Exploring traditional medicine utilisation during antenatal care among women in Bulilima District of Plumtree in Zimbabwe - Nature
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
www.nature.com/scientificreports
OPEN Exploring traditional medicine
utilisation during antenatal care
among women in Bulilima District
of Plumtree in Zimbabwe
1*
Nicholas Mudonhi , Wilfred Njabulo Nunu1,2, Nomathemba Sibanda1 &
Nkosana Khumalo1
Traditional medicine utilisation during antenatal care has been on the increase in several countries.
Therefore, addressing and reinforcing the Sustainable Development Goal of maternal mortality
reduction, there is a need to take traditional medicine utilisation during pregnancy into consideration.
This paper explores traditional medicine utilisation during antenatal care among women in Bulilima
District of Plumtree in Zimbabwe. A cross-sectional survey was conducted on 177 randomly selected
women using a semi-structured questionnaire. Fisher’s Exact Test, Odds Ratios, and Multiple Logistic
Regression were utilised to determine any associations between different demographic characteristics
and traditional medicine utilisation patterns using STATA SE Version 13. The prevalence of Traditional
Medicine utilisation among pregnant women was estimated to be 28%. Most traditional remedies
were used in the third trimester to quicken delivery. The majority of women used holy water and
unknown Traditional Medicine during pregnancy. There was a strong association between age and
Traditional Medicine utilisation as older women are 13 times more likely to use Traditional Medicine
than younger ones. Women use traditional medicine for different purposes during pregnancy, and
older women’s likelihood to use Traditional Medicine is higher than their counterparts. The traditional
system plays an essential role in antenatal care; therefore, there is a need to conduct further studies
on the efficacy and safety of utilising Traditional Medicines.
Maternal health is generally of global concern, and to ensure safe pregnancies and delivery, several countries
have been challenged to provide adequate maternal and child health services as enshrined on the Sustainable
Development Goal (SDG) of reduction in maternal mortality of 7.5% per year between 2016 and 20301–3. How-
ever, different countries utilise different health systems to achieve these global targets4,5. In Africa (particularly
in Sub-Saharan Africa), access to modern health facilities is a challenge due to exorbitant costs associated with
it and the health care recipients’ economic status6.
Traditional medicine (TM) utilisation has been on the upsurge in several African countries as it plays a vital
role during antenatal c are7. It could contribute positively or negatively towards the attainment of SDG 3, empha-
sising reducing the Global Maternity mortality rate to 70 per 100,0003,7,8. The use of traditional medicines in
pregnancy management induces and shortens labour is a well-established practice among African c ountries9,10.
Reported reasons for TM utilisation during pregnancy include; promotion of foetal growth, spiritual cleansing,
protection against evil influence, to have a male child and assisting childbirth just to mention a few11,12. The route
of TM exposure during antenatal care varies; some are ingested, inhaled, or applied as an ointment for different
purposes13,14. Determinates such as women’s belief, lower cost, and accessibility of TM triggers them to have
trust in their effectiveness compared to western medicines15.
In the Zimbabwean context, preference to deliver at home and utilisation of TMs has been influenced by the
cost of health care, distance, educational level, and r eligion16–18. Traditional medicines have been utilised since
the pre-colonial era, with over 80% of the population still relying on traditional remedies and the Indigenous
Knowledge (IK) being passed down to generations19,20. Women prefer birth attendants that understand their
spiritual background, and they feel at peace when they perform their cultural activities that are believed to be
1
Department of Environmental Science and Health, Faculty of Applied Sciences, National University of Science
and Technology, Corner Gwanda Road and Cecil Avenue, P O Box AC 939, Ascot, Bulawayo, Zimbabwe. 2Scientific
Agriculture and Environment Development Institute, Bulawayo, Zimbabwe. *email: nicholasnicky70@gmail.com
Scientific Reports | (2021) 11:6822 | https://doi.org/10.1038/s41598-021-86282-3 1
Vol.:(0123456789)
www.nature.com/scientificreports/
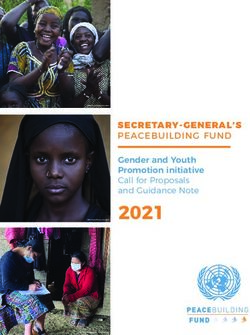
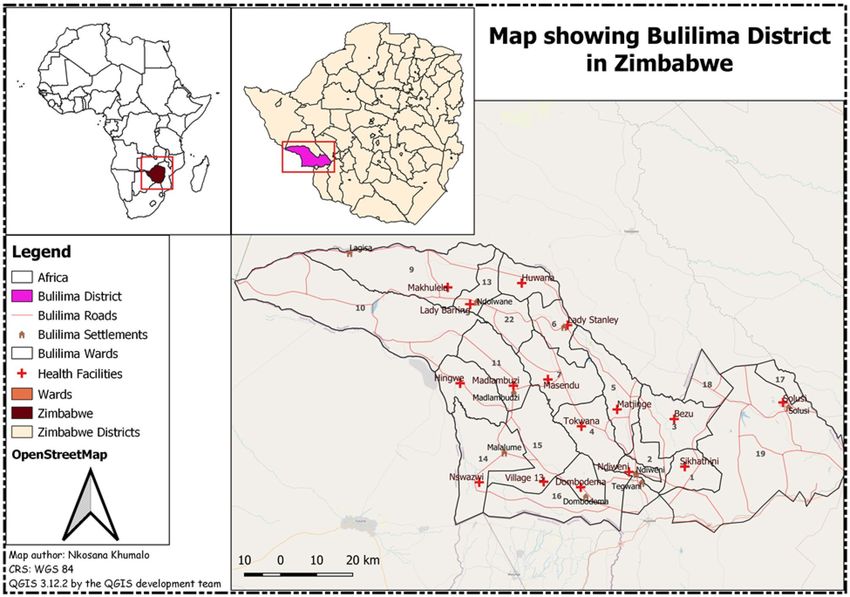
Figure 1. Map showing Bulilima District and its health facilities.
beyond human c apabilities17. In addition, the Zimbabwe Maternal and Perinatal Mortality Study conducted by
the Ministry of Health and Child Care in 2007 found that women prefer to go into labour at traditional birth
attendants and faith healers’ homes21. In Zimbabwe’s rural areas, lack of access to western medicines has been an
influencing factor for women to use TM. In addition, better modern health facilities with required expertise and
equipment are largely centralised in urban setups, making it difficult for rural women to access these s ervices22.
There have been several strategies that have been implemented in rural Zimbabwe including the establish-
ment of Maternal Waiting Homes (MWH) to try and reduce barriers such as cost of transport, distance and
prevent maternal complications (just to name a few) to improve access of women to modern maternal health
services3,23. However, most women still prefer to utilise TM despite campaigns that discourage women from
utilising TM as some have unforeseen adverse r eactions24. The majority of users; therefore utilise TM secretly
and rarely disclose to the health service providers. In Plumtree, particularly in Bulilima District, the average
distance walked by women to the nearest health facility is estimated at between 5 and 10 km, influencing them
to consult the traditional system which is readily available in their c ommunities25. Generally, it is suggested that
there should be a health facility within a 5 km radius in different communities and women should not walk more
than the 5kms in search of maternal services18. Therefore, this study explores traditional medicine utilisation
trends during antenatal care among women in Bulilima District of Plumtree in Zimbabwe. This study presents
a window of opportunity to determine the TM utilisation patterns that would inform policy makers in coming
up with strategies that would strengthen the current existing health systems.
Methods
Study area. Bulilima is one of the seven districts with 22 wards located in Matabeleland South province
and is in Region 5, prone to severe drought26. The district has one main referral hospital with sixteen clinics
that usually refer pregnant women with complications to a district hospital and has an average household size
of 527. Generally, it is estimated that this district is home to 57,68128. The average distance that women walk to
the nearest clinic is estimated to be 5–10 km. The study area is illustrated in Fig. 1 which was developed using
Quantum Geographic Information System (Credit: QGIS 3.12.2 by the QGIS development team). Although a
similar study was conducted in Harare, Zimbabwe which is an urban set up with a different population composi-
tion predominantly the Shona tribe, our study was entirely rural-based and in a different region of the country
with predominantly Kalanga and Ndebele speaking people relying on different TM as compared to some other
regions as the belief systems differ27,29.
Scientific Reports | (2021) 11:6822 | https://doi.org/10.1038/s41598-021-86282-3 2
Vol:.(1234567890)www.nature.com/scientificreports/
Traditional medicines utilisation
Didn’t use TM Used TM
Variable Freq % Freq % Fisher Exact MLR-OR MLR-95% CI MLR P-value
Age
15–19* 33 26.0 5 10.0 ***
20–24 26 20.5 7 14.0 1.78 0.51–6.25 0.37
25–29 25 19.7 9 18.0 2.38 0.71–7.97 0.16
30–34 18 14.2 8 16.0 2.93 0.84–10.30 0.09
0.011
35–39 18 14.2 9 18.0 3.30 0.96–11.35 0.06
40–44 5 3.9 7 14.0 9.24 2.10–40.75 < 0.01
45–49 2 1.6 4 8.0 13.2 1.90–91.91 < 0.01
50–54 0.00 0.0 1 1.0 1
Mean (sd)
27.4 (8.4) 33.4 (9.6)
29.1 years (9.1)
Marital status
Single* 18 14.2 7 14.0 ***
In a relationship 45 35.4 14 28.0 0.80 0.28–2.31 0.68
Married 42 33.1 18 36.0 1.10 0.39–3.10 0.85
0.853
Widowed 7 5.5 5 10.0 1.84 0.43–7.77 0.41
Divorced 6 4.7 2 4.0 0.86 0.14–5.31 0.87
Cohabiting 9 7.1 4 8.0 1.14 0.26–4.95 0.86
Tribe
Ndebele*** 58 45.7 18 36.0 ***
Shona 14 11.0 4 8.0 0.92 0.27–3.15 0.90
Kalanga 50 39.4 24 48.0 0.349 1.55 0.75–3.17 0.23
Tonga 3 2.4 1 2.0 1.07 0.11–10.97 0.95
Other 2 1.6 3 6.0 4.83 0.75–31.23 0.10
Religion
Christian*** 104 81.9 35 70.0 ***
Traditional 11 8.7 14 28.0 0.002 3.78 1.57–9.10 < 0.01
None 12 9.5 1 2.0 0.25 0.03–1.97 0.19
Level of education
Primary*** 35 27.6 13 26.0 ***
Ordinary level 54 42.5 24 48.0 1.20 0.54–2.66 0.66
Advanced level 23 18.1 8 16.0 0.94 0.34–2.61 0.90
0.342
Tertiary 11 8.7 1 2.0 0.24 0.03–2.09 0.20
Never attended
4 3.2 4 8.0 2.69 0.59–12.37 0.20
school
Employment status
Employed 22 17.3 12 24.0 ***
Self Employed 23 18.1 10 20.0 0.495 0.80 0.29–2.22 0.66
Unemployed 82 64.6 28 56.0 0.63 0.27–1.43 0.26
Place of delivery
Hospital 99 78.0 32 64.0 ***
0.086
Home 28 22.1 18 36.0 1.99 0.97–4.06 0.06
First child
Yes 47 37.0 6 12.0 ***
0.001
No 80 63.0 44 88.0 4.46 1.77–11.24 < 0.01
Parity
1 48 37.8 6 12.0 ***
2–5 75 59.1 39 78.0 0.002 4.16 1.64–10.57 < 0.01
6 > = 4 3.2 5 10.0 10.00 2.09–47.82 < 0.01
Relationship between parity and age
Used TM (Mean;
Mean (sd) sd) Did Not Use TM (Mean; sd)
15–19 1.1 (0.3)
20–24 1.5 (0.5)
25–29 1.9 (1.3)
Continued
Scientific Reports | (2021) 11:6822 | https://doi.org/10.1038/s41598-021-86282-3 3
Vol.:(0123456789)www.nature.com/scientificreports/
Relationship between parity and age
Used TM (Mean;
Mean (sd) sd) Did Not Use TM (Mean; sd)
30–34 2.0 (0.3)
35–39 2.0 (0.2)
40–44 2.7 (1.6)
45–49 2.7 (1.6)
50–54 2.7 (1.6)
Overall 1.90 (1.1) 2.3 (1.3) 1.7 (0.9)
Table 1. Demographic Characteristics of respondents and Traditional Medicine Utilisation.
Study design. A cross-sectional survey that explored traditional medicine utilisation during antenatal care
among women in Bulilima District was conducted. This study design was appropriate as it enabled the explora-
tion of traditional medicine utilisation trends in a single point in time, ensuring cost-effectiveness as this study
was not f unded30.
Target population. This study targeted all women who delivered from January-December 2019 (to mini-
mise recall bias) in Bulilima District as captured in the health facilities’ birth registers. The women who met the
inclusion criteria were 586, and there was no age limit.
Sampling. A sample size calculator on EPI INFO Version 7.2.2.6 was used to estimate the minimum sample
size required for this study. A confidence level of 95%, Width of Confidence of 5%, and the expected value of
attribute applied to the study population of 586 gave an estimated sample size of 185. Random numbers were
then generated, and the 185 selected and followed up.
Data collection tools. Pre-testing of a semi-structured questionnaire and data collection was done by the
researchers who are all Trained Public Health Specialists between January 2020-February 2020 from women
delivered at the clinic or home in Bulilima district but registered at the clinic. The questionnaire was categorised
into two sections, that is: the first section delved on socio-demographic characteristics (age, race, ethnicity, edu-
cation, marital status, parity). The second section comprised questions on the source, different types, reasons,
and frequency of TM used. The questionnaire was developed in English and then translated to the local language
that is "isiNdebele," which is mainly spoken and taught within the district.
Data analysis. Collected data was coded and entered into EpiData 3.1 then further exported to Microsoft
Excel 2013. The analysis was done with the aid of STATA version 13; for instance, descriptive statistics were
used for women’s demographic characteristics. Fisher’s Exact, Odds Ratios (OR), and Multiple Logistic Regres-
sion (MLR) were used to determine the presence and strength of associations between demographics and TM
utilisation.
Ethical approval and consent to participate. Permission to carry out the study was sought from rel-
evant authorities that are Provincial Medical Director for Matabeleland South, District Medical Officer for Bulil-
ima and National University of Science and Technology, particularly the Department of Environmental Science
and Health. Moreover, the research abides by the Nuremberg code and principles stated in the Helsinki Declara-
tion for the safety of participants involved in the s tudy46. Written consent was obtained from all the respondents
who participated in the study. Permission was sought from parents of adolescents who were less than 18 years of
age, and there were also required to assent to the study.
Results
Response rate and demographics characteristics of women. Out of the targeted 185 women, 177
responded to a pre-tested questionnaire presenting a response rate of 96%. Some of the women had left their
places of residence and could not be obtained. However, a response rate of 96% was considered sufficient by
the researchers to make meaningful inferences. The majority of women were having a partner 132 (74.6%), and
139 (78.5%) are Christians, while 110 (62.2%) are unemployed. Also, the results show that only one woman was
within the age of 50–54, as indicated in Table 1:
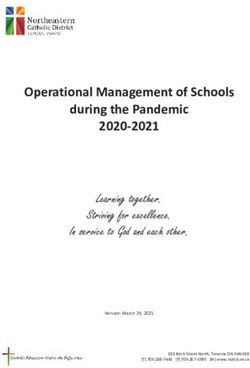
Traditional medicine used during antenatal. The majority of individuals used holy water and an
unknown type of traditional medicine, while ten women used only one type of traditional medicine. Fig. 2 and
Table 2 show different types of TMs used by women.
Prevalence and safety perception of traditional medicine use. The prevalence of TM use was 50
(28.3%) during pregnancy, and also a more significant number of women use traditional medicines during their
third trimester. Table 3 clearly shows prevalence, safety, and other variables of traditional medicines utilisation
pattern.
Scientific Reports | (2021) 11:6822 | https://doi.org/10.1038/s41598-021-86282-3 4
Vol:.(1234567890)www.nature.com/scientificreports/
Tradional Medicine Used in Pregnancy
10 10
frequency
4
3 2 2 2 2 2 1 1 1 1 1 1 1 1 1 1 1 1 1
pl ies
le alyp bela
ild oil
c
ha l
ga ld at
M c
a
Sn no r
El lo t ke
So hal est
Do rot ark
ith eza
Ho nta
M ea
ug , e Vi ng
W gle n
Bu ter af
re g
ot ar e
nt s
nk b s
p Soi
Un ate
ha orn
rli
c, rli
Ha un
ul
Bo A urin
ug w
Do ey or
le
ild W bit
ffa sna
t
Sn fat t- ssi
ey err
, W tus
Ik n
ga
rli ga
ar
p dv
e
il w im
nk ect
d
ly
w
gle uc m
ep h
ac
i
k
ly
i
Ho
as
a
n
W
e
af
ee tm
Sh in
n/
W
O
p
or
th
vi l
De
Tradional Medicine used during antenatal
Figure 2. Traditional medicine used during antenatal (n = 50).
Local name Common name Scientific name Reasons for use How it is used Trimesters
Isikhukhukhu Snuggle-leaf Pouzolzia hypoleuca Wedd Fast delivery Mix with water and drink 3rd
Inkunzane Boot protectors/Devil thon Dicerocaryum species Lubricate the birth canal washing the birth canal 3rd
umphafa Buffalo thorn Ziziphus mucronata Manage breech Drinking 1,2 and 3
Ubhuzu Donkey Berry Grewia flavescens Manage breech mix its roots with water and drink 1,2 and 3
Umganu Marula Sclerocarya caffra Inyongo (fever) Drinking 1st
Roots/barks mix with water and
Isihaqa Long tail Cassia Wild garlic Cassia abbreviate Stomach pains 1st
drink
Ikhalimela For fast delivery Mix with cold water and drink 3rd
Nyeluka Water snake/fish Fast delivery Mix its skin with water and drink 3rd
Inqwatshi kababhemi Donkey Placenta Fast delivery Mix with water and drink 3rd
Ubulongwe bendlovu Elephant Dung Manage bleeding Fumigating 1,2 and 3
Chase evil spirits and manage Mix with Vaseline and massage
Ivimbela White/Red ointment 1,2 and 3
breech stomach
Manage breech and protect from
Sheep Fat Fumigating and anointing 1,2 and 3
witchcraft
Ifutha lemvu
Anointing, mix with water and
Eucalyptus oil Protect the baby from witchcraft 1,2 and 3
drinking
Take its habitat mix with water
Muzemuze Wasp Habitant Fast delivery 3rd
and drink
Isikhundla sikamvundla Hare nest Fast delivery Mix its soil with water and drink 3rd
Protect from evil spirits and
Amanzi Angcwele Holy water Drinking and bathing 1,2 and 3
witchcraft
Protect from evil spirits and
Itiye Elingcwele Holy tea Drinking and bathing 1,2 and 3
witchcraft
Inhlabathi elomthambiso Dried soil with urine Prevent from tying and witchcraft tie dried soil with urine in a cloth 1st and 3rd
Ukuchupha unyawo Footprint soil Prevent from tying and witchcraft tie soil in a cloth 1st and 3rd
Ukuzinuka Amakhwapha Smelling your armpit Prevent from vomiting Putting nose under armpit anytime
Table 2. Traditional medicine used.
Demographic characteristics and TM use. There was a strong significant association between age and
TM utilisation as older women are 13 times more likely to use TM than younger ones. Religion and parity were
associated with TM use. On the other hand, marital status, Tribe, Level of education, employment status, and
place of delivery was not associated with TM utilisation as shown in Table 1. Age is the only variable significantly
associated with the frequency of TM use during pregnancy, as indicated in Table 4.
Discussion
The study found out that most women had a partner, were Christians, and was unemployed. Most researchers that
conducted studies in Zimbabwe supports our findings as they revealed that most women attending antenatal care
in public institutions are unemployed and are in a r elationship31,32. Results indicated that older women’s likeli-
hood of using traditional medicine during pregnancy is higher than their younger counterparts. These findings
are supported by a study conducted in Taiwan, which indicates that older women are likely to use traditional,
Scientific Reports | (2021) 11:6822 | https://doi.org/10.1038/s41598-021-86282-3 5
Vol.:(0123456789)www.nature.com/scientificreports/
TM prevalence (n=177) Frequency %
Used TM 50 28.3
Did not use TM 127 71.8
Views on safety
Safe 20 11.3
Not Safe 39 22.0
Don’t Know 118 66.7
Frequency of traditional
medicine use (n = 50)
Period & type of Traditional Medicine ↓ 1–5 times 6–10 times 11 > Total
1st trimester
Holy water 0 2 3 5
Buffalo thorns 2 0 0 2
Wild Garlic/Marula 2 0 0 2
Soil/Soil with urine 1 1 0 2
Unknown 1 0 1 2
Elephant dung 1 0 0 1
Missing 0 0 0 1
2nd trimester
Holy water 0 2 3 5
Soil 0 1 0 1
Unknown 1 0 1 2
3rd trimester
Aardvark 1 0 0 1
Devil thorn/Boot protector 0 0 1 1
Donkey berries 1 0 0 1
Elephant dung 1 0 0 1
Hare nest 2 0 0 2
Holy tea 0 1 0 1
Holy water 0 3 6 9
Ikhalimeza 0 2 0 2
Ointment-Vimbela 0 0 1 1
Sheep fat and eucalyptus oil 0 0 1 1
Snuggle leaf 2 0 0 2
Soil/ Soil with urine 1 1 0 2
Unknown 2 0 5 7
Wasp habitat 1 0 0 1
Water snake 2 1 0 3
During labour
Donkey placenta 1 0 0 1
Holy water 1 0 0 1
Snuggle leaf 2 1 0 2
Soil with urine 1 0 0 1
After labour 1 0 0 1
Devil thorn/boot protectors 1 0 0 1
Unknown 1 0 0 1
Table 3. Prevalence and safety perception of traditional medicine use.
complementary medicines than their younger c ounterparts33. Findings denote that marital status, Tribe, Level of
education, employment status, and place of delivery were not significantly associated with traditional medicine
utilisation. Studies conducted in Zimbabwe concur with our findings that religion is not related to the use of
TMs during p regnancy34.
Our findings indicated that the prevalence of TM use was 28.25%. Most scholars who conducted their stud-
ies on maternal health and traditional medicine use in Sub-Saharan countries (Zimbabwe 52%, Nigeria 68%,
Mali 80%, South Africa 55–93.6%, Mali 80%, Tanzania 55%) contradicts with our findings as they note that
the prevalence ranges from 52 to 80%29,35–39. Even though other scholars contradict our findings, multinational
studies conducted in Europe, Australia, South, and North America are aligned with our results as they revealed
a prevalence of 28.9% use herbal medicine during p regnancy7.
Scientific Reports | (2021) 11:6822 | https://doi.org/10.1038/s41598-021-86282-3 6
Vol:.(1234567890)www.nature.com/scientificreports/
Variable (n = 50) 1–5 times 6> Fisher`s exact MLR-OR MLR-95% CI MLR P-value
Age
15–19 0 (0.0) 5 (20.8) 1 ***
20–24 4 (15.4) 3 (12.5) 2.25 0.15–34.00 0.59
25–29 4 (15.4) 5 (20.8) 3.75 0.27–51.37 0.99
30–34 4 (15.4) 4 (16.7) 0.026 3 0.21–42.62 0.81
35–39 4 (15.4) 5 (20.8) 3.75 0.27–51.37 0.99
40–44 7 (26.9) 0 (0.0) 1
45–49 3 (11.5) 1 (4.2) 1
50–54 0 1 (4.2) 1
Marital status
Single 1 (3.9) 6 (25.0) ***
In a relationship 5 (19.2) 9 (37.5) 0.30 0.28–3.25 0.322
Married 12 (46.2) 6 (25.0) 0.08 0.01–0.86 0.037
0.057
Widowed 4 (15.4) 1 (4.2) 0.04 0.01–0.88 0.041
Divorced 2 (7.7) 0 (0.0) 1
Cohabiting 2 (7.7) 2 (8.3) 0.17 0.01–2.98 0.097
Tribe
Ndebele 8 (30.7) 10 (41.7) ***
Shona 2 (7.7) 2 (8.3) 0.80 0.09–7.00 0.840
Kalanga 13 (50.0) 11 (45.8) 0.910 0.68 0.20–2.31 0.534
Tonga 1 (3.9) 0 (0.0) 1 0.03–5.25 0.485
Other 2 (7.7) 1 (4.2) 0.40 0.49–3.18 0.638
Religion
Christian 16 (61.5) 19 (79.2) ***
Traditional 9 (34.6) 5 (20.8) 0.278 0.47 0.13–1.68 0.245
None 1 (3.9) 0 (0.0) 1
Level of education
Primary 5 (19.2) 8 (33.3) ***
O’level 11 (42.3) 13 (54.2) 0.74 0.19–2.92 0.666
A`level 6 (23.1) 2 (8.3) 0.308 0.21 0.03–1.47 0.115
Tertiary 1 (3.9) 0 (0.0) 1
Never attended school 3 (11.6) 1 (4.2) 0.21 0.02–2.60 0.223
Employment status
Employed 4 (15.4) 8 (33.3) ***
Self Employed 7 (26.9) 3 (12.5) 0.237 0.21 0.04–1.31 0.095
Unemployed 15 (57.7) 13 (54.2) 0.43 0.11–1.78 0.246
Place of delivery
Hospital 15 (57.7) 17 (70.8) ***
0.388
Home 11 (42.3) 7 (29.2) 0.56 0.17–1.82 0.336
First child
Yes 3 (11.5) 3 (12.5) ***
1.000
No 23 (88.5) 21 (87.5) 0.91 0.166–5.03 0.917
Parity
1 3 (11.5) 3 (12.5) ***
2–5 19 (73.1) 20 (83.3) 0.515 1.03 0.16–6.82 0.870
6≥ 4 (15.4) 1 (4.2) 0.25 0.02–3.77 0.317
Table 4. Demographics and frequency of TM use. *** Reference group.
Women revealed in our study that they use several TMs to induce and shorten labour, these include
isikhukhukhu (Snuggle-lea: Pouzolzia hypoleuca Wedd), and inkunzane (Boot protectors/devil thorn; Dicero-
caryum species). Other scholars who conducted their studies in Zimbabwe concur with our results as they indicate
that Snuggle-lea (Pouzolzia hypoleuca Wedd) was used to induce l abour9,11. It is highlighted in this study that the
majority of individuals were using holy water and an unknown type of traditional medicine. These results are in
line with a study conducted by Mureyi29, that indicated holy water as a common TM used. In addition, scholars
have noted that several herbs and their compounds are used during pregnancy are unknown40–42.
In Zimbabwe the Traditional health system is recognised and plays an important role in ensuring services
are available to those that need them43. In pursuance of SDG (3), there is a need to ensure that utilization of
Scientific Reports | (2021) 11:6822 | https://doi.org/10.1038/s41598-021-86282-3 7
Vol.:(0123456789)www.nature.com/scientificreports/
traditional medicines leads to outcomes that do not jeopardise progress towards attaining this specific goal on
maternal health44,45.
Limitations
This study cannot be generalised to the entire country since the study population was rural-based and can be
affected by recall bias even though women recruited gave birth during January-December 2019. Above all, the
research was not funded, and as such, there could have been a need for a substantial cohort to make meaningful
inferences. Authors are also involved in a project that intends to explore maternal complications and TM use
and find the active ingredient of TM used by women during antenatal care.
Conclusion
Women indeed used traditional medicine for different purposes during pregnancy, and the likelihood of older
women to use traditional medicines was higher than in young women. Most dominant traditional remedies were
used in the last trimester to quicken delivery by women. TM utilisation plays a significant role in pregnancy;
therefore, there is a need that particular attention is paid to it and possibly more research to be conducted to
assess its efficacy, safety as it gives a cheaper alternative to women who might not afford to access conventional
modern health services.
Received: 14 August 2020; Accepted: 12 March 2021
References
1. World Health Organization & UNICEF. (Geneva: World Health Organization, 2015).
2. Lawn, J. E., Blencowe, H., Kinney, M. V., Bianchi, F. & Graham, W. J. Evidence to inform the future for maternal and newborn
health. Best Pract. Res. Clin. Obstet. Gynaecol. 36, 169–183 (2016).
3. Koblinsky, M. A. Reducing Maternal Mortality: Learning from Bolivia, China, Egypt, Honduras, Indonesia, Jamaica and Zimbabwe
(The World Bank, Geneva, 2003).
4. Dunlop, D. W. Alternatives to “modern” health delivery systems in Africa: Public policy issues of traditional health systems. Soc.
Sci. Med. 1967(9), 581–586 (1975).
5. Nunu, W. N., Makhado, L., Mabunda, J. T. & Lebese, R. T. Strategies to facilitate safe sexual practices in adolescents through
integrated health systems in selected districts of Zimbabwe: A mixed method study protocol. Reprod. Health 17, 20 (2020).
6. Doctor, H. V., Nkhana-Salimu, S. & Abdulsalam-Anibilowo, M. Health facility delivery in sub-Saharan Africa: Successes, chal-
lenges, and implications for the 2030 development agenda. BMC Public Health 18, 765 (2018).
7. Kennedy, D. A., Lupattelli, A., Koren, G. & Nordeng, H. Herbal medicine use in pregnancy: Results of a multinational study. BMC
Complement. Altern. Med. 13, 355 (2013).
8. Schunder-Tatzber, S. European Information Center for Complementary and Alternative Medicine (EICCAM) gestartet. Schweiz-
erische Zeitschrift für Ganzheitsmedizin/Swiss J. Integr. Med. 22, 90–90 (2010).
9. Panganai, T. & Shumba, P. The African Pitocin-a midwife’s dilemma: The perception of women on the use of herbs in pregnancy
and labour in Zimbabwe, Gweru. Pan Afr. Med. J. 25 (2016).
10. Dika, H. I., Dismas, M., Iddi, S. & Rumanyika, R. Prevalent use of herbs for reduction of labour duration in Mwanza, Tanzania:
Are obstetricians aware? Tanzania J. Health Res. 19 (2017).
11. Chamisa, J. A. Zimbabwean Ndebele Perspectives on Alternative Modes of Child Birth (University of South Africa, Pretoria, 2013).
12. Varga, C. A. & Veale, D. Isihlambezo: Utilization patterns and potential health effects of pregnancy-related traditional herbal
medicine. Soc. Sci. Med. 44, 911–924 (1997).
13. Rahman, A. A., Sulaiman, S. A., Ahmad, Z., Daud, W. N. W. & Hamid, A. M. Prevalence and pattern of use of herbal medicines
during pregnancy in Tumpat district, Kelantan. Malays. J. Med. Sci. MJMS 15, 40 (2008).
14. Nyeko, R., Tumwesigye, N. M. & Halage, A. A. Prevalence and factors associated with use of herbal medicines during pregnancy
among women attending postnatal clinics in Gulu district, Northern Uganda. BMC Pregnancy Childbirth 16, 296 (2016).
15. Choguya, N. Z. Traditional birth attendants and policy ambivalence in Zimbabwe. J. Anthropol. 2014 (2014).
16. Muchabaiwa, L., Mazambani, D., Chigusiwa, L., Bindu, S. & Mudavanhu, V. Determinants of maternal healthcare utilization in
Zimbabwe. Int J Econ. Sci. Appl. Res. 5, 145–162 (2012).
17. Ensor, T. & Cooper, S. Overcoming barriers to health service access: influencing the demand side. Health Policy Plan. 19, 69–79
(2004).
18. Nunu, W. N., Ndlovu, V., Maviza, A., Moyo, M. & Dube, O. Factors associated with home births in a selected ward in Mberengwa
District, Zimbabwe. Midwifery 68, 15–22 (2019).
19. Mposhi, A., Manyeruke, C. & Hamauswa, S. The importance of patenting traditional medicines in Africa: the case of Zimbabwe.
Int. J. Human. Soc. Sci. 3, 236–246 (2013).
20. Kazembe, T. Traditional medicine in Zimbabwe. Rose + Croix J. 4, 55–72 (2007).
21. Munjanja, S. P., Nystrom, L., Nyandoro, M. & Magwali, T. Ministry of Health and Child Welfare. Zimba. Matern. Perinat. Mortal.
Study 2009 (2007).
22. Magadi, M. A., Agwanda, A. O. & Obare, F. O. A comparative analysis of the use of maternal health services between teenagers
and older mothers in sub-Saharan Africa: Evidence from Demographic and Health Surveys (DHS). Soc. Sci. Med. 64, 1311–1325
(2007).
23. Chandramohan, D., Cutts, F. & Millard, P. The effect of stay in a maternity waiting home on perinatal mortality in rural Zimbabwe.
J. Trop. Med. Hyg. 98, 261 (1995).
24. Ekor, M. The growing use of herbal medicines: Issues relating to adverse reactions and challenges in monitoring safety. Front.
Pharmacol. 4, 177 (2014).
25. Mudyarabikwa, O. & Mbengwa, A. Distribution of public sector health workers in Zimbabwe: a challenge for equity in health.
(EQUINET Discussion paper 34. Harare: EQUINET, 2006).
26. Dube, E. Environmental challenges posed by veld fires in fragile regions: The case of the Bulilima and Mangwe districts in southern
Zimbabwe. Jàmbá J. Disaster Risk Stud. 7 (2015).
27. David, R. & Dube, A. An assessment of health information management infrastructures for communication in the Matabeleland
South region border-line health institutions in Zimbabwe. J. Health Inform. Africa 1 (2013).
28. Agency, Z. N. S. Zimbabwe Population Census, 2012 (Zimbabwe National Statistics Agency, Harare, 2012).
29. Mureyi, D. D., Monera, T. G. & Maponga, C. C. Prevalence and patterns of prenatal use of traditional medicine among women at
selected harare clinics: A cross-sectional study. BMC Complement. Altern. Med. 12, 164 (2012).
Scientific Reports | (2021) 11:6822 | https://doi.org/10.1038/s41598-021-86282-3 8
Vol:.(1234567890)www.nature.com/scientificreports/
30. Sedgwick, P. Cross sectional studies: advantages and disadvantages. BMJ 348 (2014).
31. Muti, M., Tshimanga, M., Notion, G. T., Bangure, D. & Chonzi, P. Prevalence of pregnancy induced hypertension and pregnancy
outcomes among women seeking maternity services in Harare, Zimbabwe. BMC Cardiovasc. Disorders 15, 111 (2015).
32. Moyo, W. & Mbizvo, M. T. Desire for a future pregnancy among women in Zimbabwe in relation to their self-perceived risk of
HIV infection, child mortality, and spontaneous abortion. AIDS Behav. 8, 9–15 (2004).
33. Yeh, H. Y. et al. Use of traditional Chinese medicine among pregnant women in Taiwan. Int. J. Gynecol. Obstet. 107, 147–150 (2009).
34. Dimene, L. et al. A cross-sectional study to determine the use of alternative medicines during pregnancy in the district hospitals
in Manicaland, Zimbabwe. Afr. Health Sci. 20, 64–72 (2020).
35. Godlove, M. J. Prevalence of herbal medicine use and associated factors among pregnant women attending antenatal clinic at Mbeya
Refferal Hospital in 2010, Muhimbili University of Health and Allied Sciences (2011).
36. Ngomane, S. & Mulaudzi, F. M. Indigenous beliefs and practices that influence the delayed attendance of antenatal clinics by women
in the Bohlabelo district in Limpopo, South Africa. Midwifery 28, 30–38 (2012).
37. Tamuno, I. Omole-Ohonsi, A., and Fadare J.(2010). Use of herbal medicine among pregnant women attending a tertiary hospital
in northern Nigeria. Int. J. Gynaecol. Obstet. 15.
38. Fakeye, T. O., Adisa, R. & Musa, I. E. Attitude and use of herbal medicines among pregnant women in Nigeria. BMC Complement.
Altern. Med. 9, 53 (2009).
39. Nergard, C. S. et al. Attitudes and use of medicinal plants during pregnancy among women at health care centers in three regions
of Mali, West-Africa. J. Ethnobiol. Ethnomed. 11, 73 (2015).
40. John, L. J. & Shantakumari, N. Herbal medicines use during pregnancy: A review from the Middle East. Oman Med. J. 30, 229
(2015).
41. Pinn, G. & Pallett, L. Herbal medicine in pregnancy. Complement. Ther. Nurs. Midwifery 8, 77–80 (2002).
42. Van der Kooi, R. & Theobald, S. Traditional medicine in late pregnancy and labour: Perceptions of Kgaba remedies amongst the
Tswana in South Africa. Afr. J. Tradit. Complement. Altern. Med. 3, 11–22 (2006).
43. Mafuva, C. & Marima-Matarira, H. T. Towards professionalization of traditional medicine in Zimbabwe: A comparative analysis
to the South African policy on traditional medicine and the Indian Ayurvedic system. Int. J. Herb. Med. 2, 154–161 (2014).
44. Savelyeva, T. et al. SDG3–Good Health and Wellbeing: Re-Calibrating the SDG Agenda: Concise Guides to the United Nations
Sustainable Development Goals (2019).
45. Budhathoki, S. S. et al. The potential of health literacy to address the health related UN sustainable development goal 3 (SDG3) in
Nepal: A rapid review. BMC Health Serv. Res. 17, 237 (2017).
46. Zion, D., Gillam, L. & Loff, B. The Declaration of Helsinki, CIOMS and the ethics of research on vulnerable populations. Nat. Med.
6, 615 (2000).
Author contributions
N.M., together with W.N.N. conceptualised the research idea. N.M. crafted objectives, developed the methodol-
ogy and data collection tools. N.M. further went on to collect data together. W.N.N. coordinated the research
process and helped in drafting the manuscript with N.M. N.M. translated the data collection tools into Local
Language (Isi Ndebele) and captured the data into EPI DATA and cleaned it in preparation for analysis. N.S.
coded the data and performed data analysis on STATA. N.K. produced study area map. All the authors read and
approved the final manuscript.
Competing interests
The authors declare no competing interests.
Additional information
Correspondence and requests for materials should be addressed to N.M.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and
institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International
License, which permits use, sharing, adaptation, distribution and reproduction in any medium or
format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the
Creative Commons licence, and indicate if changes were made. The images or other third party material in this
article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the
material. If material is not included in the article’s Creative Commons licence and your intended use is not
permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from
the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
© The Author(s) 2021
Scientific Reports | (2021) 11:6822 | https://doi.org/10.1038/s41598-021-86282-3 9
Vol.:(0123456789)You can also read