Food and Nutrition Policy and Action Plan for Malta 2015 - 2020 - Health Promotion and Disease Prevention Directorate
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Food and Nutrition Policy
and Action Plan for Malta
2015 - 2020
Health Promotion and Disease Prevention Directorate
Parliamentary Secretariat for Health
September 2014
1
2
Foreward
The Maltese Government and in particular the Parliamentary
Secretariat for Health, is committed to continuously improving the
health and wellbeing of the Maltese population
The global burden from unhealthy diets is a major issue that is reflected
in high morbidity and mortality. The effects of unhealthy diets range
from chronic under nutrition to overweight and obesity. Policies to
tackle this disease burden have been developed globally and at the European level, including
the Vienna Declaration on Nutrition and Noncommunicable Diseass in the context of Health
2020 (2013), the European Charter on Counteracting Obesity (2006), the Action Plan for the
Implementation of the European Strategy for the Prevention and Control of Noncommunicable
Disease 2012 - 2016, the Health 2020 framework (2012) and the EU Action Plan on Childhood
Obesity 2014-2020.
The World Health Organisation has developed an updated European Food and Nutrition
Action Plan 2015-2020 which proposes a number of measures developed through a
consultative process within the WHO European Region.
This National Food and Nutrition Policy and Action Plan which covers the period 2015-2020
was developed by an intersectoral working group that set out to identify priority action areas in
order to address the main public health challenges facing the Maltese Nation in the area of
nutrition and food security. The whole-of-government and the whole of society approach has
been taken in order to effectively coordinate policies and actions in other non-health sectors
that could have an impact on health. This Policy and Action Plan complements the Healthy
Weight for Life Strategy (2012), the National Cancer Plan (2011), and the Noncommunicable
Disease Control Strategy for Malta (2011) which all focus on improving dietary habits in order
to maximise health and well-being. In line with the WHO European Health Policy - Health
2020, the action plan adopts a life course approach since the impact of nutrition on health
accumulates from prenatal, foetal life continuing through early childhood, adolescence,
adulthood and old age. Recognizing the fact that social inequities have a great impact on this
public health challenge, this national policy ultimately seeks to enhance health and well-being
and reduce Malta’s burden of disease by achieving change in an equitable manner.
I would like to thank the working group and all of those who provided feedback to the
consultation document launched in February this year. I now invite and urge all institutions,
governmental and nongovernmental organisations, all stakeholders and individuals to pledge
their commitment to the implementation of this Policy and Action Plan.
Better health and well being can only be achieved through the concerted efforts of all
concerned.
Hon Mr Christopher Fearne
Parliamentary Secretary for Health
34
Preface
The burden of noncommunicable diseases is rapidly increasing
worldwide. Out of a total of 57 million deaths which occurred in the
world during 2008, 36 million (63%) were due to noncommunicable
diseases, principally cardiovascular diseases, diabetes, cancer and
chronic respiratory diseases. These deaths are projected to increase
by 15% globally between 2010 and 2020 (to 44 million deaths).
Diet is one of the major modifiable risk factors for chronic diseases.
In the WHO European Region it is estimated that seven risk factors; tobacco, alcohol, low fruit
and vegetable intake, physical inactivity, high blood pressure, high cholesterol, overweight and
obesity account for 60 % of the disease burden in Europe. Five of these are directly related to
diet. Hence, as expected, food and nutrition are considered to be one of the priority areas in
the definition of objectives, strategies and recommendations of several programmes and
policies of the World Health Organisation and the European Commission. Indeed many
countries have put food and nutrition as one of the priorities in their prevention strategies.
Factors influencing food choice are not only based upon individual preferences, but are
constrained by circumstances that are social, cultural and economical and are dependent on the
environment. These factors include biological determinants such as hunger, appetite, and taste;
economic determinants such as cost of food and individual/family income; physical
determinants such as access to food, education of the person, skills and time; social
determinants which include a complex mix of class, culture, and social context; psychological
determinants such as mood, stress and guilt and attitudes, beliefs; and knowledge about food.
Nutrition is increasingly being identified as a major modifiable determinant of chronic disease,
with scientific evidence supporting the fact that alterations in diet have strong effects, both
positive and negative, on health throughout life. It is evident that the burden being posed by
inadequate diets needs further action. Both population based approaches and individual
targeted interventions are needed, using a collaborative health-in-all polices and whole-of-
government approach involving all levels of government and relevant stakeholders. Improving
diets will require a change in the environments we live in and a policy that supports making
the healthy choice the easy choice. This is the basis for the development of the Food and
Nutrition Policy and Action Plan. For this intersectoral plan to achieve its aim and objectives,
we need coordinated action to bring about the desired changes in order to reduce the burden
from diet related conditions and improve health and well being.
I would like to thank the team who developed this policy and all the stakeholders from various
sectors who gave their input during the consultation phase and look forward to the
implementation of the actions outlined.
Dr Charmaine Gauci
Director, Health Promotion and Disease Prevention Directorate
5List of Abbreviations MSDEC-AFRD Agriculture and Fisheries Regulation Department BMI Body Mass Index COSI Childhood Obesity Surveillance Initiative DAFNE Data Food Networking DHIR Directorate for Health Information and Research EHD Environmental Health Directorate ESPAD European School Survey Project on Alcohol and Other Drugs EU European Union FAO Food and Agriculture Organisation GDP Gross Domestic Product HBSC Health Behaviour School-aged Children Survey HELP Healthy Eating Lifestyle Plan HESC Home Economics Seminar Centre HFSS High Fat, Sugar and Salt HIS Health Interview Survey HLG High Level Group (Nutrition and Physical Activity) HPDPD Health Promotion and Disease Prevention Directorate HPCDU Health Promotion and Chronic Disease Unit ICCO Intersectoral Committee to Counteract Obesity IDF International Diabetes Federation KPH Kooperattiva tal-Produtturi tal-Ħalib (Ltd.) KIM Kooperattiva ta’ min Irabbi l-Majjal (Ltd.) KMS Kunsill Malti Għall-iSports (Malta Sports Council) NEHAP National Environment and Health Action Plan MCCAA Malta Competition and Consumer Affairs Authority MEDE Ministry of Education and Employment MEPA Malta Environment and Planning Authority MEH Ministry for Energy and Health MFH Ministry for Health MHEC Ministry for Health, The Elderly and Community Care MRA Malta Resources Authority MRRA Ministry for Resources and Rural Affairs MSDEC-RDAD Rural Development and Aquaculture Department NOIS National Obstetric Information System NSO National Statistics Office WASH World Action on Salt and Health WCMP Water Catchment Management Plan WHA World Health Assembly WHO World Health Organisation WSC Water Services Corporation 6
List of Contributors
Agriculture, MSDEC-AGR
Ms. Maria Carla Ciscaldi
Mr. Justin Zahra
Health Promotion and Disease Prevention Directorate, MEH
Dr. Mariella Borg Buontempo
Dr Ray Busuttil
Dr Charmaine Gauci
Ms Petra Mallia
Ms Lucienne Pace
Health Information and Research Directorate, MEH
Dr. Neville Calleja
Ms. Dorothy Gauci
Malta Environment & Planning Authority
Mr. Kevin Mercieca
Mr. Alvin Spiteri Debono
Malta Competition and Consumers Affairs Authority
Ms. Ingrid Busuttil
Mr. Tristan Camilleri
Mr. Mark A. Cassar
Malta Sports Council
Ms. Maria Mifsud Bonnici
Mr. Robert Portelli
Mr. Bernard Vassallo
National Statistics Office
Mr. Etienne Caruana
Ms. Mary Rose Debono
Ministry for Sustainable Development, the Environment and Climate Change
Dr. Marguerite Camilleri
Sedqa (Aġenzija), Foundation for Social Welfare Services
Ms. Sina Bugeja
Mr. Manuel Mangani
WasteServ Malta Ltd.
Ms. Henriette Putzulu Caruana
Water Services Corporation
Ms. Paula Grech Bonnici
Ing. Stephen Galea St. John
Dr. Ing. Paul R. Micallef
7World Health Organisation Dr. Joao Breda (WHO, EURO Regional Office for Europe, Copenhagen)) Dr. Godfrey Xuereb (WHO, Headquarters, Geneva) Editors Dr Mariella Borg Buontempo Dr Ray Busuttil Dr Charmaine Gauci 8
Table of Contents
Chapter 1 - Background 13
Chapter 2 – Situation Analysis 19
2.1. – Epidemiological Situation 20
2.1.1. – Overweight and obesity 20
2.1.2. – Dietary habits of the Maltese population 23
2.1.3. – Diet-related non-communicable diseases 27
2.14. – Mortality data for non-communicable diseases 28
2.1.5. – Micronutrient deficiencies 29
2.2. – Current strategies and legislative measures 29
2.2.1. – The Food and Nutrition Policy for Malta(1990) 29
2.2.2. – National nutrient goals and dietary guidelines 30
2.2.3. – Changes in the food supply over the years 30
2.2.4. – National legislation, policies, strategies, committees and groups
with a focus on diet, physical activity and health 31
2.3. – Current initiatives in food and nutrition in Malta 32
2.4. – Sectors involved in the area of food and nutrition 32
2.4.1. – Ministry responsible for Health 33
2.4.2. – Ministry responsible for Education 34
2.4.3. – The Media 34
2.4.4. – Ministry responsible for the Environment 35
2.4.5. – Ministry responsible for Agriculture and Fisheries 36
2.4.6. – Ministry responsible for Social Affairs 37
2.4.7. – Ministry responsible for Home Affairs and National Security 38
Chapter 3 – Guiding Principles 39
3.1. – Whole of government approach 40
3.1.1. – Trade and marketing policies 40
3.1.2. – Fiscal policies 40
3.1.3. – Climate change 41
3.2. – Focus on Equity 42
93.3. – Life course approach 43
3.3.1. – Pregnancy and breastfeeding 43
3.3.2. – Healthy eating during school years 43
3.3.3. – Healthy eating during adulthood 43
3.3.4. – Healthy ageing 44
3.4. – Strengthening health systems 44
Chapter 4 – Scope, Vision, Goals, Objectives and population nutrient goals 47
4.1. – Scope 48
4.2. – Vision 48
4.3. – Goals 48
4.4. – Objectives 48
4.5. – Population dietary and nutrient goals 49
4.6. – Timing 49
Chapter 5 – Implementation of the Policy 51
5.1. – Priority Action Areas 52
5.2. - Implementation plans for priority actions 53
5.3. – Development and Implementation of Action Plan 58
Annex 1 – Demography 61
Annex 2 – Detailed epidemiological situation 63
A2.1. – Prevalence of overweight and obesity 64
A2.2. – Dietary habits of the Maltese population 67
A2.3. – Diet-related non-communicable diseases 72
A2.4. – Mortality data for non-communicable diseases 76
A2.5. – Micronutrient deficiencies 79
Annex 3 – Current initiatives for food and nutrition in Malta 81
References 87
10CHAPTER 1
BACKGROUND
11The joint Food Agriculture Organisation and World Health Organisation (FAO/WHO)
World Declaration on Nutrition (FAO/WHO, 1992) states that ‘… access to nutritionally
adequate and safe food is a basic individual right’. It also emphasises that healthy
nutrition and food safety are vital in the prevention of a wide-range of diseases and
disorders and are prerequisites for improving health. The right to food is safeguarded in
several treaties relating to human rights. The notion of the right to food as a human right
brought with it legal responsibilities on the state and community of states to guarantee the
right to food for all. Nutritional status was defined as a ‘corner stone’ to the development
of civilisation in the United Nations Millennium Development Goals (United Nations,
2013).
Over many years, the World Health Assembly (WHA) by its adoption of a large number of
resolutions and policy documents supported national and international efforts in satisfying
the fundamental right of access to sufficient quantities of safe and healthy food. These
include:
1. The WHO Global Strategy on Diet, Physical Activity and Health (2004). This
strategy describes the responsibilities of various stakeholders (WHO, international
partners, private sector, civil society and nongovernmental organizations) to take
action to improve diet and promote physical activity for the prevention of
noncommunicable diseases. It called for a ‘balanced’ approach between individual
responsibility for lifestyle choices and societal responsibility to make the ‘healthy
choice’ the easier choice.
2. The European Charter on Counteracting Obesity (WHO, European Ministerial
Conference on Counteracting Obesity, 2006). Countries within the European
Region committed themselves to demonstrate a slow down and bring to an end the
obesity epidemic within the next 4–5 years, especially among children, and that the
obesity prevalence trends should be reversed before 2015. The Charter calls for
action beyond health education and therefore calls for changes in the physical,
political, informational and social environments to facilitate a healthy energy
balanced lifestyle. The multidisciplinary and ecological approach was a step
forward for public health policy and practice in Europe at that time.
3. The WHO European Action Plan for Food and Nutrition Policy 2007-2012 (WHO,
2007). This Action Plan focuses on addressing public health challenges in the area
of diet-related noncommunicable diseases; obesity trends in children and
adolescents; micronutrient deficiencies and foodborne diseases. It outlines six
action areas. These are: (i) supporting a healthy start; (ii) ensuring a safe, healthy
and sustainable food supply; (iii) providing comprehensive information and
education to consumers; (iv) carrying out integrated actions to address related
determinants; (v) strengthening nutrition and food safety in the health sector and,
(vi) monitoring and evaluation.
4. The 2008 Action Plan for the Global Strategy for the Prevention and Control of
Noncommunicable Diseases (WHO, 2008). This strategy gives clear action points
for countries to work towards reducing the risk factors for noncommunicable
diseases. It further underlines the need for the identification and dissemination of
information on evidence-based interventions and structures as previously
12mentioned in the 2004 WHO Global Strategy on Diet, Physical Activity and
Health.
5. The United Nations (UN) Political Declaration of the High-Level Meeting of the
General Assembly on the Prevention and Control of Noncommunicable Diseases
(UN General Assembly, 2011). This declaration expresses concern over food
security due to the various variables affecting adequate food supply and their effect
on the control and prevention of noncommunicable diseases. It also calls for the
need for immediate, coordinated and multi-sectoral efforts to address those impacts
by all relevant stakeholders.
6. The most recently adopted WHO European Health Policy Framework and
Strategy, ‘Health 2020’ (WHO, 2012). One of the main objectives of Health 2020
is to ‘improve health for all and reduce health inequalities’. Mindful of the various
factors that determine exposure and vulnerability, Health 2020 focuses on
addressing the major health challenges across the Region through tackling the
social and lifestyle determinants of health through a whole of government and
whole of society approach across the life course.
7. The Global Nutrition Policy Review (2013) provided information on whether the
countries have nutrition policies and programmes, how they are being
implemented, what the implementation coverage is, who the stakeholders are, what
the coordination mechanism is, and how the monitoring and evaluation are being
implemented. Most countries that responded to the survey had policies and
programmes that are addressing key nutrition issues, such as under nutrition,
obesity and diet-related NCDs, infant and young child feeding, and vitamin and
mineral malnutrition.
8. In July 2013 Ministers of Health of the European Region signed the Vienna
Declaration on Nutrition and Noncommunicable Diseases in the Context of Health
2020 which commits member states in the European Region to address the root
causes of obesity and diet-related noncommunicable diseases and to empower
citizens to make healthy choices.
9. The vision of the updated European Food and Nutrition Action Plan 2015-2020
which will be presented for endorsement at the Regional Committee in September
2014 is to aim for a health promoting Europe free of the preventable burden and
impact of diet-related non communicable diseases, under nutrition and
micronutrient deficiencies, premature death and avoidable disability.
In view of the dramatic rise in the levels of overweight and obesity and the worsening
trend of poor diets and low physical activity levels across large parts of Europe, the EU
began to significantly ramp up its action in this area approximately ten years ago.
1. Recognising the human suffering and the economic consequences caused by
the increasing incidence of obesity, in 2004 The Council of Ministers of the EU
invited the Commission to contribute to promoting healthy lifestyles, and to
study ways of promoting better nutrition within the European Union. In 2005
the European Commission published the Green Paper Promoting healthy diets and
13physical activity: a European dimension for the prevention of overweight, obesity
and chronic diseases.
2. In the same year the EU published the Blueprint for Action - Protection, promotion
and support of breastfeeding in Europe: a blueprint for action 2004. The Blueprint
for Action provides a framework for the development of such plans. The Blueprint
has been available to all those Governments, institutions and organizations who are
willing to work together for the protection, promotion and support of breastfeeding.
3. In order to establish a common forum for action the European Platform for
Action on Diet, Physical Activity and Health was launched in March 2005. The
Platform brings together all relevant players active at European level that are
willing to enter into binding and verifiable commitments aimed at halting and
reversing current overweight and obesity trends. The objective of the Platform
is to catalyse voluntary action across the EU by business, civil society and the
public sector working together.
4. In May 2007, the European Commission established a coherent and comprehensive
Community Strategy to address the issues of overweight and obesity, by adopting
the Strategy on Nutrition, Overweight and Obesity-related Health Issues which
focuses on action that can be taken at local, regional, national and European levels
to reduce the risks associated with poor nutrition and limited physical exercise,
while addressing the issue of inequalities across member states. It advocates a
partnership approach, and encourages action by four main groups of actors: the EU
itself, Member States, private actors, and international cooperation with the WHO.
It provides an integrated framework for action intended to contribute to reducing ill
health due to poor nutrition, overweight and obesity in the EU.
5. The Strategy launched in 2007 was evaluated in 2012 in order to assess both the
implementation process as well as its impact. The outcome of the evaluation was
that progress has been made (albeit to a varying extent) towards all of the
objectives defined in the Strategy. The measures taken were clearly steps in the
right direction, although their contribution has in most cases not led to major
changes as the levels of overweight and obesity continue to be high across the EU.
The evaluation highlighted that most of the action taken in Europe to date (both at
the EU and at the national levels) has been of a relatively soft nature, and has relied
primarily (although the extent varies by country) on information provision and
education, limited interventions in specific environments (such as schools), and
voluntary actions by the food industry and other private actors, so as to generate an
impact via a series of relatively subtle changes The argument for the introduction
of more intrusive measures was put forward. The report also highlighted that a
greater focus on the promotion of physical activity and a greater consideration of
the impact of any measures introduced on the lower socio-economic groups not to
increase social inequalities was needed.
6. The EU Action Plan on Childhood Obesity 2014-2020 was published in February
2014. Despite action at the European level to reverse the rising trend in
overweight and obesity, the proportion of the population who are overweight or
obese remains worryingly high for adults and for children and young people. The
14implications of overweight and obesity in Europe are stark: the prevalence of
obesity has more than tripled in many European countries since the 1980s
and with this rise comes a concomitant increase in rates of associated non-
communicable diseases.
In the 1980s, Malta was the first country to have a National Food and Nutrition Policy.
Although developed much before the action plan, Malta’s policy set a visionary direction
and aligned well with the First Action Plan for Food and Nutrition Policy adopted by the
World Health Organisation (EURO Region) for the period 2000-2005. The latter
emphasised the need for food and nutrition policy development to protect and promote
health and reduce the burden of food-related diseases, while contributing to socio-
economic development.
Malta highlighted the importance of preventing such diseases in the Health Vision 2000
(Malta) National HealthPolicy:
“Prevention of many of the major diseases, or their complications, such as coronary heart
disease, certain cancers, and non-insulin dependent diabetes is possible and this calls for
a shift in emphasis towards prevention and health promotion. The lifestyle risk factors of
smoking, unhealthy diets, obesity and lack of physical activity must be tackled seriously.
We must provide the environment and facilities for people to be able to make the right
choices. This requires a long-term commitment and a standardised approach to the
evaluation of health promotion initiatives.”
Major noncommunicable diseases (NCDs) are responsible for about 82% of deaths in
Malta. In 2012, cardiovascular disease was the top cause of mortality in Malta accounting
for 46.7% of all deaths (National Mortality Register, 2012). Neoplasia was the second
commonest cause of mortality in Malta accounting for 27.1% of all deaths. The published
data for Malta, through the IDF Diabetes Atlas estimate that the diabetes prevalence in
Malta is 10.14% of the adult population, representing 33,260 people in 2013 (IDF Diabetes
Atlas 2013) and the atlas forecasts a rise in prevalence to 11.6% of the Adult population,
representing 36,600 people by 2025 (IDF Diabetes Atlas, 2006).
Currently, the majority of NCD deaths, disability and morbidity occur disproportionately
in poorer communities and are contributing to widening health gaps between and within
countries. This results in enormous human suffering and produces an increased threat to
the socio-economic development of many countries. Poor nutrition still accounts for an
important percentage of the total disease burden.
Poor diets and sedentary lifestyles are contributing to an increase of obesity in most
countries of the WHO European region, with lower socio-economic groups bearing the
biggest burden. Following the documentation of local data on obesity among the Maltese
population, international scientific and health agencies such as the World Health
Organisation and the International Obesity Task Force have reiterated that Maltese
children and adults are amongst the heaviest both within Europe as well as globally
(WHO, 2010).
This Food and Nutrition Policy and Action Plan 2015-2020, addresses these health
challenges in order to seek to reduce mortality and morbidity and address the economic
implications of poor nutrition. The projected national health care cost attributed to obesity
15is expected to increase from €25,390,000 to €34,980,000 by 2020, if no change in the proportion of overweight and obese individuals in the population and no changes in the average health care usage takes place. However, in the scenario, where a 4.3 % reduction in obesity to normal weight category by 2020, around €3,000,000 per year could be saved as part of the health care cost being borne by the state and which is attributed to overweight and obesity (A Healthy Weight for Life: A National Strategy for Malta 2012- 2020, MHEC, 2012). Globally, acute undernutrition is still documented in areas facing food insecurity and chronic undernutrition due to micronutrient deficiencies. In Malta the latter have not been considered as a major public health challenge. However, at national level, no studies have been carried out to determine the extent of micronutrient deficiencies amongst the Maltese population. Several EU countries are now paying serious attention to iodine, iron, folic acid, vitamin D and calcium since they may significantly contribute to chronic diseases in industrialised societies with impacts among vulnerable groups including women, children, and the middle-aged and older people. An important challenge for public health is to understand the epidemiology of micronutrient deficiencies and then implement successful methods of prevention. Food insecurity is also a problem facing vulnerable groups. Indicators show that Malta’s position with regards to food security is a stable one. In response to the Rome Declaration on World Food Security and the World Food Summit Plan of Action held in 1996, Malta reported that it is not facing any problems of food security, whether in availability, stability or access to food supplies. Moreover, according to the Food and Agricultural Organization (FAO, 2010), the food deficit of undernourished people in Malta in 2006- 2008 was that of 100kcal/person/day. A review of progress since the First International Conference on Nutrition (ICN) in 1992 including the identification of the major constraints encountered in the implementation of National Plans of Action for Nutrition will take place at the Second International Conference on Nutrition which will take place in Rome in November 2014. This high- level political event will bring together all the relevant sectors (food, agriculture, health, education and social protection) to mobilise the political will and resources to improve nutrition and reach consensus around a global multi-sector nutrition framework with concrete steps to improve nutrition. The Food and Nutrition Action Plan for Malta will not address the issues of food safety, the harmful use of alcohol and physical inactivity as these issues are being dealt with in other documents. Malta has already an established comprehensive system for food safety as regulated by the Food Safety Act (2004). The National Alcohol Policy which aims to regulate alcohol consumption and minimise risk, has been formulated and is currently undergoing consultation. Through the Sports Act (2003), the Malta Sports Council was set up to promote, develop and implement programmes that promote participation in physical activity in the Maltese Islands which are available to all ages, abilities and needs. A National Sports Policy is being developed by the a Working Group appointed by the Parliamentary Secretary responsible for Sports and a Strategy for Health-Enhancing Physical Activity will be developed by the Health Promotion and Disease Prevention Directorate in 2015. 16
CHAPTER 2
SITUATION
ANALYSIS
172.1. Epidemiological Situation
2.1.1. Overweight and Obesity
Worldwide, at least 3.4 million people die each year as a result of being overweight or
obese, and an estimated 35.8 million (2.3%) of global DALYs are caused by overweight or
obesity. The worldwide prevalence of obesity has nearly doubled between 1980 and 2008.
Overweight and obesity is on the increase in the Maltese islands as well at all ages.
2.1.1.1. Children and adolescents
A cohort of children who were measured at age 7 and then at age 9 showed on average a
13% increase in the proportion of overweight and obese children along the years (Table 1).
The proportion of obese 9 year olds had increased by 9.1% while the proportion of
overweight 9 year olds had increased by 11.6% (WHO, 2012).
Children born in 2001
Age 7 Years Age 9 years Age 11 years
(2008) (2010) (2012)
Boys Girls Boys Girls Boys Girls
% overweight 8.8 16.1 17.6 16.6 22.4 23.7
% obese 17.3 13.5 26.4 23 27.8 20
% o/w +
obese 26.1 29.6 44.4 39.6 50.2 43.7
Table 1: Measured BMI trends in cohort as measured in 2008, 2010 and 2012
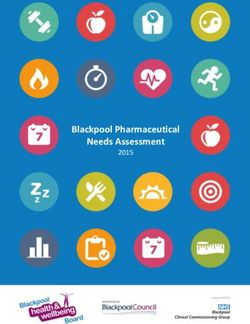
In the Health Behaviour in School Children (HBSC) Study, the body mass index (BMI) is
based on self-reported weight and height. Figure 1 shows the percentage overweight and
obesity rates by gender. This study showed that BMI amongst Maltese school children in
Malta is one of the highest in the world, with Malta ranking second to the USA for
overweight and obese children aged 11 and 13, while ranking first for children aged 15. In
comparison with current anthropometric data, these self-reported results are probably an
underestimate (HBSC, 2010).
Comparing this data to that from previous studies, one can identify increasing rates in 11
year old boys and girls and in 13 year old boys, and decreasing rates for 13 year old girls
and 15 year old boys and girls.
18Figure 1. Overweight and Obesity in 11,13 and 15 year olds (HBSC 2010)
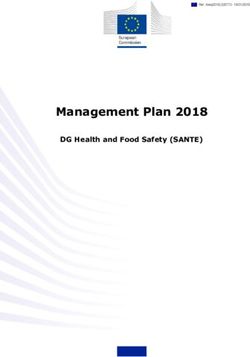
2.1.1.2. Adults
According to the European Health Interview Survey (DHIR, 2008) that covered the
population aged over 15 years, approximately 22% of the Maltese population is obese
(BMI >30 kg/m2) and a further 36% are overweight (BMI > 25 kg/m2).
50% Male Female 44.7%
40.0%
40%
28.0% 28.4%
30% 24.3%
20.6%
20%
8.4%
10%
0.7% 2.6% 2.4%
0%
=30.01
BMI Group
Figure 2: Self-reported BMI in population aged 15+, 2008
The European Health Examination Survey 2010 (pilot study) (DHIR, 2012) showed that
the percentage of the population aged 19 years and over that is obese is 29.8 % and a
further 47.2 % are overweight (Figure 2). When compared to EU member states, Malta
has the highest rate of obesity amongst adult males and the third highest rate amongst
females.
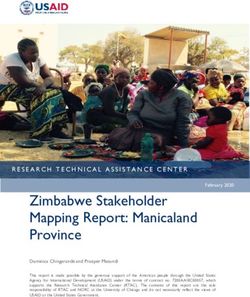
The effect of obesity reduction on the prevalence and incidence rates of a number of
diseases including cancers, cardiovascular disease, osteoarthritis, diabetes and
hypertension for Malta were studied by WHO (Webber L, Divajeva D, Marsh T, et al
192014). These projections indicate that more males tend to be overweight over the age of 25
years. Obesity is predicted to increase in the younger age groups by 2030, but to fall in
other age groups. When the proportion of obese persons in the population loose weight, it
is expected that the overweight category will increase. According to this modelling study,
there would be a substantial increase in number of cases of noncommunicable diseases
which could be avoided between 2010 and 2030 per 100 000 of the Maltese population in
the case of a 1% (scenario 1) or a 5% (scenario 2) decrease in obesity (Figures 3,4). The
incidence /prevalence reduction was highest for hypertension.
Cumulative incidence cases avoided between 2010 and 2030 per
100 000 of the population by scenario 1 and 2 Malta
4500
Incidence cases avoided
4000
3500
3000
2500
2000
1500
1000
500
0
Cancers CHD & Stroke Osteoarthritis Diabetes Hypertension
Scenario 1 34 228 8 136 372
Scenario 2 165 992 22 619 1431
Figure 3 Effect of obesity reduction by 1% (scenario 1) and by 5% (scenario 2) on cumulative
incidence cases avoided (supplementary analysis)
Prevalence cases avoided in 2030 per 100 000 of the population by
scenario 1 and 2 Malta
2500
Prevalence cases avoided
2000
1500
1000
500
0
Cancers CHD & Stroke Osteoarthritis Diabetes Hypertension
Scenario 1 9 51 2 71 296
Scenario 2 59 225 11 344 997
Figure 4 Effect of obesity reduction by 1% (scenario 1) and by 5% (scenario 2) on prevalence
cases avoided (supplementary analysis)
202.1.2. Dietary habits of the Maltese Population
The traditional Maltese cuisine has been primarily Mediterranean, based on seasonal
agricultural products and seafood and with strong Sicilian influence. Over time and with
advancing development, there has been a rapid shift from a state of food shortage to one of
affluence, based in a cultural context where the identity is no longer Mediterranean but has
a strong Anglo-Saxon influence. (Tessier and Gerber 2005).
The eating patterns of the Maltese population were reprted by Dr Mary Bellizzi in 1993.
The data was derived from the 1989 -1990 Household Budgetary Survey and can be seen
in Table 2.
1. The staple cereal available in Malta was wheat, predominantly processed as bread
(78 %); followed by pasta (11 %).
2. Beef and pork were the most popular types of meat followed by poultry and rabbit;
however processed meats (ham, luncheon meat and bacon) contributed up to 60 %
of all pork purchased.
3. Fish consumption was low compared to meat with the average consumption per
capita of 52 grams.
4. Maltese consumed an average of five to six eggs (per person) in a week.
5. Nearly two-fifths of the cheese consumed was the high fat Cheddar cheese as it
was inexpensive compared with the other cheeses. Low-fat milk was not available
in the market in the 1980’s.
6. The proportion of energy taken from fruit and vegetables in 1986-1988 was 6 %.
7. Sugar supply in Malta was one of the highest in Europe and is the highest in the
European Mediterranean region. It was estimated that Malta was the second highest
per capita consumer of soft drinks.
8. Fats provided 16.2 % of total energy intake (excluding alcohol) in 1986-88; of
which 13.3 % came from vegetable oils and margarine and 3 % from animal fats.
Table 2: Eating Patterns in the 1980’s as reported by Dr. Mary Bellizzi (1993)
2.1.2.1. Adolescents (11-15 years) (HBSC, 2010)
Breakfast
Average daily breakfast consumption reduces with age from an average of 55% in those
aged 11 to an average of 45% in those aged 15. This is similar to the trends observed in
the HBSC average. In 2010 consumption was greater in boys when compared to girls in
the older age groups of 13 and 15 while consumption was greater in girls in the younger
age group. For all three age categories, the proportion of Maltese children consuming
breakfast daily is lower than the HBSC average for 2010.
Fruit and Vegetables
Amongst girls, daily fruit consumption remains relatively constant throughout the three
age groups at approximately 42%. Amongst boys there is a sharp decline in the 15 year old
age group with only 25% consuming fruit daily when compared to 40% in the younger
21categories. There was an increase in consumption of fruits in girls aged 15 and an increase
in 13 year olds boys since 2006.
When compared to the HBSC average for 2010, Maltese girls aged 13 and 15 consume
fruit more often while boys aged 11 and 13 are also above the average. The trends
observed for the data from Malta is similar to the trend in the HBSC average where we see
a decline with age and a difference between genders with girls consuming fruit more than
boys.
Girls report that they consume
Food Consumption vegetables on a daily basis
11yrs 13yrs 15yrs adults more often than boys across
(%) (%) (%) (%)
all ages. On average 21 % of
Breakfast 55 43 45
the girls and 16 % of the boys
daily fruit 42 41 34 74 consume vegetables on a daily
daily vegetables 16 15 15 51 basis. This difference seems to
daily soft drinks 44 44 49 21 increase as age increases. As
never soft drinks 57 age increases, more girls tend
cereals >3x/wk 28 to consume vegetables on a
daily basis. However, there is
rice/pasta 30
a slight decrease as age
fried potatoes 32 increases in boys. Across all
slices bread/day 2 ages, Malta is below the
fish 1-2x/wk 52 HBSC 2010 average. This
chicken/rabbit 1-2x/wk 72 difference increases as the age
meat 1-2x/wk 62 increases.
no cheese 35
Soft Drinks
no low fat cheese 40
cheese 1-2x/wk 65 Amongst boys; daily soft
veg. oil in food prep 53 drink consumption increases
olive oil on bread 39 with age from 44% in 11 year
sweets 1-2x/wk 26 olds to 49% in 15 year olds.
never sweets 38
On the other hand, amongst
sweet pastries 1-
girls consumption decreases
33 with age from 44% in 11 year
2x/wk
never sweet pastries 31 olds to 34% in 15 year olds. In
add salt with cooking 47 2010 the daily consumption of
soft drinks did not vary
never add salt 35
amongst genders in 11 year
add salt at table 58 olds but by the age of 13 and
always add salt at more it does vary such that by
24
table
the age of 15, boys consume
more soft drinks when
compared to girls.
The proportion consuming soft drinks daily is well above the HBSC average for all three
age groups. As age increases the HBSC average for soft drink consumption increases and
the percentage consumption is greater amongst boys when compared to girls in all age
groups. This is the same pattern observed in the data for Malta. The trend since 2002
22shows an increased softy drinks consumption in 11 year olds, 13 year old girls and 15 year
old boys.
2.1.2.2. Adults
Data on dietary habits of the Maltese population aged 16 and over is available from two
surveys: the 2002 National Health Interview Survey and the 2008 European Health
Interview Survey. The former contained questions on dietary intake of starchy food, fish,
saturated fat, sugar and sugary drinks, and salt, while the latter provided data on fruit and
vegetable consumption.
Starchy Food (2002)
The consumption of starchy foods on three or more days a week was generally low.
Approximately 28% consumed cereals three or more days a week, 30% consumed rice or
pasta, 10% consumed fried potatoes and 32% consumed other potato products. Maltese
bread remained the most common type of bread consumed with an average of 2 slices per
day while brown bread is the bread least consumed by the population.
Fish (2002)
Fish was most commonly eaten one to two days per week at 51.8% with no difference
between males and females. The results showed that the consumption of fish increased
with advancing age. Education did not appear to play a significant role in the consumption
of fish in the population.
Protein and Fat Intake (2002)
Chicken and rabbit consumption was similar in both genders with 71.8% of the population
reporting eating these products on one to two days a week. There were no differences in
consumption by age and educational level. Meat was consumed on one to two days a
week by 62% of the population. There is an inverse association between the frequency in
the consumption of meat and meat products and educational level.
Thirty five per cent of the population reported never eating cheese while 40% never
consumed low fat cheese. Amongst those who ate cheese or low fat cheese, it was
consumed on one to two days a week. Educational level did not appear to play a major role
in the consumption of cheese or low fat cheese by the population.
Contrasting habits were noted in the use of oils/fats for cooking and those used on bread.
Other vegetable oils were the most common oils used for food preparation at 53% and
olive oil was the most commonly used oil/fat on bread at 38.7%. The use of olive oil and
other vegetable oils varies by age with the use of olive oil reducing as age increases and
the use of other vegetable oils increasing with older age groups.
Sugar (2002)
38% of respondents reported never consuming sweets while 26% said they consumed
sweets on one to two days a week. 33.4% of the population said they consumed sweet
pastries on one to two days a week while another 31% said they never consumed sweet
23pastries. The highest daily consumption was for the younger age groups. Daily consumption rose again in those aged 75 years and over. 57% reported never consuming sugared soft drinks while 21% consumed such drinks daily. The highest daily consumption was for the younger population aged 15-24 years where 50% of males and 22% of females in this age group consumed sugared soft drinks daily. Similar to the pattern observed with sweets and sweet pastries, while consumption of sugared soft drinks decreased with age, it was noted to increase again in those aged 75 years and over. Educational level seems to play a significant role in the consumption of sugared drinks; in fact those who consumed sugared soft drinks daily had a significantly lower number of years of completed education. Salt (2002) 47 % of the population ‘almost always add salt’ while cooking and 35% reported never adding salt or ‘use low salt alternatives’. 58% never add salt at the table or ‘use a salt alternative’ while 24% always add salt at the table. Education was not significantly associated with habits related to salt usage. Fruit and Vegetables (2008) 74% of adults reported consuming fruits at least once a day while 51% reported consuming vegetables at least once a day. Daily fruit and vegetable consumption was highest amongst females and increased with age. Amongst those aged 45 years and over, approximately 80% reported consuming fruit daily while approximately 56% report consuming vegetables daily. 2.1.2.3. Food Consumption Surveys The first Food Consumption Survey which attempted to look at foods consumed by the adult population was carried out by the Malta Standards Authority (2010). This showed that the Maltese still have poor eating habits that can be further enhanced for better health attainment. It determined that Maltese people still consume high amounts of sweets and sugary foods and that consumption of vegetables was low. A common limitation to all of the above-mentioned food consumption survey reports is the lack of adequate information on the quantity of food (grams) and drink (litres) consumed by the targeted population. Hence, the dire need for Malta to set up a methodologically sound scientific food consumption survey to be carried out periodically across all age groups so as to monitor nutrition trends and evaluate interventions in the area of nutrition. A National Food Consumption Survey aimed at determining the food consumption patterns of the Maltese population aged 7 years and over is being carried out by the Health Promotion and Disease Prevention Directorate. The preparatory work and piloting of the study will be carried out in 2014 while the actual fieldwork will be carried out during 2015/2016. In addition to food consumption, the study will also look into food consumption frequency, engagement in physical activity, salt intake and urinary sodium excretion will be estimated in a sub-sample of the study population. 24
2.1.3. Diet-related Noncommunicable Diseases
Noncommunicable diseases account for nearly 86% of deaths and 77% of the disease
burden in the WHO European Region, putting increasing strain on health systems,
economic development and the wellbeing of a large part of the population (Action Plan for
Implementation of the European Strategy for the Prevention and Control of
Noncommunicable Diseases 2012 – 2016, WHO, 2012).
This section provides an outline of the epidemiological data for hypertension, diabetes,
hypercholesterolaemia, cardiovascular disease and some specific cancers for the Maltese
population.
2.1.3.1. Hypertension
The self-reported life time prevalence of hypertension in the adult population is 22%
(EHIS 2008). Prevalence increases with age in both genders, with half the population
reporting hypertension at age 75 years and over. Females have a slightly higher
prevalence than males, though the difference is not significant.
The pilot European Health Examination Survey (2010), reported normal blood pressure in
67.9 % participants. There were 23.5% with stage 1 hypertension (Systolic ≥140-159
mmHg or Diastolic ≥90-99 mmHg) and a further 8.5% with stage 2 hypertension (Systolic
≤160 mmHg or Diastolic ≤100mmHg) (MHEC, 2012).
2.1.3.2. Diabetes
The self-reported life time prevalence of diabetes among the Maltese population as
reported in the European Health Interview Survey (EHIS, 2008) was 8.3%. Estimates by
the International Diabetes Federation in 2006 put the prevalence rate at 9.8% of the adult
population (IDF Diabetes Atlas, 2006) Prevalence increases with age in both genders. The
prevalence rate doubles in the age group 55 to 64 years when compared to the age group
45 to 54 years.
The European Health Examination Survey (2010) estimated the prevalence rate amongst
the population aged 20-79 years to be 10.1% with a higher rate in women (10.7%) than
men (9%) (EHES, 2010). Estimates by the International Diabetes Federation in 2013 put
the prevalence rate at 10.14% of the adult population (IDF Diabetes Atlas, 2013).
2.1.3.3. Hypercholesterolaemia
According to self-reported data on hypercholesterolemia from the National Health
Interview Survey 2002, the self-reported life time prevalence of hypercholesterolemia in
the population is 8.9%. According to the EHES (2010), 37.5 % had low risk total serum
cholesterol level (≤ 5.00mmol/l); 40 % higher risk total serum cholesterol level (>5.00 –
6.18 mmol/l) and 22 % a high risk total serum cholesterol level (>6.18 mmol/l)(MHEC,
2012).
252.1.3.4. Colorectal Cancer In 2012 the European age standardised incidence rate for colorectal cancer amongst Maltese males was approximately 60 cases per 100,000 population while for Maltese females it was 38 cases per 100,000 population (EUCAN,2012). These rates show that the incidence of colorectal cancer in Malta was very close to that of the EU-27 average. 2.1.3.5. Stomach Cancer In Malta the European age standardised incidence rate for stomach cancer amongst males was approximately 14 cases per 100,000 population while for females it was approximately 5 cases per 100,000 population (DHIR, 2012). 2.1.3.6. Liver Cancer In Malta the age standardised incidence rate for liver cancer amongst males is approximately 9 cases per 100,000 population while for females it is approximately 3 cases per 100,000 population (DHIR, 2012). 2.1.4. Mortality data for Noncommunicable Diseases Diseases of the circulatory system, namely ischaemic heart disease, stroke and heart failure are the leading causes of death accounting for 46.7% of all deaths. Despite a downward trend in mortality rates from diseases of the circulatory system, rates are higher than the average for the EU-15. 2.1.4.1. Ischaemic Heart Disease In 2012 ischaemic heart disease was the leading cause of death with a European age standardised mortality rate of 143 deaths per 100,000 population with a male to female ratio of 1.7. The age standardised mortality rate for Malta is well above the EU-15 average. This is considerably higher than the Standardised Death Rate for the EU 15 and has approached the rate of the EU 13. 2.1.4.2. Cerebrovascular Disease The age standardised death rate for cerebrovascular disease in Malta is above the EU-15 average, though the difference is not as wide as for ischaemic heart disease. In 2012 there were 41 deaths due to cerebrovascular disease per 100,000 in accounting for 8.1% of all deaths. 26
2.1.4.3. Colorectal Cancer
Colorectal cancer mortality rates for Malta do not follow a similar pattern as those of
incidence rates. While in males the mortality rate is similar to the EU-27 average, in
females the mortality rate is slightly higher than the EU average. Amongst males in 2012
there were approximately 23 deaths per 100,000 population due to colorectal cancer
compared to 24 deaths per 100,000 in Europe. On the other hand in females in 2012, there
were approximately 16 deaths due to colorectal cancer per 100,000 population in Malta
compared to 14 deaths per 100,000 in Europe.
2.1.4.4. Stomach Cancer
In 2012 the European age standardised death rate for cancer of the stomach in males was
approximately 10 deaths per 100,000 population while in females it was approximately 5
deaths per 100,000 population. Both figures are lower than the EU average.
2.1.4.5. Liver Cancer
The European age standardised death rate for diseases of the liver was 6.6 per 100,000
population. In 2012, there were 40 deaths of which 28 were males and 12 were females. Of
these, 12 males and 2 female deaths were attributed to alcoholic liver disease. Mortality
due to chronic liver disease is low for males and even lower for females in Malta when
compared with EU-15 and EU-13 (Figure A12).
2.1.5. Micronutrient Deficiencies
As opposed to obesity, back in the late 1980’s micronutrient deficiencies were not
considered to be a major public health challenge in the Food and Nutrition Policy for
Malta (Department of Health, 1990); and thus far, no studies at national level have been
carried out to determine if and to what extent micronutrient deficiencies exist among the
Maltese population. It is envisaged that any such existing deficiencies will be identified
from the national food consumption survey that is currently being undertaken by the
Directorate.
2.2. Current strategies and legislative measures
2.2.1. The Food and Nutrition Policy for Malta (1990)
Malta’s Food and Nutrition Policy was endorsed by the Government of Malta in
November 1988 following a review of available data on food and the health situation in
Malta in 1986. At that time, it was observed that the prevalence of noncommunicable
diseases including overweight and obesity in the Maltese Islands was high and that dietary
patterns needed to be improved. The Second National Nutrition Conference in 1988 made
strong recommendations to improve the nutritional status of the Maltese population and
27emphasised the need for political support for policies and actions within the food and
nutrition field.
2.2.2. National Nutrient Goals and Dietary Guidelines
The first Conference on Nutrition in Malta held in 1986 recommended for the Maltese
population the nutrient goals outlined in Table 3 below.
NUTRIENT GOALS FOR AVERAGE MALTESE DIET
Total Fats 30% of Total Energy Intake
Saturated Fats 10% of Total Energy Intake
PS Ratio 0.5-1.0
CholesterolFurthermore, a gradual reduction over the years of small corner shops in some villages was
noted, with a concurrent increasing trend among the population to depend for their daily
food purchases on a few large suppliers. Efforts by government officials to exert any
effective control on the local market as originally indicated by the 1990 National Food and
Nutrition Policy, on the supply and availability of unhealthy food products was made
difficult by the growth of trade agreements, common market(s) and trans-national
marketing of food products and food chains as well as an overwhelming increase in the
number of fast food outlets.
2.2.4. National Legislation, policies, strategies, committees and groups
with a focus on diet, physical activity and health
In line with the values and principles expressed in international documents, the
Government of Malta is committed to improve the health of its nation through food safety
and nutrition policy and in promoting healthy living with a particular focus on vulnerable
groups in the population. The adopted documents include:
The National Breastfeeding Policy Consultation Document (2014) which reviews
the National Breastfeeding Policy (2000)
Food Safety Act (2004)
A Sustainable Development Strategy for the Maltese Islands (2007)
National Environmental and Health Action Plan (2010) (currently under review)
A Strategy for the Prevention and Control of Noncommunicable Diseases in Malta
(2010)
The National Cancer Plan (2011)
A Healthy Weight for Life Strategy (2012)
National Environment Policy (2012)
The main National Committees set up include:
Food Safety Commission (FSC)
Intersectoral Committee for Counteracting Obesity (ICCO)
Intersectoral committee on environmental health
Malta is also very active in the context of the European Union, namely at the High Level
Group (HLG) on Nutrition and Physical Activity. This High Level Group seeks to find
solutions to obesity-related health issues by:
i. Offering an overview of all government policies on nutrition and physical
activity.
ii. Helping governments share policy ideas and practices
iii. Improving liaison between governments and the EU Platform for Diet,
Physical Activity and Health, so that relevant public-private partnerships
can be quickly identified and agreed on.
292.3. Current Initiatives for Food and Nutrition in Malta A large number and variety of initiatives have taken place over the last twenty years. These include research in the form of anthropometric BMI surveillance of school children, self reported adult BMI population surveys and a pilot anthropometric population survey. Prenatal maternal, breastfeeding and weaning programmes, are delivered by means of parent craft classes, breastfeeding walk-in clinics and NGO support in various localities. National awareness-raising and education campaigns on healthy eating and physical activity take place on a regular basis and target both the general population as well as specific population groups. These have focused on the Mediterranean diet, and the regulation of portion sizes. Ongoing campaigns also promote seasonal fruit, vegetables and fish and waste reduction. About 22% of the amount of food purchased every week ends up as solid waste. Initiatives to minimise food waste will have an impact on sustainable food consumption in Malta (NSO, 2013). In this regard a startegy is being drafted by a committee set up by the Minister responsible for the Environment Ongoing initiatives include the development of the skills required to encourage behaviour change and focus on cooking healthy meals for the family within a budget. Weight management classes are available in the community for people who are overweight and obese and focus on the delivery of information and skills development on healthy eating and increased physical activity. Relevant government departments implement European Union initiatives such as Aid to the Deprived1 and the School Fruit Scheme. Community education and support takes various forms such as the local Farmers Market ensuring fresh and cheap fruit and vegetables directly from growers, and free weight management and aerobic classes in different communities. Annex 3 of this document contains details of initiatives related to food and nutrition within the past 10 years from various Government entities. These target different population groups across all ages within different settings. 2.4. Sectors involved in the area of food and nutrition The information included in this chapter in the area of food and nutrition is a result of a series of bilateral and multilateral meetings held throughout the summer of 2012, with the different stakeholders involved in the area of food and nutrition. 1 The Aid to the Deprived Scheme which is fully funded by the EU, provides aid in the form of food products such as cereals, rice, pasta and jam to the most deprived within the community, including people living in poverty and families in difficulty. These are certified by the Department of Social Policy. The Scheme is administered by the Agriculture and Rural Payments Agency and the aid is distributed by participating organisations such as church parishes and other NGOs. 30
2.4.1. Ministry responsible for Health
Public health policy makers have a responsibility to act as advocates and to demonstrate
stewardship and leadership for health across different departments and entities in both the
public and private sectors (WHO, 2008). The Ministry for Health in Malta has developed
policies and action plans aimed at improving the diet food choices of the Maltese
population. These include the Healthy Weight for Life Strategy, the Noncommunicable
Disease Strategy, the National Cancer Plan and the National Environment and Health
Performance Review.
Health should also ensure that a national initiative to provide nutrition education is
embarked upon. Nutrition education is any combination of educational strategies,
accompanied by environmental supports, designed to facilitate voluntary adoption of food
choices and other food-and nutrition-related behaviors conducive to health and well-
being.” (Contento, I.R. 2008).
This definition implies three essential components
a. an awareness-raising component to focus attention on nutrition and increase
motivation to improve diets through effective education and communication
strategies,
b. an action component, where the goal is to facilitate people’s ability to take
action to improve their diets, and
c. an environmental component where nutrition educators work with
policymakers at national and community levels to make healthy foods more
accessible.
One of the proposed areas for action is to support a healthy start to life including better
health for the mother and child. The percentage of infants with a low-birth weight in
Malta stands at an average of 6.1% (N0IS 2012); whereas the breastfeeding rate at
discharge from hospital is still rather low (56%) when compared to the recommended rate
(90%) in the Breastfeeding Policy for Malta (Department of Health, 2000). In addition, the
breastfeeding rate after six months was 38% (Attard Montalto et al., 2008). As
recommended in the Healthy Weight for Life Strategy, the breastfeeding policy for Malta
has been reviewed and has been published for consultation.
Strengthening primary health care services is viewed as another priority area of action for
Malta, particularly the strengthening of nutrition services in the health sector since these
are still lacking. In addition, offering a service of dietary and physical activity counselling
at primary care level as part of a multi-disciplinary team of health professionals is
considered to be an effective preventive approach to tackle early malnutrition and diet-
related noncommunicable diseases. Within the Primary Care Services, healthy lifestyle and
nutrition advice is offered by both general practitioners and community nurses trained in
health promotion and healthy lifestyles skills. Within Secondary Care, the Dietetics
Service provides specialised dietetic advice depending on the clinical needs of both
inpatients and outpatients. Efforts to increase human resources are currently being made,
due to the increasing demands laid on the service from an ageing population and
increasingly complex chronic diseases.
31You can also read