EXAMINING THE INTERSECTION BETWEEN NCDs AND COVID-19: LESSONS AND OPPORTUNITIES FROM EMERGING DATA - A report by The Economist Intelligence Unit ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

EXAMINING THE INTERSECTION BETWEEN NCDs AND COVID-19: LESSONS AND OPPORTUNITIES FROM EMERGING DATA A report by The Economist Intelligence Unit for The Defeat-NCD Partnership May 2021
Cover Photo: Nayan Khanolkar Permission is required to reproduce any part of this publication: It must not be distributed to, or accessed or used by, anyone else without prior written permission from The Defeat-NCD Partnership. Commercial use is not permitted without prior written agreement from The Defeat-NCD Partnership. Please cite this report as follows: The Defeat-NCD Partnership 2021. “Examining the intersection of NCDs and COVID-19: Lessons and opportunities from emerging data”. For further information please contact The Defeat-NCD Partnership secretariat by email: secretariat@defeat-ncd.org or telephone: +41 22 917 8334 May 2021 © 2021 The Defeat-NCD Partnership, all rights reserved.
EXAMINING THE INTERSECTION BETWEEN NCDs AND COVID-19: LESSONS AND OPPORTUNITIES FROM EMERGING DATA A report by The Economist Intelligence Unit for The Defeat-NCD Partnership May 2021
Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 2
Contents
About this report 3
Executive summary 4
Project overview 5
Background 5
Objectives 5
Understanding the impact of underlying NCDs on COVID-19 fatality 6
Identifying factors that exacerbate the relationship between NCDs and COV- 6
ID-19
What factors exacerbate COVID-19 more than others? 7
NCD burden has a causal relationship with COVID-19 mortality 9
Understanding the impact of COVID-19 on NCD services. 12
Disruptions to NCD services during COVID-19 12
Funding shortages for NCDs in LMICs 12
Funding for COVID-19 in LMICs 13
Development funding for COVID-19 response 13
Domestic health-related expenditure for COVID-19 14
COVID-19 response funding compared with spending on NCD care 14
COVID-19 as an opportunity for better NCD care 15
Increased funding for NCD treatment via better universal health coverage in 15
LMICs
Protection and prioritisation of community healthcare workers 15
Telehealth, m-health and other technology to manage NCDs. 16
Integrated COVID-19 and NCD care 16
Policy actions 18
Appendix 1. Search strategy 19
Appendix 2. Causal inference methods 20
Appendix 3. Statistical regression methods 21
Appendix 4: Statistical results tables 23
Table A1 23
Table A2 24
Table A3 25
References 26Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 3 About this report Produced by The Defeat-NCD Partnership Prepared by: The Economist Intelligence Unit: Chrissy Bishop, Project Lead, London, Health Policy and Clinical Evidence; Anelia Boshnakova, Project research, London, Health Policy and Clinical Evidence; and Peter Tennant, Consultant Data Scientist, Leeds, Causal Insights. Overall guidance and oversight: Mukul Bhola, Chief Executive Officer, The Defeat-NCD Partnership; and Praveen Pardeshi, Programme Coordinator for Global Scale-up, The Defeat-NCD Partnership. Technical inputs: Antony Chan, Business Development Analyst, The Defeat-NCD Partnership; and Shruti Choudhary, External Collaborator. This report describes the methods and main findings examining the intersection between non-communicable diseases (NCDs) and COVID-19 deaths in low and middle income countries (LMICs). This report presents the results of a literature review and a statistical regression exploring the relationship between NCDs and COVID-19 deaths. The statisti- cal regression reveals a range of socioeconomic, health and environmental factors which influence the relationship between NCDs and COVID-19 deaths. Using these factors com- bined with findings from the literature and expert engagement, we propose key strategies for mitigating COVID-19 that are sensitive to NCD burden in LMICs. To note, the findings and views expressed in this report are those of The Defeat-NCD Partnership and the The Economist Intelligence Unit. In addition to the financial and human resources allocated by The Defeat-NCD Partnership for the development of this report, The Economist Intelligence Unit has received support from Viatris through a financial contribution towards the preparation of this report.
Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 4
Executive summary
Progress towards reducing premature disruptions will leave a long tail of NCD
deaths from non-communicable diseases morbidity and mortality once the spread
(NCDs) has been made across the globe, of COVID-19 has receded. The already
but not at the pace required to meet the UN under-resourced healthcare systems of
Sustainable Development Goals (SDGs) for LMICs will struggle to grapple with this.
2030. Developments made to NCD servic- NCD care must be integrated into COV-
es are unequal across regions and income ID-19 mitigation to help manage the back-
groups, thus exacerbating inequalities. log of patients unable to access care during
NCDs are known to cluster in poorer areas, lockdowns.
where there is unequal access to health-
care. A body of fairly recent science explor- Funding for NCDs in LMICs is insuf-
ing COVID-19 suggests that more severe ficient, yet during COVID-19, LMICs re-
cases are seen in people with pre-existing ceived a radical increase in funding to tack-
illness. It is therefore impossible to ignore le COVID-19 response. COVID-19 funding
the possibility that NCDs and COVID-19 are should also be sensitive to NCD morbidity,
inextricably linked. to allow integrated care. This could start
with guidelines on and delivery of screen-
COVID-19 has rendered those populations ing programmes for NCDs during COV-
affected significantly by NCDs even more ID-19 vaccination programmes. COVID-19
vulnerable to ill health, making the pandem- vaccination centres provide a prime oppor-
ic a wakeup call for strengthened NCD ser- tunity to engage with hard-to-reach popu-
vices. This report arrives at the following lations. Funding an increase of community
policy actions to drive scalable solutions health workers could enable the delivery of
that both mitigate COVID-19 and address NCD health advice to patients in conjunc-
underlying NCD population morbidity in tion with administering COVID-19 vaccina-
low- and middle-income countries (LMICs): tions.
There is a causal relationship between Telehealth and mobile health pro-
underlying NCDs and COVID-19 fatality. grammes could be another cost-ef-
Our analysis revealed that factors strongly fective way to improve access to ba-
influencing this relationship include age, sic NCD care. Telehealth could further
gender, smoking and healthcare expend- increase the reach of community health
iture. Once these factors are accounted workers and enable digital access to infor-
for, our modelling suggests that a 10% re- mation on managing common NCDs such
duction in NCD mortality, through better as diabetes and obesity. Guidelines on the
access to healthcare, would have reduced use of digital health need to be developed
COVID-19 fatality by 20% in LMICs. In an and proposed as an option for accessing
LMIC of average population size, reduc- healthcare in LMICs. Traditional options
ing the NCD mortality by a third (to meet need to remain for older people and those
SDG3) would have averted 36,000 deaths with no access to technology.
from COVID-19.
Underinvestment in public health sys-
COVID-19 has severely disrupted NCD tems across the world hinders both
services, leaving a backlog of patients chronic NCD prevention and epidemic
who require care and support. The ex- preparedness. COVID-19 mitigation strat-
cess deaths due to COVID-19 service dis- egies that simultaneously address NCDs in
ruptions are currently unknown in most LMICs must be put in place alongside im-
LMICs and need to be better understood. provements to universal health coverage to
Despite this, it is likely that routine service ensure long-term sustainability.Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 5 Project overview Background Objectives In September 2020, as COVID-19 deaths In this report, we explore the theory that worldwide reached 1m, The Lancet pub- responsive, equitable and accessible NCD lished an editorial entitled “Offline: COV- services, provided via better access to ID-19 is not a pandemic.”1 The editorial universal health coverage in LMICs, could illuminated the real story behind the COV- improve population health and protect the ID-19 statistics—that “two categories world from future pandemics. To explore of disease are interacting within specific this hypothesis we aim to better under- populations—infection with severe acute stand the magnitude of the relationship respiratory syndrome coronavirus 2 (SARS- between NCDs and an increased risk of dy- CoV-2) and an array of non-communicable ing from COVID-19, as well as identifying diseases.”1 The syndemic of COVID-19 the factors that influence this relationship. and non-communicable diseases (NCDs) is Once identified, these factors are lever- exacerbated by pre-existing socioeconom- aged to propose COVID-19 mitigation strat- ic inequalities and disparities in access to egies that address NCD burden and health healthcare. The editorial emphasised that gaps, acknowledging that failure to do so addressing NCDs “will be a prerequisite for will further increase health inequalities and successful containment” of COVID-19.1 worsen population health. To do this we: In 2021 the World Health Organisation 1. Gain a better understanding of the fac- (WHO) reported that NCDs accounted for tors that influence the relationship be- over 40m deaths a year, with nearly 18m tween country-level burden of NCDs from cardiovascular diseases, more than and COVID-19 deaths using information 9m from cancer, over 4m from respirato- from the literature and publicly available ry diseases, and 1.5m from diabetes. The demographic, economic and health da- majority of these deaths, over 31m (77%), tasets to support a generalised linear occur in low-and middle-income countries regression. (LMICs).2 If addressing NCDs is essential for containing COVID-19, the world is al- 2. Explore the literature outlining the NCD ready off course.3 In 2020 the devastation services landscape in LMICs (in terms of a pandemic left prevention and treat- of funding and resources) and the dis- ment services for NCDs severely disrupted ruptions to these following COVID-19. across the care continuum. Around 94% of countries have reassigned health ministry 3. Propose COVID-19 mitigation strategies staff working in the area of NCDs to roles that simultaneously address NCD bur- focused on dealing with the pandemic.4 den (through an exploration of the liter- Poorer countries have seen more severe ature and findings from objectives 1 and disruptions. Only 20% of LMICs allocated 2). additional funding from government budg- ets to include the provision of NCD servic- 4. Discuss the implications of the findings es into the national COVID-19 plan.3 Given and make recommendations for the fu- that around 85% of the world’s population ture. reside in LMICs, the impact of tokenistic NCD resource allocation during COVID-19 is likely to have an aftershock on global morbidity and mortality.5 This aftershock will be intensified by social inequities that disproportionately effect NCD burden and exacerbate the impact of COVID-19. Simul- taneously, COVID-19 is exacerbating social inequities, which will lead to a greater NCD burden in LMICs and worldwide if action is not taken immediately.6
Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 6
Understanding the impact
of underlying NCDs on
COVID-19 fatality
To establish the extent to which NCDs in- ity and access to quality healthcare were
crease the risk of death from COVID-19 in investigated in three studies.8, 12, 13 A few
LMICs, we firstly conducted a literature studies discussed the impact of air pollu- A modelling study of
review and audit of publicly available de- tion on COVID-19 outcomes. Pozzer et al. 188 countries estimated
mographic, economic and health datasets concluded that air pollution is an impor- that 22% of the global
to develop a better understanding of the tant factor, increasing the risk of mortality
population, or 1.7bn
factors that exacerbate this relationship from COVID-19.14 In addition, studies also
people, have at least one
(such as pre-existing socioeconomic ine- found evidence on the impact of obesity,8,
qualities and disparities in access to health- 15
chronic renal disease,9, 16, 17 chronic liver
underlying condition
care). Once these factors were identified, disease18, 19 and chronic lung disease.12, 13 that puts them at
we used a causal inference approach to increased risk of severe
systematically explore the possible factors A modelling study of 188 countries esti- COVID-19 if infected
that confound the relationship between the mated that 22% of the global population,
exposure (NCDs) and the outcome (COV- or 1.7bn people, have “at least one under-
ID-19 mortality). We then conducted a sta- lying condition that puts them at increased
tistical regression, adjusting for the identi- risk of severe COVID-19 if infected (rang-
fied confounders, the results of which are ing from 66% of those aged 70 years or
are available in appendix 2 and 3). older).”20 The list of conditions explored in
this study included both infectious diseas-
Identifying factors that ex- es and NCDs. The region with the highest
acerbate the relationship be- proportion of people estimated to be at
increased risk of severe COVID-19 with at
tween NCDs and COVID-19
least one underlying condition was Europe
(31%), followed by North America (28%),
We focused on the evidence for the impact
Oceania (24%), Asia (23%), Latin America
of underlying NCDs on COVID-19 mortality
and the Caribbean (21%), and Africa (16%).
in LMICs only. We identified 14 systematic
The base-case scenario estimates for pop-
reviews and meta-analyses (four or which
ulations at high risk of COVID-19 with mul-
were primarily focused on China). We
tiple underlying conditions were largest in
found a limited number of primary studies
Europe (6.5%), followed by North America
from Brazil (n=7), Burkina Faso (n=1), China
(5.8%), Oceania (4.6%), Asia (4.5%), Lat-
(n=10), India (n=5), Iran (n=1), Turkey (n=2),
in America and the Caribbean (4.1%), and
and South Africa (n=1). A few studies cov-
Africa (3.1%). The study reported that the
ered a number of African or Latin American
share of the population at increased risk
countries.
of severe COVID-19 was highest in coun-
tries with older populations, African coun-
The majority of the studies were retrospec-
tries with high HIV/AIDS prevalence, and
tive cohort studies or systematic reviews/
small island nations with high diabetes
meta-analyses that included primary re-
prevalence. Estimates of the number of in-
search from LMICs as well as higher-in-
dividuals at increased risk were most sen-
come countries. Most of the selected
sitive to the prevalence of chronic kidney
studies had a nationwide or province/state-
disease, diabetes, cardiovascular disease
wide coverage and included hospitalised
and chronic respiratory disease.20 A num-
patients.7-10 Many studies were based on
ber of studies also highlight that in addition
data from the initial months of the pan-
to underlying NCDs, other factors such as
demic (the first quarter or half of 2020).8,
malnutrition or HIV may have an impact on
11
Almost all of the studies aimed to iden-
COVID-19 mortality in LMICs, especially in
tify significant associations with underlying
the under 60s.21
conditions to inform better clinical care for
people with COVID-19. Socio-demograph-
Since the beginning of the pandemic, pub-
ic factors such as social inequality, ethnic-
lic health authorities and governments haveExamining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 7
been collating evidence about underlying tween COVID-19 deaths and a range of var-
conditions placing individuals at high risk of iables for which data are publicly available.
severe COVID-19 including death. The US These included variables describing popula-
Centers for Disease Control and Preven- tion morbidity and proxies for health system
tion (CDC) last updated its list of conditions strength and government responsiveness
for which there is “sufficient evidence” in all LMICs. We found positive correlation
to draw conclusions in December 2020.22 coefficients between life expectancy, pop-
The evidence for the conditions and factors ulation density, cancer mortality, health ex-
listed in column 1 of Table 1 is considered penditure per capita, healthcare workforce
by the CDC as demonstrating the strong- and COVID-19 death. Listed in column 2 of
est and most consistent influence on the Table 1 are factors that we also found likely
relationship between NCDs and COVID-19 to influence the relationship, both accord-
death.23 In addition to assessing the litera- ing to the literature and those identified in
ture, we also conducted some descriptive our descriptive data analysis.
data analysis measuring the correlation be-
Table 1: NCDs and other factors reported to increase the risk of COVID-19 death
NCDs reported to have an impact Other possible confounders
of COVID-19 mortality23
Cancer Air pollution
Cardiovascular disease Social inequality
Chronic obstructive pulmonary disease (COPD) Ethnicity
Type 2 diabetes (including Access to quality healthcare (including workforce)
undiagnosed diabetes)
Pregnancy Global region
Smoking Chronic liver disease
Obesity (BMI> 30 kg/m2) and severe Chronic lung disease
obesity (BMI ≥ 40 kg/m2)
Chronic renal disease Age
Sickle cell disease Stringency of government response
Solid organ transplantation COVID-19 testing capabilities
Healthcare expenditure
Population density
What factors exacerbate COV- differences in COVID-19 reporting and re-
ID-19 more than others? sponse. Indeed, two previous studies only
found a positive correlation between NCDs
Following our literature review findings, and COVID-19 deaths when confounders
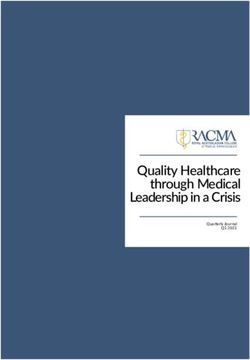
we checked the correlation coefficient be- had been taken into account.24, 25 We there-
tween NCD mortality (Institute for Health fore used our knowledge of other factors
Metrics and Evaluation, Global Burden of influencing the relationship between NCDs
Disease) and COVID-19 mortality in 112 and COVID-19 death (outlined in Table 1)
LMICs and found a negative correlation to conduct a causal inference analysis. A
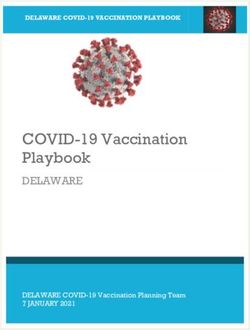
(Figure 1). Interpreted at face value, this causal inference analysis is a visual map-
means that having NCDs makes you less ping exercise that is often used before a
likely to die from COVID-19. However, this statistical regression to help identify con-
result cannot be interpreted in any mean- founding variables requiring adjustment
ingful sense, as there is likely to be substan- in the regression. It also helps to identify
tial confounding and heterogeneity from a minimally sufficient adjustment set for aExamining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 8
regression. This is especially important in power and could lead to spurious results.
analyses that involve estimating COVID-19 Therefore, using causal inference to iden-
deaths due to the abundance of influential tify a minimally sufficient adjustment set
factors. In statistical terms, adjusting for builds confidence in the results that the
too many confounders in a model reduces model produces.
Figure 1
COVID-19 mortality and NCD mortality
Correlation coefficient
All Countries -0.267298664
12,000
NCD Mortality/M 2016
10,000
8,000
6,000
4,000
2,000
0
0 200 400 600 800 1,000 1,200 1,400 1,600
COVID Mortality/M
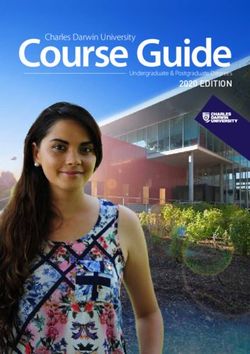
Figure 2 presents the causal diagram of 2. Key health behaviours including obesi-
factors influencing the relationship be- ty30, 33 and smoking.31, 34
tween country-level NCD burden and COV-
ID-19 fatality ratio in LMICs, as refined by 3. The funding and coverage of the health
critical discussion with domain experts. system35 examined through four meas-
We use fatality ratio as it refers to the risk ures: the number of doctors per popula-
of death in people who catch a disease, tion33, the number of hospital beds per
rather than mortality, which is the risk of population33, total healthcare expend-
death in people without the disease. Figure iture36 and total public health expendi-
2 visually maps the variables of interest and ture.
the direction of the relationships. Besides
the exposure and outcome (highlighted in 4. Environmental factors, of which only air
grey) and the confounding variables (high- pollution (referred to as all particulate
lighted in red), the causal diagram also matter pollution and ambient ozone)
identifies competing exposures (variables was hypothesised.14
that cause the outcome and are a potential
source of error). Figure 2 hypotheses four Highlighted in green is the population den-
main sources of confounding and the min- sity and each country’s response to the
imal adjustment set for estimating the to- COVID-19 pandemic—including the strin-
tal causal effect of the burden of NCDs on gency of nine non-pharmaceutical interven-
COVID-19 fatality. These are highlighted in tions such as school closures, workplace
red in Figure 2 and relate to: closures and travel bans (the Stringency In-
dex), and the number of tests performed.37,
1. Demographic and economic factors in- 38, 39
These were also hypothesised to act
cluding GDP,26, 27 total population size,28, as competing exposures (that is, important
29
and distribution by age,30 sex30 and ur- sources of heterogeneity between coun-
ban/rural location.31, 32 tries). The causal diagram also indicatesExamining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 9
that adjustment for the following variables reproduction number40). The total number
may improve precision (but not necessari- of COVID-19 tests performed was also
ly reduce confounding): population density hypothesised to be a potentially-important
(examined by adjusting for population and cause of COVID-19 fatality, but information
country size concurrently) and the coun- was only available for 61 of the 104 LMICs,
try’s response to the COVID-19 pandem- and so was only examined in sensitivity
ic (examined through two measures: the analyses.39
average Stringency Index39 and average
Figure 2
Causal diagram explaining the relationship between country-level burden of NCDs and death from COVID-19
Demographics and economics
Health
Males behaviours
Health system funding
Females Obesity and coverage COVID-19 response
GDP prevalence
and control
Doctors per Beds per
Urban Smoking population
population
Rural prevalence Stringency
Total
population
0–49 years Health system
funding and
50–69 years COVID-19
coverage
≥ 70 years response and
control
Public health Healthcare
expenditure expenditure
Reproduction Testing
number
Country Population
area density
COVID-19
incidence
Air COVID-19
pollution cases
Severe non-communicable
disease
COVID-19 fatality
NCD DALYs
COVID-19
deaths
Severe non-
communicable
disease
NCD deaths
Arrows represent hypothesised causal rela- NCD burden has a causal rela-
tionships. The exposure (burden of NCDs) tionship with COVID-19 mortality
and the outcome (mortality and fatality from
COVID-19) are shown in grey, confounders Next, we conducted a statistical regression
are shown in red and competing exposures to determine the strength of the relation-
are shown in green. Directly observable ship between NCDS (NCD mortality ra-
variables are shown as rectangles and var- tio—that is, deaths per population per year)
iables that cannot be directly observed are and COVID-19 fatality, adjusting for the
shown as ovals. Variables with double-out- confounders in Figure 2. We also looked at
lined edges are fully determined by oth- the total, predicted causal effect of NCD-
er variables in the diagram, making them linked disability-adjusted life year (DALY)
mathematically redundant, but they are ratios—in terms of DALYs per population—
shown to aid interpretation. on COVID-19 fatality. We were able to do
this across 104 LMICs that had complete
information on age and sex distribution,
cases and deaths from COVID-19, and
deaths and DALYs from NCDs.Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 10
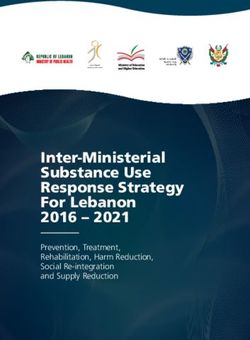
A strong relationship was observed be- rate according to the model include Brazil,
tween NCD mortality and COVID-19 fatal- India and Indonesia). We hypothetically
ity (see Table A2 in Appendix 4). This was reduced the NCD mortality by a third to A 10% reduction in
tested in three different ways to ensure meet SDG 3, which resulted in a reduc- NCD mortality, via, for
the strength of the relationship. Initially, tion in COVID-19 fatality to 18 per 1,000 example increasing
we accounted for only age, sex and pop- people, equivalent to 36,000 deaths access to universal
ulation in the analysis. This revealed that averted (countries with a similar case fa- health coverage in
a 10% higher annual NCD mortality ratio tality rate include Pakistan and Paraguay).
LMICs, would result
(equivalent to ≈50 per 100,000 population) Further reducing the average NCD mortal-
in a 20% reduction in
was associated with a 13% (95% CI: 9-18) ity by half would reduce COVID-19 fatality
higher COVID-19 fatality ratio. We then to 14 per 1,000 cases and avert 60,000
COVID-19 fatality.
accounted for smoking and healthcare ex- deaths (countries with a similar case fatal-
penditure, which increased the estimate to ity according to this model are Gambia and
22% (95% CI: 16-28); corresponding to an Rwanda, although these estimates are less
increase from the average case fatality rate robust owing to poor data quality).
of 2.4% to 2.9%. Lastly, we also accounted
for COVID-19 testing, which did not change For DALYs, a similar relationship was ob-
the results a great deal [22% (95% CI: 14- served, although there was uncertainty in
30)]. The sample of countries with informa- terms of modelling (see Table 3). Firstly,
tion on COVID-19 testing was smaller, and accounting only for age, sex and popula-
the results including testing should there- tion revealed that a 10% higher NCD DALY/
fore be interpreted with caution. A similar population ratio (equivalent to ≈2,000 per
result was also obtained when adjustment 100,000 population) was associated with
was made for all of the confounders and a 14% (95% CI: 2-28) higher COVID-19 fa-
competing exposures outlined in Figure 2 tality ratio. This estimate increased slightly
except for COVID-19 testing (18%; 95% to 16% (95% CI: 2-33) once smoking and
CI: 10-27). Figure 3 outlines the impact healthcare expenditure were accounted
that a reduction in the NCD burden would for, corresponding to an increase from the
have on COVID-19 deaths according to average case fatality rate of 2.4% to 2.7%.
the model results. A 10% reduction in Accounting for COVID-19 testing produced
NCD mortality, via, for example, increas- a similar estimate [16% (95% CI: -1-37)],
ing access to universal health coverage in which increased modestly with adjustment
LMICs, would result in a 20% reduction for the number of tests performed [20%
in COVID-19 Fatality. The average NCD (95% CI: 3-42)]. A similar result was also
mortality ratio in all LMICs modelled was obtained when adjustment was made for
5 per 1,000 people and the average COV- all confounders and competing exposures
ID-19 case fatality was 24 per 1,000 peo- (except COVID-19 testing) [22% (95% CI:
ple (countries with a similar case fatality 3-44)].Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 11
Figure 3
Applying the model results to an example country with an average population size of 60m people.
↓10% ↓20% COVID-19
Annual NCD
Mortality Ratio Case Fatality
Ratio
5.00 per 1,000 population 24 per 1,000 cases
5
4
Example: Country with 60 million people
6 million infected people 144 thousand deaths
COVID−19 CFR (Observed − Predicted)
3
2
India
1
Indonesia
0
−1
Brazil
−2
−3
−4
−5
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
NCD Annual Mortality Ratio (per 1,000)
↓10% ↓20% COVID-19
Annual NCD
Mortality Ratio Case Fatality
Ratio
5.00 per 1,000 population 24 per 1,000 cases
3.75 per 1,000 population 18 per 1,000 cases
5
Example: Country with 60 million people
4
6 million infected people 108 thousand deaths
COVID−19 CFR (Observed − Predicted)
3
Paraguay
2
India
1
Indonesia
0
−1
Brazil
−2
Pakistan
−3
−4 36 thousand deaths averted
−5
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
NCD Annual Mortality Ratio (per 1,000)
↓10% ↓20% COVID-19
Annual NCD
Case Fatality
Mortality Ratio
Ratio
5 5.00 per 1,000 population 24 per 1,000 cases
3.75 per 1,000 population 18 per 1,000 cases
4
2.50 per 1,000 population 14 per 1,000 cases
COVID−19 CFR (Observed − Predicted)
3
Gambia Paraguay
2
Example: Country with 60 million people
India 6 million infected people 84 thousand deaths
1
Indonesia
0
−1
Brazil
−2
Pakistan
−3 Rwanda
−4
−5
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
NCD Annual Mortality Ratio (per 1,000) 60 thousand deaths averted
Controlled for: Demographics, density, climate, economics, health
behaviors, health system funding & coverage, COVID-19 responseExamining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 12
Understanding the impact of
COVID-19 on NCD services.
Having seen that the statistical regression all healthcare workers are likely to get in-
indicates a relationship between under- fected, irrespective of social-distancing
lying population-level NCD burden and policies.69 Supply-chain disruptions also In contrast with other
COVID-19 deaths, we moved to exploring continue to persist, limiting the availability healthcare areas, it is
and proposing effective ways to mitigate of essential medicines for treating condi- estimated that less than
COVID-19 that are sensitive to NCD bur- tions such as NCDs.70 2% of donor funding is
den. Firstly, we used the literature to iden- allocated for NCDs.
tify critical factors, occurring both before Funding shortages for
and during the pandemic, that place NCD NCDs in LMICs
services at a disadvantage. These include
pre-pandemic financial underinvestment in Ten years ago, the WHO reported that na-
NCD services and disruptions to NCD ser- tional healthcare budgets were “increas-
vices during the pandemic. Our final rec- ingly allocated to treatment of cardiovas-
ommendations therefore aim to target are- cular disease, cancer, diabetes and chronic
as with the most lost ground to regain, as respiratory disease.”71 To understand how
well as solutions for improving future NCD LMICs address the growing burden of
care in LMICs. NCDs, we looked at the available data on
health systems’ spending on NCDs. Unfor-
Disruptions to NCD ser- tunately, these data are somewhat scarce,
vices during COVID-19 as most cost-of-illness studies are con-
ducted in high-income countries.72-74 Data
Some countries have been making pro- from the WHO Global Health Expenditure
gress towards universal health coverage, Database (GHED) reveals that the vast ma-
but the COVID-19 pandemic has impacted jority of 48 LMICs with available data are
the ability of health systems everywhere funding NCD care from domestic sources.
to provide undisrupted health services. In the five years between 2013 and 2018,
According to a survey conducted by the government expenditure on NCDs as a
WHO, 66% of responding countries had percentage of total healthcare expenditure
established national policies or documents (THE), as well as a percentage of GDP,
stating that essential health services would increased. However, it then levelled out
be maintained during COVID-19. Despite from about 2016, with very little increase
this, disruptions of some extent were al- in 2016-18. In some countries, spending on
most unanimous (around 55% of essential NCDs reduces in 2016-18, although there
health services were disrupted in the Afri- are some outliers—for example, in Botswa-
can region, for example).41 We found litera- na government expenditure on NCDs as
ture reporting on substantial disruptions to a percentage of THE increased threefold,
oncology,42-45 cardiovascular conditions46-49 from 18% to 54%.75
and stroke,50, 51 as well as a detrimental
impact on healthcare staffing levels. Com- Only a few countries with relevant GHED
mon strategies for managing some routine data, such as Malawi and São Tomé and
healthcare included simplifying treatment Príncipe, received funding from external
pathways in order to reduce the need for sources (equal to 1% GDP in 2014 for the
face to face appointments.52-67 former, and 1% of GDP in 2014 and 2017
for the latter). In 2018 none of the 48 coun-
The burden of COVID-19 on the already tries received any funding for NCDs from
scarce healthcare workforce in LMICs has external sources.75 In contrast with other
been substantial. As well as healthcare healthcare areas, it is estimated that less
staff being pulled from clinical practice to than 2% of donor funding is allocated for
COVID-19 task forces, high numbers of NCDs.76 A recent report by The Lancet
healthcare workers contracted COVID-19 NCDs and injuries (NCDIs) Poverty Com-
in LMICs. One explanation for this is the mission also highlighted the “inadequate
lack of personal protective equipment development assistance” for NCDs.77 In
(PPE).68 In countries where PPE is difficult 2017 the WHO provided NCDI funding of
to access, it is predicted that 70-100% of US$164m, accounting for 20% of all de-Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 13
velopment assistance (US$800m).77 The Health-related funding alone accounted for
main report of the Lancet NCDIs Poverty US$10,475,985m, the second largest allo-
Commission called for “augmented inter- cation after that provided for economic re- Health-related funding
national development assistance” targeted covery, US$18,563,983m.82 for COVID-19 accounted
at low-income families to bridge the gap to for US$10,475,985m, the
universal health coverage for the poorest The most significant funding for the second largest allocation
1bn of the world’s population.78 health-related response efforts was from after that provided for
public sources such as national govern- economic recovery,
A 2019 paper analysing public-sector ex- ments and the European Commission (over US$18,563,983m.
penditure on NCDIs in India, found that 90% of funding).82 The rest of the funding
the total expenditure was less than 0.5% came from multilateral organisations and fi-
of GDP (US$230m in purchasing power nancial institutions such as the IMF, the Eu-
parity terms).79 The spending on NCDIs ropean Investment Bank, the World Bank,
was just over 25% of total health spending and the Global Fund to fight AIDS, Tuber-
in the country, with about 80% provided culosis and Malaria.82 Below are some ex-
by the states and only 20% by the central amples of the areas prioritised for funding
government. In GDP terms, central gov- for LMICs in the form of grants or financial
ernment expenditure on NCDIs remained tools:
almost unchanged from fiscal-year 2012/13
(April-March) to 2016/17, ranging between • supply of tests, treatments and vaccines
0.057–0.065% of GDP.79 (for example, UNICEF’s new US$2.5bn
fund for LMICs);
Funding for COVID-19 in LMICs
• procurement and distribution of vac-
Development funding for cines (for example, US$750m for Indo-
COVID-19 response nesia from the Asian Development Bank
and US$150m for Ecuador from the
In October 2020 the Global Preparedness World Bank); and
Monitoring Board (GPMB), which moni-
tors preparedness for global health crises, • expansion of testing capacity and pro-
reported that US$11trn had been spent curement of personal protective equip-
worldwide on pandemic response efforts ment in LMICs (US$ 3.5bn pledged by
since COVID-19 had begun to spread.80, 81 the US to the Global Fund).82
One of the findings of the report citing that
figure was that “it would take 500 years In many LMICs, the pandemic response
to spend as much on investing in prepar- has predominantly been financed by ex-
edness as the world is losing” as a result ternal sources such as other governments,
of the pandemic.80 The GPMB couldn’t be global and regional multilateral organisa-
clearer that preparing for pandemics costs tions, and financial institutions. In February
a lot less than responding to them. What’s 2020 the WHO estimated that the fund-
more, the GPMB calculated the cost of pre- ing needed to resource its Strategic Plan
paredness as an additional investment of for Health Systems Strengthening was
just US$5 per person annually.80 US$675m. This estimate was updated in
May 2020 to US$1.74bn, in the light of the
As the world is still in the grip of the COV- evolution of the pandemic and the needs
ID-19 pandemic, all currently available of LMIC priority countries. In the first half
spending data are fluid and incomplete. of 2020, WHO distributed US$702m to its
Despite this, the figures are indicative of own Country Offices, Regional Offices and
the huge financial costs of the fight against Headquarters, and to priority countries or
COVID-19. A report by Devex, a news and territories as defined by the UN COVID-19
analysis organisation focused on global Global Humanitarian Response Plan.83
development funding, has been tracking
the funding provided to fight the COV- In the first few days of May 2021 India,
ID-19 pandemic.82 This funding is spread which is one of the countries that do not or-
across 19 areas, including economic re- dinarily rely on development assistance for
covery, response, small and medium-sized healthcare, began to receive international
enterprises, education, environment, re- funding to support its fight against a surge
search, and manufacturing, among others. in COVID-19 cases.Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 14
Domestic health-related ex- grammes. For example, the data available
penditure for COVID-19 for Botswana reveal that the country has
made an upfront payment to the COVAX It is apparent that
Data on disaggregated domestic health-re- initiative for 940,800 vaccine doses and an the amounts spent on
lated expenditure for COVID-19 is not only additional payment of US$7.1m to the Afri- NCDs and on financing
fluid but also extremely limited. Very often can Vaccine Acquisition Task Team to se- COVID-19 response are
the figures on spending include funding for cure more doses.85 in different categories
economic, social and healthcare purposes. of magnitude.
In the case of India, according to a govern- COVID-19 response funding com-
ment report from May 2020 the country pared with spending on NCD care
had spent US$2bn on the “containment” of
COVID-19 since the beginning of the pan- Even without reliable and consistent data
demic. This funding was allocated for test- for individual LMICs, it is apparent that the
ing labs and kits, essential items, provision amounts spent on NCDs and on financing
of PPE, telemedicine rollout, and insurance COVID-19 response are in different cate-
cover for health professionals, among oth- gories of magnitude. Development assis-
er things.72, 84 In addition to this, the IMF’s tance for NCDIs in 2017 was estimated at
COVID-19 Policy Tracker reported that the US$800m, while donor funding for COV-
new budget for fiscal-year 2021/22 in India ID-19 response is measured in billions or
provides for “expanded spending on health trillions. With 77% of all NCD deaths in
and wellbeing”, a category including the 2021, LMICs are disproportionately affect-
COVID-19 vaccination programme.85 ed by NCDs in terms of mortality.2 Health
systems are increasingly spending more of
The IMF Policy Tracker data on domestic their budgets on NCDs, but the huge un-
health-related spending for COVID-19 are derfunding of healthcare in LMICs means
limited to a few countries. Where such that many of the poorest families incur cat-
data are available, they reflect only some astrophic expenses for health and become
aspects of spending, such as costs relat- trapped in a never-ending cycle of illness
ed to rolling out national vaccination pro- and poverty.71, 78Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 15
COVID-19 as an opportunity
for better NCD care
Many of the challenges highlighted by the in ensuring that no one is left without uni-
impact of COVID-19 in LMICs are an ex- versal healthcare coverage.77, 78
acerbation of longstanding issues within Instead of funding
governments and healthcare systems, Low levels of funding for NCDs translate diseases in isolation,
while others are new challenges caused by into limited access to healthcare in LMICs. health investments
the pandemic. Whether facing old or new A 2016 study in Malawi showed that even in LMICs should
problems, LMICs will struggle to get them- though the Essential Health Package in take a systemic
selves out of the current COVID-19 crisis the country should provide free care at the approach to prevent
without support.45 As noted in this report, point of use, the economic burden of NCDs chronic diseases and
well-resourced governments and organisa- for the population is high and can lead to communicable diseases
tions have stepped in to help erase debt in catastrophic spending.74 This only aggra-
while meeting the
some countries and provide interest-free vates poverty—and, as the 2010 WHO
challenge of universal
loans.86 However, a continuation of vertical report pointed out, “poverty contributes
responses to COVID-19 in health systems to NCDs and NCDs contribute to poverty,”
health coverage.
in LMICs risks focusing solely on prevent- thus creating a vicious cycle of inequality
ing and containing COVID-19. If COVID-19 and ill health in the poorest countries.71 The
response does not consider the affects to study in Malawi concluded with a call for
the wider health system, underlying health further investments to ensure adequate
conditions such as NCDs and pre-existing and affordable care for people with chron-
resource constraints, LMICs will remain ic NCDs, a conclusion that is applicable for
vulnerable.87 We propose the following key the majority of LMICs.74, 78 One of the key
factors for generating COVID-19 mitigation messages of a Lancet Commission report
strategies that simultaneously address was that “essential NCDI services must be
NCD burden, health system coverage and financed through pooled, public resources,
resource constraints. either from increased domestic funding or
external funds.”78
Increased funding for NCD
treatment via better univer- Underinvestment in public health systems
across the world—a very real problem—
sal health coverage in LMICs
hinders both chronic NCD prevention and
epidemic preparedness. As a recent US re-
In our statistical analysis, where a person
port shows, even in high-income countries
lives and the relative wealth of the coun-
funding of public health systems is cycli-
try was found to influence the relationship
cal—with a pattern of temporary increases
between underlying NCDs and death from
in funding in times of crises and followed
COVID-19.26, 27 Instead of funding diseases
by decreased spending when the crisis is
in isolation, health investments in LMICs
over. The underinvestment in public health
should take a systemic approach to pre-
systems affects not only the primary pre-
vent chronic diseases and communicable
vention of chronic diseases but also epi-
diseases while meeting the challenge of
demic preparedness. Moreover, the report
universal health coverage.88 It is appar-
highlights that health equity is not sepa-
ent that the amounts spent on NCDs and
rate from preparedness,89 which is clearly
on financing COVID-19 response are in
demonstrated in the causal effect between
different categories of magnitude. The
NCD mortality and COVID-19 mortality.
striking statement in the GPMB report
that “it would take 500 years to spend as
much on investing in preparedness as the Protection and prioritisation of
world is losing” as a result of the pandemic community healthcare workers
serves as a reminder about the dangers of
short-sightedness in healthcare planning.80 Community health workers are key to pro-
Investing in health is imperative, as it is viding basic medical care in LMICs, includ-
much cheaper than financing the response ing care for NCDs. Our statistical analysis
for a future pandemic or disaster. It is crit- showed us that the coverage of the health-
ical, therefore, to invest in prevention and care system is an important determinant of
better management of chronic NCDs, and whether NCDs in the underlying populationExamining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 16
increase the risk of death from COVID-19. 35 and cancer.66, 95-104 A basic mobile-phone
It is suggested in the literature that increas- function such as text messaging (rather
ing the number of community health work- than smartphone app-based services) can …population vaccination
ers will both improve coverage of care for assist in the delivery of quality services by also provides a
households and generate return on invest- facilitating access to information on preven- convenient opportunity
ment, owing to a healthier population. A tion. Mobile phones are being increasingly for NCD screening.
modelling study put this theory to the test used in LMICs to improve access to com-
in South Africa, estimating that increasing munity health workers as well as improving
the number of community health workers communication between community- and
to 96,000 (from 60,000) and paying them hospital-based physicians.105 Guidelines to
the minimum wage would contribute an ensure that telehealth and mobile health
additional R13.6bn (US$1bn) to the econo- services continue after COVID-19 should
my over three years. This is the equivalent be developed to continue delivery of NCD
of 0.3% of GDP.90 care.
As well as providing basic medical support, In order to ensure vulnerable populations
the role of community health workers has such as the elderly and very poor are not
become increasingly diverse during the excluded, digital solutions must be adopt-
COVID-19 pandemic, incorporating tasks ed alongside traditional ones93 There are
such as helping pharmacists and provid- also blurred lines between telehealth and
ing mental health support. Disruptions social media, which can lead to misinfor-
to pharmaceutical supply-chains due to mation. To make online healthcare options
lockdowns and a public reluctance to visit more reliable, governments must design
pharmacies due to COVID-19 transmission and implement better strategies to tackle
risk mean that prescriptions to manage misinformation, both during the pandemic
NCDs have been hard to come by.91, 92 The and beyond.106
Pan American Health Organisation (PAHO)
suggests that access to medicines can be Integrated COVID-19
improved by policies that advocate for a and NCD care
90-day supply to ensure management of
NCDs without the need to physically visit a Amid the dual challenges of COVID-19 and
pharmacy. PAHO also says that home deliv- NCDs, there are opportunities to develop
ery services should be set up through com- integrated care. Some evidence suggests
munity health worker networks and strong that population vaccination also provides
monitoring of NCD medication stocks.91 a convenient opportunity for NCD screen-
The Lancet Psychiatry also proposed task ing. NCD screening serves two purpos-
shifting as a method of upskilling commu- es: on the one hand, it provides a better
nity health workers to include basic mental understanding of population morbidity to
health support within their job roles during help appropriately commission NCD ser-
the COVID-19 pandemic.93 vices; on the other, it reveals acute health
concerns in individuals. Emerging evidence
Telehealth, m-health and other indicates that many patients admitted to
technology to improve access hospital with severe COVID-19 often face
to care to manage NCDs. other acute health concerns. For example
in Latin America, a large multi-centre study
Many countries lack the regulatory frame- found a high proportion of patients with
works required to integrate and reimburse abnormal liver function on admission for
telemedicine platforms within their health COVID-19.107 Meta analyses have shown
systems. It is hoped that COVID-19 may hyperglycaemia in non-diabetics was asso-
be the force that encourages wider adop- ciated with more severe illness in those ad-
tion. Mobile health (m-health) is not only a mitted for COVID-19.108 Glycaemic testing
method for maintaining the care delivery and control are emerging as important to all
for people with NCDs during a pandemic, COVID-19 patients, even when they have
the surge in its usage can facilitate NCD no pre-existing diabetes diagnosis, as most
risk-factor surveillance and improve the COVID-19 patients end up being prone to
management of chronic conditions.94 Tele- glucose metabolic disorders.109 One study
health services have been used as a backup suggests that guidelines for glycaemic
for delivering NCD care during COVID-19 testing on COVID-19 patients should be
across the NCD disease spectrum, includ- developed, given that better outcomes are
ing mental health, stroke, hypertension expected for those who have improved gly-
caemic control.110Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 17
Although screening the global population educated on screening for NCDs when
for NCDs in tandem with vaccinating for they consult with patients at a COVID-19
COVID-19 would present too many upfront vaccination centre. COVID-19 vaccination …COVID-19 vaccination
costs, prioritisation based on risk groups centres are therefore a prime opportunity centres are therefore
could be a more feasible option.111 (At-risk for both screening and directing more peo- a prime opportunity
groups, according to our statistical analy- ple to the appropriate care as deemed cost for both screening and
sis, are those that smoke,31, 34 are obese,30, effective for managing NCDs in LMICs directing more people
33
are pregnant, are over the age of 50,30 according to the WHO “best buy” scenar- to the appropriate care
live in poorer areas or (not tested in our ios.112 A few such examples include drug as deemed cost effective
analysis) have several underlying health therapy for cardiovascular disease and for managing NCDs
conditions at the same time.) However, diabetes, screening women for cervical in LMICs according
governments and healthcare leaders must cancer, advice on physical activity and diet,
to the WHO “best
be cautious of the large numbers of peo- and providing inhaled salbutamol for people
buy” scenarios.
ple with NCDs that a screening approach presenting with asthma.112 For those who
might uncover and must have practical inevitably present to healthcare provid-
solutions to provide care for these people. ers with severe COVID-19 and underlying
Care could be as subtle as providing health health conditions, medications or medical
advice in a leaflet at a COVID-19 vaccina- procedures may be required. Those affect-
tion centre; registering previously unregis- ed by severe cases of COVID-19 should
tered people on the health system, mak- leave the hospital with an understanding of
ing it easier to contact them virtually or by their underlying health concerns and how
mail; and conducting tests such as blood to manage them, as well as advice on re-
pressure, cholesterol and glucose meas- covery from COVID-19 itself.
urements. Healthcare workers can be alsoExamining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 18
Policy actions
In this report, we have established a causal • Funding for NCDs in LMICs before the
relationship between underlying NCDs and pandemic was insufficient, whereas
COVID-19 death, explored the literature LMICs received a radical increase in The mitigation
discussing NCD service disruptions dur- funding to respond to COVID-19. COV- strategies highlighted
ing COVID-19 and NCD funding deficits, ID-19 funding should be partly directed in this report have the
and proposed COVID-19 mitigation strat- to integrated COVID-19 and NCD care. potential to improve
egies to facilitate access to NCD services This might include creating guidelines on population health
in LMICs. These mitigation strategies have and delivering screening for NCDs dur- by facilitating access
the potential to improve population health ing COVID-19 vaccination programmes, to NCD services and
by facilitating access to NCD services and as well as increasing the numbers of
protect the world from
protect the world from future pandemics. (and up-skilling) community health work-
future pandemics.
From this exploration we arrive at five key ers to deliver NCD advice during vacci-
points: nation programmes.
• There is a causal relationship between • Telehealth and mobile health pro-
underlying population NCDs and COV- grammes could be employed as a
ID-19 fatality. Factors that influence this cost-effective way to increase the reach
relationship include age, gender, smok- of community health workers and pro-
ing and healthcare expenditure. Ac- vide easy access to information to man-
counting for smoking and healthcare ex- age common NCDs such as diabetes
penditure in addition to age and gender and obesity. Guidelines on the use of
increased the average case fatality rate digital health need to be developed and
from 2.4% to 2.9%. COVID-19 testing proposed as an option for accessing
rates did not greatly affect the results, healthcare in LMICs. Traditional options
although this may be due to incomplete need to remain for older people and
data. those with no access to technology.
• COVID-19 has severely disrupted NCD • Underinvestment in public health sys-
services, leaving a backlog of patients tems across the world hinders both
who require care and support. The chronic NCD prevention and epidem-
excess deaths due to COVID-19-re- ic preparedness. COVID-19 mitigation
lated service disruptions are currently strategies that simultaneously address
unknown in most LMICs, but it is like- NCDs in LMICs must be implemented
ly that there will be a long tail of NCD alongside improvements to universal
morbidity and mortality after COVID-19 health coverage to make sure that they
that already under-resourced healthcare are sustainable in the long term.
systems in LMICs will need to grapple
with. Cost-effective strategies for deal-
ing with this are urgently needed.Examining the intersection between NCDs and COVID-19: Lessons and opportunities from emerging data 19
Appendix 1. Search strategy
This review was not designed to be fully The searches retrieved 2046 articles, and
comprehensive. Rather, it followed a struc- after a first sift we identified 765 potential-
tured methodology using the following ly relevant studies; about a third of these
search approaches: were studies from China. The 389 stud-
ies selected after the second sift focused
• Bibliographic database search via Em- on all aspects of the relationship between
base.com (MEDLINE and Embase) non-communicable diseases (NCDs) and
COVID-19. Studies that explored the im-
• Grey literature searches to identify rel- pact of COVID-19 on the mental health of
evant reports that are not published in healthy populations, including pregnant
the scientific journals and therefore not women, or where the focus was solely on
included in bibliographic databases the epidemiology and clinical management
of the infection, were excluded as out of
• Supplementary search techniques such scope.
as internet search using advanced Goog-
le search techniques, citation tracking The 389 studies selected at second sift in-
and checking the references in relevant cluded mostly observational studies such
publications. as surveys, cross-sectional studies and
retrospective cohort studies. Systematic
After a scoping search identified a huge reviews and meta-analyses were also in-
volume of studies (over 6,000), the search cluded if they covered LMICs.
strategy was revised to focus on low- and
middle-income countries (LMICs). The In the third sift, we prioritised 104 studies
main database search retrieved 2045 stud- based on study methodology and quality
ies—634 of which were from China— as well as study sample size.
based on the keywords assigned to the bib-
liographic records. The database searches
were limited to English language reports
published since January 2020.You can also read