Health Provider Compliance Strategy 2021-22
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Health Provider Compliance Strategy 2021–22

Copyright © 2021 Commonwealth of Australia as represented by the Department of Health. This work is copyright. You may copy, print, download, display and reproduce the whole or part of this work in unaltered form for your own personal use or, if you are part of an organisation, for internal use within your organisation, but only if you or your organisation: (a) do not use the copy or reproduction for any commercial purpose; and (b) retain this copyright notice and all disclaimer notices as part of that copy or reproduction. Apart from rights as permitted by the Copyright Act 1968 (Cth) or allowed by this copyright notice, all other rights are reserved, including (but not limited to) all commercial rights. Requests and inquiries concerning reproduction and other rights to use are to be sent to the Communication Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to copyright@health.gov.au. This document is intended to provide additional guidance to stakeholders about the approach we take to compliance and enforcement activities. These functions are carried out in accordance with statutory requirements and this strategy cannot override those requirements. It does not constitute legal advice.

Contents Introduction...................................................................................................................................... 1 Health Provider Compliance............................................................................................................ 2 2021–2022 Compliance Priorities ................................................................................................... 3 Compliance Approach..................................................................................................................... 4 Identifying Non-Compliance ........................................................................................................... 5 Compliance Activities ...................................................................................................................... 5 Our Responsibilities....................................................................................................................... 10 Supporting Compliance................................................................................................................. 11 How to Report Non-Compliance................................................................................................... 11 Resources....................................................................................................................................... 12
Introduction
In the 2020-21 financial year, it is estimated that the Australian Government will have spent in excess of
$42.6 billion* on three key public funding schemes and health incentive programs. These are the Medicare
Benefits Schedule (MBS), the Pharmaceutical Benefits Scheme (PBS), the Child Dental Benefits Schedule
(CDBS) and Practice Incentive Program (PIP). These programs represented approximately half of all
Australian Government expenditure on health.
The Department of Health (the Department) administers these programs enabling access to subsidised
health services and medicines available to all Australians at low or no cost. The Department ensures the
integrity of these funding schemes by identifying and treating incorrect claiming, inappropriate practice
and fraud.
An overview of the public health funding schemes is as follows:
Medicare Benefits Schedule
The MBS, established under the Health Insurance Act 1973, is Australia’s national
health insurance scheme which subsidises the cost of selected medical services
for eligible patients that are provided by eligible practitioners.
Pharmaceutical Benefits Scheme
The PBS, established under the National Health Act 1953, is part of the Australian
Government’s broader National Medicines Policy. Under the PBS, the Australian
Government subsidises the cost of medicine for most medical conditions.
Child Dental Benefits Schedule
The CDBS, established under Part VAA of the Health Insurance Act 1973
and the Dental Benefits Act 2008, is a Commonwealth funded dental scheme.
The scheme provides benefits for a wide range of dental services, such as
examinations, x-rays and preventive treatments to children up to 17 years of age
whose families receive certain government benefits (eligible children).
Practice Incentive Programs
Practice Incentive Program (PIP) payments support eligible general practices that
meet specific performance criteria designed to encourage quality care, enhanced
capacity, and improved access and health outcomes for patients. Incentive
payments include eHealth, quality improvement, teaching, Indigenous health,
after hours care, procedural activities and loadings for
rural locations.
* To be confirmed in the 2021 Department of Health Annual Report.
1 Health Provider Compliance Strategy 2021/22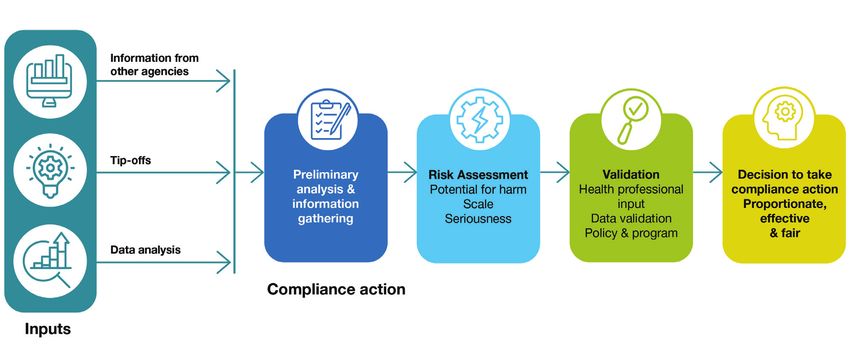
Health Provider Compliance
The Australian Government, the public, and health professionals expect that providers (health practitioners
and organisations that deliver health services) understand and adhere to legislated rules and requirements
that govern access to Australia’s health programs.
These rules include eligibility requirements for practitioners providing services and medicines and the
patients accessing them. They ensure Australian Government public health funding is directed towards
services and medicines that are clinically effective, cost effective and achieve their intended health
outcomes for all Australians.
The Department recognises that the majority of providers maintain high professional standards and adhere
to their obligations through simple measures such as:
• proactively educating themselves on the rules and requirements utilising the range of services and
resources provided by the Department and Services Australia
• providing clinically relevant services, referrals and access to medicines that are necessary for the
appropriate treatment of the patient
• ensuring that only eligible services or benefits are claimed
• creating and retaining contemporaneous clinical and administrative records
• retaining oversight of registration, approvals, billing and claiming and remediating any errors
• proactively contacting the Department and Services Australia if they make or discover errors in
their claiming.
Purpose
The Health Provider Compliance Strategy (the Strategy) identifies the principles which govern the Department’s
compliance and enforcement function, and the Department’s compliance and enforcement priorities.
The Strategy aligns with the Department’s Corporate Plan 2021–22 and Fraud Control Plan 2021–23.
The Strategy will also assist health practitioners, administrators, corporate health service providers and
practices to understand their compliance obligations and the steps the Department may take where there
are concerns about non-compliance.
2 Health Provider Compliance Strategy 2021/22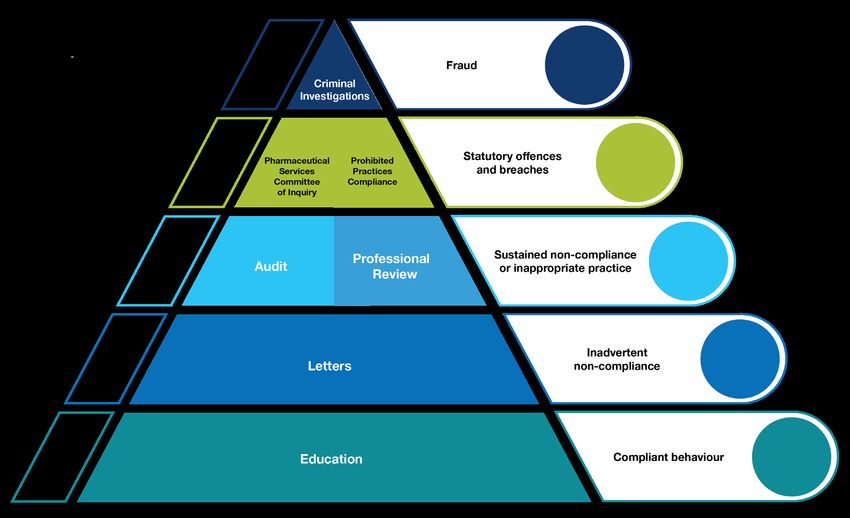
2021–2022 Compliance Priorities
In taking actions to encourage, strengthen and enforce compliance with public health funding schemes,
and in alignment with the Department’s compliance principles and legislative requirements, the Department
will always prioritise the interests of patients and the integrity of the health payments system.
This includes prioritising action to address practices that:
• subject patients to the risk of harm for the purposes of maximising revenue from health programs.
• undermine the clinical independence of practitioners - claiming should always reflect the
provision of the clinically relevant service as determined and rendered by the practitioner.
• demonstrate repeated or wilful non-compliance by a person or entity.
• involve fraud - we use mechanisms to detect and investigate fraud, as required by the Public
Governance, Performance and Accountability Rule 2014.
In addition to the above, in 2021-22, the Department will concentrate on the following compliance priorities:
Referrals, Requests and Prescriptions
A valid referral, request or prescription helps to ensure that patients receive the right
treatment at the right time. Where invalid documents are used, patient care can be
compromised, and in some cases, health program funds can be obtained fraudulently.
The department prioritises compliance in relation to claiming for services or dispensing
of medicines that occurs without a valid referral, request or prescription, or when they
are provided in excess of what is specified.
Telehealth and Vaccine Administration
Telehealth arrangements and payments for the administration of vaccines have
been introduced in response to the pandemic, and to service the evolving needs of
Australian patients. Practitioners are key to ensuring that these arrangements are
used for the purposes for which they were intended.
Claims are being evaluated to ensure that the rules and requirements for vaccine,
telehealth and associated services are met. Claiming data is used to detect patterns
that may indicate these services are being misused. This includes practices such
as the use of telehealth items for ‘pre-consultation screenings’ or co-claiming of
attendances and vaccine services without clinical justification.
Practice Incentive Payments
Practice incentive payments support general practices to provide quality care,
enhance capacity, and improve access and health outcomes for patients. These
outcomes are compromised when the requirements for these payments are not met.
The Department is increasing the rigour applied to analysing claims for incentive
payments. This includes supporting policy and payment system improvements,
increased eligibility checks and post payment compliance activities.
Practices that receive incentive payments are responsible for ensuring that the
requirements have been met prior to the payment being received. They should also ensure
that they can supply evidence of compliance with these requirements upon request.
3 Health Provider Compliance Strategy 2021/22Corporate Compliance
Arrangements between an organisation and a practitioner that remove the
practitioner’s control over their claiming or undermine the practitioner’s clinical
independence are detrimental to the integrity of health programs.
The Department is prioritising reform of the compliance program to support
enforcement action where we believe that an organisation or corporate health provider
is engaged in over-servicing or the provision of low value care for the purpose of
maximising Medicare revenue. Claiming administered by a person other than the
treating practitioner must reflect the provision of the clinically relevant service as
determined and rendered by that practitioner.
Compliance Approach
The Department’s overarching provider compliance model ensures that resources and effort are prioritised
based on the seriousness and scale of compliance concerns. This allows for a responsive and proportionate
approach to compliance utilising the wide range of tools and powers available to the Department.
Figure 1: Compliance Model
*Note that this is not an escalation model. Our response to instances of non-compliance will correspond with the type and
seriousness of the behaviour.
4 Health Provider Compliance Strategy 2021/22Identifying Non-Compliance Information about potential non‑compliance is received from a range of sources including tip‑offs from the public and healthcare professionals, data analysis and referrals from other agencies and stakeholders. Targeted data analysis and intelligence collection are used to investigate concerns and identify providers whose registration, approval, or claiming patterns raise compliance concerns. The results of these detection techniques are validated through human analysis, including review by health professionals, compliance officers and experts. Engagement with our stakeholders is relied upon to help us understand the nature of the concerns and environmental factors that might be relevant. Figure 2: Compliance Action Compliance Activities The Department recognises that most non-compliance is inadvertent and works with providers to resolve issues and promote good compliance practices. Compliance activities are targeted to the type of non-compliance identified. This allows for a responsive and proportionate approach to addressing compliance concerns. Letters Where there are concerns about approval, billing or claiming by a provider, early intervention letters are used to provide information and guidance on appropriate access to health program payments. These letters are not an audit or formal review. If you receive a letter, you are encouraged to reflect on how you are complying with the rules and requirements for health programs and make changes if required. You may also be requested to review your records and voluntarily repay any non-compliant claiming that you identify. 5 Health Provider Compliance Strategy 2021/22
Example
New rules were introduced in July 2020 that require all medical practitioners working in general
practice settings to have an established clinical relationship with a patient before using the
COVID-19 telehealth items for consultations. Our analysis of claiming data identified that
approximately 2.5% of all COVID-19 telehealth services may not have met this requirement.
A number of virtual practices had been established that capitalised on COVID-19 telehealth
items and were providing these services to patients with whom they had no established
clinical relationship.
Targeted letters were sent to practitioners to invite them to review their claiming practices and
to repay claims for ineligible services. This enabled practitioners who had misunderstood the
requirements remediate their claims and ensure that future claims were compliant.
These letters resulted in the identification of $688,725 of inappropriately claimed MBS services.
Audit
An audit is an assessment of whether a claim for a health program benefit was correctly made.
This process is usually commenced with a request for information or documents from the practitioner
to assist in determining whether the rules and requirements for that claim were met.
If the rules were not met, the provider may have a debt raised against them because false or misleading
information was provided as part of the claiming process. False or misleading information can be found to
have been provided even in circumstances where there was no intention to defraud or to be dishonest and
an error has occurred.
Compliance audits are conducted in relation to claims for services under the:
• Medicare Benefits Schedule (MBS)
• Pharmaceutical Benefits Scheme (PBS)
• Child Dental Benefits Schedule (CDBS)
Example
Analysis of Medicare claiming data indicated that a practitioner was incorrectly billing multiple
initial consultation MBS items using the same referral.
Following a review of the documentation used to support the claims, the practitioner was
found to have been non-compliant for over sixty percent of approximately six hundred services
audited. They had incorrectly claimed payments where referrals had expired, had been used for
more than one initial consultation, were incomplete or missing, or the service had not met the
requirements for an initial consultation.
The practitioner accepted the findings and agreed to repay over $30,000 in incorrect payments.
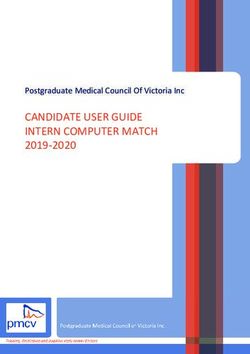
6 Health Provider Compliance Strategy 2021/22Professional Review
If analysis indicates that a practitioner may be rendering or initiating health services in a manner unacceptable to
a body of their peers, a review may be undertaken under the Practitioner Review Program (PRP). Concerns may
include providing services that do not meet MBS, PBS or legislative requirements or are not clinically relevant.
These reviews are conducted by a Professional Advisor (a health practitioner) and involve reviewing a
practitioner’s claiming/servicing data to identify whether their behaviour varies from their peers. In most
circumstances, practitioners are provided several opportunities to explain their practice and respond to any
concerns. Where concerns have been resolved, cases may be closed at any stage in the PRP process.
The seriousness of the concern or the potential that inappropriate practice may be occurring,
will determine the approach taken under the PRP.
Where the concerns are not resolved under the PRP, practitioners or a corporate entity may be referred
to the Director of Professional Services Review.
Figure 3: Practitioner Review Program Process
*Note – This is a high-level representation of the PRP process. For further detail see Professional reviews - a practitioner guide.
Example
Through routine compliance data analysis, a cardiologist was referred to the Department’s
Practitioner Review Program because their claiming was at a much higher level than their peers. The
practitioner was interviewed by a medical advisor and offered six months to review and remediate
their practice. As there was no change in billing practice over this period, the practitioner was invited
to make a submission. The delegate reviewed the submission and remained concerned that the
practitioner may be engaged in inappropriate practice.
The case was accepted by the Professional Services Review, who found that MBS requirements
were not always met. The Director of Professional Services Review and practitioner entered into an
agreement under section 92 of the Health Insurance Act 1973. The practitioner acknowledged they
had engaged in inappropriate practice, agreed to repay $100,000 and was disqualified from providing
the Medicare services in question.
7 Health Provider Compliance Strategy 2021/22Civil and Administrative Enforcement Behaviours that influence, or result in, approvals and claiming that pose a risk to the integrity of health programs may also be investigated for breaches of civil and administrative penalty provisions in our legislation. Prohibited Practices in Relation to Pathology and Diagnostic Imaging Healthcare providers have responsibility to patients to recommend pathology and diagnostic imaging providers, based on the patient’s clinical needs and best interests. Allowing this recommendation to be influenced by commercial arrangements between the practitioner and the provider can compromise patient outcomes and lead to over servicing. Legislation prescribes several prohibited practices aimed at preventing inducements to request pathology and diagnostic imaging services. Where it is suspected that healthcare organisations may be engaging in these practices, investigations may be undertaken. This can result in civil litigation to enforce financial penalties. These provisions carry civil and criminal penalties of up to five years imprisonment for anyone breaking these laws. Pharmaceutical Services Federal Committee of Inquiry The Pharmaceutical Services Federal Committee of Inquiry was established to investigate matters of non- compliance with conditions of approval for approved pharmacists. It is a peer review body which inquires into the conduct of approved pharmacists and reports its findings to the Minister, who has the power to issue sanctions (reprimand, suspend or revoke the pharmacist’s approval to supply PBS medicines). The Committee may investigate a matter referred to it by the Minister or the Secretary that relates to the services or conduct of approved pharmacists in connection with the supply of pharmaceutical benefits under Part VII of the National Health Act 1953. The Committee has broad ranging powers that enable it to summon witnesses to appear before it and produce specific evidence. Public Hospital Compliance – Duplicate Payments As part of the 2020-2025 Addendum to the National Health Reform Agreement (NHRA), the Australian Government and all States and Territories committed to ensuring the integrity of public hospital and Medicare payments through detecting and addressing duplicate payments. As part of this commitment, all parties to the NHRA agreed that public hospital funding and Medicare data will be matched on a yearly basis and, where there are concerns about potential duplication of payments, matched data will be provided to the Department of Health for compliance purposes. 8 Health Provider Compliance Strategy 2021/22
Serious Non-Compliance
Fraud against the Commonwealth is a criminal offence that directly impacts Australians. It diverts tax-
payer funds from important public health initiatives, can deny patients access to health services to which
they are entitled and undermines public confidence in the health system and health professions. If a
person is suspected of intentionally obtaining or attempting to obtain a health payment by deception, we
may undertake a criminal investigation. Criminal investigations can result in prosecution and reparation
orders made by the courts. The decision to prosecute is made by the Commonwealth Director of Public
Prosecutions (CDPP).
Example
Following a tip-off, an investigation identified a psychologist practicing in two locations had
submitted fraudulent claims totalling $720,000 for services never provided to patients. A Brief
of Evidence was referred to the CDPP and following charges being laid, the provider entered a
plea of guilty to eight counts of breach section 135.2(1) Criminal Code Act 1995.
The psychologist was sentenced to imprisonment for three years and a reparation order was
issued requiring the repayment of the full amount of the fraudulently claimed money.
Example
Several tip-offs were received in relation to the fraudulent claiming of cancer drugs and insulin
by an approved pharmacist. This included information from an employee of the pharmacist
reporting discrepancies in dispensing software, stock anomalies, and unusual claiming patterns.
Another health practitioner reported their prescriber number, and those of other prescribers, had
been used by the pharmacist to claim prescription items.
An investigation identified the pharmacist had lodged 524 fraudulent PBS claims without
supplying the medicines to patients. As a result, a total of $365,922 in pharmaceutical benefits
were fraudulently claimed.
The Department referred a Brief of Evidence to the CDPP and following charges being laid, the
pharmacist entered a plea of guilty to two counts of dishonestly intending to obtain a gain under
the Criminal Code Act 1995. They were convicted and sentenced to 18 months imprisonment,
served in the community by way of an Intensive Correction Order. A reparation order was issued
for the full fraud amount of the fraud.
Example
In separate tip-offs, members of the public alleged that an exercise physiologist had claimed
Medicare services that were not provided to them.
The investigation identified that the practitioner had submitted fraudulent documents purporting
to be an accredited exercise physiologist in order to obtain a Medicare provider number. A total
of 627 claims for 14,500 services were submitted and $486,215 was paid in Medicare benefits.
The practitioner was found guilty of one count of using a forged document with intention that
it is accepted as genuine by a Commonwealth public official; and one count of obtaining a
financial advantage by deception. On appeal, the practitioner was convicted and sentenced to
imprisonment for one year and nine months with a non-parole period of nine months.
A reparation order was issued for the full amount of the fraud.
9 Health Provider Compliance Strategy 2021/22Our Responsibilities
Compliance Program Principles
The Department strives to ensure that the Compliance Program is administered in accordance with
our principles:
Accountability – compliance decisions are made in accordance with clearly defined governance
processes and legislative requirements. Our processes, procedures and policies regularly undergo internal
and external review to ensure our compliance with our obligations and objectives.
Fairness – structures and systems are in place to support fairness. These include:
• providing the tools, information and means for practitioners to comply voluntarily
• taking formal compliance action only where it is necessary and appropriate
• making administrative law decisions that are consistent with the principles of procedural fairness
• balancing the rights of the individual with the expectations and values of healthcare professionals,
the community and government
• working with practitioners and peak bodies to minimise non-compliance through consultation,
education and collaboration.
Flexibility – while there is an obligation to comply with legislation, flexibility is applied wherever possible by:
• recognising health professionals may experience increased demands and pressures, especially
during times of emergency such as bushfires, floods and pandemics
• considering the unique circumstances of practitioners that could explain anomalous claiming patterns
• working with practitioners to resolve compliance issues.
Proportionality – our compliance program is designed to apply proportionate actions and outcomes
based on the risk and seriousness of the behaviour, harms to patients and the Medicare system, and the
intent of the parties involved.
Timeliness – compliance and enforcement activities are completed in a timely way to minimise uncertainty
for the practitioner or organisation.
Conduct and Values
The Department upholds and complies with the APS Code of Conduct and APS Values that are set out
in the Public Service Act 1999. No matter why you are contacted by our compliance staff, you can and
should always expect:
• to be treated with respect
• to be given quality information
• fair and transparent service
• genuine consultation
• efficiency in the conduct of our processes.
10 Health Provider Compliance Strategy 2021/22Procedural Fairness and Review Rights
Procedural fairness when making administrative law decisions means the Department will:
• avoid actual and perceived conflicts of interest and act in an impartial and objective manner
• afford a person or organisation a reasonable opportunity to be heard and/or respond to the case
before making an adverse decision affecting their interests.
This supports decisions that are fair, reasonable and made without bias.
Privacy
Your personal information will be handled in a way that protects your privacy in line with the Privacy
Act 1988 (Cth) (Privacy Act). This includes the Australian Privacy Principles (APPs) and the Australian
Government Agencies Privacy Code. The Department’s Privacy Policy can be found on our website.
In addition, the Health Insurance Act 1973 and National Health Act 1953 contain a range of secrecy
provisions that further protect your sensitive information when undertaking our compliance and
enforcement role.
Supporting Compliance
Education and Preventative Action
Supporting practitioners, healthcare organisations and peak bodies to correctly claim health payments
through education, engagement and consultation is our preferred method for achieving compliance.
Education and support offerings are being expanded across multiple platforms and services, including
AskMBS, e-learning, online resources and advisories. More information on these resources can be
found here.
Payment Systems and Policy Change
The Department engages with a wide range of stakeholders including health profession and industry peak
bodies, medical colleges as well as health program policy areas in the Department and Services Australia.
This engagement supports better Medicare compliance outcomes through program design, policy
development and payment system improvements.
Legislative Reform
The nature of health practice in Australia is rapidly evolving and presents new challenges for practitioners
and the Compliance Program. Periodic reviews and amendments of our legislative framework are
undertaken to ensure the continued relevance and effectiveness of our compliance program.
How to Report Non-Compliance
The Department is committed to preventing the occurrence of fraud or other inappropriate claiming of
health program payments. Specific concerns relating to a practitioner or healthcare organisation are
received through the tip-off form and the 1800 314 808 Provider Benefits Integrity Hotline.
Tip-offs can be made anonymously.
11 Health Provider Compliance Strategy 2021/22Resources
Where to find Support and Education
Additional information and resources on health payment programs compliance and enforcement for practitioners include
the following.
AskMBS - The AskMBS email service responds to enquiries from providers of services listed on the MBS seeking advice on
the interpretation of MBS items, explanatory notes and associated legislation.
More information about AskMBS can be found on the AskMBS Email Advice Service page.
Record Keeping - Guidelines for administrative and clinical record keeping can be found at the Department of Health website
on the Administrative record keeping guidelines for health professionals page.
Medicare Billing Toolkit - Information to assist with the prevention of non-compliance and to assist healthcare professionals
to bill correctly can be found at the Compliance education for health professionals Medicare Billing Assurance Toolkit on the
Department of Health website.
Services Australia - Services Australia is responsible for the administration of Medicare. More information can be found on
the Services Australia website at Medicare information for health professionals.
E-learning
Introduction to compliance within Medicare - This is a three module introductory course targeted at practitioners and
designed to help practitioners understand compliance. The course can be accessed on the Department of Health’s website
at: Introduction to Compliance within Medicare.
Doctor Portal Learning – Medicare Billing Compliance - Practitioner compliance continuing professional development
modules on Medicare Billing Compliance, Introducing Medicare Billing, Understanding Compliance Regulations and
Procedures, Billing & Record Keeping, Substantiating Claims and Voluntary Acknowledgement are available at
Medicare Billing Compliance on the CDP learning website.
Billing Medicare in public hospitals - Online learning for practitioners billing Medicare in public hospitals can be found at
the Department of Health website on Billing Medicare in Public Hospitals.
Medicare Program Information
Medicare Benefits Schedule - Information on the MBS, eligible services and the rules under which services are subsidised
can be found on MBS Online.
Pharmaceutical Benefits Scheme - Information on the PBS and subsidised medicines can be found on the Pharmaceutical
Benefits Scheme (PBS) website.
Child Dental Benefits Schedule - Information about the CDBS is available at: The Child Dental Benefits Schedule page on
the Department of Health website.
Practice Incentive Programs - Information about PIP can be found on the Services Australia website at the Practice Incentives
Program page.
Pathology and Diagnostic Imaging - Guidance on prohibited practices in relation to pathology and diagnostic imaging can
be found in The Red Book on the Department of Health website.
Compliance Contacts
Key contact details can be found on the Department of Health website at Provider Benefits Integrity Division contact information.
These contacts include:
• Review of Compliance Audit Decision
• Pathology Rents
• Tip-Offs
• Voluntary Acknowledgement of Incorrect Payments
12 Health Provider Compliance Strategy 2021/22health.gov.au
DT0001686
All information in this publication is correct as at July 2021.You can also read