Empirical in vitro fertilization for recurrent pregnancy loss
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Empirical in vitro fertilization for
recurrent pregnancy loss
Raoul Orvieto M.D. and Michal Kirshenbaum M.D.
- Department of Obstetrics and Gynecology,
Chaim Sheba Medical Center, Ramat Gan, Israel
- The Tarnesby-Tarnowski Chair for Family Planning and Fertility Regulation,
Sackler Faculty of Medicine, Tel-Aviv University, Israel.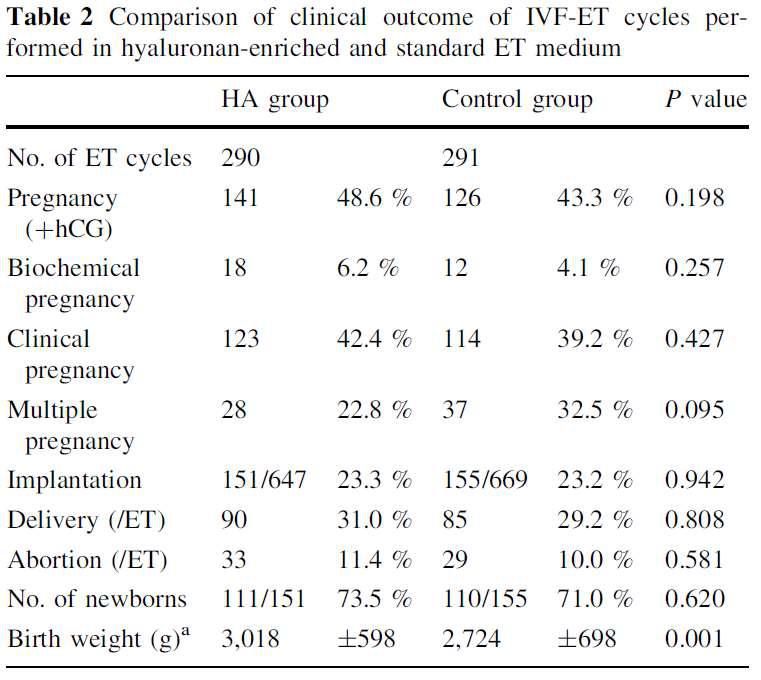
No relevant financial relationships
to disclose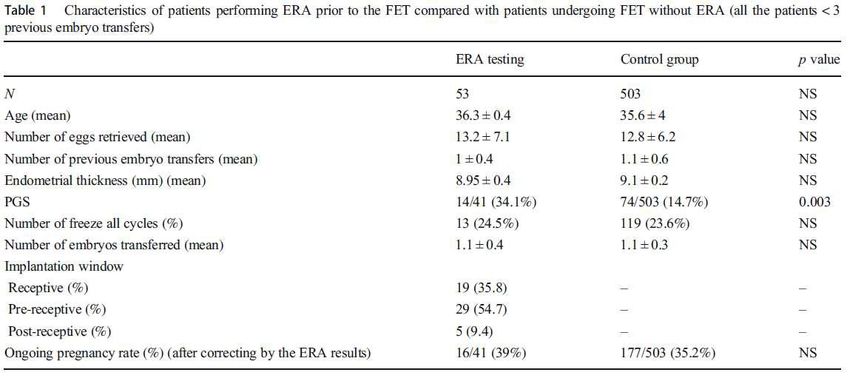
Recurrent pregnancy loss (RPL)
Non fertile- Infertility treatment including
assisted reproductive technique (ART)
Fertile- Empirical adjunct treatments or
‘add-ons’
Improving the chance of a live birth
Shortening the time to conception
Improving embryo quality
Improving implantation
Improving synchrony between endometrium &
embryo
3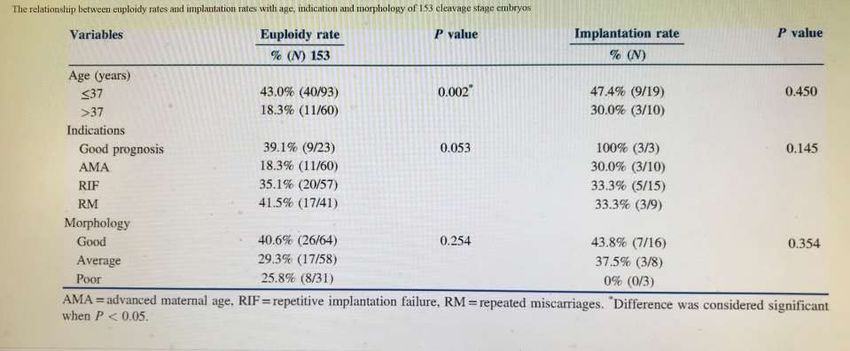
Improving the chance of a live birth Subsequent live birth rate is dependent on: # of previous live births Maternal age Genetic aberrations Whether the losses are early or late
Improving the chance of a live birth
Quoting success
RPL- Number of live births per pregnancy
IVF - Clinical pregnancy rate per cycle
- Live births per cycle
(2015)
5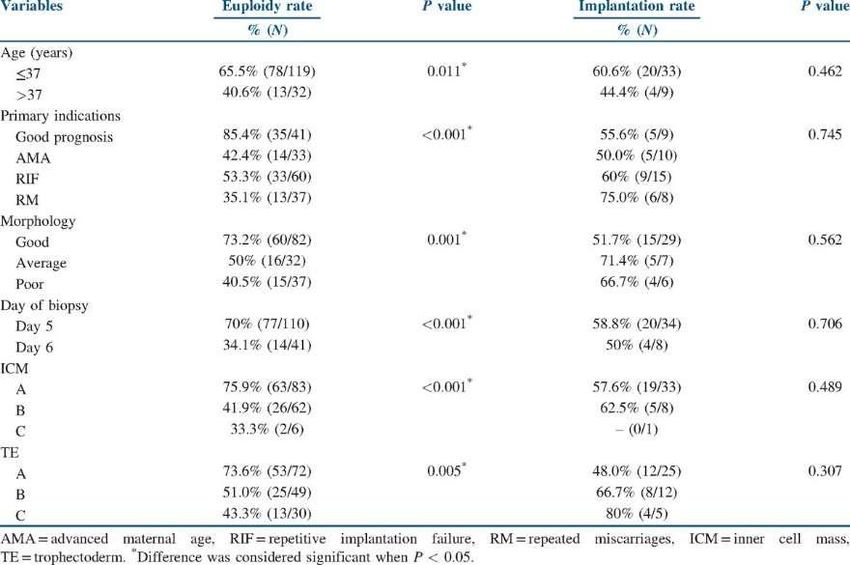
Shortening the time to conception
Previous studies have reported a longer
mean interval to subsequent conception after
a pregnancy loss, compared to the time to
conceive before a pregnancy [Hassan 2005; Sapra 2014]
6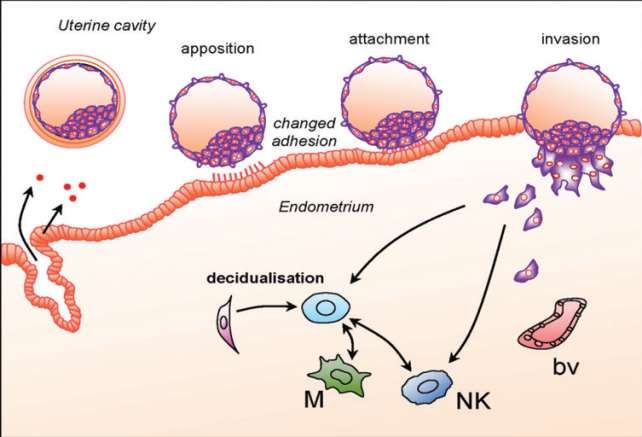
(2016) 7
Improving embryo quality 8
Sperm selection techniques
Sperm of men with RPL have significantly
reduced viability, increased proportion of
DNA damage (Ruixue 2013; Gil-Villa 2010; Brahem 2011)
and reduced sperm function parameters
such acrosomal status and nuclear
chromatin decondensation (Saxena 2008)
9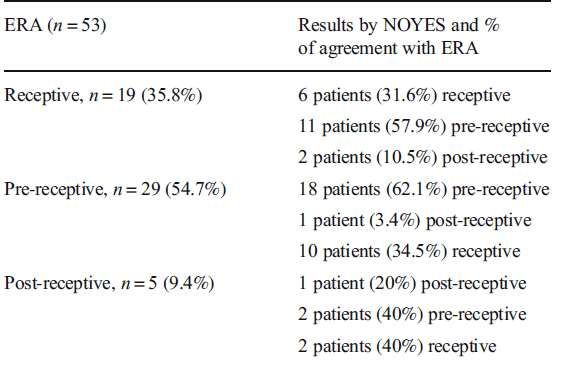
Sperm selection techniques
Washing
Density gradient centrifugation
Swim up
Electrophoretic sperm selection
Magnetic activated cell sorting and glass wool
separation columns utilizing the magnetic
properties of phosphatidylserine to separate
apoptotic from non‐apoptotic sperm.
Physiological intracytoplasmic sperm
injection (PICSI)
Intracytoplasmic morphologically selected
10
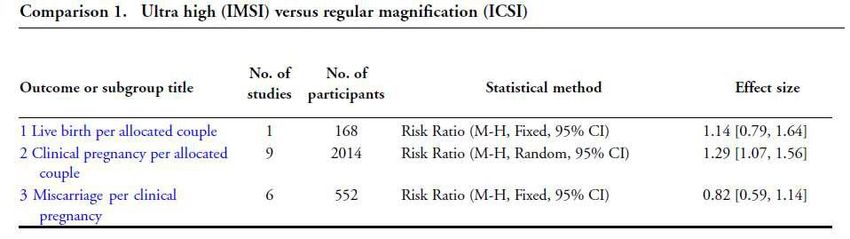
sperm injection (IMSI)Sperm selection techniques 11
12
Sperm selection techniques Intracytoplasmic morphologically selected sperm injection (IMSI) (2013) A technique to select sperm for injection to the egg by examining the organelle morphology, such as the acrosome, postascrosomal lamina, neck, mitochondria, tail and nucleus using ultra-high magnification (≥6000x) microscopy.
Selecting the best embryo
Embryo morphology
17 ± 1 h 27 ± 1 h 44 ± 1 h 68 ± 1 h 92 ± 2 h 116 ± 2 h
Time- lapse system Embryoscopy
Preimplantation genetic testing- aneuploidy
(PGT-A )
14Embryo morphology Embryo morphology is thought to be highly indicative of pregnancy outcome. Morphological grading of the embryo may allow the selection of "the best" embryos for transfer.
Selecting the best embryo
Relationship Between Morphology, Euploidy
and Implantation Potential of Cleavage and
Blastocyst Stage Embryos. (Majumdar et al 2017)
<
16
16Embryo morphology Correlation between standard blastocyst morphology, euploidy and implantation Capalbo et al, 2014 A moderate relation between blastocyst morphology and CCS data was observed, but the ability to implant seems to be mainly determined by the chromosomal complement of preimplantation embryos, rather than developmental and morphological parameters conventionally used for blastocyst evaluation.
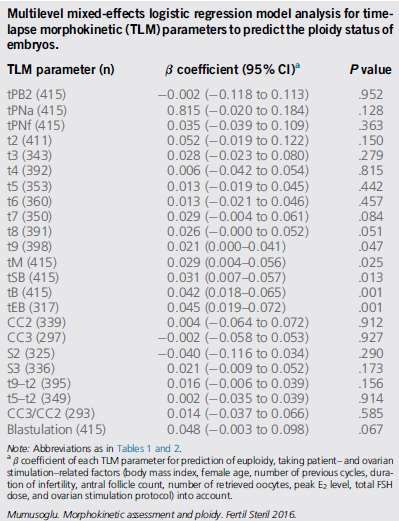
Time- lapse system Embryoscopy
Conclusion:
Five TLM parameters, all related to
timing of blastocyst development,
have limited ability to predict
euploidy when patient and ovarian
stimulation related factors are taken
into account.
18Time- lapse system Embryoscopy
(2018)
19Preimplantation genetic testing-
aneuploidy (PGT-A)
20Improving implantation
Assisted hatching
Biologic glue
Immunological “add ons”
21Assisted hatching (AH)
Assisted hatching (AH) is a manipulation of
the zona pellucida in order to facilitate
implantation.
Several techniques:
Partial mechanical zona • Acid tyrodes
dissection • Proteinases
Zona drilling • piezon vibrator
Zona thinning manipulators
• Lasers
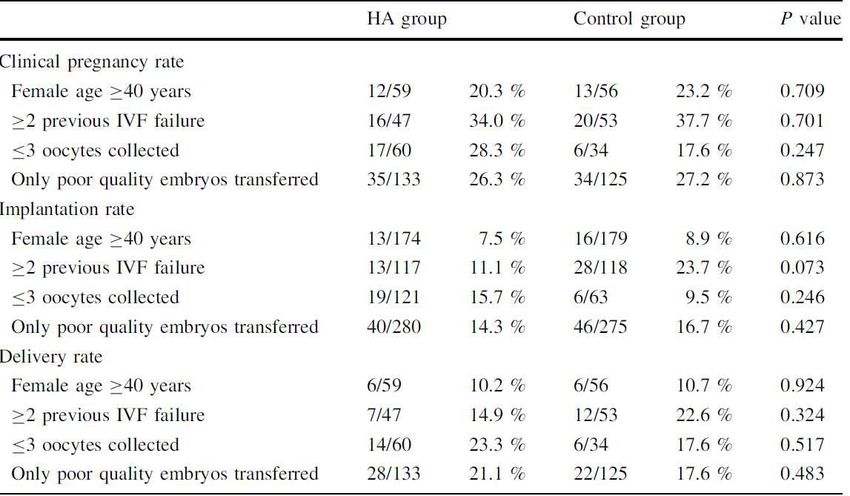
22Biologic glue
Various compounds have been added to the
embryo transfer medium in order to improve
adherence and subsequent implantation and
pregnancy rates.
Hyaluronic acid forms a viscous solution, that
might prohibit embryo expulsion, and may
facilitate diffusion and integration of the embryos
in the viscous solution that characterizes
intrauterine secreted fluid.
23Biologic glue
(2017)
24(2015) 25
Immunological “add ons”
(ASRM 2018)
Given the lack of evidence to support improved IVF outcomes, there isgood
evidence to recommend against the routine use of low-dose
aspirin to improve the outcome of live birth in ART cycles in the general population.
(From Level-I studies of Good and High quality). (Grade A).
There is good evidence to recommend
against the routine use of
corticosteroids during stimulation to improve the outcome of live birth in
ART cycles in the general population. (From principally Level-I studies of Good quality).
(Grade A).
There is good evidence to recommend against the routine use of corticosteroids during
the implantation window to improve the outcome of live birth in ART cycles in
the general population. (From principally Level-I studies of Good quality). (Grade A).There is insufficient
evidence to recommend for or against local G-CSF to
improve endometrial thickness in women with thin endometrium or clinical
pregnancy rates with IVF. (From principally Level-I studies of Good quality and Level-II
studies of Low and Good quality with inconsistent findings). (Grade C). There is
insufficient evidence to recommend for or against G-CSF or GM-CSF administered locally
or systemically to improve IVF outcomes. (From principally Level-I studies of Good
quality and Level-II studies of Low and Good quality with inconsistent findings). (Grade C).
There is insufficient evidence to routinely recommend intravenous fat
emulsions for infertile women pursuing IVF. (From one Level-I study of High quality and
one Level-II study of Low quality). (Grade C).
There is insufficient evidence to recommend IVIG administration as part of IVF
to improve IVF outcomes. (From two Level-I, but underpowered, studies, one Good quality
and one Low quality). (Grade C).
There is insufficient evidence to recommend adalimumab treatment to
improve IVF outcome. (From Level-II studies of Low quality). (Grade C).
There is insufficient evidence to recommend intrauterine infusion of
autologous peripheral mononuclear cells prior to ET to improve IVF outcome.
(From one Level-I study of Low quality and one Level-II study of Low quality). (Grade C).
There is insufficient evidence to recommend tacrolimus to improve IVF-ET
outcome. (From a single Level-II study of Low quality). (Grade C).Improving synchrony between
endometrium & embryo
28Improving synchrony between
endometrium & embryo
Timing of conception in relation to ovulation may affect
the spontaneous miscarriage rate.
Furthermore, aging of both spermatozoa and ova before
fertilization is accompanied by a higher probability of
miscarriage. (Guerrero et al. 1975; France et al. 1984)
(Gray et al 1995)
2930
EFFECT OF COH ON ENDOMETRIAL
DEVELOPMENT AND RECEPTIVITY
Estradiol and P are closely linked to endometrial
development and maturation.
Two frequently observed features of endometria
after COH are:
advanced histology
advanced down-regulation of the P receptor
Indicating an advanced receptive phase
An embryo–endometrium asynchrony.Horcajadas et al. 2007
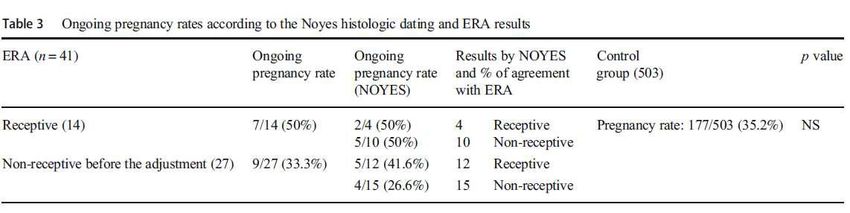
Dıaz-Gimeno et al. 2011
Endometrial gene expression profile reflects
human endometrial cycle and specifically its
receptive status based on its transcriptomic profile.
IVI group has developed a molecular diagnostic tool
based on the specific transcriptomic signature that
identifies the receptive endometrium (at LH7 in a
natural cycle or at day 5 of P (P 5) after proper E2
priming in a hormonal replacement therapy cycle).The endometrial receptivity array (ERA) consists of a customized array containing 238 differentially expressed genes, which is able to identify endometrial samples that are within the window of implantation regardless of their histologic appearance. Genes whose expression was consistent among three different models of endometrial receptivity: the natural cycle as the optimal model, the COH cycle as suboptimal, the refractory endometrium as a negative control.
35
36
THANK YOU
37
37You can also read