Hair Loss Management with PRP at AGA and Hair Transplants
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Hair Loss Management with PRP at AGA and Hair
Transplants
Introduction:
Androgenetic alopecia (AGA) is the most common form of hair loss. It can affect not only
men but also women (1). Prevalence increases with age, affecting up to 80% of men and 40%
of women (2). AGA can lead to a considerable impairment of the quality of life up to
depression (3). Therefore, early intervention and management of AGA with evidence-based
medicine (EBM) is of great importance (4.5). Autologous Platelet-Rich plasma (PRP) has
recently been used for AGA. However, the market has grown faster than the research for this
promising technology and there are still many open questions.
Objective: Development of a recommendation for an evidence-based management of AGA
with PRP and as an addition to hair transplants.
Recommendation on how to proceed with consultation and diagnosis
Before a possible treatment of hair loss with PRP, its cause must be clarified exactly. Because
PRP is not a meaningful therapy for everyone or any kind of hair loss. The temporal and
schematic course of the hair loss, possible stress-inducing events in the last 3 to 6 months as
well as current blood values must be examined.
No therapy should be carried out without sufficient diagnostics!!!!
Often it is only a case of diffuse hair loss (teleogenic effluvium) in which more hair falls out
over the whole head than usual. Hair loss can be an indication of an existing disease or the
result of a traumatic event that occurred shortly before. If the cause of the hair loss disappears,
in this case the hair also starts to grow again, i.e. the hair grows even without the use of PRP
(6).
Procedure in case of diffuse hair loss: clarify cause, remove trigger and wait and see
If you have recently changed a medication that may affect your hair metabolism, you will also
need to wait and see.
A dermatoscopic examination of the scalp is mandatory and a trichsoscan (Fig. 1,2) would be
desirable.
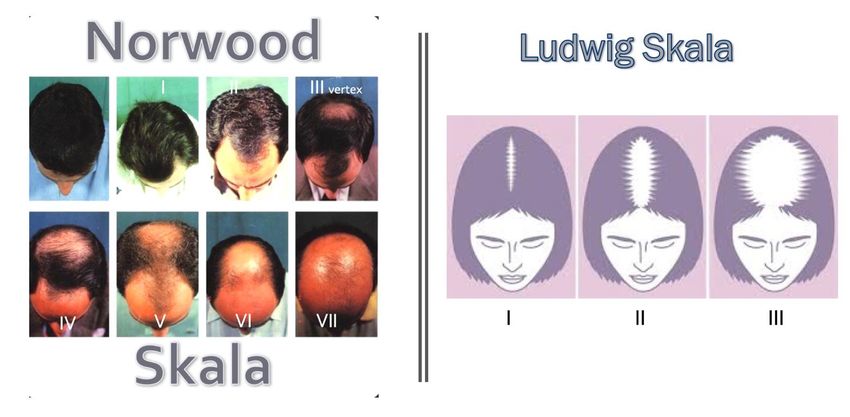
Over 90% of patients are diagnosed with AGA (1). This form of hair loss is hereditary and is
mostly of hormonal origin and follows a pattern which is classified according to Norwood (7)
in men as NW I - VII and in women as Ludwig (8) LW I - III (Fig.3).
Currently, topical minoxidil and oral finasteride are the only drugs approved by the Food and
Drug Administration (FDA) for the treatment of AGA (Fig. 4).
Currently available therapies are sometimes considered to have limited efficacy, which is why
it is very important to find new therapies such as PRP for this pathology (9).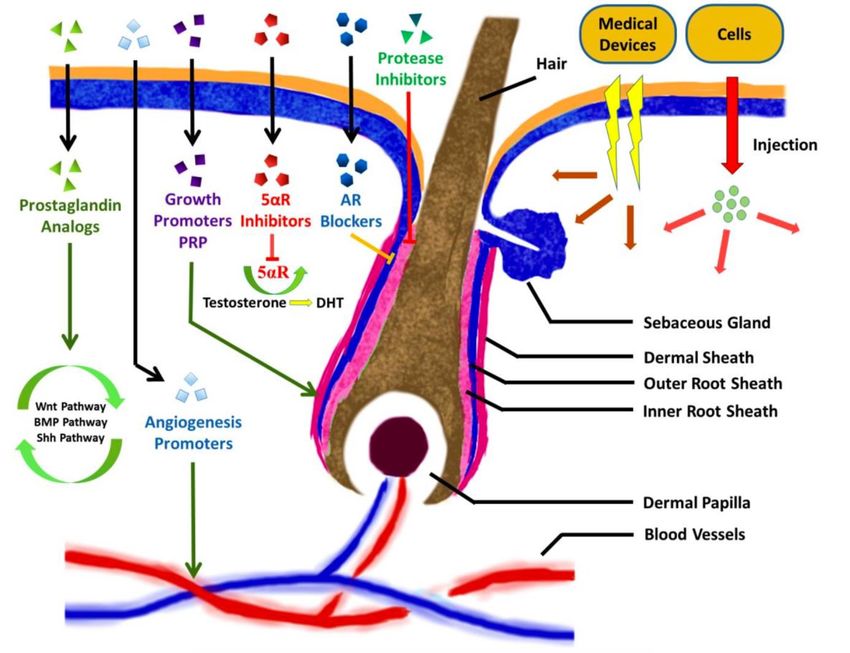
Therapy management by AGA AGA therapy management should be evidence-based to ensure the best possible consultation and treatment. In practice, this means integrating individual clinical expertise with the best available external evidence (10), taking into account the patient's values and wishes (Fig. 5). The EBM is based on 3 pillars - individual clinical experience - current status of clinical research (Table 3-S3 Guideline) - Values and wishes of the patient In order to be able to make a recommendation for the various therapeutic approaches of AGA treatment according to the best EBM principles, an evidence level was assigned to each therapy per se. A low level corresponds to a high evidence level, a high level to a low evidence level (Table 1). The level of evidence is determined by the fact that each study is assigned a quality level (A1 = randomized double-blind studies with high quality to D = expert opinion with low quality). The quality grades of all studies belonging to a therapy scheme are then combined into an evidence level (Table 2) (4.5). The resulting evidence levels of the various therapy approaches for AGA are listed in Table 3 and serve as guideline S3 (11) for orientation in the recommendation for the management of AGA therapy. This primarily takes into account their level of evidence, the therapy results to be expected, the practicability for physician and patient as well as the compliance of the patient. Together, the 3 pillars of EBM should decide which individualized therapy is best suited for the patient (Table 3). New recommendation of the S3 Guideline and current therapy approaches today and in the future for the AGA. While minoxidil and finasteride have been the only evidence-based therapies for AGA in recent decades, further developments with new approaches have progressed in recent years. Figure 6 shows the main components of AGA pathogenesis and current and future therapeutic approaches (12). Very much correspondingly, the topical 25% finasteride solution (13), which, like the topical androgen receptor blocker Clascoterone (14), is still in the preclinical study phase. For the efficacy of prostaglandin (PGE2 and PGF2) analogues and PDG2 antagonists (15) the result of an ongoing study (16) has yet to be determined. For other approaches such as JAK inhibitors (17), stem cell therapy (18), mesotherapy (19) and carboxytherapy (20), there is currently no sufficient scientific evidence of efficacy. Currently, only low-level laser therapy (LLLT) (evidence level 2) and PRP (evidence level 3) meet the criteria of the S3 guideline in order to be recommended for AGA management alongside minoxidil and finasteride. Evidence level 3 in PRP was achieved through two studies evaluating the efficacy of PRP in male and female patients with AGA, both with evidence level C and meeting inclusion criteria for the guideline (21,22,23). However, there is currently no standard procedure for PRP, no standardized techniques or kits for isolation and activation, and no standardized protocols for dosage and frequency of injections. There is also uncertainty about the combination with other substances and cells. It
is therefore difficult to objectively assess the impact of PRP on AGA in order to achieve a higher level of evidence in the long term. Postulated effect of PRP The platelets enriched in PRP produce growth factors that positively influence proliferation, survival and differentiation of many different cells. This also seems to be true for hair follicle cells. The higher the number of platelets, the higher the concentration of growth factors. The most important growth factors involved in hair follicle formation are probably vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), insulin-related growth factor (IGF)-1 and fibroblast growth factors (FGFs) (24,25). AGA results from the shortening of the anagen phase and extension of the telogen phase which results in follicle miniaturization. The injection of activated PRP into mice was shown to reverse this process with an increased anagen telogen rate and a larger number of hair follicles in the anagen phase (26) (Fig.7). A similar conclusion was reached by Li and colleagues (2012) who found that activated PRP stimulates the proliferation of human DP cells, promotes the survival of hair follicle cells through its anti-apoptotic effects (Akt) on dermal papilla (DP) cells and can stimulate hair growth by prolonging the anagen phase of the hair cycle (27) (Fig.8). The most likely mechanisms of action are the triggering of various signalling cascades including the β- Catenin (BC) pathway, the extracellular signal-regulated kinase (ERK) cascade and the protein kinase B (Akt) cascade, which positively affect cell survival, proliferation and differentiation (28). Activate or not activate? Growth factors are usually physiologically present in an inactive form. It should not be debated whether these factors have to be activated in order to achieve an effect. The important question is "how and when to activate". Options include calcium chloride, bovine thrombin, mechanical (e.g. ultrasound, etc.) or autologous thrombin serum. In a recently published study by Inslaco, a significantly improved Hair mass index for activation with 20Hz ultrasound of 48% was found compared to 25% in the calcium chloride control group. There was also an increased hair density (57% compared to 33%) and a larger hair diameter (10% compared to the initial level of 0%) (29) But also other activation methods such as extracellular matrix (Acell), autologous lipocytes or fat stem cells can achieve good results. PRP Protocol - Techniques to be considered Different PRP protocols differ significantly in preparation and execution. It is recommended to use platelet concentrations 1.5 to 4 times higher than the physiological level. Giusti et al. showed that the optimal platelet concentration to promote angiogenesis in human endothelial cells is 1.5 million / µl and that higher concentrations may be worse (30). The literature recommends one PRP session per month for 3 to 4 months and a subsequent maintenance interval of 3 to 6 months. Injection of PRP into a subdermal layer at a depth of approximately 3 to 4 mm may allow diffusion into connective tissue and subdermal space, allowing PRP to reach the base of the hair follicle and DP cells without damaging the vessels and nerves below and parallel to the skin surface (31) (Fig.9).
Effect of PRP on hair transplants Hair transplants (Fig.10), 11) not only obviously improve the current hair condition, but as a recently published study could show, also the quality of life and even health (32) (Fig.12). PRP as adjuvant therapy shows an improved result in wound healing as well as in the growth rate of transplanted follicles. In 2006, Übel and his colleagues published their first paper on the use of PRP as an additional therapy for hair transplantation. They were able to show a significant difference in the transplant density of the scalp previously treated with PRP compared to the untreated control area: on average the transplant density in the scalp treated with PRP was 18.7 follicular units (FUT) per cm 2 compared to 16.4 FUTs per cm2 in the untreated scalp (33) Garg et al. This study also showed a significant influence on the quantity and quality of hair growth when PRP was injected into the prefabricated slits during hair transplantation (34). Some advocate PRP as the optimal holding solution for transplants compared to NaCl solution (35), but there is still no evidence for this. Since PRP promotes wound healing (36), it should also be recommended for use in the extraction area, as healthy hair can also be injured here, which can be reduced by PRP. PRP stimulates the formation of new blood vessels, scarring is reduced and the regeneration of grafts traumatised by transplantation is improved, which can ultimately lead to an improved growth rate of implanted grafts. Conclusion (Fig.13) Although hair loss is very common in both men and women, FDA approved drug treatments are currently limited to Minoxidil and Finasteride. PRP is a promising new option to bridge the gap between medical and surgical options for AGA. Animal models suggest that PRP promotes hair growth, and several clinical studies have shown that PRP is effective in androgenetic alopecia in a variety of settings, including maintaining hair density. Also, its supportive effect as an adjuvant during and after hair transplantation is significant. Further controlled studies with quantifiable measures of treatment success are now needed to confirm these results.
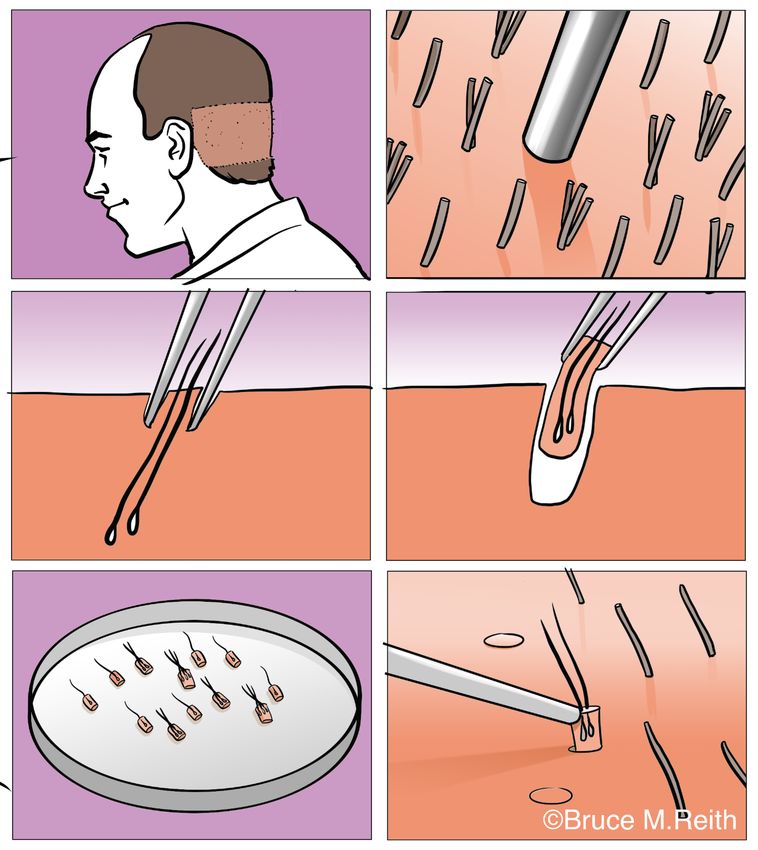
Table 1: Evidence level (1-4)
1 Studies with evidence level 1 or studies with predominantly consistent results with
evidence level A2
2 studies Level of evidence A2 or studies with predominantly consistent results with
Level of evidence B
3 studies with evidence level B or studies with predominantly consistent results
evidence level C
4 Little or no standardized evidence
Source: Kant et al. 2018
The evidence level takes into account the methodological quality of the studies (evidence
levels) and the interim consistency of the results.
Table 2: Evidence evaluation (grades A1..D)
A1 A1 Meta-analysis comprising at least one randomised clinical trial with evidence
of grade A2 with consistent results from different studies.
A2 Randomized, double-blind, high quality, comparative clinical trials (e.g., sampling,
patient involvement flowchart, ITT analysis, sufficient size).
B Randomised, lower quality clinical trials or other comparable studies (non-
randomised, cohort or case-control studies)
C Non-comparable studies
D expert opinion
Source: Kant et al. 2018
The methodological quality of each study included in the evidence-based analysis was defined
in degrees by the quality of the evidence according to the following scheme ( A1..D).
Table 3: Current recommendation for the management of AGA according to S3 Guideline
1/2018
Therapy Eviden Evidence evidence Safet practicabil practicabil
ce level prevent condition y ity ity
progressi improvem patient doctor
on ent
Men
Finasteride 1mg 1 +++ ++ +++ ++++ ++
Dutasteride 1 +++ +++ ++ ++++ ++
0,5mg
Minoxidil 5% 1 +++ ++ +++ +/++ +++
+
Hair 2 - +++ ++ + interv. +
transplantation
with/without adj. +++longter
therapy m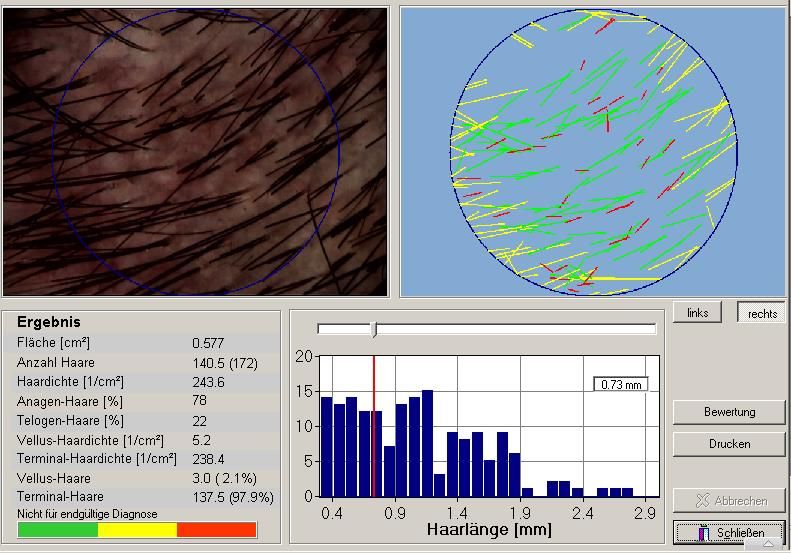
LLLT (Low-level 2 +/- +/- + +/- +
Laser Therapie)
PRP 3 +/- +/- + +/- +
Women
Minoxidil 2% 1 +++ ++ +++ + +++
Lsg. +
Minoxidil 5%
Schaum
Hormones oral 3 + + + +++ ++
Hyperandrogenis
mus
Hormones oral 3 +/- +/- + +++ ++
normal
Hormones
Hair 4 - ++ ++ + +
transplantation Eingriff
with/without adj. +++
therapy Langzeit
LLLT (Low-level 2 +/- +/- ++ +++ +++
Laser Therapie)
PRP ( Platelet- 3 +/- +/- 1 +/- +
Rich Plasma)
Overall rating - +/- + ++ +++ ++++
niedrig hoch
Quelle: Kanti et al. 2018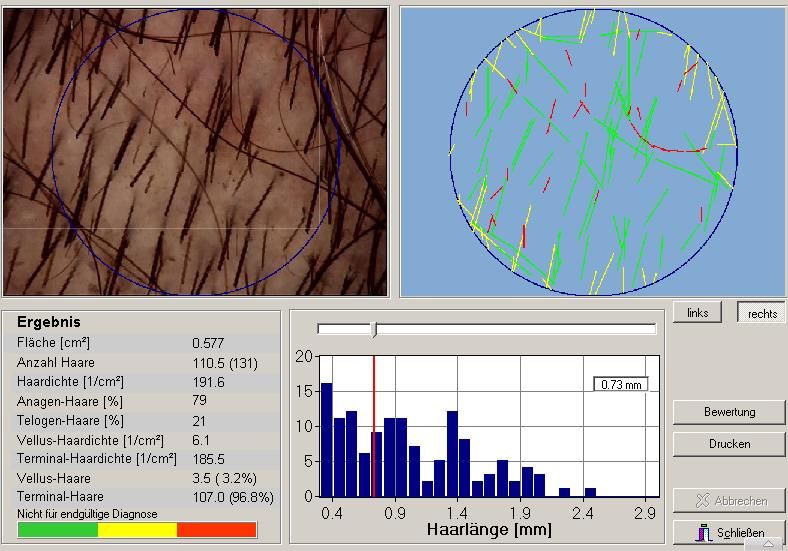
Figure 1: Trichoscan before PRP treatment Bestimmt die Haaranzahl, deren Dichte und die Rate der Haare in der Ruhephase (Telogenrate)
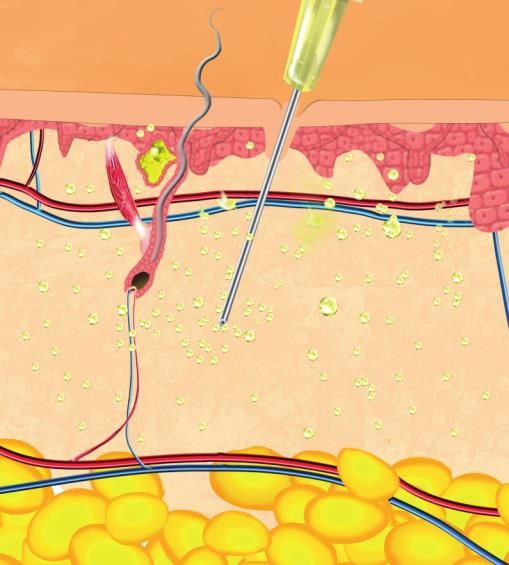
Figure 2: Trichoscan 6 months after 4 x PRP treatments Total number of hairs, hair density and number of growing hairs are significantly improved. Figure 3: Classification of the AGA according to Norwood and Ludwig. Quelle: Norwood, 1975, Ludwig, 1977
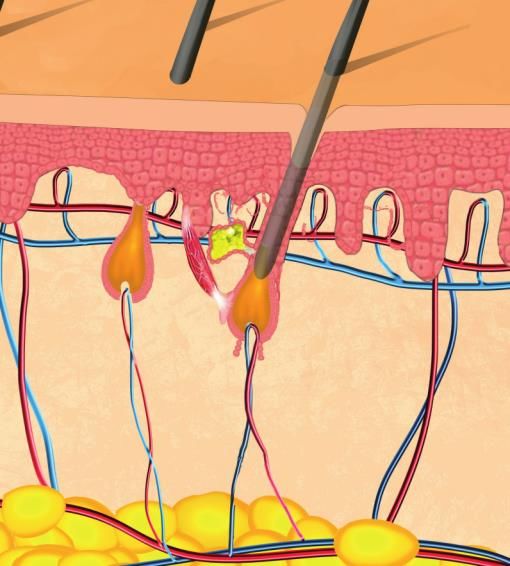
Figure 4: Previous FDA approved medication
©Bruce Reith
Quelle: Autor
While in the last 3 decades only 2 substances, Minoxidil and Finasteride, were the only
substances of choice at AGA, new and improved therapies have developed rapidly in the last
6 years.
Multiple drug treatments as well as cell therapeutics or medical devices are still in preclinical
development or clinical trials. However, these could soon come onto the market.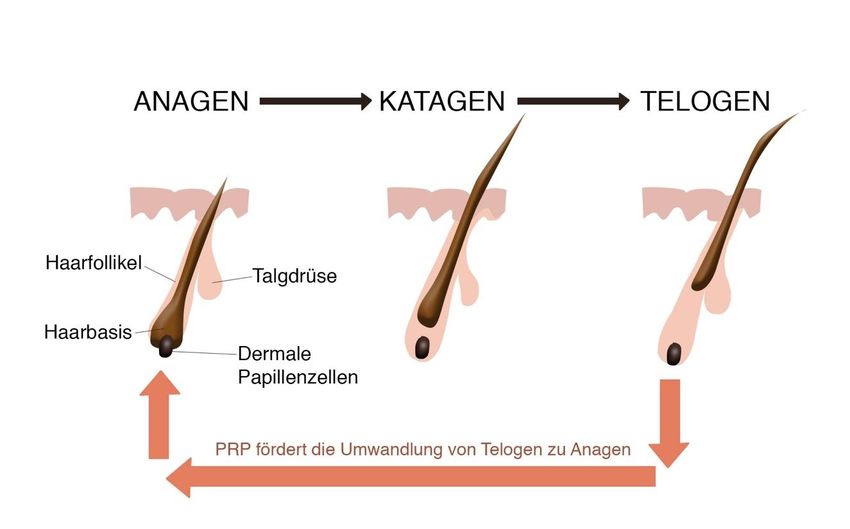
Figure 5: Triad of Eivdenzbased Medicine (EbM) Quelle: Autor
Figure 6: Pathogenesis and therapeutic approaches in AGA. Quelle: Gua H. et al. 2017 The main components of AGA pathogenesis are genetically susceptible hair follicles, the conversion of dihydrotestosterone (DHT) in the skin from circulating androgens, accumulated DHT-inducible suppressors of hair follicle growth, micro-inflammations and cell aging, some of which are caused by androgen-mediated DNA damage. Current and future treatment strategies include reducing local DHT production, targeting androgen-regulated factors in follicular epithelial cells and dermal papilla cells, improving perifollicular vascular supply, controlling microscopic follicular inflammation, and possibly controlling connective tissue remodelling by balancing protease/antiprotease systems.
Figure 7: Effect of PRP on hair growth cycle ©Bruce Reith Dermal papilla cells: Regulate the development and growth of hair follicles and is considered a reservoir of multipotent stem cells.
Figure 8: Mechanical model of the PRP effect on the dermal papilla cells Quelle: Autor Activated PRP stimulates hair growth by promoting vascularization and angiogenesis, and encourages hair follicles to enter and extend the anagen phase of the growth cycle. The process is achieved by increased activation of β-Catenin (BC), extracellular signaling regulated kinase (ERK) and protein kinase B (Akt) signaling pathways mediated by growth factors, leading to the necessary cell proliferation and differentiation. Akt also simultaneously prevents apoptosis A
Figure 9: Main protocol PRP in 4 steps Quelle: Autor
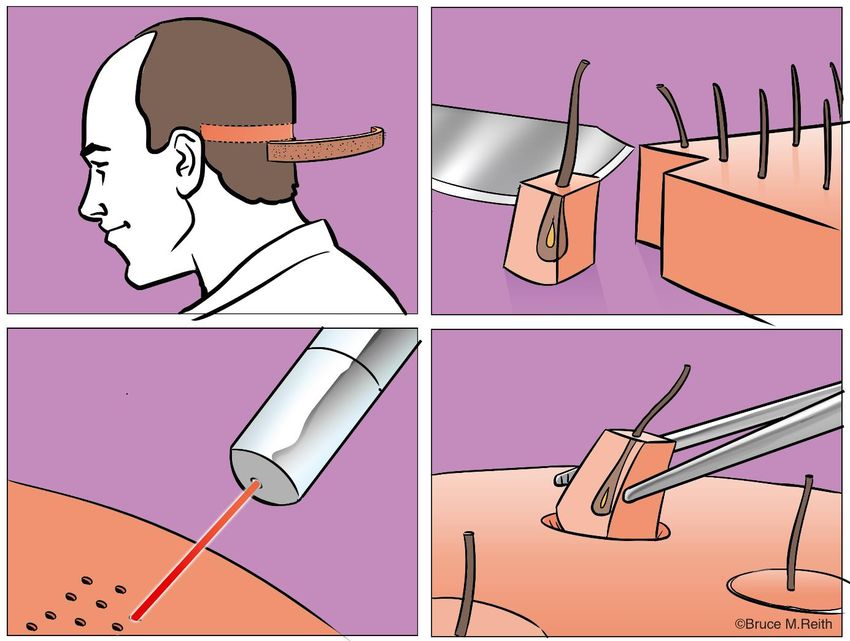
Figure 10: Hair transplantation Strip method- FUT Quelle: Autor
Figure 11: Single removal - FUE A hair transplant is a surgical procedure that transplants hair follicles from the scalp, which is resistant to hair loss, to bald or sparse areas. The hair follicles are removed either with strips (FUT) (Fig.10) or individually (FUE) (Fig.11), preserved in a holding solution and then implanted into the slits prefabricated by the doctor.
Figure 12: Influence of hair transplantation on quality of life and health
Verbessern Haartransplantationen die geistige und körperliche Gesundheit?
Reith Bruce, MD, PhD., Mojto Viliam, MD, PhD, Kottman Tanja, MD.
Medizinischer Direktor bei medical hair & esthetic (Munich,Germany) / Medizinischer Direktor Haarzenrum Bodenseeklink (Lindau, Deutschland )
Kontakt: brucereith@me.com
Ausschluß: COI; Keine; Off-Label Usage; Keine.
RESULTS 5) AQoL-8D Resultat
Einleitung 1) Kein signifikanter Unterschied in der Alters- und Ge- AQoL 8D Werte pro
Das Haar ist ein wesenlicher Bestandteil unserer Erscheinung. schlechtsverteilung zw. Prä- und postoperativer Gruppe: Dimension prä- (n=188)
Zahlreiche Studien zeigten die negative Auswirkungen des Haar- Durchschnittsalter 37.0 ± 12.1 Jahre und 88.7% männlich versus postoperativer
Gruppe (n=129)
ausfalls auf das Wohlbefinden und die Lebensqualität. Darüber im Vergleich zu 36.9 ± 11.8 Jahre und 88.5% männlich.
hinaus wurde ein Zusammenhang mit psychischen Problemen 2) 96.6% sagten, dass die Transplantation ihr Leben positiv ver- Die AQoL 8D Werte waren in
(z.B. geringes Selbstvertrauen) und Depressionen beobachtet. änderte und 97.7% würden sich wieder operieren lassen (n=213).
allen 8 Dimensionen der prä-
opertiven Gruppe signifikant
3) Auswirkung von schönen Haaren auf…… höher (p< 0,001) imVergleich
Studienziel zur postoperativen Gruppe
100
Diese Studie untersuchte die Auswirkungen einer Haartrans-
Patienten mit hoher Punktzahl (% )
Pic: www.worth1000.de
plantation auf die psychische Gesundheit im infolge des Haar- 80
ausfalls und auf die allgemeine Lebensqualität. 60
6) BDI-II Resultat
40 BDI-II-Gesamtpunktzahl in
Material und Methoden der prä- und postoperativen
Ø Studiendesign: retrospektive 2 Zenter Kohortenstudie 20 Behandlungsgruppe
Ø 130 Pateinten mit erblichem bedingten Haarausfall welche 0 Die Differenz zwischen dem
eine Transplantation 9 -36 Monate vor Einschluss erhielten Se
lb At tr Mä Ge
sun
“ Mein volles Haar hat mir zum Erfolg
Mittelwert von 9,58 ± 9,45
st v akt We nnlic alsSchauspieler geholfen”
Ø 194 Geschlechts- und Altersgleiche Patienten die sich noch e rtr
aue
ivit
ä t
ibli hke
chk it /
dh
eit
(George Clooney) der präoperativen und 3,31
n e it ± 5,33 der postoperativen
keiner Haartransplantation unterzogen haben Patienten ist statistisch
Prozentsatz der Patienten, die auf die Frage nach der Wirkung von schönen Haar eine
Ø Alle Patienten füllten 3 Umfragen aus: (1) Autorenfragebogen hohe Wichtigkeit (4,5 or 6 on 6-point Likert scale) angegeben haben (n=401) signifikant (p 20)
Patienten mit hoher Punktzahl (% )
Ø 83 weitere Pilotstudienpatienten haben den vom Auto erstel- Minimale Depression 9 - 13 16,6% 6,3% wurden bei 18,2% der prä-
Pic: www.worth1000.de
80
lten Fragebogen ausgefüllt (in Analyse mit einbezogen). operativen Patienten fest-
Milde Depression 14 - 19 4,8% 4,7%
60 gestellt, verglichen mit 2,4%
Mittelschwere Depr 20 - 28 11,2% 1,6% der postoperativen Patienten.
40 Schwere Depression 29 - 63 7,0% 0,8%
20 Fazit
“ mit den Haaren verliert man auch Ø Erfolgreiche Haartransplantationen haben einen signifikant
0 sein Selbstvertrauen”
Selb Ane Part Beru positiven Einfluß auf die geistige Gesundheit und verbessern
stw und rkenn nerw f
e Bek ung ahl
rt
ann im F das Wohlbefinden und die allg.Lebensqualität des Pateinten.
ten re
kre unde
is s- Ø Haartransplantationen sind nicht nur rein kosmetische Ein-
Patientenanteil, die bei der Befragung zu den Auswirkungen des Haarusfall eine hohe griffe sondern auch medizinische notwendige Behandlungen
Quelle : Richardson, J.
Bedueutung (4,5 or 6 on 6-point Likert scale) angegeben haben (n=401) welche ebenso bedeutend für die Gesundheit sind.Figure 13: Current recommendation for AGA Quelle:Autor
Literaturverzeichnis 1.STOUGH, D., STENN, K., HABER, R., PARSLEY, W. M., VOGEL, J. E., WHITING, D. A., & WASHENIK, K. 2005. Psychological Effect, Pathophysiology, and Management of Androgenetic Alopecia in Men. Mayo Clin Proc, 2005, 80, 10, 1316–1322. 2.Severi G, Sinclair R, Hopper JL, et al. Androgenetic alopecia in men aged 40-69 years: prevalence and risk factors. Br J Dermatol. 2003;149:1207-13. 3.Grimalt R. Psychological aspects of hair disease. J Cosmet Dermatol. 2005;4:142-147. 4.Izet Masic, Milan Miokovic, Belma Muhamedagic. 2008. Evidence Based Medicine – New Approaches and Challenges. Acta Inform Med. 2008; 16(4): 219–225. 5.Sackett DL, Richardson WS, Rosenberg W, Haynes RB. Evidence-based medicine: how to practice and teach. 2. ed. Edinburgh: Churchill-Livingstone, 2000 6. Malkud S. A Telogen Effluvium A Review. A J Clin Diagn Res. 2015 Sep;9(9):WE01-3. 7. NORWOOD, O. T. 1975. Male pattern baldness: classification and incidence. South Med J, 1975,69, 11, 1359–1365 8. Ludwig E. Classification of the types of androgenetic alopecia (common baldness) occurring in the female sex. Br J Dermatol. 1977;97:247–54. 9. Falto-Aizpurua L, Choudhary S, Tosti A. Emerging treatments in alopecia. Expert Opin Emerg Drugs 2014;19:545–56. 10. Internet: https://www.cochrane.de/de/ebm (Abruf:6.1.2019) 11. Kanti V, Messenger A, Dobos G et. Al S3-Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men – short version , J.Eur. Acad. Dermatol. Venerol. 2018 Jan; 32(1):11-22. 12. Guo H, Gao WV, Endo H, McElwee KJ. Experimental and early investigational drugs for androgenetic alopecia. Expert Opin Investig Drugs. 2017 Aug;26(8):917-932. 13.Blume-Peytavi U et al, Efficacy and safety of a new 5% minoxidil formulation in male androgenetic alopecia: A randomized, placebo-controlled, double-blind, noninferiority study. J Cosmet Dermatol. 2018 Apr 16. 14. Internet: http://www.cassiopea.com/news-and-media/press-releases/yr- 2018/180716.aspx,( abgerufen 6.1.20199 15.Guo et al. Experimental and early investigtional drugs for androgentic alopecia. Expert opinion Investig. Drugs. 2017 Aug 26(8):917-932 16. A. Rossi et. al (2018) A preliminary study on topical cetirizine in the therapeutic management of androgenetic alopecia, Journal of Dermatological Treatment, 29:2, 149-151, 17. Harel S, et al. Pharmacologic inhibition of JAK-STAT signaling promotes hair growth. Science Advances 23 Oct 2015:Vol. 1, no. 9. e1500973. 18.Shin H, Won CH, Chung WK, Park BS. Up-to-date Clinical Trials of Hair Regeneration Using Conditioned Media of Adipose-Derived Stem Cells in Male and Female Pattern Hair Loss. Curr Stem Cell Res Ther. 2017;12(7):524-530. 19.Saceda-Corralo D et al. Mesotherapy with Dutasteride in the Treatment of Androgenetic Alopecia. Int J Trichology. 2017 Jul-Sep;9(3):143-145. 20.Doghaim NN, El-Tatawy RA, Neinaa YME, Abd El-Samd MM. Study of the efficacy of carboxytherapy in alopecia. J Cosmet Dermatol. 2018 Dec;17(6):1275-1285. 21.Schiavone G, Raskovic D, Greco J et al. Platelet-rich plasma for androgenetic alopecia: a pilot study. Dermatol Surg 2014; 40: 1010–1019. 22.Alves R, Grimalt R. Randomized placebo-controlled, double-blind, half-head study to assess the efficacy of platelet-rich plasma on the treatment of androgenetic alopecia. Dermatol Surg. 2016;42:491–497. 23. Gkini MA, Kouskoukis AE, Tripsianis G et al. Study of platelet-rich plasma injections in the treatment of androgenetic alopecia through an one-year period. J Cutan Aesthet Surg 2014; 7: 213–219.
24. Maria-Angeliki G, Alexandros-Efstratios K, Dimitris R, et al. Platelet-rich Plasma as a Potential Treatment for Noncicatricial Alopecias. Int J Trichology. 2015;7:54-63 25. Chaudhari ND, Sharma YK, Dash K, et al. Role of Platelet-rich Plasma in the Management of Androgenetic Alopecia. Int J Trichology. 2012;4:291-2. 26. Crabtree Judy et al. A Mouse Model of Androgenetic Alopecia, Endocrinology, Volume 151, Issue 5, 1 May 2010, Pages 2373–238. 27. Li ZJ, Choi HI, Choi DK, Sohn KC, et al. Autologous platelet-rich plasma: a potential therapeutic tool for promoting hair growth. Dermatol Surg 2012;38:1040–6 28. Gupta A, Carviel J. Mechanistic Model of Platelet-Rich Plasma Treatment for Androgenetic Alopecia. Dermatologic Surgery: December 2016 - Volume 42 - Issue 12 - p 1335–1339 29. Insalaco C, 2018 PRP IN PATTERN HAIR LOSS.COMPARISON OF TWO METHODS OF PRP ACTIVATION, ISHRS World Congress, Hollywood oct.2018, oral presentation. 30. Giusti,I et al. Platelet Concentration in Platelet-Rich Plasma Affects Tenocyte Behavior In Vitro. Biomed Res Int. 2014; 2014: 630870. 31. Internet: https://www.medestheticsmag.com/subdermal-depo-prp(abgerufen:7.1.2019) 32. Reith B., Mojto V., Kottman T., 2018. Verbessert eine Haartransplantation auch die Gesundheit – ist sie doch mehr eine medizinische als eine kosmetische Indikation? kosmetische Medizin 4/18:14-19 33. Uebel CO, da Silva JB, Cantarelli D, et al. The role of platelet plasma growth factors in male pattern baldness surgery. Plast Reconstr Surg. 2006;118:1458-1466. 34. Garg et al. Outcome of Intra-operative Injected Platelet-rich Plasma Therapy During Follicular Unit Extraction Hair Transplant: A Prospective Randomised Study in Forty Patients. J Cutan Aesthet Surg. 2016 Jul-Sep;9(3):157-164. 35. Reese R. In: Regenerative Medicine Part 2: Use of Platelet Rich Plasma in Hair, Hair Transplant 360. Lam S, editor. Vol. 3. New Delhi: Jaypee Brothers Publishing; 2014. pp. 565–573. 36. Lacci KM, Dardik A. Platelet-rich plasma: support for its use in wound healing. Yale J Biol Med. 2010;83(1):1–9. Kontakt Dr.Bruce Reith, (MD, PhD) Chefarzt Medical Hair& Esthetic Brunnstrasse 11 80331 München Chefarzt Haarklinik Bodenseeklinik Graf-Lennart-Bernadotte-Str. 1 DE 88131 Lindau / Bodensee Email: Brucereith@me.com
You can also read