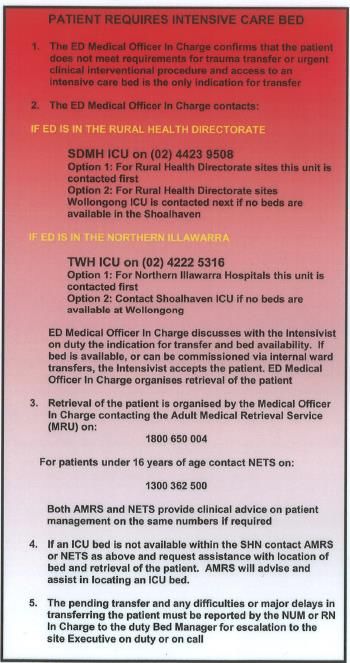
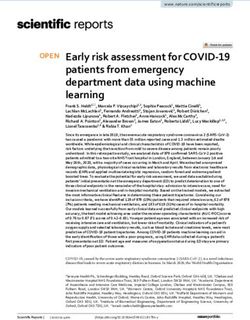
b) Dept map – amenities – tea room, toilet etc.
ED offices, Tea Room, Toilets and Lockers Resuscitation
Imaging
Acute Treatment Area (non-ED)
Tutorial
room and
Rapid MH office
Assessment
Zone (RAZ)
Triage and
Waiting room
ED Staff
Specialist
office
Fast Track Overcensus Unit (non-ED) Paediatric bay
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin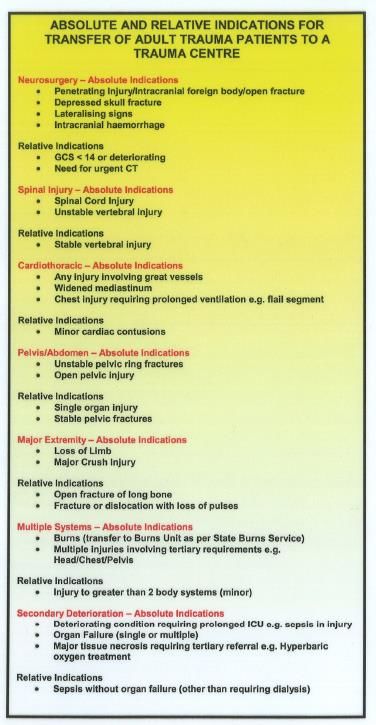
c) Who’s who?
Director Emergency Dept - Dr Simon Tucker
Simon.Tucker@health.nsw.gov.au
Director Emergency Medicine Training – Dr Peter Llewellin
Peter.Llewellin@health.nsw.gov.au
EMET Staff Specialist - Prof.Andrew Bezzina
AndrewJoseph.Bezzina@health.nsw.gov.au
Staff Specialist - Dr. Brona Geary
Brona.Geary@health.nsw.gov.au
Staff Specialist - Dr. Mark Newcombe
Mark.Newcombe@health.nsw.gov.au
Staff Specialist - Dr Richard Wheatley
Richard.Wheatley@health.nsw.gov.au
Staff Specialist - Dr Anne Smith
Anne.Smith3@health.nsw.gov.au
Staff Specialist - Dr Matthew Brandon
Matthew.Brandon@health.nsw.gov.au
Staff Specialist - Dr Michael Nitzberg
Michael.Nitzberg@health.nsw.gov.au
MMO – Dr. James Swinton
James.Swinton@health.nsw.gov.au
VMO – Dr. Glenn Browning
Glenn.Browning@health.nsw.gov.au
NUM - Ms. Wendy Fetchet
Wendy.Fetchet@health.nsw.gov.au
Clinical Nurse Educator – Ms. Sharyn Balzer
Sharyn.Balzer@health.nsw.gov.au
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin
Clerical Co ordinator – Ms. Lee Lloyd
Lee.Lloyd@health.nsw.gov.au
Executive Support/PA to Director – Ms. Tracey Garnam
Tracey.Garnam@health.nsw.gov.au
d) Who to see for…..
eMR access – ED Roster Co-ordinator 0436 948 874
will arrange access and four hours of training before commencement where
possible. If any problems refer to Lee Lloyd or in-charge RN.
Roster problems – ED Roster Co-ordinator (as above) in hours.
- After hours Nursing Manager on duty 44239738.
Medical Records
• All documentation is carried out within the electronic medical record.
• All pathology and imaging results can be accessed through the eMR.
• Be careful when accessing imaging results. If you wish to access all
results in order to compare previous images then you must open the
entire folder not just the image you are interested in.
Folder – leads to all results to date
Single Test result only – no old images
1.1 WORK PRACTICE STRUCTURE
This Emergency Department has some staff delineations you may not see
elsewhere.
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin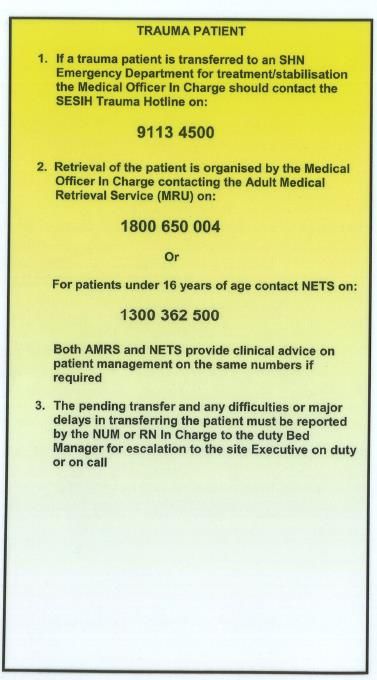
Advanced Clinical Nurses (ACN)
These nurses do not wear specific uniforms.
– They are accredited to apply standing orders and carry out procedures
such as cannulation of veins, blood gases, venepuncture, plasters etc.
This is done in conjunction with standing orders and does not remove the
imperative for the patients to be seen by a Medical Officer. This early
access to investigations is to aid you in your assessment of patients but
should never be ‘expected’ as standard management. You still need to
sign off the medications they administer OR if you are unhappy to do so
then notify the Lead Medical Officer on duty.
Nursing staff:
On every shift there is 1 triage nurse, 1 resuscitation nurse and 1 in-charge
nurse.
There is also a Nurse Practitioner on duty for the hours of 12.00 to 20.30 (5
days per week)
The Nurse In-charge is the person to discuss admissions with. If they are not
present at the main desk then they will be carrying a portable phone that you
can contact at any time through extension 9457
EDSO
(Emergency Department Support Officers) These non-clinical staff (wearing
red or green scrubs) are an important part of the structure and carry out tasks
such as courier work, patient transport, procedure set ups and patient meals.
There is 1 each shift. DECT 9572
Clerical Staff
Each day there are 2 staff morning and afternoon, one on at night. During the
morning and afternoon one staff will be based at the clinical desk to assist
with communication issues. All calls to outside consultants, pages for
registrars, chasing of old notes etc should where possible be made through
this clerk.
Medical Officers:
Medical staffing varies through the day commensurate with patient demand.
Handover Rounds – all medical staff required at 08:00, 17:00 and finally at
22:30. See below.
It is the responsibility of each doctor at the end of their shift to make sure that
their patients are medically handed over to the next doctor. Communication is
vital in the ED and handovers should be done professionally, concisely and
documented in eMR.
The senior doctors on day and evening shift will be indicated on the roster as
SMO1 and SMO2 and when available, SMO3
• SMO 1 has overall responsibility for the Acute area of the ED and takes calls
from GPs and the Community.
• SMO2 supervises the Fast Track area and has primary responsibility for the
resuscitation room when a SMO 3 role is not assigned. These roles will be
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin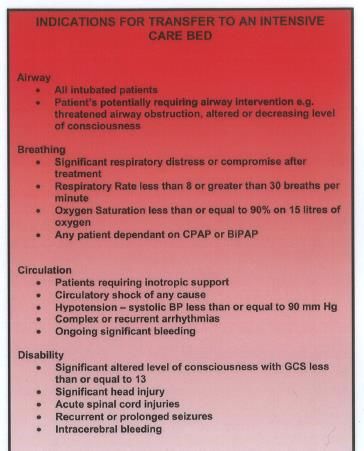
filled by a FACEM or a “multi skilled Medical Officer Level 3” (MMO 3) or
equivalent.
• SMO3 has the role of senior assessment and streaming, and functions
primarily in the RAZ area. This role is designed to facilitate rapid early
decision making with regard to investigation and treatment to help streamline
the patient journey through the ED. When assigned they will take the lead role
in the Resus room
1.2 Emergency Department Medical Officers Ward Duties out of Hours
10pm – 8am 7 days a week.
Out of hours there is limited MO cover on the wards. ICU and Medical
Registrar are available 24 hours. Surgical Registrar is on call after 10.30
pm.
PACE Tier 2 calls at any time must be attended by one of the ED MOs.
The SMO2 is the allocated person for that role. Team meetings are held
at 08:30 and 17:30 with the other PACE team members at which role
allocation will be agreed.
1.3 Ward Rounds and Clinical Handovers
• 0800 hours - Hand over from Night EDMOs to Day EDMOs (including
NUM and RN in-charge) at computer in main write up area OR
preferably using the computer on wheels at the bedside
• 1700 hours – NUM, Acute Area EDMOs, in-charge RN, NP and any
RN available, attend walk around ward round( may use computer on
wheels)
• 22:30 hours – Hand over from Day EDMOs to Night EDMOs (including
in-charge RN) at computer in main write up area or using the computer
on wheels at the bedside
• At the end of each shift- each clinician (medical and nursing) is
responsible for handing over care to the oncoming staff. Handover is to
include information per ISBAR guidelines(Introduction,
situation/diagnosis, background/history, assessment findings,
recommendation/plan)
• A handover tool as a laminated sheet is present with the computer on
wheels. (See Appendix 2)
1.4 Team Responses
The following are required responses within the ED. When these situations
are paged via the overhead speakers the required medical officers should
attend the indicated area immediately and remain until the Team Leader
releases them.
Category 2 Doctor – Each shift, an EDMO will be nominated as the ‘Cat 2’
medical officer. This will typically be an SRMO or Registrar grade MO, whose
role is to be the first responder for a category 2 patient being triaged into the
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellinacute treatment area. They will assume primary responsibility for the patient, but should liase closely with the SMO1 if they have a clinical concern regarding management. In the event of multiple category 2 patients being triaged in a short time period, it is expected that this caseload will be shared between the SMO1 and Cat 2 doctor Trauma Call Standby (9222) – for trauma presentations fitting trauma call ‘mechanism of injury’ ONLY then the following should attend ED in support - Cat 2 doctor (if triaged to Acute Area) or SMO2/3 (if triaged to Resus Room) - Surgical Registrar within 30 mins (+/or consultant) Trauma Call Attend Now (9222) – for trauma presentations fitting trauma call ‘mechanism of injury’ criteria AND either physiological or anatomical criteria as per the trauma call protocol, immediate attendance of the following - SMO 2/3 +/- Cat 2 doctor if required - Surgical registrar (+/- consultant) - ICU registrar (+/- consultant) - Anaesthetic registrar (+/- consultant) The ED SMO2/3 or night shift senior will be the team leader and should allocate tasks along traditional lines - ABC. If the Emergency Department senior doctor deems themselves inadequately skilled to function as team leader they may delegate that role to an attending consultant (surgery/ICU/Anaesthetics) if present. There is a trauma hotline for connection with the Trauma centre at St George Hospital - (02) 9113 4500. Note that patients bought to the ED by Ambulance Service NSW may already have a Retrieval team en-route as part of the state-wide Trauma Service network. Where a Retrieval team has been tasked, assessment and management should be aimed at providing treatment of immediate life threats only, and when appropriate, patients should be handed over for transport to SGH Trauma service (as most category 1 trauma patients are likely to have requirements that exceed the capabilities of Shoalhaven Hospital) Resuscitation team Response For non-trauma critical care responses e.g. cardiac arrest, unconscious patient, unstable arrhythmia the ED SMO2/3 is again the team leader and at least 2 ED Medical Officers (resource allowing) should attend to these cases initially. Of paramount importance- if you have an unwell patient with deteriorating vital signs then involve the senior MO and ICU early! 1.5 Rostering Medical Officers must comply with the roster provided. They must be punctual and available at all times during shift and must attend immediately when required by the Emergency Department nursing staff. If you intend to leave the department (even briefly to get lunch etc) you MUST let the other medical staff/in-charge RN know that you are going. Developed November 1993 - Current Revision 31 Jan 2020 Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin
NO ROSTER CHANGES ARE TO BE MADE without notifying the Medical
Director and completing the appropriate “Shift Swap” form (available via the
clerks). If swaps occur without notification and a “no show” occurs the person
originally on the roster will be held responsible for that shift.
1.6 Important Department Policies
1.6.1 Disposition decisions (Admit/ Transfer or Discharge must be
documented in eMR including times and conveyed to the In Charge
Nurse or Navigator.
1.6.2 No patient should be admitted to ANY ward without documentation,
and having been discussed with the admitting VMO/ staff specialist or
their registrar.
1.6.3 If there is a delay beyond 1 hour for a registrar to review a patient then
direct contact with the admitting MO should be made and the ward
transfer expedited.
1.6.4 Where conflict difficulties arise in relation to admissions under inpatient
teams then this should be escalated to the admitting SMO1 or SMO2
and the admitting VMO. Failure to achieve resolution at that point
requires escalation to the Director of Clinical Services in hours or to the
Executive on call out of hours.
1.6.5 Transfers to higher level care are arranged according to the ISLHD
Emergency Department Admission Process.
1.6.6 No patient should be transferred to ANY other hospital without
documentation(in eMR), discussion and acceptance with the registrar
or VMO for that specialty
1.6.7 All patients requiring significant alteration in management before
discharge (e.g. changes to usual medication) or follow up should be
discharged with a letter to the GP
1.6.8 If you perform investigations on a patient then arrange if possible for
copies of reports to go to the GP. The results can be incorporated in
the discharge letter in eMR or they can be printed off separately from
eMR results.
1.6.9 Emergency Department Medical Officers will check pathology/x-ray
reports and follow up as appropriate. Pathology results will be on eMR
and are best authorised as you check them on the day. MO’s are
responsible for the appropriate follow up of these results
1.6.10 Discharge requires that it be safe for the patient to go home.
Consideration of capacity for self-care, availability of supervision and
ease of access to review where appropriate should be considered.
Night time discharges are most prone to risk and between 12 am and 6
am should only occur provided the patient is capable and safe by these
criteria.
1.6.11 In NSW all pedestrians, bicycle riders, horse riders, motor bike riders or
drivers over the age of 14 who present as the result of a motor vehicle
accident on a public road within 12 hours require a blood alcohol by
law. This vial number must be documented in the notes. Failure to do
this will lead to fines to the MO
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin1.6.12 Transfers to Nowra Community Hospital for surgical procedures MUST
have a review by anaesthesia BEFORE confirming transfer. (The
private facility has no after-hours medical cover).
1.7 General Info
ID cards are required to access the hospital. Please see Lee Lloyd or the
clerks to obtain an access form. Security will process your ID card.
Lockers are available for use in the tea room; these all require a BYO
padlock. At the completion of the shift, these should be emptied and left
unlocked for others to use. The cafeteria is open from 8am to 2pm for meals.
The main entrance Coffee Cart has meals and coffee, hours are 8am to 2pm.
1.7 Education
From the commencement of the hospital year, the following education
activities will be available in the ED. All sessions will start promptly at 0830
unless otherwise specified
Wednesday A.M; SRMO/EM Registrar/EM diplomates; Sim session conducted
by Dr. Brona Geary and/or Dr. Rik Wheatley (Held in Resus 2 or SDMH Sim
Lab)
First Thursday of the month 0830hrs All EM clinicians/students; ED Mortality
and Morbidity Meeting conducted by Dr James Swinton (Held in ED tutorial
room)
Thursday A.M; All EM clinicians/students; General EM teaching conducted by
Dr Peter Llewellin or EM Registrar (Held in ED tutorial room)
Quarterly - Thursday AM 0830hrs – ED Education DAY – All EM
clinicians/students; conducted by Dr Andrew Bezzina and others. Programme
flyers distributed with the day course content in advance.
SECTION 2
2.1 Pathology Ordering
On the SEIAHS Intranet – under Clinical Services, there is an informative
Pathology Handbook. Please refer to this to guide you in tests and tubes
needed for specific conditions.
2.1.1 Request Forms
Pathology requests are made via eMR. Forms are however printed out and
must be sent with the samples. Group and crossmatch must have the form
signed by the collector.
Patient labels are found in the patient file.
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P LlewellinABG and VBG samples are labelled with patient bradma (sticky label) and
sent to pathology. No request form is necessary Please ring them on 9234 so
they can find the sample and process it.
2.1.2 Specimen Container Colours
TEST COLOUR OF TUBE TOP
Haematology - FBC PURPLE (small)
- Coags BLUE
Biochemistry BROWN
Blood Cultures OWN SEPARATE BOTTLES depending on
Paed or Adult
Cross-match PURPLE (large)
2.1.3 Laboratory Hours
• There is a Pathology staff member onsite 24 hours
• Almost all Blood Investigation are done on site except for
- Microbiology (Sent to TWH including microscopy)
- Serology (Sent to TWH)
• Group and Hold/Cross-match are done on site. Limited blood supplies
are available, please communicate as much as possible with pathology
when urgent blood is required.
2.1.4 Blood Transfusions
The policy of the NSW Health Department is that before any transfusion of
blood or blood product is commenced, two people should check the details of
the recipient’s identity, the blood pack and the cross-match at the bedside.
Consent forms for transfusion are now mandatory before a transfusion can be
started. Medial Officers are responsible for signing consent forms, so please
complete these when ordering blood for cross-match.
Note that the on-site blood bank does not carry platelets routinely and only
has a limited supply of Prothrombinex. Access to such products will require
discussion with the haematologist on duty at Wollongong.
2.2 Medical Imaging
At Shoalhaven Medical Imaging facilities include Plain film, CT and
Ultrasound but no onsite MRI or nuclear medicine capacity. There is no OPG
capacity.
There is a private MRI facility in Nowra, which can be used after consultation
with the Radiologist/VMO.
Nuclear medicine is available offsite
Non inpatient referral requires Specialist provider number.
2.2.1 Radiology
Radiology Staff are present in the hours
- 8am to 11pm Mon to Fri
- 8am to 7.30pm Sat-Sun
- Outside these hours staff are available on-call
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin2.2.2 Call backs All Medical Officers should consider the benefits of imaging before calling Radiographer. Please avoid call backs where management is not directly and acutely influenced by imaging and in any patient where delay will not endanger patient, e.g., undisplaced fracture of extremities. Confine all callbacks to those where you need imaging to carry on treatment. Developed November 1993 - Current Revision 31 Jan 2020 Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin
SECTION 3 SUPPORT SERVICES PHYSIOTHERAPY: There is a formal allocation of physiotherapy to the ED. 9561 physio practitioner 10 am to 6 pm weekdays. They will review patients in ED, assess mobility and review acute musculoskeletal injury. Please note that EDMO’s are expected to have made a basic assessment of mobility (i.e can the patient get out of bed or stand?) and attended to analgesia requirements PRIOR to calling for a physiotherapy assessment Arrangements can be made for follow up in the soft tissue injury clinic. Weekends hospital physio available 8am to 4.30pm via AHNM 9738 OCCUPATIONAL THERAPY Business hours 9716 SPEECH PATHOLOGY Business hours 9729 SOCIAL WORK Business hours 9224. After hours via AHNM 9738 DRUG AND ALCOHOL - 0421 616 637 ABORIGINAL SUPPORT OFFICER MS SHARON BLOXSOME 4428 7624 OR MOB 0423024278 AGED SERVICES IN EMERGENCY TEAM 7 days a week 0700-1530 there is an ASET clinician (on 9563), who will be available to assess patients over 70, from a discharge perspective. You can leave a message in their contact book for outpatient or inpatient assessment at a later date. MENTAL HEALTH Currently SDMH does not have an acute on-site admission service. There is an ED Mental Health CNC is available on site Mon to Fri 9413 or via the mobile phone 0402 892 504. Once called, the ED Mental Health CNC will evaluate patient and arrange transfer to Shellharbour Mental Health Unit. All Mental Health patients MUST have a medical assessment and this documented in their notes. After hours, the Shellharbour Hospital Psychiatry Registrar should be contacted by EDMO to arrange assessment and/or admission if they feel it is required. Discuss the admission with the ED in charge RN to arrange transport to an inpatient unit once admission is agreed upon. Developed November 1993 - Current Revision 31 Jan 2020 Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin
HOSPITAL IN THE HOME (COMMUNITY BASED IV CARE)
THERE IS A STRICT REFERRAL PROCESS.
1. RING THE HITH OFFICE 9362 OR MOBILE 0401 140 587
TO CHECK SERVICE AVAILABILITY.
2. RING DR PRATT 0405 313 185 AND HAND OVER PATIENT TO
TACT SERVICE. IF BUSY DR PRATT WILL ACCEPT MESSAGE ON
MOBILE PHONE.
3. COMPLETE REFERRAL FORM, OBTAIN CONSENT AND GIVE
INFORMATION SHEET TO PATIENT
4. LEAVE FILE AND MED CHART COMPLETED IN TACT BOX IN ED.
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P LlewellinSECTION 4
ADMISSIONS
4.1 Classification of Patients
Emergency Department Medical Officers should be aware of whether patient
is “chargeable” when contacting Admitting Medical Officer for admission.
Clerical staff should be contacted to clarify this and document this on the
patient file.
4.1.1 Insured (chargeable) patients have the right to select the doctor of their
choice (except where this is inappropriate for the condition). The Emergency
Department Medical Officer will contact the selected practitioner. If admission
to Nowra Community Hospital (NCH the local private hospital) is arranged,
copies of the admission documentation by Medical Officer accompanies
patient. There is also a separate drug chart to be written out .
4.1.2 Uninsured (non-chargeable) patients – Admission is under the Duty
Doctor of the day.
4.1.3 Veterans’ Affairs (Repatriation) – Vet Affairs are admitted to SDMH if a
bed is available, admitted under the doctor of their own choice (if available) or
may be transferred to NCH from Emergency Department. Emergency
Department in-charge RN is to advise Nursing Administration to arrange
approval with Vet Affairs.
4.2 Notifying Attending Medical Officer
Duty Roster – The first point of contact for admission is the registrar for the
admitting team. If they are not contactable or if they fail to attend within 2
hours then notify VMO/Staff Specialist according to duty doctor rosters for
SDMH and TWH kept in Emergency Department. If VMO/SS uncontactable
for any reason, contact Medical Administration.
Stroke unit admissions should be notified directly to the admitting consultant
and the patient transferred to the stroke unit expeditiously.
VMO/SS– Once the VMO/Staff Specialist has been informed of the admission
their admitting team is responsible for the ongoing management issues. In
hours, this team should be informed so they can attend to the patient that day.
Whilst the patient remains in the ED however the ED staff are responsible for
any acute medical issues arising.
4.3 Admission Policy
Documentation
All “admissions” must have documented:
- Date
- Reason for admission
- Relevant history
- List of medications
- Allergies
- Relevant and general physical examination
- Working diagnosis
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin- Plan of management and /or investigation:
- tests done and results needing to be checked
- tests to be ordered
- Instructions to nursing staff re diet, positioning, ambulation,
observations, etc
- Whether VMO, GP notified.
4.4 Non-urgent Admissions
Admissions direct to ward – when a VMO decides that a patient needs
admission and will be managing the patient in hospital, that doctor has the
responsibility of organising the admission.
Patient will be admitted directly to the ward if bed available when their
registrar is on duty.
GP admissions – Occasionally GPs will ring ED to discuss admission. These
patients should be seen in ED and admissions performed if appropriate. If
patient is not to be admitted the GP must be contacted personally.
4.5 ADMISSION PROCEDURES AND PARTICULAR SPECIALITIES
The SMO1 or SMO2 medical Officer should be notified of cases before
contact with inpatient teams is made.
Anaesthetist – Duty Anaesthetists are rostered on for 24 hours from 8am to
8am. Calls to the duty Anaesthetist from ED should be made by a Medical
Officer, personally wherever possible. Calls to the duty Anaesthetist should
not be initiated by non-medical staff except if directed by medical staff.
Nursing staff can provide experienced advice to the Medical Officer regarding
the contact with an anaesthetist.
Paediatrics – There is a paediatric referral policy available on Med from the
Shed that outlines referral criteria to the Paediatric team at SDMH. ED
medical officers should make themselves familiar with this document.
In brief however, all Category 1 children and all children meeting sepsis
criteria, and those in whom non-accidental injury is a concern should be an
automatic acute response call to the paediatric team.
Any febrile or otherwise unwell child under 3 mths of age, children whose vital
signs are persistently not ‘Between the Flags’, child who have re-presented to
the ED, and those in whom significant parental anxiety is being expressed
should have a low threshold for paediatric referral +/- admission.
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P LlewellinOrthopaedics – There are 3 orthopaedic surgeons with admitting rights to
SDMH and there are 2 other privately available Orthopaedic surgeons in the
Shoalhaven. Only Dr Jarman and the 2 privately available orthopaedic
surgeons have admitting rights Nowra Community Hospital (the local private
hospital).
All can be contacted regarding privately insured patients (at a reasonable
hour). Dr Jarman has admitting rights to Shoalhaven Hospital and has
allocated days on call as does Dr. Thornton-Bott and Dr Steele. See on-call
roster.
For patients not requiring admission or immediate advice but where they have
fractures or other orthopaedic issues requiring follow up there are several
possible pathways -
a) Privately insured patients – these should have initial care arranged
e.g. backslab etc and then advised to call and arrange appointment
at a private orthopods rooms (Dr. Jarman will accept these even if he
is not on call for a particular day). If a patient is given a referral to an
Orthopaedic VMO privately they should be informed that there would
be an upfront fee.
b) For public patients where follow up is felt necessary, the EDMO
contacts the orthopaedic registrar at Shoalhaven during reasonable
hours to confirm management and arrange fracture clinic follow up.
For overnight presentations, place pt. sticker in fracture clinic book at
staff station and/or notify orthopaedic registrar on the following
morning 0700 hrs, and they will arrange fracture clinic follow up of the
patient
c) If the patient has suffered a relatively minor injury e.g. undisplaced,
uncomplicated clavicular fracture, minor torus(buckle) fracture of
forearm, and the patient has a GP they can access, then they may be
referred to their GP for follow up.
All fractures requiring plaster immobilisation must initially be given POP Back
slab, appropriate analgesia and referral to LMO/ Physio/Orthopaedic surgeon
for application of full plaster.
Vascular Surgeon: There are no vascular surgeons at SDMH. Contact TWH
for Vascular Surgeon Registrar (business hours) or General Surgical
Registrar on –call (all other hours)
In the event of an emergency (e.g. ruptured AAA) the General Surgeon may
be contacted for advice
ENT –Available for rooms consults from ED only (Dr Serefli). Rooms consults
via referral. ENT Reg at TWH on call for more urgent cases.
Urology –
Patients presenting to the Emergency Department of Shoalhaven Emergency
Department with isolated urological problems will like other groups fall into
three broad categories: -
a) Simple problems that can be dealt with in the Emergency Department by
medical staff on site – e.g. urinary retention requiring insertion of indwelling
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellincatheter, haematuria without evidence of haemodynamic compromise or clot
retention.
b) Relatively simple problems that require admission but not urgent urological
intervention – e.g. ureteric colic with uncontrolled pain, haematuria with clot
retention requiring 3 way IDC and irrigation.
c) Seriously unwell patients requiring urgent surgical or procedural intervention
to avoid loss of life or appendage. e.g. obstructed kidney with urinary sepsis,
renal laceration, testicular torsion.
Disposition options –
Presuming appropriate resuscitation and stabilisation the disposition
options are –
Patient group a) will be simple and generally ambulatory and can be
discharged home for outpatient follow up.
Patient group b)
• 3 days per week and one weekend in three Dr. Spencer Murray
provides on call cover.
• Outside those hours discuss the case with the senior doctor in ED who
may decide to approach the surgical team at SDMH or contact the
urologist on duty at Wollongong.
Patient Group c) - These should be stabilised and resuscitated as
appropriate to their presentation. If Dr. Murray is on call for the day the
contact the surgical registrar at SDMH. Otherwise their early transfer to the
urology service at Wollongong should be arranged ASAP in tandem with
the resuscitation process. The exception is the case of testicular torsion
which can be managed by the local general surgeon on duty whose
registrar should be contacted ASAP and if any delay in that contact then
the consultant contacted directly.
4.6 Drug and Alcohol Dependent Persons presenting to SDMH
• Drug and alcohol dependent persons shall only be admitted for medical
or surgical complications that necessitate hospital admission.
• Drug and alcohol dependent persons will not be admitted for the sole
purpose of detoxification (exception – alcohol withdrawal with
significant risk of delirium tremens).
• Medical Practitioners may not prescribe a drug of addiction to a person
known or suspected by the prescriber to be an addict without the
written authority of the Department of Health, NSW. It is illegal under
Section 28 of the Poisons Act, 1966.
• If the patient is on Methadone, the Methadone unit or outside
Pharmacy should be contacted to obtain the dosage scheduling and
dosing.
• Medical Officers should consult with the Drug and Alcohol Services
where the patient is a known patient, to aid them in management.
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin4.7 Admissions to David Berry Hospital
Rehabilitation/Medical Unit
- Rehabilitation of patients requiring daily Allied Health support
(physiotherapy, occupational therapy and diet services). The
Rehabilitation Specialist has admitting rights to the hospital. He has a
Registrar and will accept and may also be called upon by the admitting
general practitioners on a consultative or “joint” admission basis.
4.8 Palliative Care Unit (Karinya) at David Berry Hospital, in Berry.
- Ring Karinya 4464 1950 and check bed availability
- A Palliative Care CNC is available for consultation.
- If bed available they will inform you who is the on-call AMO for Karinya.
They are contacted and care accepted.
- There is a palliative care folder regarding the details and requirements
for admission to the Palliative Care Service. Essentially their service is
for “end of life” care
4.9 Admissions to Intensive Care Unit, Shoalhaven Hospital
Major Criteria – any acute, life threatening, remediable condition where an
AMO/Staff Specialist considers admission necessary, e.g medium term
invasive ventilation.
High Dependency Criteria – conditions where it is considered that
management in the ICU will help reduce patient morbidity/mortality.
CCU Criteria- conditions where it is considered that cardiac monitoring would
be beneficial for the patient.
During the day, if you are expecting a patient to be admitted to ICU, please
contact the ICU registrar.
Generally patients admitted to the ICU will be adult although older children
can also be managed there. Neonates and infants requiring ICU are
transferred to Sydney.
Where ICU technology, e.g. monitoring equipment, is needed to care for
Paediatric patient, patient can be admitted to ICU and a Paediatric trained
registered nurse will accompany the patient and stay until retrieval. The
Paediatrician will be responsible for the care of the patient. ICU registered
nurses will provide expertise, e.g, setting up equipment.
4.10 Bed Availability in ICU
Because there is increasing pressure on ICU beds at SDMH, there may be
times when a patient requires intensive care/cardiac monitoring when the ICU
is full. In this situation the ICU registrar/ consultant should be advised. Please
see the retrieval/transfer section.
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P LlewellinAll admissions must be accompanied by at least a registered nurse. A doctor must accompany all intubated patients or those requiring ventilator assistance. All patients should be monitored in transit to ICU 4.11 RETRIEVAL AND TRANSFERS See appendix at end of document. 4.12 DEATHS IN THE ED All deaths in the ED, unexpected or expected should have a coroners checklist, death certificate, and cremation certificate completed by the attending MO If expected, the AMO/Staff Specialist should be informed at a convenient time. If unexpected, the AMO/Staff Specialist should be informed as soon as possible. If the patient is thought to be a coroner’s case please refer to 5.3 SECTION 5 5.1 Ambulance There are only a limited number of ambulance crews available in the Shoalhaven. The in-charge and triage RN will at times be involved in unloading patients promptly for the ambulance officers. The in-charge RN will liaise with the Bed Manager when ambulances can’t be unloaded. The ambulance will ring the in-charge RN portable phone in the event of a time critical patient (e.g. major trauma, cardiac arrest). These patients should be seen immediately they present by the most senior doctor available as a Category Resuscitation Call. 5.2 Deceased Persons DOA’s are not brought into the Emergency Department, but go straight to the Mortuary. They must be signed for in the Mortuary Book (by a member of hospital staff) and the body clearly labelled with a tag attached to the other sheet stating name and usual Local Medical Officer (if known) and date of death. All bodies must be sighted and pronounced dead before being placed in the refrigerated cabinet. If the body has not been seen by the GP, the Emergency Department Medical Officer or VMO on duty must sight the body. This can be done in the Ambulance or in the Mortuary. There is a form in the ED to use to declare life extinct. All DOA’s are then registered with the clerk in ED to be entered into eMR. Police are to be notified by the Medical Officer. Police then contact the Coroner regarding post mortem and liaise with Government Medical Officer or his deputy. If patient is not considered a Coroner’s Case then a death certificate must be issued: Options are to contact the attending GP; Registrar or AMO whose Developed November 1993 - Current Revision 31 Jan 2020 Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin
team has already reviewed the patient in ED; or if cause of death is clear then
EDMO can complete the Death Certificate. Please ask family if cremation is
preferred. You must complete a cremation certificate.
5.3 Criteria for Coroner’s Case
• If death was the result of an accident or injury
• If death sudden or unusual
• If patient had not seen a medical practitioner in the past three (3)
months
• These patients have a coroners checklist form filled out and a
certificate of life extinct completed, but NOT a death
certificate/cremation certificate.
5.4 Reports for Legal Purposes
Any request by Solicitors or Client for medico-legal reports relating to alleged
negligence are to be made through Medical Administration/medical records
Attending Emergency Medical Officers will provide statement to police on
those patients they have treated in ED that do not involve medical negligence,
eg, assault cases, accident victims, etc.
5.5 Child Protection Help Line (Previously DOCS)
CPHL notifications can be notified online via the ISLHD intranet homepage.
Urgent situations should involve the Paediatrics team and Social Worker
5.6 Sexual Assault Assessments
These cases are best managed by people who have the training to carry
out forensic assessments properly. The role of the Emergency Medical
Staff is to assess and manage associated trauma, injury. When this has
been completed or is not required they may then be referred to the Sexual
Assault Service. On call 24/7 via RN In-charge in ED. 44239211
5.7 Patients referred from Corrections Health
Background –
There are several background issues to be considered when dealing with
these patients.
a) They are patients like any other and our duty of care and requirements
for confidentiality remain the same.
b) They have NO Medicare Number. This is forfeit on their entry to jail.
The implication for them and us is that they cannot have any medical
interventions, imaging etc except in the context of a public facility. This
means they will come to us for apparently minor things like accessing a
plain X ray. (There is a plain film facility at the Jail but they have been
unable to recruit a radiographer).
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellinc) Prisoners are subject to frequent movements between facilities making
follow up arrangements for all but the more short term issues difficult to
ensure completion. The best option for conditions requiring follow up
longer than a few days is to arrange care via POW as irrespective of
which facility they are in they can be transferred there for review.
d) There is only a medical officer on site at the jail 2 days per week
(usually Tuesday and Wednesday). This means that follow through on
any plans of management, on referral etc .will be subject to potential
significant delay.
e) Policy prevents any dispensing of narcotic medications at the jail. As
such it is pointless referring back on oxycodone for pain. It will not be
given. The maximum medication possible is Panadeine Forte® bd (not
qid). This can be written on the discharge letter – no need for a script.
f) Despite a vigorous trade in drugs within the jail there is NO clean
needle program in action.
Implications for ED care –
Step 1 – See and manage the patient like you would any other.
• Maintain as much confidentiality as possible within the constraints of
having to have guards present.
• Do not discuss care with guards or use them as a pipeline for
communication with clinicians at the correctional facility.
• Furthermore do not be guided or pressured by guards with respect to
either care or disposition.
Step 2 – if the patient can be discharged then return to corrections facility with
a letter that has a clear plan of management that would cover the next 5 days.
• If strong analgesia is required that Panadeine Forte ® plus other
measures is unlikely to control then consider admission for analgesia
as narcotic analgesia will not be given at the facility.
• If an outpatient appointment is required for the follow up then where
possible make the arrangements for the follow up appointment prior to
transfer back to the correctional facility. Do not just put the suggestion
in the discharge letter and expect follow up to be arranged via the jail
unless the condition can tolerate long delays before review.
Step 3 – if the patient requires admission –
a) Short term problem manageable at SDMH with minimal follow up
required – e.g. abscess drainage – admit to SDMH or refer to TWH
like any other similar patient.
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellinb) Acute problem requiring admission but facility not available at
SDMH/TWH OR likely to require longer term follow up (more than a
few days to a week) – aim to admit to Prince of Wales Hospital.
c) Admissions to Prince of Wales MUST go via the ED with notification of
the Emergency Physician there.
d) Any uncertainty or problems ring the on call number for Corrections
Health to discuss with the Nurse Manager or with the on call medical
officer.
-Treat all prisoners as you would anyone else. Don’t bow to correctional
facility pressure to do what is convenient.
-There is an on-call nurse or doctor available to answer our questions 24/7.
Clinical Director or A/Cd use the paging system 9937 2506
AH Nurse Manager 93112707
ROAMS MO 130076267
The AH Nurse is a pivotal person who is across all matters clinical & will
assist in contacting the clinician as needed
Developed November 1993 - Current Revision 31 Jan 2020
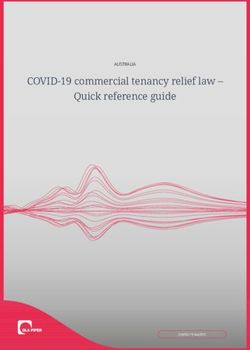
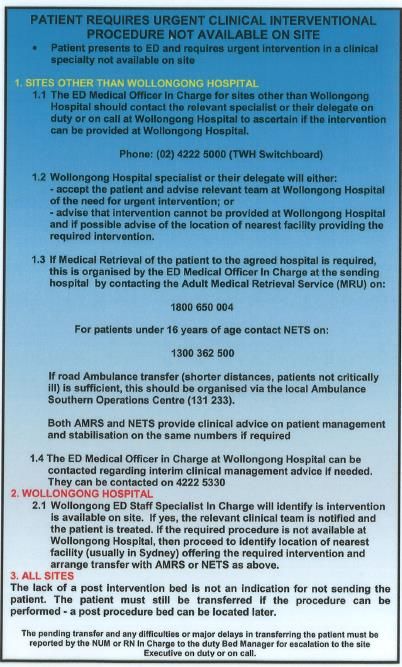
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P LlewellinAPPENDIX Retrieval process for Emergency Department. Developed November 1993 - Current Revision 31 Jan 2020 Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin
Developed November 1993 - Current Revision 31 Jan 2020 Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin
Developed November 1993 - Current Revision 31 Jan 2020 Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin
Developed November 1993 - Current Revision 31 Jan 2020 Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin
Developed November 1993 - Current Revision 31 Jan 2020 Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin
Developed November 1993 - Current Revision 31 Jan 2020 Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P Llewellin
Appendix 2
ED Handover
1. Patient Identity/Alerts
(Name/Age)
2. Situation –
Provisional Diagnosis /Background
(or presenting problem if early in work up)
3. Vital Signs Normal – Y/N?
4. Admitted – Y/N?
(Admitted means that the patient has been seen by the relevant
registrar and bed booking in the pipeline OR you have had the
relevant consultant directly accept the patient)
5. Outstanding issues –
Further resuscitation required?
Reg review
Path/Investigations pending
No idea where to go from here?
6. Processes Complete?
Admitted –
Med chart/Fluid chart/Documentation
Discharge likely-
Scripts/Letters to GP/ ASET review/ physio review/
pharmacy review/ Carers or Nursing Home aware as
appropriate.
Developed November 1993 - Current Revision 31 Jan 2020
Author – Dr. Andrew Bezzina, Staff Specialist, Emergency Medicine. Revised 2019, 2020 Dr P LlewellinYou can also read