Generalized Mechanical Nerve Pain Hypersensitivity in Children With Episodic Tension-type Headache
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ARTICLES
Generalized Mechanical Nerve Pain Hypersensitivity in
Children With Episodic Tension-type Headache
AUTHORS: Daniel M. Fernández-Mayoralas, MD, PhD,a,b WHAT’S KNOWN ON THIS SUBJECT: Some studies suggest the
César Fernández-de-las-Peñas, PT, PhD,c,d,e Ricardo presence of central sensitization in children with headache;
Ortega-Santiago, PT,c,d Silvia Ambite-Quesada, PT, MSc,f however, conflicting results have been found. Furthermore,
Rodrigo Jiménez-García, MD, PhD,g and Alberto previous studies focused on muscle tissues but not on nerve
Fernández-Jaén, MDa,b
tissues.
aDepartment of Neuropediatry, Hospital Quirón de Madrid,
Madrid, Spain; bDepartment of Neuropediatry, Centro “CADE,” WHAT THIS STUDY ADDS: This is the first study to reveal
Madrid, Spain; cDepartment of Physical Therapy, Occupational
Therapy, Rehabilitation and Physical Medicine, dEsthesiology bilateral and generalized pressure hypersensitivity over both
Laboratory, fDepartment of Anatomy, and gPreventive Medicine trigeminal and nontrigeminal nerves in children with FETTH.
and Public Health Teaching and Research Unit, Department of
Health Sciences, Universidad Rey Juan Carlos, Alcorcón, Spain;
and eCentre for Sensory-Motor Interaction, Department of
Health Science and Technology, Aalborg University, Aalborg,
Denmark
KEY WORDS
abstract
tension-type headache, pressure pain threshold, sensitization, OBJECTIVES: The objective of this study was to analyze the presence of
children
generalized pressure pain hypersensitivity over nerve tissues in tri-
ABBREVIATIONS geminal and nontrigeminal regions in children with frequent episodic
PPT—pressure pain threshold
CNS— central nervous system tension-type headache (FETTH).
FETTH—frequent episodic tension-type headache METHODS: Thirty children, 7 boys and 23 girls (mean age: 8.8 ⫾ 1.7
NPRS—numerical pain rate scale
BDI-II—Beck Depression Inventory, Second Edition years) with FETTH and 50 age- and gender-matched healthy children (14
TTS—Total Tenderness Score boys, 36 girls; mean age: 8.5 ⫾ 2.1 years; P ⫽ .743) were recruited.
CI— confidence interval Pressure pain thresholds (PPTs) were bilaterally assessed over supra-
ANOVA—analysis of variance
orbital (V1), infra-orbital (V2), mental (V3), median (C5), radial (C6),
www.pediatrics.org/cgi/doi/10.1542/peds.2010-0012
and ulnar (C7) nerves by an assessor who was blinded to the patient’s
doi:10.1542/peds.2010-0012 condition.
Accepted for publication Mar 24, 2010
RESULTS: The analysis of variance showed that PPT levels were signif-
Address correspondence to César Fernández de las Peñas, PT,
icantly bilaterally decreased over both trigeminal (supra-orbital, infra-
PhD, Facultad de Ciencias de la Salud, Universidad Rey Juan
Carlos, Avenida de Atenas s/n, 28922 Alcorcón, Madrid, Spain. orbital, and mental) and nontrigeminal (median, ulnar, and radial)
E-mail: cesar.fernandez@urjc.es nerves in children with FETTH as compared with control subjects (all
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). sites, P ⬍ .001). There was a greater magnitude of PPT decrease within
Copyright © 2010 by the American Academy of Pediatrics trigeminal nerves as compared with nontrigeminal nerves (P ⬍ .03).
FINANCIAL DISCLOSURE: The authors have indicated they have PPTs over infra-orbital (rs ⫽ ⫺0.4, P ⬍ .05) and radial (rs ⫽ ⫺0.5, P ⬍
no financial relationships relevant to this article to disclose. .01) nerves were negatively correlated with the duration of headache
attacks (P ⬍ .05).
CONCLUSIONS: Our study revealed bilateral and generalized pressure
hypersensitivity over both trigeminal and nontrigeminal nerves in chil-
dren with FETTH. Diffuse hypersensitivity of peripheral nerves evi-
dences the presence of hyperexcitability of the central nervous system
in children with FETTH. Pediatrics 2010;126:e187–e194
PEDIATRICS Volume 126, Number 1, July 2010 e187
Downloaded from pediatrics.aappublications.org by guest on March 8, 2015Tension-type headache is the most tween child populations with head- [NPRS]), and no aggravation of head-
common form of headache,1 and its ache (episodic versus chronic tension- ache during physical activity. Only 1,
chronic form is 1 of the most neglect- type headache) or to the fact that either photophobia or phonophobia,
ed2 and difficult headaches to treat. It sensitivity to manual palpation of mus- was permitted. No children reported
has been shown that on the World cle tissues may be not sensitive to re- vomiting or evident nausea during
Health Organization’s ranking of the flect central sensitization in children pain attacks. Other primary headaches
world’s most disabling disorders, with headache. were excluded. Each child fulfilled the
headache is among the 10 most dis- There is increasing evidence that sen- criteria for FETTH, and no apparent ev-
abling disorders for both genders.3 sitization of pain pathways leads to idence of secondary headaches was
Several studies have been conducted mechanical pain hypersensitivity of present. Medication overuse head-
of adults with tension-type headache, nerve tissues. In fact, lower PPTs over ache, according to International Head-
but less has been conducted of chil- different peripheral nerves in patients ache Society criteria, was excluded.21
dren. In an epidemiologic study, the with whiplash,15 chronic tension-type None of the children was taking any
6-month prevalence of headaches was headache,16 lateral epicondylalgia,17 prophylactic drug; however, they could
53.2% among children from 7 to 14 unilateral migraine,18 or temporoman- continue with their acute drug therapy
years of age.4 Lewis et al5 estimated dibular pain disorders19 as sign of during headache attacks. In addition,
that ⬃20% of the children with pri- heightened pain sensitivity and hyper- age- and gender-matched children
mary headache need medical therapy. excitability of the central nervous sys- without history of head or neck pain
Although there has been an increasing tem (CNS)20 has been found. To our symptoms were recruited from volun-
interest in the pathogenic mecha- knowledge, no previous studies have teers who responded to a local an-
nisms of tension-type headache, the assessed generalized pressure hyper- nouncement. Ethical approval was
true patho-anatomic mechanisms re- sensitivity over peripheral nerves in granted by local ethics committee
main inconclusive.6 It is clear that hy- children with tension-type headache. (URJC/FHA043). Informed consent was
perexcitability of peripheral and cen- To investigate central nociceptive pro- obtained from both children and par-
tral nociceptive pain pathway plays an cessing gain in children with tension- ents, and all procedures were con-
important role in this condition.7 These type headache, we aimed to analyze ducted according to the Declaration of
sensitization mechanisms result in in- the presence of generalized pressure Helsinki.
creased muscle tenderness8 and pres- pain hyperalgesia over nerves within
symptomatic (trigeminal) and non- Self-reported Measures
sure pain hyperalgesia,9–11 particularly
symptomatic (upper extremity) re- Children completed a headache diary
in adults with tension-type headaches;
gions in children with frequent epi- for 4 weeks to complement the diagno-
however, the results from studies that
sodic tension-type headache (FETTH). sis.22 An 11-point NPRS23 (0 ⫽ no pain,
included children who presented with
tension-type headache are controver- to 10 ⫽ maximum pain) was used to
METHODS assess headache intensity. The head-
sial. An early study reported that chil-
dren with migraine but not with Subjects ache diary was used to calculate the
tension-type headache showed in- Consecutive children who received a following variables: (1) headache in-
creased tenderness of pericranial, diagnosis of FETTH by an experienced tensity, calculated from the mean of
neck, and shoulder muscles.12 In a neuropediatrist from the Neurology the NPRS of the days with headache;
more recent study, the same authors Department of Hospital Quirón were (2) headache frequency, calculated by
found that children with neither mi- screened for eligibility criteria. For all dividing the number of days with head-
graine nor episodic tension-type head- children, headache features, temporal ache by the number of the analyzed
ache had increased extracephalic profile, and family history were as- weeks (days per week); and (3) head-
muscle hypersensitivity.13 Tüzun et al14 sessed from the clinical history. To be ache duration, calculated by dividing
showed pressure pain hyperalgesia included, children had to describe the the sum of the total hours of headache
(lower pressure pain threshold [PPT] characteristics that are typical of by the number of days with headache
levels) in the upper trapezius muscle FETTH following the common criteria of (hours per day).
in adolescents with chronic tension- the International Headache Society21: The Beck Depression Inventory, Sec-
type headache compared with healthy bilateral location, pressing or tighten- ond Edition (BDI-II), a 21-item self-
children. Discrepancies between stud- ing pain, mild/moderate intensity (ⱕ6 report measure that assesses affec-
ies may be related to differences be- on a numerical pain rate scale tive, cognitive, and somatic symptoms
e188 FERNÁNDEZ-MAYORALAS et al
Downloaded from pediatrics.aappublications.org by guest on March 8, 2015ARTICLES
of depression, was also used.24 Chil- high (intraclass correlation coeffi- variation for PPT measures of 20%.
dren, with the help of the parents, cient ⫽ 0.91 [95% confidence inter- This generated a sample size of at least
were asked to choose from a group of val (CI): 0.82– 0.97]).29 16 participants per group.
sentences that best described how Children attended a preliminary ses-
they had been feeling in the preceding PPT Data Management
sion for familiarization with the pres-
2 weeks. For example, to assess sad- sure test procedures. Children were In this study, the magnitude of sensiti-
ness, they could choose either, “I do tested on headache-free days. PPT lev- zation was investigated to assess the
not feel sad,” “I feel sad much of the els were measured bilaterally over differences of absolute and relative
time,” “I am sad all the time,” or “I am supra-orbital (V1), infra-orbital (V2), PPT values between groups. For rela-
so sad or unhappy that I cannot stand mental (V3), median (C5), ulnar (C7), tive values, we calculated a PPT index
it.” The BDI-II has shown good internal and radial (C6) nerves by an assessor by dividing PPT of each participant at
consistency (␣ ⫽ .86), with higher ho was blinded to the children’s condi- each point by the mean of PPT score of
scores indicating higher levels of de- tion. The order of assessment was ran- the control group at the same point. A
pressive symptoms.25,26 domized among the participants. PPT index ⬍100% indicate pressure
pain sensitization.
Pericranial Tenderness All nerves were identified by manual
Examination palpation and marked with a pencil. Statistical Analysis
The supra-orbital nerve (V1) was lo-
Total Tenderness Score (TTS) was Data were analyzed with the SPSS 14.0
cated over the supra-orbital foramen
used to assess pericranial tender- (SPSS Inc, Chicago, IL). Results are ex-
(at the junction between the lateral
ness.27 Briefly, 8 pairs of muscles and pressed as means and 95% CI. The
and medial third of the upper part of
tendon insertions (masseter, tempo- Kolmogorov-Smirnov test was used to
ral, frontal, trapezius, sternocleido- the margin of the orbit), the infra- analyze the normal distribution of the
mastoid, and suboccipital muscles and orbital nerve (V2) was located over the variables (P ⬎ .05). Quantitative data
coronoid and mastoid processes) infra-orbital foramen above the canine without a normal distribution (pain
were palpated.27 Manual palpation was fossa, and the mental nerve from the history, headache intensity, frequency,
conducted with small rotational move- mandibular nerve (V3) was located or duration) were analyzed with non-
ments of the assessors’ second and over the mental foramen on the ante- parametric tests, and data with a nor-
third fingers during 4 to 5 seconds. rior surface of the mandible. The me- mal distribution (PPTs) were analyzed
Tenderness was scored on a 4-point dian nerve (C5) was located over the with parametric tests. The intraclass
(0 –3) scale at each location (local ten- cubital fossa medial to and adjacent to correlation coefficient was used to as-
derness score). A TTS is calculated the tendon of biceps, the ulnar nerve sess intraexaminer reliability of PPT
from the sum of scores from both (C7) was located in the groove be- data. Differences in TTS between study
sides (total maximum score: 48).27 tween the medial epicondyle and the groups were assessed with the un-
olecranon, and the radial nerve (C6) paired Student’s t test. A 3-way analy-
PPT Assessment was marked where it passes through sis of variance (ANOVA) test was used
PPT is defined as the minimal amount the lateral intermuscular septum be- to investigate the differences in PPT
of pressure where a sensation of pres- tween the medial and lateral heads levels with point (supra-orbital, infra-
sure first changes to pain.28 An elec- of triceps to enter the middle to lower orbital, mental, median, radial, and ul-
tronic algometer (Somedic AB, Farsta, third of the humerus. nar nerves) and side (dominant or
Sweden) was used to measure PPT nondominant) as within-participant
(kPa). The pressure was applied ap- Sample Size Determination factors and group (FETTH or control
proximately at a rate of 30 kPa/second. The sample size determination and subjects) as between-participant fac-
All participants were instructed to power calculations were performed tors. A 2-way ANOVA test was also used
press the switch when the sensation with an appropriate software (Tamaño for assessing differences in PPT index
changed from pressure to pain. The de la Muestra 1.1 [Madrid, Spain]). The with side (dominant/nondominant) as
mean of 3 trials (intraexaminer reli- calculations were based on detecting, a within-patient factor and with point
ability) was calculated and used for at least, significant clinically differ- (supra-orbital, infra-orbital, mental,
the main analysis. A 30-second resting ences of 20% on PPT levels between median, radial, ulnar nerves) as a
period was allowed between each both groups30 with an ␣ level of .05 and between-patient factor. Posthoc com-
measurement. The reliability of pres- a desired power of 80% and an esti- parisons were done with the Tukey
sure algometry has been found to be mated interparticipant coefficient of test. Finally, the Spearman’s rho (rs)
PEDIATRICS Volume 126, Number 1, July 2010 e189
Downloaded from pediatrics.aappublications.org by guest on March 8, 2015test was used to analyze the associa- TABLE 1 Differences in PPTs (kPa) Over the Supra-orbital (V1), Infra-orbital (V2), and Mental (V3)
Nerve Trunks Between Children With Tension-type Headache and Healthy Control Subjects
tion between PPTs and the clinical vari-
Parameter Supra-orbital Nerve (V1)a Infra-orbital Nerve (V2)a Mental Nerve (V3)a
ables relating to pain symptoms. The
Children with FETTH
statistical analysis was conducted at a Dominant 132.2 ⫾ 30.3 (120.1–144.3) 152.6 ⫾ 29.5 (140.5–164.7) 185.1 ⫾ 35.7 (173.1–197.2)
95% confidence level, and P ⬍ .05 was Nondominant 126.6 ⫾ 27.1 (114.5–138.7) 147.9 ⫾ 30.4 (135.8–160.1) 185.8 ⫾ 39.7 (173.7–197.9)
considered statistically significant. Children without
headache
Dominant 269.1 ⫾ 21.1 (260.0–278.1) 272.1 ⫾ 22.8 (263.1–281.1) 291.4 ⫾ 24.7 (282.3–300.4)
RESULTS Nondominant 263.1 ⫾ 21.3 (254.0–272.1) 271.2 ⫾ 20.1 (262.1–280.2) 288.7 ⫾ 27.7 (279.6–297.7)
Data are means ⫾ SD (95% CI).
Demographic and Clinical Data of a Significant differences between patients and control subjects (2-way ANOVA test).
the Sample
Fifty-two consecutive children who
Pericranial Tenderness than did healthy control subjects (P ⬍
presented with headache between
Children with FETTH showed a signifi- .001). In addition, trigeminal nerves
September and December 2009 were
cantly (t ⫽ 15.986; P ⬍ .001) greater showed lower PPT as compared with
screened for eligibility criteria.
TTS (mean ⫾ SD: 19.4 ⫾ 5.8) as com- nontrigeminal nerves (P ⬍ .001). The
Twenty-two (42%) children were ex-
pared with healthy children (mean ⫾ posthoc analyses revealed an increasing
cluded: migraine (n ⫽ 7), hemicranial
SD: 3.8 ⫾ 2.9). No significant associa- PPT gradient from supra-orbital (V1),
headache (n ⫽ 7), higher levels of de-
tion between TTS and clinical features infra-orbital (V2), mental (V3), median
pression (BDI-II ⬎15), and anxiety (n ⫽
of headache were found (P ⬎ .3). (C5), radial (C6), and ulnar (C7) nerves in
8). Finally, a total of 30 children, 7 boys
both groups (P ⬍ .01). Table 1 summa-
and 23 girls, aged 5 to 11 years (mean: Pressure Pain Sensitivity Over rizes PPT assessed over trigeminal
8.6 ⫾ 2.1 years) satisfied all of the in- Peripheral Nerves nerves for both sides within each study
clusion criteria and agreed to partici- group, and Table 2 shows PPT levels over
The intraexaminer repeatability of PPT
pate. In our sample, headache history nontrigeminal nerves in both groups.
readings for nerve trunks ranged from
was 1.8 years (95% CI: 1.5–2.1 years),
0.90 to 0.93 for the dominant side and
mean headache period per day was 4.1 PPT Indices
from 0.91 to 0.94 for the nondominant
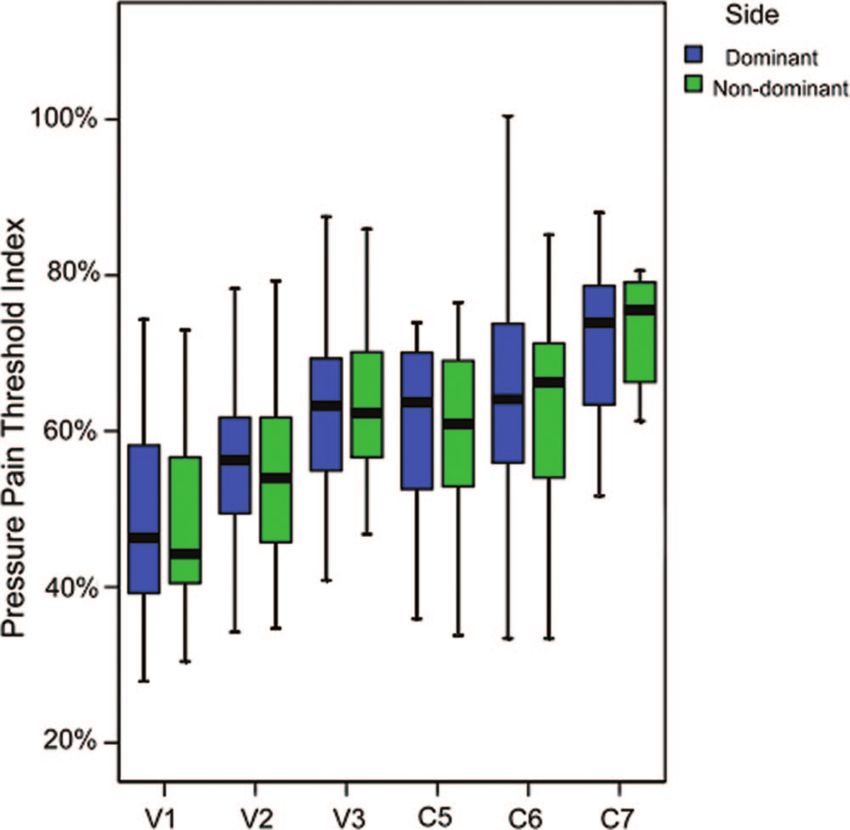
hours (95% CI: 3.2– 4.9 hours), mean side. The SE of measurement ranged The ANOVA showed significant differ-
intensity per episode was 5.1 (95% CI: from 4.3 to 5.0 kPa for the dominant ences for PPT indices between points
4.7–5.5), and number of days per week side and from 4.8 to 5.5 kPa for the (F ⫽ 22.723, P ⬍ .001) but not sides
with headache was 3.5 (95% CI: 2.8 – nondominant side. (F ⫽ 0.136, P ⫽ .712). Furthermore, no
3.8). No significant associations be-
The ANOVA revealed significant differ- significant side * points interaction
tween headache parameters (inten-
ences between groups (F ⫽ 319.8, P ⬍ (F ⫽ 0.198, P ⫽ .963) was found.
sity, frequency, or duration) were
.001) and points (F ⫽ 430.2, P ⬍ .001) but Posthoc analysis revealed that PPT in-
found (P ⬎ .7). Children were tested on
not sides (F ⫽ 0.219, P ⫽ .640). A signifi- dices in the trigeminal nerves (supra-
headache-free days and when at least orbital: 49% [95% CI: 44%–53%]; infra-
cant interaction between group and
5 days had elapsed since the last head point was also found (F ⫽ 4.434, P ⫽ orbital: 55% [95% CI: 50%–59%];
pain attack to avoid possible related .001). In such a way, over each nerve, pa- mental: 63% [95% CI: 59%– 69%]) were
allodynia. Five children usually took tients showed bilateral lower PPT levels significantly more impaired (P ⬍ .03)
ibuprofen during acute headaches. Fi-
nally, the BDI-II score was 3.8 (95% CI:
3.2– 4.3). In fact, a significant positive TABLE 2 Differences in PPTs (kPa) Over the Median (C5), Radial (C6), and Ulnar (C7) Nerve Trunks
Between Children With Tension-type Headache and Healthy Control Subjects
relation (rs ⫽ 0.503, P ⫽ .005) between
Parameter Median Nerve (C5)a Radial Nerve (C6)a Ulnar Nerve (C7)a
BDI-II and headache frequency was Children with episodic
found: the greater the frequency of frequent tension
type headache
headache attacks, the greater the level Dominant 204.6 ⫾ 37.1 (192.6–216.7) 227.8 ⫾ 51.4 (215.8–239.9) 286.7 ⫾ 55.2 (274.6–298.8)
of depression. In addition, 50 age- and Nondominant 201.2 ⫾ 39.5 (189.1–213.2) 225.7 ⫾ 48.2 (213.7–237.8) 292.9 ⫾ 49.7 (280.8–304.9)
Children without
gender-matched children without headache
headache, 14 boys and 36 girls, aged 5 Dominant 336.8 ⫾ 50.4 (327.8–345.8) 350.4 ⫾ 22.0 (341.3–359.4) 410.1 ⫾ 29.2 (400.9–419.1)
Nondominant 334.6 ⫾ 32.1 (325.5–343.6) 359.2 ⫾ 23.3 (350.2–368.3) 409.6 ⫾ 26.6 (400.5–418.6)
to 11 years (mean: 8.5 ⫾ 2.1 years) Data are means ⫾ SD (95% CI).
participated (P ⫽ .743). a Significant differences between patients and control subjects (2-way ANOVA test).
e190 FERNÁNDEZ-MAYORALAS et al
Downloaded from pediatrics.aappublications.org by guest on March 8, 2015ARTICLES
⫺0.46, P ⫽ .013; Fig 2) and over the ra-
dial (dominant: rs ⫽ ⫺0.601, P ⬍ .001;
nondominant: rs ⫽ ⫺0.556, P ⫽ .002)
nerves were found: the longer the dura-
tion of headache attacks, the lower the
PPT levels. No significant correlation be-
tween TTS and headache clinical param-
eters were found (P ⬎ .1).
DISCUSSION
The main finding of this study was bilat-
eral and generalized pressure pain hy-
persensitivity over trigeminal and non-
trigeminal nerves in children with FETTH
when compared with healthy children. In
fact, generalized hypersensitivity of pe-
ripheral nerves supports the presence
of hyperexcitability of the CNS in children
with FETTH. The decrease in PPTs, partic-
FIGURE 1
PPT indices in both trigeminal and extratrigeminal points. The boxes represent the mean and percen- ularly over trigeminal nerves, was asso-
tile scores, and the error bars represent the SD. ciated with the duration of headache at-
tacks, supporting a role of nerve
as compared with PPT indices in the Pressure Sensitivity and Clinical peripheral nociception in the sensitiza-
nerves of the nontrigeminal area (me- tion mechanisms.
Features in Children With Tension-
dian: 60% [95% CI: 56%– 65%]; radial: type Headache In this study, PPT was significantly de-
63% [95% CI: 59%– 68%]; ulnar: 70% creased bilaterally over the supra-
[95% CI: 66%–75%]). Furthermore, the Significant negative correlations be- orbital, infra-orbital, mental, median,
PPT index of the ulnar nerve was less tween duration of headache with PPT ulnar, and radial nerves in children
impaired than PPT indices in the me- over the infra-orbital (dominant: rs ⫽ with FETTH as compared with control
dian and radial nerves (P ⬍ .05; Fig 1). ⫺0.41, P ⫽ .033; nondominant: rs ⫽ subjects, suggesting both trigeminal
FIGURE 2
Scatter plots of relationships between duration of headache attacks and PPT levels over infra-orbital nerve (n ⫽ 30).
PEDIATRICS Volume 126, Number 1, July 2010 e191
Downloaded from pediatrics.aappublications.org by guest on March 8, 2015and extratrigeminal sensitization of af- tization could depolarize nociceptive neurons, so stimulation or sensitiza-
ferent inputs from neural tissues. Our second-order neurons, and this will tion of peripheral elements communi-
results agree with previous studies enhance head pain perception36; how- cates centrally; therefore, once central
conducted of whiplash,31 lateral epi- ever, the potential role of the cal- sensitization is established, nociceptive
condylalgia,17 unilateral migraine,18 citonin gene–related peptide and inputs that originate from trigeminal
and temporomandibular pain disor- neurogenic inflammation has been ex- nerve trunks may become a perpetuat-
ders,19 which showed a generalized de- tensively studied in migraine but not in ing factor for central sensitization in chil-
crease in PPTs over peripheral nerves tension-type headache. Nevertheless, dren with FETTH. Undoubtedly, other trig-
as sign of hyperexcitability of the these mechanisms also may be impli- gers for FETTH exist.
CNS.20 The presence of pressure hyper- cated in tension-type headache pain In addition to sensitization mecha-
sensitivity over extratrigeminal areas according to the continuum theory be- nisms, the results from this study re-
can be considered a manifestation of tween these headaches, in which flect a dysfunctional state of endoge-
sensitization of second-order (or tension-type headache would be a mild nous pain modulatory systems, which
higher) nociceptive neurons in the expression of migraine.37 has been previously reported in adults
CNS. In fact, the presence of general- An interesting result of this study was with chronic tension-type head-
ized lower PPT levels found in children that the magnitude of PPT changes in ache.41,42 Furthermore, recent studies
with FETTH may be a common finding of children with FETTH was greater within highlight the importance of risk genes
central sensitization in other forms of the trigeminal nerves (supra-orbital: for enhanced pain sensitivity (eg, poly-
chronic pain, such as chronic abdomi- 49%; infra-orbital: 55%; mental: morphisms in the gene coding for the
nal pain, sickle cell disease, chronic 63%) as compared with nontrigemi- cathecol-o-methyl-transferase) have
arthralgias, and fibromyalgia. It would nal nerves (median: 60%; radial: been associated with headache in
be interesting to investigate whether 62%– 65%; ulnar: 70%). Our results adult populations.43,44 We do not know
the identified sensitization mecha- suggest that the sensitization process whether a combination of sensitization
nisms found in this study in children is restricted not only to the trigeminal mechanisms, descending pain modu-
with FETTH are also present in children second-order neurons but also to ex- lation, and genetics can be implicated
with other chronic pain syndromes. tratrigeminal nociceptive neurons in in the development of FETTH in
Previous studies determined that neu- children with FETTH. Nevertheless, the children.
rogenic inflammation during head- degree of sensitization within the tri- We should recognize some limitations
ache attacks, particularly migraine, geminal area was greater, which sup- of this study. First, we included a sub-
may activate trigeminal afferents that ports a role of peripheral sensitization group of children who had FETTH with
project to brain areas that are involved mechanisms. In fact, because hyperex- high frequency of headache attacks
in nociceptive processing.32 That tri- citability of the CNS is considered a dy- (3.5 per week) and lower levels of de-
geminal neurons release calcitonin namic condition that is influenced by pression according to the BDI-II. One of
gene–related peptide under condi- various factors, particularly periph- the main reasons for controlling the
tions that mimic neurogenic inflamma- eral nociceptive inputs,38 it may be pos- degree of depression in children with
tion supports its role in pain percep- sible that peripheral nociceptive bar- FETTH is that depression induces an in-
tion during headache attacks.33 In fact, rage contributes to this sensitization creased effect on pressure pain sensi-
a neurogenic inflammation triggered process. In this study, PPT levels over tivity.45 We recognize that the BDI-II has
by antidromic discharges that origi- the infra-orbital nerve were negatively good psychometric properties in chil-
nate from the CNS could sensitize pe- associated with the duration of head- dren aged ⱖ12 to 13 years26,46–48; how-
ripheral nerve trunks,34 which may de- ache attacks, suggesting a potential ever, no study has investigated psycho-
polarize nociceptive second-order (or role of prolonged peripheral nocicep- metric properties of the BDI-II in
higher) neurons.35 Over time, this tion in the sensitization process. In children aged ⬍12 years, so our re-
might affect the physical condition of such scenario, the sensitization of sults related to “lower level of depres-
the nerves and would lower the thresh- nerve nociceptors may result in spon- sion” should be considered with cau-
old of the nociceptive fibers of the taneous neural discharges,39,40 which tion. Moreover, we did not assess
nervi nervorum (nerves that innervate contribute to the irritation of the tri- anxiety levels in our children with
the connective tissue layers of the geminal nerve nucleus caudalis. This FETTH, which may influence pain-
nerve itself). Finally, low-threshold A- phenomenon may be related to the fact enhanced sensitivity. We do not know
fiber inputs in states of central sensi- that many pain circuits are bipolar whether our results would be similar
e192 FERNÁNDEZ-MAYORALAS et al
Downloaded from pediatrics.aappublications.org by guest on March 8, 2015ARTICLES
in other subgroup of patients with included 7 boys with FETTH, we could healthy children. Generalized pain hy-
FETTH or children with chronic tension- not compare pressure pain hypersen- persensitivity of peripheral nerves
type headache. In addition, children sitivity between genders. Future stud- supports the presence of a state of hy-
from a specialized neurologic clinic ies should analyze gender differences perexcitability of the CNS in children
may not represent the characteristics in these sensitization mechanisms. Fi- with FETTH. The decrease in PPT levels,
of the general population of children nally, another limitation of this study is particularly over trigeminal nerves,
with headache; therefore, extrapola- that we can speculate on the mecha- was associated with the duration of
tion of our results should be con- nisms (peripheral or central) that are headache attacks, supporting a role of
ducted with caution. Population-based responsible for the increased mechan- nerve peripheral nociception in the
epidemiologic studies with larger ical pain sensitivity only over periph- sensitization mechanisms. Additional
eral nerves. Additional studies are re- studies are required to define the po-
samples are needed to permit a more
quired to define the potential role of tential role of nerve tissue hypersensi-
generalized interpretation of these re-
nerve tissue hypersensitivity in the tivity in the perpetuation of central
sults. Second, we included both girls
perpetuation of central sensitization in sensitization in children with tension-
and boys with FETTH. It has been shown
children with tension-type headache. type headache.
that women have greater susceptibil-
ity to the development of temporal CONCLUSIONS ACKNOWLEDGMENTS
summation of chemical,49 mechani- We found bilateral and generalized This study received funds from a grant
cal,50 and thermal51 pain and less effi- pressure hypersensitivity over trigem- conceded by the Universidad Rey Juan
cient diffuse pain inhibitory path- inal and nontrigeminal nerves in chil- Carlos and Comunidad de Madrid (ref-
ways52,53 than men. Because we dren with FETTH when compared with erence CCG10-URJC BIO-5011).
REFERENCES
1. Andlin-Sobocki P, Jonsson B, Wittchen HU, Type and Cervicogenic Headache: Patho- pain threshold in children with headache.
Olesen J. Cost of disorders of the brain in physiology, Diagnosis and Treatment. Balti- Eur J Pain. 2006;10(7):581–585
Europe. Eur J Neurol. 2005;12(suppl 1):1–27 more, MD: Jones & Bartlett Publishers; 14. Tüzun EH, Karaduman A, Eker L. Pressure
2. Bendtsen L, Jensen R. Tension type head- 2009:97–106 pain thresholds in adolescent patients with
ache: the most common, but also the most 8. Fernández-de-las-Peñas C, Cuadrado ML, Ge chronic tension-type headache. Pain Clinic.
neglected headache disorder. Curr Opin HY, Arendt-Nielsen L, Pareja JA. Increased 2005;17(2):127–131
Neurol. 2006;19(3):305–309 peri-cranial tenderness, decreased pres- 15. Sterling M, Jull G, Vicenzino B, Kenardy J.
3. Stovner L, Hagen K, Jensen R, et al. The sure pain threshold, and headache clinical Sensory hypersensitivity occurs soon
global burden of headache: a documenta- parameters in chronic tension type head- after whiplash injury and associated
tion of headache prevalence and disability ache patients. Clin J Pain. 2007;23(4): with poor recovery. Pain. 2003;104(3):
worldwide. Cephalalgia. 2007;27(3): 346 –352 509 –517
193–210 9. Bendtsen L, Jensen R, Olesen J. Decreased 16. Fernández-de-las-Peñas C, Coppieters MW,
4. Kröner-Herwig B, Heinrich M, Morris L. pain detection and tolerance thresholds in Cuadrado ML, Pareja JA. Patients with
Headache in German children and chronic tension type headache. Arch Neu- chronic tension type headache demon-
adolescents: a population-based epidemio- rol. 1996;53(4):373–376 strate increased mechano-sensitivity of the
logical study. Cephalalgia. 2007;27(6): 10. Schoenen J, Bottin D, Hardy F, Gerard P. Ce- supra-orbital nerve. Headache. 2008;48(4):
519 –527 phalic and extra-cephalic pressure pain 570 –577
5. Lewis D, Ashwal S, Dahl G, et al. Practice thresholds in chronic tension type head- 17. Fernández-Carnero J, Fernández-de-las-
parameter: evaluation of children and ado- ache. Pain. 1991;47(2):145–149 Peñas C, De-La-Llave-Rincón AI, Ge HY,
lescents with recurrent headaches— Arendt-Nielsen L. Widespread mechanical
11. Ashina S, Babenko L, Jensen R, Ashina M,
report of the Quality Standards Subcommit- pain hyper-sensitivity as sign of central
Magerl W, Bendtsen L. Increased muscu-
tee of the American Academy of Neurology sensitization in unilateral lateral
lar and cutaneous pain sensitivity in ce-
and the Practice Committee of the Child epicondylalgia: a blinded, controlled study.
phalic region in patients with chronic
Neurology Society. Neurology. 2002;59(4): Clin J Pain. 2009;25(7):555–561
tension-type headache. Eur J Neurol.
490 – 498 18. Fernández-de-las-Peñas C, Arendt-Nielsen L,
2005;12(7):543–549
6. Fumal A, Schoenen J. Tension-type head- Cuadrado ML, Pareja JA. Generalized me-
ache: current research and clinical man- 12. Anttila P, Metsahonkala L, Mikkelsson M, et chanical pain sensitivity over nerve tissues
agement. Lancet Neurol. 2008;7(1):70 – 83 al. Muscle tenderness in pericranial and in patients with strictly unilateral migraine.
neck-shoulder region in children with Clin J Pain. 2009;25(5):401– 406
7. Fernández-de-las-Peñas C, Arendt-Nielsen L,
headache: a controlled study. Cephalalgia.
Simons DG, Cuadrado ML, Pareja JA. Sensi- 19. Fernández-de-las-Peñas C, Galán-del-Río F,
2002;22(5):340 –344
tization in tension type headache: a pain Fernández-Carnero J, Pesquera J, Arendt-
model. In: Fernández-de-las-Peñas C, 13. Metsahonkala L, Anttila P, Laimi K, et al. Nielsen L, Svensson P. Bilateral widespread
Arendt-Nielsen L, Gerwin R, eds. Tension Extra-cephalic tenderness and pressure mechanical pain sensitivity in myofascial
PEDIATRICS Volume 126, Number 1, July 2010 e193
Downloaded from pediatrics.aappublications.org by guest on March 8, 2015temporomandibular disorder: evidence of chronic idiopathic neck pain. Clin J Pain. tients with migraine without aura. J Clin
impairment in central nociceptive process- 2005;21(2):175–181 Neurol. 2007;3(1):24 –30
ing. J Pain. 2009;10(11):1170 –1178 32. Parsons A, Strijbos P. The neuronal versus 44. Hagen K, Pettersen E, Stovner LJ, Skorpen F,
20. Zusman M. Central nervous system contri- vascular hypothesis of migraine and corti- Zwart JA. The association between head-
bution to mechanically produced motor and cal spreading depression. Curr Opin Phar- ache and Val158Met polymorphism in the
sensory responses. Aust J Physiother. 1992; macol. 2003;3(1):73–77 catechol-O-methyltransferase gene: the
38(2):195–120 33. Durham P. Calcitonin gene-related peptide HUNT Study. J Headache Pain. 2006;7(2):
21. Headache Classification Subcommittee of (CGRP) and migraine. Headache. 2006; 70 –74
the International Headache Society: The In- 46(suppl 1):S3–S8 45. Rhudy JL, Meagher M. Fear and anxiety: di-
ternational Classification of Headache Dis- 34. Daemen M, Kurvers H, Kitslaar P, Slaaf DW, vergent effects on human pain thresholds.
orders, 2nd edition. Cephalalgia. 2004; Bullens PH, Van den Wildenberg FA. Neuro- Pain. 2000;84(1):65–75
24(suppl 1):9 –160 genic inflammation in an animal model of 46. Kapci EG, Uslu R, Turkcapar H, Karaoglan A.
22. Phillip D, Lyngberg AC, Jensen R. Assess- neuropathic pain. Neurol Res. 1998;20(1): Beck Depression Inventory II: evaluation of
ment of headache diagnosis: a comparative 41– 45 the psychometric properties and cut-off
population study of a clinical interview with 35. Hoheisel U, Mense S, Simons DG, Yu XM. Ap- points in a Turkish adult population. De-
a diagnostic headache diary. Cephalalgia. pearance of new receptive fields in rat dor- press Anxiety. 2008;25(10):E104 –E110
2007;27(1):1– 8 sal horn neurons following noxious stimu-
47. Basker M, Moses PD, Russell S, Russell PS.
23. Jensen MP, Turner JA, Romano JM, Fisher L. lation of skeletal muscle: a model for
The psychometric properties of Beck De-
Comparative reliability and validity of referral of muscle pain? Neurosci Lett. 1993;
pression Inventory for adolescent depres-
chronic pain intensity measures. Pain. 153(1):9 –12
sion in a primary-care paediatric setting in
1999;83(2):157–162 36. Woolf CJ, Thompson SW. The induction and India. Child Adolesc Psychiatry Ment Health.
24. Beck AT, Steer RA, Brown GK. Beck Depres- maintenance of central sensitisation is de- 2007;1(1):8
sion Inventory. 2nd ed. San Antonio, TX: Psy- pendent on N-methyl-D-aspartic acid recep-
chological Corporation; 1996 tor activation; implications for the treat- 48. Steer RA, Kumar G, Ranieri WF, Beck AT.
ment of post-injury pain hypersensitivity Use of the Beck Depression Inventory-II
25. Beck AT, Steer RA, Garbin MG. Psychometric
states. Pain. 1991;44(3):293–299 with adolescent psychiatric outpatients.
properties of the Beck Depression
J Psychopathol Behav Assess. 1998;20(2):
Inventory: twenty-five years of evaluation. 37. Cady RK. The convergence hypothesis. Head-
127–137
Clin Psychol Rev. 1988;8(1):77–100 ache. 2007;47(suppl 1):S44 –S51
49. Ge HY, Madeleine P, Arendt-Nielsen L. Sex
26. VanVoorhis WC, Blumentritt TL. Psychomet- 38. Herren-Gerber R, Weiss S, Arendt-Nielsen L,
ric properties of the Beck Depression et al. Modulation of central hypersensitivity differences in temporal characteristics of
Inventory-II in a clinically-identified sample by nociceptive input in chronic pain after descending inhibitory control: an evalua-
of Mexican American adolescents. Journal whiplash injury. Pain Med. 2004;5(4): tion using repeated bilateral experimental
of Child and Family Studies. 2007;789 –798 366 –376 induction of muscle pain. Pain. 2004;
110(1–2):72–78
27. Langemark M, Olesen J. Pericranial tender- 39. Bove G, Light A. The nervi nervorum: missing
ness in tension headache: a blind controlled link for neuropathic pain? Pain Forum. 1997; 50. Sarlani E, Greenspan JD. Gender differ-
study. Cephalalgia. 1987;7(4):249 –245 6(2):181–190 ences in temporal summation of mechani-
cally evoked pain. Pain. 2002;97(1–2):
28. Vanderweeën L, Oostendorp RB, Vaes P, Du- 40. Watkins L, Maier S. Neuropathic pain: the
quet W. Pressure algometry in manual ther- immune connection. Pain Clin Update. 2004; 163–169
apy. Man Ther. 1996;1(5):258 –265 13(1):1– 4 51. Fillingim RB, Maixner W, Kincaud S, Silva S.
29. Chesterton LS, Sim J, Wright CC, Foster NE. 41. Pielstickera A, Haagc G, Zaudigh M, Lauten- Sex differences in temporal summation but
Inter-rater reliability of algometry in mea- bachera S. Impairment of pain inhibition in not sensory-discriminative processing of
suring pressure pain thresholds in healthy chronic tension-type headache. Pain. 2005; thermal pain. Pain. 1998;75(1):121–127
humans, using multiple raters. Clin J Pain. 118(1–2):215–223 52. Staud R, Robinson ME, Vierck CJ, Price D.
2007;23(9):760 –766 42. Sandrini G, Rossi P, Milanov I, Serrao M, Cec- Diffuse noxious inhibitory controls (DNIC)
30. Prushansky T, Dvir Z, Defron-Assa R. Repro- chini AP, Nappi G. Abnormal modulatory in- attenuate temporal summation of second
ducibility indices applied to cervical pres- fluence of diffuse noxious inhibitory con- pain in normal males but not in normal fe-
sure pain threshold measurements in trols in migraine and chronic tension-type males or fibromyalgia patients. Pain. 2003;
healthy subjects. Clin J Pain. 2004;20(5): headache patients. Cephalalgia. 2006;26(7): 101(1–2):167–174
341–347 782–789 53. Serrao M, Rossi P, Sandrini G, et al. Effects
31. Scott D, Jull G, Sterling M. Widespread sen- 43. Park JW, Lee KS, Kim JS, Kim YI, Shin HE. of diffuse noxious inhibitory controls on
sory hypersensitivity is a feature of chronic Genetic contribution of catechol-O- temporal summation of the RIII reflex in hu-
whiplash-associated disorder but not methyltransferase polymorphism in pa- mans. Pain. 2004;112(3):353–360
e194 FERNÁNDEZ-MAYORALAS et al
Downloaded from pediatrics.aappublications.org by guest on March 8, 2015Generalized Mechanical Nerve Pain Hypersensitivity in Children With Episodic
Tension-type Headache
Daniel M. Fernández-Mayoralas, César Fernández-de-las-Peñas, Ricardo
Ortega-Santiago, Silvia Ambite-Quesada, Rodrigo Jiménez-García and Alberto
Fernández-Jaén
Pediatrics 2010;126;e187; originally published online June 7, 2010;
DOI: 10.1542/peds.2010-0012
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/126/1/e187.full.h
tml
References This article cites 50 articles, 8 of which can be accessed free
at:
http://pediatrics.aappublications.org/content/126/1/e187.full.h
tml#ref-list-1
Citations This article has been cited by 2 HighWire-hosted articles:
http://pediatrics.aappublications.org/content/126/1/e187.full.h
tml#related-urls
Subspecialty Collections This article, along with others on similar topics, appears in
the following collection(s):
Neurology
http://pediatrics.aappublications.org/cgi/collection/neurology
_sub
Neurologic Disorders
http://pediatrics.aappublications.org/cgi/collection/neurologic
_disorders_sub
Permissions & Licensing Information about reproducing this article in parts (figures,
tables) or in its entirety can be found online at:
http://pediatrics.aappublications.org/site/misc/Permissions.xht
ml
Reprints Information about ordering reprints can be found online:
http://pediatrics.aappublications.org/site/misc/reprints.xhtml
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
publication, it has been published continuously since 1948. PEDIATRICS is owned, published,
and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk
Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy of Pediatrics. All
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Downloaded from pediatrics.aappublications.org by guest on March 8, 2015Generalized Mechanical Nerve Pain Hypersensitivity in Children With Episodic
Tension-type Headache
Daniel M. Fernández-Mayoralas, César Fernández-de-las-Peñas, Ricardo
Ortega-Santiago, Silvia Ambite-Quesada, Rodrigo Jiménez-García and Alberto
Fernández-Jaén
Pediatrics 2010;126;e187; originally published online June 7, 2010;
DOI: 10.1542/peds.2010-0012
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/126/1/e187.full.html
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
publication, it has been published continuously since 1948. PEDIATRICS is owned,
published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point
Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Downloaded from pediatrics.aappublications.org by guest on March 8, 2015You can also read

















































