Hormonal Treatments for Major Depressive Disorder: State of the Art
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
REVIEWS AND OVERVIEWS
Hormonal Treatments for Major Depressive Disorder:
State of the Art
Jennifer B. Dwyer, M.D., Ph.D., Awais Aftab, M.D., Alik Widge, M.D., Ph.D., Carolyn I. Rodriguez, M.D., Ph.D.,
Linda L. Carpenter, M.D., Charles B. Nemeroff, M.D., Ph.D., Ned H. Kalin, M.D., APA Council of Research
Task Force on Novel Biomarkers and Treatments
Major depressive disorder is a common psychiatric disorder hypothalamic-pituitary-gonadal (HPG) axes and review the
associated with marked suffering, morbidity, mortality, and evidence for selected hormone-based interventions for the
cost. The World Health Organization projects that by 2030, treatment of depression in order to provide an update on
major depression will be the leading cause of disease bur- the state of this field for clinicians and researchers. The
den worldwide. While numerous treatments for major de- review focuses on the HPA axis–based interventions of
pression exist, many patients do not respond adequately corticotropin-releasing factor antagonists and the gluco-
to traditional antidepressants. Thus, more effective treat- corticoid receptor antagonist mifepristone, the HPT axis–
ments for major depression are needed, and targeting cer- based treatments of thyroid hormones (T3 and T4), and
tain hormonal systems is a conceptually based approach the HPG axis–based treatments of estrogen replacement
that has shown promise in the treatment of this disorder. A therapy, the progesterone derivative allopregnanolone, and
number of hormones and hormone-manipulating com- testosterone. While some treatments have largely failed to
pounds have been evaluated as monotherapies or ad- translate from preclinical studies, others have shown
junctive treatments for major depression, with therapeutic promising initial results and represent active fields of study
actions attributable not only to the modulation of endocrine in the search for novel effective treatments for major
systems in the periphery but also to the CNS effects of depression.
hormones on non-endocrine brain circuitry. The authors
describe the physiology of the hypothalamic-pituitary-
adrenal (HPA), hypothalamic-pituitary thyroid (HPT), and AJP in Advance (doi: 10.1176/appi.ajp.2020.19080848)
Major depressive disorder is a common psychiatric disorder approach that has shown promise in the treatment of major
that is associated with marked suffering, morbidity, mortality, depression.
and cost (1, 2). The lifetime prevalence of major depression in Alterations in hormones and endocrine function may play
adults in the United States is estimated to be 17% (3); prev- an important role in mechanisms underlying the patho-
alence is higher in women than men (21% and 13%, re- physiology of major depression. Primary abnormalities in
spectively) (4), and 12-month prevalence is approximately 7% the adrenal, thyroid, and gonadal axes are associated with
(5). In 2010 the economic cost of depression in the United alterations in mood, and medications that target endo-
States was estimated to be $210 billion (2). The World Health crine function are often accompanied by mood-related and
Organization projects that worldwide, major depression will cognitive effects. These clinical observations prompted
be the leading cause of disease burden by 2030 (6). While exploration of the roles that hormones may play in the
numerous treatments for major depression exist, many pa- pathophysiology of major depression and of potential treat-
tients do not respond adequately to traditional antidepres- ment approaches targeting specific hormonal systems. A
sants. In the Sequenced Treatment Alternatives to Relieve number of hormones and hormone-manipulating compounds
Depression (STAR*D) trial, one-third of patients with major have been evaluated as monotherapies or adjunctive treatments
depression experienced a remission of depressive symptoms for major depression, with therapeutic actions attributable
with their first antidepressant trial of citalopram, and only not only to the modulation of endocrine systems in the pe-
two-thirds of patients overall cumulatively experienced a riphery but also to the CNS effects of hormones on non-
remission after four sequential treatments (7). Thus, more endocrine brain circuitry. Here we review the evidence for
effective treatments for major depression are needed. Tar- clinically relevant interventions for the treatment of depression
geting certain hormonal systems is a conceptually based that are based on the hypothalamic-pituitary-adrenal (HPA),
ajp in Advance ajp.psychiatryonline.org 1HORMONAL TREATMENTS FOR MAJOR DEPRESSIVE DISORDER
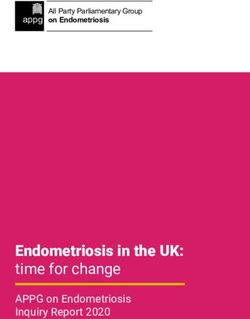
FIGURE 1. Hypothalamic-pituitary-adrenal (HPA) axisa peripheral circulation, ACTH acts on the adrenal cortex,
stimulating the synthesis and secretion of glucocorticoids
Cortex, hippocampus, thalamus (e.g., cortisol) into the systemic circulation. A cortisol-
binding globulin, transcortin, is found in plasma, and when
cortisol is bound to transcortin, it is unable to interact with its
Hypothalamus (PVN) receptors (11). AVP is also produced locally in the adrenal
Negative Negative
feedback CRF feedback
medulla and can stimulate release of cortisol, underscoring its
AVP role as a positive HPA regulator (12).
Anterior pituitary gland In the periphery and the brain, cortisol acts via two distinct
modes of signaling: membrane-bound glucocorticoid re-
ACTH ceptors that activate rapid protein kinase signaling, and the
more classic, protracted nuclear receptor signaling, in which
Adrenal glands
intracellular glucocorticoid receptors translocate to the nu-
cleus to transcriptionally regulate gene expression (13, 14).
Two receptors bind cortisol: the mineralocorticoid receptor
Glucocorticoids (MR) and the glucocorticoid receptor (GR). The MR has a
higher affinity for cortisol than the GR, and this greater
sensitivity to low cortisol concentrations allows it to regulate
Glucocorticoid receptors
physiological fluctuations in HPA activity (e.g., the circadian
Mineralocorticoid receptors
rhythm of cortisol release). The MR is also thought to play an
important role in inhibiting HPA axis activity (15) that is
a
In the HPA axis, the paraventricular nucleus of the hypothalamus (PVN) associated with adaptive coping and resilience to stress (16).
releases corticotropin-releasing factor (CRF) and, to a lesser extent,
arginine-vasopressin (AVP). These factors stimulate the anterior pi- The lower-affinity GR is better suited to detecting high
tuitary to release adrenocorticotropic hormone (ACTH) into the pe- cortisol concentrations, such as those released during the
ripheral circulation, which stimulates the adrenal glands to release stress response. Although the expression of the MR is re-
glucocorticoids (e.g., cortisol). Glucocorticoids act on both gluco-
corticoid receptors and mineralocorticoid receptors. Negative feed- stricted to limbic brain regions, the GR is expressed much
back occurs at the level of the pituitary, the hypothalamus, and more widely, highlighting the broad impact that cortisol can
higher brain structures (e.g., cortex, hippocampus, and periventricular have in modulating brain function.
thalamus).
When intracellular glucocorticoid receptors are activated,
they translocate to the nucleus and bind to glucocorticoid
hypothalamic-pituitary thyroid (HPT), and hypothalamic- response elements on DNA to activate or repress gene ex-
pituitary-gonadal (HPG) axes. pression to mediate the diverse set of responses to stress and
to efficiently terminate the stress response, a concept known
as feedback inhibition. Glucocorticoid receptor–mediated
HYPOTHALAMIC-PITUITARY-ADRENAL AXIS
negative feedback occurs at multiple levels and via several
Overview of Physiology mechanisms within the CNS and pituitary (Figure 1). At the
The HPA axis is a critical endocrine system that orchestrates level of the hypothalamus and pituitary, both rapid inhibition
the stress response, a complex set of behavioral, neuroen- via fast, membrane-bound signaling (17, 18) and slower nu-
docrine, autonomic, and immune responses enabling adap- clear receptor–mediated transcriptional repression of the
tation to aversive psychological and physiological stimuli genes that produce CRF and ACTH exist (19). The GR also can
(8). The main components of the HPA axis are the para- down-regulate its own activity in response to cortisol via
ventricular nucleus (PVN) of the hypothalamus, the anterior transcriptional induction of the chaperone protein FK506
lobe of the pituitary gland, and the adrenal cortex. binding protein 5 (FKBP5), which sequesters the GR in the
The principal central initiator of HPA axis activity cytoplasm, preventing it from entering the nucleus (20).
is corticotropin-releasing factor (CRF), also termed corticotropin- Glucocorticoid receptors also mediate feedback inhibition
releasing hormone (9), a peptide secreted by the PVN in more indirectly via limbic areas such as the hippocampus (21),
response to stress (Figure 1). CRF is released into the paraventricular thalamus (22), and prefrontal cortex (23),
hypothalamo-hypophyseal portal system and stimulates which likely play a larger role in the processing of psycho-
the release of adrenocorticotropic hormone (ACTH) from logical versus physiological stressors (21). The regulation of
the anterior pituitary into the systemic circulation. Another negative feedback within the HPA axis is complex but crit-
hypothalamic peptide, arginine-vasopressin (AVP), either ically important in modulating adaptive responses to stress,
can be released into the hypophyseal portal system like CRF that is, creating a system that can quickly respond to a
or can be released from axon terminals in the posterior pi- stressor, and then efficiently terminate, reset, and await the
tuitary. AVP synergistically enhances ACTH release in next event.
combination with CRF, an action that may be especially In addition to the classic endocrine functions of the HPA
relevant in states of chronic stress (10). Once released into the axis, the hypothalamic peptides (CRF, and to a lesser extent
2 ajp.psychiatryonline.org ajp in AdvanceDWYER ET AL.
AVP) also regulate neural circuits relevant to stress, anxiety, treat major depression. Several strategies showed initial
and mood processing. CRF is a member of a family of pep- promise in small clinical trials but were subsequently
tides and is expressed not only in the PVN but also in limbic abandoned. These strategies included cortisol synthesis in-
regions, including the central nucleus of the amygdala, cere- hibitors in patients with major depression with or without
brocortical areas, and the brainstem (24). CRF’s two pre- hypercortisolemia, glucocorticoids in patients with major
dominant receptors (CRFR1 and CRFR2) also have significant depression with hypocortisolemia, and vasopressin receptor
extrahypothalamic expression. A binding protein, CRFBP, is antagonists. For example, the cortisol synthesis inhibitor
thought to modulate CRF activity by preventing its access to metyrapone showed positive antidepressant effects as an
its receptors. Taken together, the extrahypothalamic roles of augmentation agent in several small trials (Ns ranging from
the CRF system are critically important, and alterations in six to nine) (41–44) and one larger double-blind inpatient
these systems have been implicated in the pathogenesis of study (N=63) (45); however, a larger multisite randomized
affective and anxiety disorders. controlled trial (N=165) was negative (46). Stimulation of
MRs (e.g., with the MR agonist fludrocortisone) is also a
HPA Abnormalities in Major Depression strategy under investigation (47). Treatments focused on the
Early work on the pathophysiology of depression suggested CRF and GR systems have been the most extensively studied,
hyperactivity of the HPA axis and impairment in its sensi- and here we discuss these approaches in more depth: CRFR1
tivity to negative feedback regulation in major depression, antagonists, driven by highly promising preclinical data but
although more recent investigations suggest a much more which have so far not proved effective in humans, and the GR
complex picture. Alterations at every level of the HPA system antagonist mifepristone, which shows promise in the treat-
have been reported, although these reports have not always ment of major depression with psychotic features and re-
been replicated, and the various reported alterations may mains an active area of investigation.
occur only in subsets of individuals with major depression.
In general, patients with major depression are reported to CRFR1 antagonists. The potential of CRFR1 antagonists
exhibit hyperactivity of the HPA axis, with impaired sensi- generated considerable interest given the preclinical and
tivity to negative feedback; however, subsets of patients clinical evidence implicating excess CRF production in the
with hypocortisolemia have been reported (25). It is note- pathophysiology of major depression. Preclinical studies
worthy that HPA axis overactivity appears to be particu- showed that central injection or overexpression of CRF in
larly enriched in the melancholic and psychotic depression certain brain areas such as the amygdala generates anxious
subtypes (26–28). and depressive phenotypes, and that CRFR1 antagonists
While HPA axis abnormalities have been studied in large block these behavioral manifestations (48–50). The human
numbers of patients (e.g., a meta-analysis including over studies suggesting hyperactivity of the CRF system in major
18,000 individuals [29]), results are heterogeneous overall depression and its resolution with antidepressant treatment
and effect sizes modest. That said, the most prominently (51) bolstered the rationale for targeting this system directly.
reported HPA axis alterations associated with depression Despite initial positive results (52), this line of research has
include 1) blunted cortisol circadian rhythms with elevated suffered from a series of disappointments. Two early com-
levels late in the day (29); 2) negative feedback insensitivity, pounds were abandoned because of hepatotoxicity (R-121919
as characterized by a failure to suppress morning cortisol and PF-00572778), and subsequent double-blind, placebo-
after the administration of dexamethasone (30); 3) in- controlled trials yielded negative results or were stopped
creased release of cortisol in response to exogenously ad- early because of lack of efficacy (ONO-2333 Ms [N=278] [50],
ministered ACTH (31); 4) blunted ACTH in response to CRF CP-316,311 [N=123] [53], BMS-562086 [N=260 for generalized
administration (32); 5) exaggerated ACTH and cortisol anxiety disorder (54); trial ended unpublished for major
responses in the combined dexamethasone-CRF test (33, depression]). Although the current CRFR1 antagonists do not
34); 6) increased cerebrospinal fluid CRF concentrations appear to have efficacy as a monotherapy for major de-
(35, 36); and 7) down-regulation of brain CRHR1 receptors pression, there appears to be value in further studying novel
and mRNA, hypothesized to reflect compensatory changes compounds with different pharmacokinetic profiles in sub-
to persistently high CRF concentrations (37). Additionally, populations selected for functional genetic alterations in the
genetic studies have identified single-nucleotide polymor- CRF system (38). Moreover, the lack of a positron-emission
phisms (SNPs) in genes relevant to the stress response, tomography ligand to assess receptor occupancy of the
modulators of glucocorticoid function (e.g., GR, FKBP5), CRFR1 antagonist has precluded an understanding of
and the CRF system (e.g., CRFR1, CRFR2, CRFBP) that are whether the doses used were sufficient to adequately test the
associated with major depression and/or potentially related efficacy of this strategy. In addition, these compounds have
to treatment response (38–40). never been tested in combination with other antidepressants.
Strategies targeting the other major CRF receptor (CRF2) and
HPA Axis–Based Treatments for Major Depression the CRF binding protein could also be useful. According to
A number of strategies have attempted to modulate HPA ClinicalTrials.gov, no current CRF antagonist trials are ac-
function and/or extrahypothalamic targets as an approach to tively recruiting patients.
ajp in Advance ajp.psychiatryonline.org 3HORMONAL TREATMENTS FOR MAJOR DEPRESSIVE DISORDER
GR antagonists. GR antagonists have been tested primarily in be replicated in clinical trials specifically designed to test
depression with psychotic features for the following reasons: this hypothesis. Although mifepristone is associated with
1) patients with Cushing’s syndrome and patients receiving some gastrointestinal side effects and headache, very few
high-dose exogenous glucocorticoids often have marked patients discontinued because of side effects. These data
mood and psychotic symptoms; 2) effective treatment of the are a promising start and represent a nontraditional dos-
endocrine abnormality in these patients frequently reverses ing advantage of a time-limited treatment with persisting
these symptoms; and 3) HPA axis abnormalities are enriched benefit (at least 56 days). Multiple studies of mifepristone
in patients with major depression with psychotic features are listed on ClinicalTrials.gov, typically as an adjunctive
(39). Preclinical data from animal models of depression treatment in depression (to ECT in nonpsychotic depression
supported the use of GR antagonists as augmenting agents, [NCT00285818] and to a mood stabilizer in bipolar de-
enhancing both the speed of effect and the overall efficacy of pression [NCT00043654]), and also as a monotherapy for
SSRIs (55). Small early studies with ketoconazole, an anti- alcohol use disorder (NCT02179749) (63). Neurocognitive
fungal medication that also antagonizes GR receptors and symptoms associated with psychiatric disorders are another
inhibits cortisol synthesis, showed mixed results: antide- interesting potential application, as patients with bipolar
pressant effects in an open study (43) of multiple cortisol disorder treated with mifepristone show improvements in
synthesis inhibitors (N=17); antidepressant effects in hyper- spatial working memory (64). Of note, other GR antagonists
cortisolemic but not eucortisolemic patients in a double- with better selectivity for the GR receptor are being de-
blind study (N=20) (56); and no significant antidepressant veloped and tested, which underscores the level of inter-
effects in a double-blind study (N=16) (57). Mifepristone, est and activity in exploring the therapeutic use of GR
which antagonizes both the GR and the progesterone re- antagonists.
ceptor, has been the most rigorously tested GR antagonist.
The mifepristone studies are unusual in that participants Summary of HPA axis–targeted interventions. Overall, the
received the medication for 7 days, and symptoms were strongest support for HPA axis interventions in the treat-
measured 1 week later, 1 month later, and even later, when ment of depression is for the use of GR antagonists for the
patients were on standard antidepressant monotherapy. treatment of psychotic symptoms in psychotic depression
Although results from individual clinical trials have been (Table 1). While variation in response in individual mifep-
somewhat inconsistent (see Table S1 in the online supple- ristone clinical trials occurred, combined reanalysis of all trial
ment), a summary of seven clinical trials, five of them data supports efficacy, especially when plasma levels are
double-blind (Ns ranging from five to 433), suggests that considered. Despite considerable preclinical data, the clinical
mifepristone has efficacy in reducing psychotic symptoms, trial literature does not support the use of currently available
the primary outcomes of the trials. Two double-blind trials CRFR1 antagonists for the treatment of major depression or
showed a significant difference in the proportion of res- other psychiatric disorders. Other HPA-based treatments
ponders to mifepristone compared with placebo (response (e.g., cortisol synthesis inhibitors, glucocorticoids, and va-
was defined as a reduction of 50% in score on the positive sopressin receptor antagonists) have been tested in small
symptom subscale of the Brief Psychiatric Rating Scale clinical trials, and together the evidence does not support
[BPRS] [58] and a 30% reduction in the full BPRS score [59]). their use in clinical practice.
Depressive symptoms were considered as secondary outcomes
in these trials and often did not show a separation from
HYPOTHALAMIC-PITUITARY-THYROID (HPT) AXIS
placebo (60).
Notably, mifepristone’s effectiveness appears to be opti- Overview of Physiology
mized when it attains a plasma level of ;1600 ng/mL, which Thyroxine (T4) and triiodothyronine (T3) are the two pri-
equates to roughly 1200 mg/day orally (61). Thus, inadequate mary thyroid hormones, and they are responsible for regu-
dosing may explain the results of some earlier trials that did lation of metabolism and protein synthesis throughout the
not show significant differences from placebo (58). Indeed, body (65). Thyrotropin-releasing hormone (TRH), primarily
a recent study combining and reanalyzing the data from released from neurons that originate in the hypothalamic
five placebo-controlled trials (mifepristone, N=833; placebo, PVN, regulates the release of thyroid-stimulating hormone
N=627) showed that when patients with psychotic major (TSH) from the anterior pituitary gland (Figure 2). TSH
depression achieved therapeutic plasma levels, a robust stimulates the production of T4 and, to a lesser degree, T3
improvement in psychotic symptoms was observed, starting from the thyroid gland. Serum free T4 and free T3 levels
at 28 days and lasting through 56 days, the last time point regulate pituitary TSH release through negative feedback. T4
examined, with a number needed to treat of 7 (compared with is primarily converted by the tissue deiodinases into the more
48 for patients with low plasma mifepristone levels) (62). biologically active T3 and the inactive metabolite reverse T3.
Patients with high mifepristone plasma levels also showed a Thyroid hormones are highly protein bound, and it is only the
reduction in depressive symptoms relative to patients in the free fraction that is biologically available. Effects of thyroid
placebo group, while patients with low mifepristone plasma hormones are primarily mediated by their binding to nuclear
levels did not (62). These are intriguing findings that should receptors that transcriptionally regulate gene expression.
4 ajp.psychiatryonline.org ajp in AdvanceDWYER ET AL.
TABLE 1. Summary of evidence for hormonal treatments for major depressive disordera
Intervention Disorder/Population Level of Evidence
CRF1 antagonists Major depression Strong evidence of no benefit
GR antagonists (e.g., mifepristone) Major depression with psychotic Moderate evidence of efficacy for psychotic
features symptoms if minimum plasma level achieved;
additional prospective studies needed
T3 augmentation of antidepressants Treatment-resistant major Moderate evidence of efficacy; efficacy of
depression augmentation with SSRIs requires demonstration
in placebo-controlled trials
T3 for acceleration of antidepressant Major depression Strong evidence of efficacy
effect with TCAs
T3 for acceleration of antidepressant Major depression Strong evidence of no benefit
effect with SSRIs
Estrogen replacement therapy Perimenopausal women with Moderate evidence of efficacy
(or combined hormone major depression and physical
replacement therapy) menopause symptoms
Estrogen replacement therapy Perimenopausal women without Weak evidence of benefit
(or combined hormone major depression (prevention)
replacement therapy)
Estrogen replacement therapy Postmenopausal women with Poor as monotherapy, preliminary evidence as
(or combined hormone major depression adjunct to SSRIs in geriatric depression
replacement therapy)
Oral contraceptives PMDD Moderate evidence of efficacy for drospirenone-
containing oral contraceptives, weak evidence of
efficacy for other oral contraceptives, despite
being considered second-line treatment after
SSRIs
Allopregnanolone stabilization PMDD Moderate evidence of efficacy
Allopregnanolone enhancement Postpartum depression Strong evidence of efficacy
Testosterone replacement Depressive symptoms secondary Strong evidence of efficacy
therapy to clinical hypogonadism
Testosterone augmentation Subthreshold depressive Preliminary evidence of efficacy
symptoms
in men without clinical
hypogonadism
Testosterone augmentation Treatment-resistant major Strong evidence of no benefit
depression
in men without clinical
hypogonadism
a
CRF1=corticotropin-releasing factor receptor 1; GR=glucocorticoid receptor; PMDD=postmenstrual dysphoric disorder; SSRI=selective serotonin reuptake
inhibitor; TCA=tricyclic antidepressant.
Thyroid receptors have two predominant isoforms, TRa1 and number of transport proteins, including transthyretin (67).
TRb1, with varying sensitivity to T4 and to T3. TRa1 is the Transthyretin is secreted into the CSF by the choroid plexus
predominant isoform in the brain, and while it is activated by and is the primary CSF carrier of T4. Lower levels of
both T3 and T4, it has heightened sensitivity to T4 compared transthyretin have been reported in the CSF of depressed
with TRb1. T3 and T4 enter the brain either directly across patients compared with control subjects, and this has been
the blood-brain barrier or indirectly across the choroid suggested to lead to a state of “brain hypothyroidism” despite
plexus epithelium into cerebrospinal fluid (CSF) (66, 67). normal peripheral thyroid hormone levels (69). This concept
The transport across the blood-brain barrier happens via a remains speculative, because in animal studies, rodents with
number of identified and unidentified transporter proteins, absent transthyretin maintain normal T3 and T4 levels in
such as MCT8 or OATP1C1. Although both T3 and T4 are brain as a result of additional transport systems (70).
transported from circulation into the CNS, T4 is thought to be
transported in preference to T3 (66, 67). In the brain, deio- HPT Abnormalities in Major Depression
dinase 2 in astrocytes is the primary enzyme that converts T4 Clinical hypothyroidism is frequently associated with de-
into T3, which is critical for the local generation of T3 that pressive symptoms (71), and subclinical hypothyroidism
interacts with neurons. Deiodinase 3, another CNS thyroid (defined as elevated serum TSH with normal serum T3 and
enzyme, is selectively expressed in neurons. Deiodinase T4 levels) is commonly reported in treatment-resistant de-
3 inactivates both T4 and T3 by deiodination (66, 68). Thyroid pression (72, 73). However, most patients with depression do
hormones in the CSF help maintain the brain interstitial not have biochemical evidence of thyroid dysfunction (69,
levels of thyroid hormones. T4 is carried in the CSF via a 74). Other reported abnormalities in depression include TSH
ajp in Advance ajp.psychiatryonline.org 5HORMONAL TREATMENTS FOR MAJOR DEPRESSIVE DISORDER
FIGURE 2. Hypothalamic-pituitary-thyroid (HPT) axisa Acceleration of antidepressant effect with tricyclic
antidepressants. Research investigating this effect began with
Hypothalamus (PVN) TCAs before the approval of the use of SSRIs, which occurred
Negative Negative in the late 1980s. T3 treatment initiated within 5 days of
feedback feedback
TRH initiating TCA treatment produced a faster onset of antide-
pressant response compared with the TCA alone. Evidence
Anterior pituitary gland
for this accelerated response comes primarily from a meta-
TSH analysis of six double-blind placebo-controlled studies
(N=125) of T3 use with imipramine and amitriptyline (79). In
Thyroid gland the pooled analysis, T3 significantly accelerated the clinical
response compared with placebo, with a moderate effect size
(0.58). These trials were of short duration (less than 4 weeks),
and the time to response was generally within 7–14 days in the
T4 T3
T3 plus TCA treatment, compared with 21–28 days for the
Deiodinases
placebo plus TCA comparator. The typical dosage of T3 used
in these studies was 25 mg/day. In three of the studies, T3 was
Thyroid receptors
discontinued after 2–4 weeks, but in all three studies, par-
ticipants remained well after T3 discontinuation. Of note, the
a
In the HPT axis, the paraventricular nucleus of the hypothalamus (PVN) effect size for accelerated response with T3 in the meta-
releases thyroid-releasing hormone (TRH), which stimulates the anterior
pituitary to release thyroid-stimulating hormone (TSH) into the peripheral analysis increased as the percentage of women participating
circulation. The thyroid gland then releases T4 and T3 into the circulation. in the study increased, suggesting that women may be more
Circulating T4 can also be converted to T3 via deiodinases. These hor- likely than men to benefit from the addition of T3, a finding
mones act on thyroid receptors in target organs and as a means of reg-
ulating negative feedback at the level of the hypothalamus and pituitary. that warrants further investigation.
Evidence from randomized controlled trials indicates that
levels in the “normal” but high range, low T3 levels, elevated this acceleration of antidepressant response is not general-
T4 levels, elevated reverse T3 levels, a blunted TSH response izable to all classes of antidepressants: T3 accelerates re-
to TRH, positive antithyroid antibodies, and elevated CSF sponses to TCAs but does not appear to have this effect with
TRH concentrations (69). Abnormalities in the HPT axis in SSRIs. A meta-analysis of four placebo-controlled random-
depression have mostly been demonstrated in cross-sectional ized controlled trials of patients with major depression
studies; data from larger longitudinal prospective studies are (N=444) found no evidence for a quicker response onset
scarce, and findings have been inconsistent (75, 76). The when T3 was used in combination with SSRIs (80). Reasons
literature suggests a link between subtle thyroid dysfunc- for the discrepancy between the effects of T3 with TCAs
tion and major depression, but more conclusive data are compared with SSRIs remain unknown.
needed (77). Augmentation strategy for inadequate response to antide-
pressant monotherapy. Evidence for T3 augmentation efficacy
HPT Axis–Based Treatments for Major Depression with TCAs comes from a meta-analysis of eight controlled
T3, T4, TRH, and TSH have all been investigated as potential trials (N=292) in patients with major depression who did not
treatments for major depression. Aside from T3, hormones experience remission with TCA treatment alone (81). Four of
of the thyroid axis either appear to lack efficacy or have not these studies used a randomized double-blind design; of the
been well-studied in major depression. T4 has been studied, other four, three were unblinded studies with retrospective
with promising results, in bipolar disorder, particularly in cohorts and one was a double-blind trial in which each pa-
rapid-cycling bipolar disorder. A number of small placebo- tient served as his or her own control. Patients receiving
controlled studies have evaluated intravenous and oral TRH T3 augmentation were twice as likely to respond to TCAs
administration, and the majority have not demonstrated than those receiving placebo augmentation, with a 23% im-
efficacy for TRH in the treatment of depression (71). A provement in response rates. Improvements in depression
1970 study in women reported rapid augmentation of re- scores were moderately large (effect size, 0.62). However,
sponse with a tricyclic antidepressant (TCA) after in- across studies, there was inconsistent evidence of efficacy,
travenous administration of TSH compared with placebo and study quality varied. Although the two larger double-
(78), but no subsequent clinical trials have been reported. blind randomized controlled trials (N=33 and N=38) were
robustly positive in favor of T3 augmentation, pooled results
Triiodothyronine (T3). The bulk of evidence suggests that T3 of the four double-blind randomized controlled trials were
has clinical utility in depression for two purposes: to accel- not significant (p=0.29). One negative randomized controlled
erate antidepressant response when used with tricyclic trial included in this analysis was particularly problematic
antidepressants, and as an augmentation agent to treat de- because of a 2-week crossover design and unequal baseline
pression in patients with insufficient response to antide- depression severity in the randomized groups. This may
pressant monotherapy. partly explain the negative pooled results for the four
6 ajp.psychiatryonline.org ajp in AdvanceDWYER ET AL. double-blind randomized controlled trials. Among the trials nervousness, and palpitations, T3 administration has been included in the meta-analysis, only one established relative well tolerated without serious side effects (85). Thyroid treatment resistance on the basis of an antidepressant monitoring guidelines proposed by Rosenthal et al. (65) for T3 treatment duration of 6 weeks, which is now considered the augmentation recommend assessing TSH, free T4, and free minimum duration for determining lack of response. In T3 levels at baseline, at 3 months, and then every 6–12 months. addition to the controlled trials, additional support for the Because hyperthyroidism can induce bone resorption leading use of T3 as augmentation with TCAs comes from five to an increased risk of fractures, monitoring bone density positive open-label studies with reported response rates every 2 years is recommended with use of thyroid hormones greater than 50% (71). in postmenopausal women. Notably, no placebo-controlled trials have demonstrated the efficacy of T3 augmentation with SSRIs or serotonin- Thyroxine (T4). Limited evidence from small open-label norepinephrine reuptake inhibitors in treatment-resistant studies using T4 as an augmentation agent in major de- depression. The only placebo-controlled trial to have ex- pression exists, but the efficacy of T4 remains to be estab- amined this hypothesis was a small trial with a treatment lished in placebo-controlled randomized controlled trials duration of 2 weeks that reported negative results (82). (86). While T4 is understudied in unipolar depression, Support for this approach for patients with treatment- supraphysiological doses of T4 (250–500 mg/day) have been resistant depression comes primarily from level 3 of STAR*D, investigated as maintenance treatment in rapid-cycling bi- in which response to T3 augmentation (up to 50 mg/day; polar disorder as well as in treatment-resistant bipolar de- N=73) was compared with lithium augmentation (up to pression, with generally favorable results (87). Bauer and 900 mg/day; N=69) or a new antidepressant monotherapy Whybrow (88) were the first to conduct an open-label trial of (mirtazapine or nortriptyline). All participants who entered adjunctive supraphysiological doses of T4, in 11 patients with level 3 had not experienced remission of depression after at treatment-refractory rapid-cycling bipolar disorder, with least two different medication treatments. These participants improvement in both depressive and manic symptoms, and did not respond with prospective citalopram treatment in this finding was replicated in additional open-label studies level 1 and with medication switch (bupropion, sertraline, or (87). Recently, the first comparative double-blind placebo- venlafaxine) or medication augmentation (bupropion or controlled trial of T4 and T3 as adjunctive treatments was buspirone) in level 2 (83). Remission rates were 25% with T3 conducted in 32 patients with treatment-resistant rapid- augmentation and 16% with lithium augmentation after a cycling bipolar disorder (89). Participants in the T4 group mean treatment duration of about 10 weeks. This difference spent significantly less time in a depressed or mixed state and was not statistically significant. T3 had superior tolerability, greater time euthymic, whereas there were no significant as lithium was more frequently associated with side effects differences with T3 and placebo (89). and greater rates of discontinuation. Supraphysiologic doses of T4 have also been studied in The efficacy of T3 augmentation in depression was also open-label trials as adjunctive therapy for treatment- demonstrated in a network meta-analysis of 48 randomized resistant bipolar depression, and beneficial effects have controlled trials investigating the efficacy of 11 different been noted on depressive symptoms, with response rates augmentation agents in treatment-resistant depression. around 50% (87). A randomized double-blind placebo- These trials consisted of direct comparisons between the controlled study of 300 mg of T4 as an adjunct to mood drugs as well as comparisons with placebo. Six trials of stabilizers and/or antidepressants in bipolar depression thyroid hormone augmentation (T3 or T4) were included. (N=62) showed improvements in depression, but the overall The odds of remission in treatment-resistant depression were results were not statistically significant because of a high three times greater with thyroid hormone augmentation placebo response rate (90). Significant improvement in de- compared with placebo, with comparable tolerability (84). pression compared with placebo, however, was noted in a Given the tremendous variability of the design of the T3 trials secondary analysis of female participants. and their failure to establish treatment resistance, the results Overall, these studies show promising evidence for ad- of the network analysis should be viewed cautiously. junctive use of supraphysiological doses of T4 in rapid- A meta-analysis of four randomized controlled trials found cycling bipolar disorder (87), while more research is no evidence that adding T3 to SSRIs enhanced the antide- needed for use of T4 in acute bipolar depression. pressant effect of SSRI treatment in depressed patients who were not antidepressant treatment resistant (80). While HPT axis: conclusions. Evidence from randomized controlled the STAR*D findings suggest that T3 is beneficial as an trials with TCAs and from STAR*D suggests clinical benefits augmentation agent with SSRIs in treatment-resistant de- of T3 as an augmentation agent with antidepressants in pa- pression, this benefit remains to be demonstrated in ran- tients with major depression who have not responded to domized placebo-controlled trials. antidepressant monotherapy. This conclusion is consistent T3 has been reported overall to be safe and tolerable. with practice guidelines for the pharmacological treatment of Although a small number of participants in clinical trials major depression from the American Psychiatric Association, have experienced side effects such as sweating, tremor, the Canadian Network for Mood and Anxiety Treatments, ajp in Advance ajp.psychiatryonline.org 7
HORMONAL TREATMENTS FOR MAJOR DEPRESSIVE DISORDER
and the World Federation of Societies of Biological Psychi- The actions of estradiol are primarily mediated by two
atry, which recommend augmentation of antidepressants nuclear estrogen receptors (ERs), ERa and ERb, which
with thyroid hormones as a treatment option in cases where modulate gene transcription by binding to estrogen response
monotherapy has failed (91–93). Clinicians also recommend elements on DNA (97). There is also some evidence for fast-
using thyroid hormone supplementation in patients with acting membrane-bound estrogen receptor signaling (98).
depression who do not respond, especially in patients with ERs are expressed in the brain in males and females with
TSH levels in the high normal range (94). Researchers should largely similar distributions, although with higher receptor
aim to demonstrate, in future placebo-controlled trials, the numbers in females (99). ERa is thought primarily to mediate
efficacy of T3 as an augmentation agent with SSRIs in reproductive functions given its high expression in a number
treatment-resistant depression. In addition to use as aug- of hypothalamic nuclei (100). Preclinical gene knockout
mentation, evidence from multiple randomized controlled studies suggest that ERb may regulate estradiol-mediated
trials supports use of T3 for acceleration of antidepressant effects on HPA activity and mood, via its expression in the
response with TCAs, with the important caveat that this PVN and limbic system (100).
acceleration of antidepressant response has not been ob- In addition to HPG axis regulation, progesterone also has
served in randomized controlled trials with SSRIs. Also, important CNS effects. Like estradiol, progesterone acts
promising evidence supports adjunctive use of supra- both through classic nuclear receptor signaling (pro-
physiological doses of T4 in rapid-cycling bipolar disor- gesterone receptors [PRs]) and also likely via fast-acting
der, and emerging evidence supports use of T4 in bipolar membrane-bound receptors (101). PRs are found in the
depression. hypothalamus, hippocampus, cortex, and amygdala, and in
general PR activation is thought to oppose the actions of
estradiol (102). Progesterone has been largely considered
HYPOTHALAMIC-PITUITARY-GONADAL (HPG) AXIS:
neuroprotective, in part via PR-mediated stimulation of
OVARIAN HORMONES
growth factors and activation of glial cells (101). Although a
Overview of Physiology relatively large number of animal studies and small clinical
In men and women, the major hypothalamic driver of the trials have examined progesterone’s effects in the context of
HPG axis is the pulsatile secretion of gonadotropin-releasing stroke and traumatic brain injury, two recent large ran-
hormone (GnRH), released from neurons residing in the domized controlled trials showed no protective effects after
medial preoptic area (Figure 3A). In response to GnRH, the brain injury (103, 104). Within psychiatry, there has been a
anterior pituitary releases luteinizing hormone (LH) and greater focus on the actions of the progesterone metabolite
follicle-stimulating hormone (FSH) into the bloodstream, allopregnanolone. Allopregnanolone is a neuroactive ste-
stimulating the ovaries to produce estradiol and progester- roid that acts as a positive allosteric modulator at synaptic
one, and the testicles to produce testosterone (Figure 3B). As and extrasynaptic GABAA receptors. It has been implicated
is common in endocrine systems, these hormones regulate as a mediator of many of the central effects attributed to
axis activity via feedback inhibition, with estradiol, pro- progesterone and is being actively investigated in clinical
gesterone, and testosterone inhibiting HPG axis activity at trials (see next section).
both the level of the hypothalamus and the pituitary (95). The
function of these sex hormones is also subject to modulation Ovarian Hormone Abnormalities in Major Depression
by binding to albumin and more specific binding proteins, Considerable clinical evidence demonstrates that fluctua-
which control hormone access to tissues and receptors (96). tions in ovarian hormones are associated with increased risk
In women, a complex feedback interplay regulates the ap- of depressive states. Women experience depression at nearly
proximately 28-day menstrual cycle (Figure 3C), character- twice the rate of men, a difference that is apparent only during
ized by 1) a follicular phase of approximately 14 days in which the reproductive years (105). Some women experience severe
LH and FSH levels are relatively low and estradiol steadily affective symptoms during the late luteal phase of their
climbs; 2) a short ovulation phase triggered by a burst of monthly cycle as progesterone and its metabolite, allopreg-
GnRH release and rapid rise of LH, triggering the release of an nanolone, progressively rise, then rapidly fall (see Figure
ovarian follicle; and 3) a 14-day luteal phase in which LH and 3C), a syndrome termed premenstrual dysphoric disorder
FSH return to relatively low levels and the corpus luteum of (PMDD) (106). An increased risk of mood symptoms and
the ovary produces increased estradiol and progesterone, major depressive disorder occurs during other periods of
stimulating proliferation of the endometrial lining. In the ovarian hormone withdrawal, including the postpartum
absence of pregnancy, estradiol and progesterone levels de- period and menopause. These findings are complemented by
cline near the end of the luteal phase, and menses proceeds. preclinical studies showing enhanced depressive-like be-
As discussed below, periods of significant hormonal change, haviors in rodents during low-estradiol times of the cycle
including the monthly end of the luteal phase, and more (107), increased behavioral despair following ovariectomy
specific endocrine events, including puberty, pregnancy, and that can be rescued with estradiol administration (108), and
menopause, are associated with mood changes and increased the ability of estradiol to enhance the release of monoamines
risk for affective disorders. (109).
8 ajp.psychiatryonline.org ajp in AdvanceDWYER ET AL.
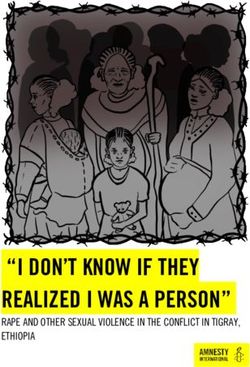
FIGURE 3. Hypothalamic-pituitary-gonadal (HPG) axis, steroid hormone synthesis, and the menstrual cyclea
A. Hypothalamic-Pituitary-Gonadal Axis B. Steroid Hormone Synthesis
Hypothalamus (mPOA) Cholesterol
Negative Negative
feedback feedback
GnRH
Anterior pituitary gland Pregnenolone
LH and FSH
Gonads Allopregnanolone Progesterone DHEA
(Ovaries) (Testes) 5D-reductase
Dehydrotestosterone Testosterone
Estradiol and Testosterone 5D-reductase
Progesterone Aromatase
Steroid hormone receptors Estradiol
C. Menstrual Cycle
Anterior FSH
pituitary
hormones LH
Progesterone
Ovarian Estradiol
hormones
Menses
Days 0 -------- Follicular Phase-------- 14 -------- Luteal Phase -------- 28
Ovulation
a
As shown in panel A, in the HPG axis, the medial preoptic area of the hypothalamus (mPOA) releases gonadotropin-releasing hormone (GnRH), which
stimulates the anterior pituitary to release luteinizing hormone (LH) and follicle-stimulating hormone (FSH) into the peripheral circulation. These factors
stimulate the gonads to produce sex hormones, with the ovaries producing estradiol and progesterone and the testes producing testosterone. Panel B
summarizes steroid hormone synthesis: Cholesterol is the precursor molecule to sex hormones, which can undergo a variety of enzymatic trans-
formations. DHEA=dehydroepiandrosterone. As shown in panel C, after the menstrual cycle begins at day 0 with the occurrence of menses, estradiol
gradually climbs during the follicular phase (days 0 through 14 of a 28-day cycle). Ovulation is triggered by the spike in anterior pituitary production of
luteinizing hormone (LH) and follicle-stimulating hormone (FSH). During the luteal phase (days 14 through 28), progesterone and, to a lesser extent,
estradiol rise. The production of both hormones then begins to fall toward the end of the luteal phase, a time of vulnerability for premenstrual dysphoric
disorder symptoms. In the absence of pregnancy, falling ovarian hormone levels lead to the shedding of the uterine lining with menses, beginning the
cycle again.
However, the impact of ovarian hormones on mood is suicidal acts, with significant risk for all hormone prepara-
complex, as demonstrated in the literature on oral contra- tions (larger effects in progestin-only products, transdermal
ceptives, which are commonly prescribed for pregnancy patches, and vaginal rings compared with combination oral
prevention or to normalize irregular menstrual cycles. Al- preparations), as well as pronounced effects in the adolescent
though oral contraceptives have long been linked with the age group (110, 111). In contrast, a smaller cross-sectional
potential to alter mood, there has been significant contro- study described an increased risk of mood disorders with
versy over whether they worsen mood, improve mood, have progestin-only oral contraceptives but a decreased risk of
more complex mood effects, or are mood neutral. Two large mood disorders when women using combined estrogen-
prospective studies examining health records of more than progestin oral contraceptives were compared with those
1 million Danish women over 10 years showed that oral taking no contraception (112). A systematic review of studies
contraceptive use is associated with increased risk for sub- of progestin-only contraception, however, reported no con-
sequent antidepressant treatment, depression diagnosis, and sistent evidence of association with depressive symptoms
ajp in Advance ajp.psychiatryonline.org 9HORMONAL TREATMENTS FOR MAJOR DEPRESSIVE DISORDER
across 26 studies, most of which were deemed by the authors of estrogen replacement therapy with reduced risks (e.g.,
as low quality or at significant risk of bias (113). A randomized endometrial and breast cancer risk). Their pharmacology,
controlled trial of 178 women from a community sample however, is complex, and SERMs also carry significant risks.
(,9% meeting criteria for a depressive disorder or currently For example, while tamoxifen decreases ER-positive breast
on antidepressants) described an even more nuanced picture, cancer risk as a result of ER antagonism, it carries a risk of
in which oral contraceptives were associated with a wors- uterine cancer as a result of endometrial ER agonism (124).
ening of mood symptoms in the intermenstrual phase in Raloxifene received a U.S. Food and Drug Administration
a subset of women, but an improvement in mood during (FDA) black box warning for increased risk of deep vein
the premenstrual phase (114). Despite these changes in thrombosis, pulmonary embolism, and death due to stroke in
mood symptoms, no difference was detected between oral at-risk postmenopausal women. While the evidence for
contraceptives and placebo in the emergence of clinical SERMs in the treatment of major depression is equivocal,
depression as assessed with the Montgomery-Åsberg De- evidence is developing for use of SERMs as an adjunctive
pression Rating Scale (114). The literature is further com- treatment for mania (125) and psychosis (126) in women and
plicated by differences in dosing schedules (e.g., monophasic men. These antimanic and antipsychotic actions are thought
versus triphasic oral contraceptive preparations), and it has to result from SERM inhibition of the protein kinase C second
been suggested that regimens with more constant hor- messenger cascade, and a number of placebo-controlled
mone distributions may carry less risk of adverse mood clinical trials are under way to examine their use for acute
effects (115). mania and schizophrenia.
The impact of oral contraceptives may also depend on the Oxytocin, which is not an ovarian hormone per se, but is
endocrine context. For example, women with polycystic a neuropeptide that plays important roles in postpartum
ovary syndrome, a disorder characterized by polycystic bonding and social cognition more broadly, has also been
ovaries, elevated androgen output, and irregular menstrua- studied in major depression. Although preclinical work has
tion, have higher rates of depression and anxiety (116), and suggested that oxytocin is a promising target, clinical trials
oral contraceptives are associated with an improvement in have not yielded convincing results for the treatment of major
depressive symptoms and health-related quality of life (117). depression or postpartum depression, although it is still being
Taken together, these complicated data, which are limited by actively studied in these disorders.
high interstudy variability in hormone preparation, dosing Here we will focus in more depth on the use of estrogen
schedule, population studied, and mood measures, suggest replacement therapy, given its clinical relevance in current
that ovarian hormones can have a significant impact on mood psychiatric practice, as well as the emerging study of the
but point to an intricate underlying biology that is sensitive to progesterone-derived neurosteroid allopregnanolone in
age, timing within the menstrual cycle, and administered PMDD, postpartum depression, and a variety of other psy-
hormone (estrogens versus progestins). chiatric conditions.
Ovarian Hormone Treatments for Major Depression Estrogen replacement therapy (ERT) or hormone replacement
The ovarian hormone treatment literature is complicated by therapy (HRT; estrogen and progestin) in peri- or post-
differences in study populations, with some trials examining menopausal major depression. Hormone replacement therapy
affective symptoms in euthymic women who receive hor- is FDA approved to treat the vasomotor symptoms (hot
mones for medical indications and other trials that di- flashes) and vulvovaginal atrophy associated with meno-
rectly study hormone-based interventions in psychiatrically pause. Women who have received a hysterectomy may take
ill populations (generally women with major depression, oral estrogen replacement therapy, whereas women with an
postpartum depression, or PMDD). Many different ovarian intact uterus must take hormone replacement therapy (es-
hormone–based strategies have been evaluated for their ef- trogen plus a progestin) to mitigate endometrial cancer risk
fects on depressed mood. Treatment guidelines suggest that posed by unopposed estrogen. Clinical trials examining mood
suppression of ovulation (118) via oral contraceptives (with in peri- and postmenopausal women treated with hormone
specific evidence for those containing the antiandrogenic replacement have yielded mixed results for several reasons.
progestin, drospirenone, with a 4-day pill-free interval [119, One complicating factor is the difference in psychiatric
120], and mixed evidence for other oral contraceptives [121]) symptomatology across studies, with the majority of studies
and GnRH agonists (e.g., leuprolide [122]) may be effective in assessing one or two mood symptoms in psychiatrically
the treatment of PMDD, although compared with SSRIs, asymptomatic women (often excluding those with major
these treatments are considered second and third line, re- depressive disorder), and a minority of studies examining
spectively (123). effects in women meeting criteria for major depressive dis-
An interesting literature reports on the use of selective order or dysthymia (109). A second complicating factor is
estrogen receptor modulators (SERMs) in psychiatric dis- treatment timing in relationship to menopause onset. Peri-
orders. SERMs (e.g., tamoxifen, raloxifene) act as estrogen menopause appears to be a distinct neuroendocrine state
receptor agonists in some tissues and antagonists in others, compared with postmenopause, with different ERT/HRT
and it was hoped that they would provide some of the benefits risks and benefits, depending on the timing of hormone
10 ajp.psychiatryonline.org ajp in AdvanceDWYER ET AL.
administration. This differential risk was initially described Studies examining mood after ERT/HRT in women
for cardiovascular risk in the exhaustive analyses of the large without psychiatric illness comprise 19 of the 24 trials de-
Women’s Health Initiative study and in subsequent trials scribed in the recent meta-analysis (109). The overall grade of
(127). In the Early Versus Late Postmenopausal Treatment the evidence in this meta-analysis was a C (i.e., low-quality
With Estradiol (ELITE) trial, a cardioprotective effect of evidence), and in these 19 trials evaluating mood in non-
ERT/HRT was observed in early menopausal women (,6 depressed women, there was little evidence of benefit, par-
years after menopause), but a risk-enhancing effect was found ticularly in women without other physical symptoms of
in women .10 years after menopause (128). ERT/HRT menopause (109). In contrast to the conclusion of the meta-
timing is important not only for understanding the general analysis, two more recent trials suggested some benefit or
medical risks of treatment, but it also appears to influence the protective effects of ERT/HRT in these groups. The Kronos
efficacy of these treatments for depressive symptoms. Ad- Early Estrogen Prevention Study (KEEPS) followed 661
ditional complicating factors in studies of perimenopausal women in the community over 4 years who received oral
women include the spontaneous return of ovarian function estrogen plus progesterone, transdermal estrogen plus pro-
(adding temporary, unpredictable endogenous sources of gesterone, or placebo. Women with clinical depression, de-
estradiol) and the co-occurring symptoms of menopause (e.g., fined as a score .28 on the Beck Depression Inventory, were
hot flashes and sleep disturbance), which can have their own excluded, but women with mild to moderate mood symptoms
impact on mood and may be responsive to HRT (129). who were being treated with an antidepressant were in-
Relatively few studies have directly tested ERT/HRT as an cluded. Improvements in depressive symptoms (effect size,
antidepressant monotherapy in peri- or postmenopausal 0.49) and anxiety (effect size, 0.26) were observed in the oral
women with major depression, comprising only five of the estrogen plus progesterone group compared with the placebo
24 trials assessing mood that were included in a recent meta- group over the course of 4 years of treatment, whereas the
analysis (109). Of these five trials conducted in depressed, transdermal estrogen group did not separate from placebo
unmedicated women, two were considered to be at high risk of (137). Another study of 172 euthymic peri- and post-
bias. Both potentially biased studies were conducted in younger menopausal women found that those in early menopausal
postmenopausal women and included one positive trial (N=129) transition (but not those in late transition or postmenopausal)
with high attrition rates (32% in the HRT group and 57% in the treated with 12 months of transdermal estrogen plus oral
placebo group) (130) and one negative trial that had baseline progesterone had a lower risk of developing depressive
differences in presence of prior episodes of major depression symptoms (138). These benefits were moderated by the
(N=57; HRT did not separate from placebo, although both number of stressful life events experienced over the pre-
groups improved) (131). Of the three higher-quality studies in ceding 6 months, with greater antidepressant effects in those
depressed women, two (132, 133) showed antidepressant effi- women with the highest number of stressful life events (138).
cacy of ERT (transdermal patches) compared with placebo in Taken together, this complex literature suggests with
perimenopausal women (N=34 and N=50). The third examined some confidence that ERT/HRT interventions are most likely
a mixed population of peri- and postmenopausal women and to be successful when implemented early in the transition to
showed that increased estradiol levels (spontaneously occur- menopause. The most clear-cut indication for the use of HRT
ring or due to ERT) were associated with depression improve- is for perimenopausal women experiencing depression who
ment in perimenopausal women (N=72) but not postmenopausal also are experiencing significant physical symptoms of
women, although both groups improved symptomatically com- menopause (e.g., hot flashes, vaginal dryness), for which
pared with the placebo group (129). time-limited HRT is already FDA approved. The use of
ERT has also been evaluated as an adjunctive treatment to ERT/HRT in late or postmenopausal women has little evidence
SSRIs. In a retrospective analysis of a multisite randomized for efficacy and is associated with increased risk for car-
controlled trial of fluoxetine in participants with geriatric diovascular events (as opposed to a protective cardiac risk
depression, women who were receiving ERT (not as a ran- profile in perimenopausal women) (127), and therefore
domized intervention, N=72) showed greater improvement should be avoided. The more ambiguous cases are those of
on fluoxetine than those who were not receiving ERT perimenopausal women who are depressed but do not have
(N=295) (134). Small studies prospectively assessing ERT in FDA-approved symptoms for HRT (some evidence for an-
conjunction with an antidepressant in postmenopausal tidepressant efficacy has been reported in this group [109]).
women have shown either no effect (135) or an acceleration, Although some studies suggest that HRT is a preventive
but not an augmentation effect (136). These studies warrant strategy for developing depression in perimenopausal women
cautious interpretation given the limitations of a high dropout (138), more evidence is needed (139).
rate (one-third of the sample [135]) and baseline differences in
age and depression severity between treatment groups (136). Progesterone and its neurosteroid derivative, allopregnanolone.
While the evidence base is relatively small, these studies Progesterone and its metabolite allopregnanolone have
suggest that ERT/HRT may have some antidepressant effi- been implicated in hormone-related mood disorders, in-
cacy in perimenopausal women, with less convincing data for cluding PMDD and postpartum depression, resulting in
postmenopausal women. multiple clinical trials targeting this system. Allopregnanolone
ajp in Advance ajp.psychiatryonline.org 11You can also read