ORIGINAL ARTICLE Hypogonadism is associated with overt depression symptoms in men with erectile dysfunction
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
International Journal of Impotence Research (2008) 20, 157–161
& 2008 Nature Publishing Group All rights reserved 0955-9930/08 $30.00
www.nature.com/ijir
ORIGINAL ARTICLE
Hypogonadism is associated with overt depression symptoms
in men with erectile dysfunction
AA Makhlouf1, MA Mohamed2, AD Seftel3 and C Neiderberger4
1
Department of Urologic Surgery, University of Minnesota, Minneapolis, MN, USA; 2Urology Department El-Minia
University Hospital, El-Minia, Egypt; 3Department of Urology, Case Western Reserve University, University Hospitals
of Cleveland, Cleveland, OH, USA and 4Department of Urology, University of Illinois at Chicago, Chicago, IL, USA
Depression and hypogonadism are associated with erectile dysfunction (ED). We evaluated the
prevalence of both conditions in men presenting to an ED specialty clinic, and tested whether
hypogonadism correlated with the presence of depressive symptoms using a validated ques-
tionnaire. From July 2001 to June 2003, 157 men referred to an ED specialty clinic prospectively
filled the Center for Epidemiologic Studies Depression Scale (CES-D), the abbreviated International
Index of Erectile Function (IIEF-5) and had testosterone serum levels drawn. Median age was 53
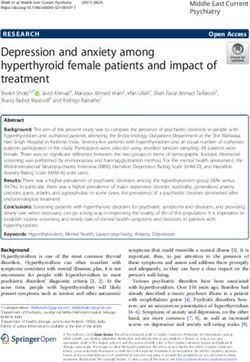
(range ¼ 21–85 years). Hypogonadism, defined as serum T (testosterone)o300 mg/dl, was present in
36% of patients. This proportion was higher in men over the median age compared to younger
patients (45 and 26%, respectively, P ¼ 0.002). Overt depression symptoms, defined as a CES-DX22,
were found in 24% of men. Mean age of men with overt depression was 49.9710.1 years vs
55.1715.8 years for those with CES-Do22 (P ¼ 0.02). Hypogonadal men were more likely to have
overt depression scores compared to eugonadal counterparts (35 vs 18%, P ¼ 0.02). This association
was statistically stronger after correcting for age in a multivariate linear model (P ¼ 0.005). The
relative risk of having overt depression was 1.94 times higher in men with hypogonadal testosterone
level (95% confidence interval: 1.13 to 3.7). We conclude that in an ED referral population,
symptoms of hypogonadism and depression symptoms are fairly prevalent, and that overt
depression symptoms are strongly associated with hypogonadism. Clinicians should consider
testosterone measurements in all men with high depression symptom scores.
International Journal of Impotence Research (2008) 20, 157–161; doi:10.1038/sj.ijir.3901576;
published online 16 August 2007
Keywords: depression; testosterone; erectile dysfunction; hypogonadism; diagnosis; IIEF
Introduction Depression was associated with 1.8-fold increase
in the prevalence of ED in the Massachussetts Male
Testosterone levels decline gradually in aging men, Aging Study independent of age or the traditional
with about 20% of men over 60 years having total organic comorbidities associated with ED.2,5 The
testosterone levels dip below the accepted normal prevalence of depression in large epidemiological
threshold.1 This drop in androgen levels parallels an studies of ED has been reported as ranging from 11
increase in the prevalence of erectile dysfunction to 25%.6,7 Even higher rates (25–55%) were reported
(ED).2 Testosterone supplementation has been in men attending andrology clinics.8,9 Furthermore,
shown to improve erectile function and rescue Shabsigh et al.8 found that patients with ED and
sildenafil failures.3,4 Thus, there is a clear incentive concomitant depression were more likely to dis-
for urologists to identify men with hypogonadism. continue therapy, making assessment of depression
symptoms an important aspect of ED evaluation.
There is an overlap between symptoms of hypo-
gonadism and depression. One study has found
that men with hypogonadal testosterone values are
Correspondence: Dr AA Makhlouf, Department of Urologic
Surgery, University of Minnesota, 420 Delaware St SE MMC
at higher risk of developing depression,10 while
394, Minneapolis, MN 55455, USA. others have not.5,11 In this paper, we examine
E-mail: makhl001@umn.edu the correlation between depression symptoms and
Received 18 November 2006; revised 3 March 2007; hypogonadsim in men attending an ED clinic. We
accepted 1 May 2007; published online 16 August 2007 specifically determine if men with hypogonadismDepression and hypogonadism associated in ED
AA Makhlouf et al
158
and depression form an overlapping sub-population Table 1 Summary data for all patients in the study
of ED patients.
Mean Median Range
Age (years) 53.8714.8 53 21–85
Methods IIEF-5 11.276.3 11 0–25
CES-D 15.178.8 15 0–40
Testosterone (ng/dl) 414.47206 369 21–1182
Total serum testosterone levels were obtained from
185 consecutive patients presenting to an andrology Abbreviations: BPH, benign prostatic hyperplasia; CAD, coronary
specialty clinic with a chief complaint of ED artery disease; CES-D, Center for Epidemiologic Studies Depres-
between July 2001 and June 2003. Samples were sion Scale; HTN, hypertension; IIEF-5, International Index of
drawn in the morning hours in most patients with Erectile Function-5.
rare exceptions. The Center of Epidemiologic Study Major comorbidites by patient-self report: diabetes, 21; Peyronie’s,
4; BPH, 3; depression, 3; CAD, 2; HTN, 2; prostate cancer, 1.
Depression questionnaire (CES-D) and the five-
question International Index of Erectile Function
(IIEF-5) was administered as measures of depression
and erectile function, respectively. The CES-D is an
Hypogonadism by Age Group
inventory of 20 questions on a 4-point scale, with a 0.5
score of 16–21 suggestive of mild or reactive *
depression, whereas a score of 22 or higher
corresponding to signs of overt depression.12,13 0.4
The IIEF-5 is widely used and validated measure
Proportion with TDepression and hypogonadism associated in ED
AA Makhlouf et al
159
are fairly prevalent in an ED clinic population, and Androgen deficiency is associated with a variety
that there is increased likelihood of finding depres- of symptoms in aging men.15 In addition to physical
sion among men with hypogonadism. signs such as loss of muscle mass and bone density,
low testosterone values are associated with forget-
fulness, insomnia, depressed mood and low sex
Table 2 2 2 contingency table showing the correlation of drive.15 Androgen blockade in prostate cancer
hypogonadism with presence or absence of overt depression patients leads to a rise in depression and anxiety
symptoms.
symptoms and weakening of verbal memory.16,17 In
Mild or no depression Overt Sxs (CES-D 421; contrast, testosterone supplementation leads to an
symptoms (CES-D n ¼ 38) improvement in the sense of well being and a rise in
p21; n ¼ 117) libido.18 Because of the effects of mood and libido
on sexual performance, we determined the rate of
Normal T 82 (82%) 18 (18%) hypogonadism in an ED referral population. Using a
Low T 37 (65%) 20 (35%) sensitive cutoff of 300 ng/dl, we found testosterone
(o300 ng/dl)
deficiency in 36% of men, while a more stringent
Abbreviations: CES-D, Center for Epidemiologic Studies Depres-
cutoff of 200 ng/dl gave a rate of 9.5%. Regardless of
sion Scale; CI, confidence intervals; T, testosterone. cutoff, hypogonadism was more common in men
The relative risk of having overt depression if hypogonadal group over the median age. Total testosterone levels did
is 1.95 higher than in eugonadal men (95% CI: 1.3–3.4). not correlate with severity of ED as measured by the
P ¼ 0.02 by w2 test. IIEF-5, even after correction for age (data not
shown). This agrees with Shabsigh et al.,3 who did
not find a correlation between Sexual Health
Inventory for Men (SHIM) score and testosterone
Normal T level in men supplemented with testosterone for ED.
T < 300 ng/dl Overall, our rate of hypogonadism was higher than
that reported for community men in general.1
0.6
Recognition of testosterone deficiency is important
since testosterone supplementation can rescue
0.5 sildenafil failures.3 This effect of testosterone is
p < 0.05
likely due to stabilization of neuronal nitric oxide
Proportion of patients
0.4 synthase expression,19 although other mechanisms
such as prevention of smooth muscle cell loss
0.3 through apoptosis have been proposed.20
Previous epidemiological studies have found a
strong correlation between the presence of ED and
0.2
depression. In a multinational survey of over 27 000
men, Rosen et al.21 found depression to be twice as
0.1 common in men with ED than in their potent
counterparts. Conversely, the presence of depression
0 correlated with a high prevalence of ED (25%),
None Mild Overt similar to the prevalence in men with hypertension
(CES-DDepression and hypogonadism associated in ED
AA Makhlouf et al
160
with the present findings. These large epidemiolo- question of whether depression contributes to the
gical surveys have been borne out in studies of men development of ED, or whether depression itself is
attending ED specialty clinics. Shabsigh et al.8 the result of organic ED. Similarly, it does not
reported that 55% of men presenting to an ED clinic establish a cause–effect relationship between hypo-
had significant depression symptoms as measured gonadism and depression. In fact, Schmidt et al.25
by the Beck Depression Inventory. Finally, treatment have found that experimental androgen deprivation
of ED with phosphodiesterase 5 (PDE5) inhibitors leads to depression in only a minority of men, while
has been shown to improve depressive symptoms in Seidman et al.26 found no benefit to testosterone
two randomized controlled trials.22,23 injections in treating depression in a small trial of
It should be noted that the prevalence of depres- men with concomitant major depression and low
sive symptoms in our cohort was significantly testosterone. Both studies therefore cast some doubt
higher than that found in epidemiological sur- on the hypogonadism-depression linkage. Second,
veys.5,6 In the Massachusetts Male Aging Study the present study is limited by the accuracy of the
(MMAS) sample, the overall prevalence of depres- CES-D in diagnosing clinically relevant depression.
sive symptoms defined as CES-D416 was 12%, The CES-D was designed as a population screening
much lower than in our study.5 This can be tool and not a diagnostic instrument in a clinical
explained by two factors. First, in the MMAS setting, and the optimal cutoff of the CES-D varies
sample, the presence of depression increased the according to the population at hand. Unfortunately,
odds of ED twofold. Therefore, the prevalence of the criterion validity of the CES-D in a population
depressive symptoms among the ED subgroup of the similar to ours (clinic-based, middle-aged, North
MMAS is necessarily higher than 12%. Second, not American males with ED) has not been established.
all men with ED in the MMAS sought treatment for Studies of other populations have found the optimal
ED, and one would expect patients presenting to a cut point to be higher than the traditional value of
clinic to be more distressed about ED and therefore 16, with most being between 18 and 22.13,27–31 In the
score was higher on the CES-D. This is supported by present work, we analyzed the data using both the
the fact that another study of ED in an andrology traditional cutoff of 16, as well as the more stringent
clinic setting revealed similarly high prevalence of cutoff of 22 recommended by Haringsma et al.,13 and
depressive symptoms.8 Still, we cannot discount the found an association of hypogonadism with the
possibility that our cohort represents a slightly more overt depression scores. This finding agrees in
skewed population of severe or refractory cases, part only with that of Delhez et al.,32 who also found
especially that the clinic is a known tertiary referral that hypogonadism was associated with depressive
center. Thus, one should be careful in generalizing scores, but reported that this association was
our findings to a non-ED clinic population, such as strongest in men with mild depression symptoms,
one presenting for screening at a health fair or for an as opposed to pathological cases. Because the two
unrelated problem at a primary care clinic. studies used different questionnaires, a direct
Since both depression and hypogonadism are comparison is not possible in the absence of
associated with ED, and since men with hypogona- clinician-verified diagnosis of depression.
dal testosterone levels are at threefold increased risk In conclusion, depression symptoms and low
of developing depression symptoms,10 we examined testosterone are prevalent in ED patients referred
the possibility that men with depression and low to specialized clinics. Although limited in some
testosterone form a single subgroup in ED patients. respects, the present study shows a significant
We found that hypogonadal men were almost twice association between the two conditions, and sug-
as likely to have high depression scores. Mild gests that men with hypogonadism and depression
elevations on the depression scale, however, were form a distinct subgroup of ED patients.
not good correlates of hypogonadism. The relation-
ship of depression and hypogonadism is even more
striking considering that they vary in inverse ways
with aging (hypogonadism more common in older References
men, while depression is less). This is borne out by 1 Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR.
the fact that correction for age improved the Baltimore Longitudinal Study of Aging. Longitudinal effects
statistical strength of our conclusion. This agrees of aging on serum total and free testosterone levels in
with the results reported by Shores et al., again healthy men. Baltimore Longitudinal Study of Aging. J Clin
stressing the need to evaluate both gonadal status Endocrinol Metab 2001; 86: 724–731.
2 Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ,
and mood in men with ED. In fact, we have McKinlay JB. Impotence and its medical and psychosocial
previously shown that depression scores can be correlates: results of the Massachusetts Male Aging Study.
used as a clinical aid to predict hypogonadism J Urol 1994; 151: 54–61.
using an artificial neural network model.24 The 3 Shabsigh R, Kaufman JM, Steidle C, Padma-Nathan H.
Randomized study of testosterone gel as adjunctive therapy
present study lends further support to this concept. to sildenafil in hypogonadal men with erectile dysfunc-
Some limitations in the current study should be tion who do not respond to sildenafil alone. J Urol 2004; 172:
pointed out however. First, it did not address the 658–663.
International Journal of Impotence ResearchDepression and hypogonadism associated in ED
AA Makhlouf et al
161
4 Rosenthal BD, May NR, Metro MJ, Harkaway RC, Ginsberg PC. synthase-containing nerve fibres and the erectile response in
Adjunctive use of AndroGel (testosterone gel) with sildenafil rat penis. BJU Int 2000; 85: 953–958.
to treat erectile dysfunction in men with acquired androgen 20 Traish AM, Munarriz R, O’Connell L, Choi S, Kim SW, Kim
deficiency syndrome after failure using sildenafil alone. NN et al. Effects of medical or surgical castration on erectile
Urology 2006; 67: 571–574. function in an animal model. J Androl 2003; 24: 381–387.
5 Araujo AB, Durante R, Feldman HA, Goldstein I, McKinlay JB. 21 Rosen RC, Fisher WA, Eardley I, Niederberger C, Nadel A,
The relationship between depressive symptoms and male Sand M. Men’s Attitudes to Life Events and Sexuality
erectile dysfunction: cross-sectional results from the Massachu- (MALES) Study. The multinational Men’s Attitudes to Life
setts Male Aging Study. Psychosom Med 1998; 60: 458–465. Events and Sexuality (MALES) study: I. Prevalence of erectile
6 Seftel AD, Sun P, Swindle R. The prevalence of hypertension, dysfunction and related health concerns in the general
hyperlipidemia, diabetes mellitus and depression in men with population. Curr Med Res Opin 2004; 20: 607–617.
erectile dysfunction. J Urol 2004; 171(6 Part 1): 2341–2345. 22 Seidman SN, Roose SP, Menza MA, Shabsigh R, Rosen RC.
7 Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Pena BM. Treatment of erectile dysfunction in men with depressive
Development and evaluation of an abridged, 5-item version of symptoms: results of a placebo-controlled trial with sildenafil
the International Index of Erectile Function (IIEF-5) as a citrate. Am J Psychiatry 2001; 158: 1623–1630.
diagnostic tool for erectile dysfunction. Int J Impot Res 11; 23 Rosen R, Shabsigh R, Berber M, Assalian P, Menza M,
319: 1999. Rodriguez-Vela L et al. Vardenafil Study Site Investigators.
8 Shabsigh R, Klein LT, Seidman S, Kaplan SA, Lehrhoff BJ, Efficacy and tolerability of vardenafil in men with mild
Ritter JS. Increased incidence of depressive symptoms in men depression and erectile dysfunction: the depression-related
with erectile dysfunction. Urology 1998; 52: 848–852. improvement with vardenafil for erectile response study. Am J
9 Mallis D, Moysidis K, Nakopoulou E, Papaharitou S, Hatzi- Psychiatry 2006; 163: 79–87.
mouratidis K, Hatzichristou D. Psychiatric morbidity is 24 Kshirsagar A, Seftel A, Ross L, Mohamed M, Niederberger C.
frequently undetected in patients with erectile dysfunction. Predicting hypogonadism in men based upon age, presence of
J Urol 2005; 174: 1913–1916. erectile dysfunction, and depression. Int J Impot Res 2006; 18:
10 Shores MM, Sloan KL, Matsumoto AM, Moceri VM, Felker B, 47–51.
Kivlahan DR. Increased incidence of diagnosed depressive 25 Schmidt PJ, Berlin KL, Danaceau MA, Neeren A, Haq NA,
illness in hypogonadal older men. Arch Gen Psychiatry 2004; Roca CA et al. The effects of pharmacologically induced
61: 162–167. hypogonadism on mood in healthy men. Arch Gen Psychiatry
11 Seidman SN, Araujo AB, Roose SP, McKinlay JB. Testosterone 2004; 61: 997–1004.
level, androgen receptor polymorphism, and depressive 26 Seidman SN, Spatz E, Rizzo C, Roose SP. Testosterone
symptoms in middle-aged men. Biol Psychiatry 2001; 50: replacement therapy for hypogonadal men with major depres-
371–376. sive disorder: a randomized, placebo-controlled clinical trial.
12 Radloff L. The CES-D scale: a self-report depression scale for use J Clin Psychiatry 2001; 62: 406–412.
in the general population. Appl Psychol Measure 1; 385: 1977. 27 Hedayati SS, Bosworth HB, Kuchibhatla M, Kimmel PL,
13 Haringsma R, Engels GI, Beekman AT, Spinhoven P. The Szczech LA. The predictive value of self-report scales
criterion validity of the Center for Epidemiological Studies compared with physician diagnosis of depression in hemo-
Depression Scale (CES-D) in a sample of self-referred elders dialysis patients. Kidney Int 2006; 69: 1662–1668.
with depressive symptomatology. Int J Geriatr Psychiatry 28 Lyness JM, Noel TK, Cox C, King DA, Conwell Y, Caine ED.
2004; 19: 558–563. Screening for depression in elderly primary care patients. A
14 R Development Core Team and the R Foundation for Statistical comparison of the Center for Epidemiologic Studies-Depres-
Computing. R: A Language and Environment for Statistical sion Scale and the Geriatric Depression Scale. Arch Intern
Computing. Vienna, Austria. http://www.r-project.org. Med 1997; 157: 449–454.
15 Wald M, Meacham RB, Ross LS, Niederberger CS. Testosterone 29 Murrell SA, Himmelfarb S, Wright K. Prevalence of depression
replacement therapy for older men. J Androl 2006; 27: 126–132. and its correlates in older adults. Am J Epidemiol 1983; 117:
16 Almeida OP, Waterreus A, Spry N, Flicker L, Martins RN. One 173–185.
year follow-up study of the association between chemical 30 Wada K, Tanaka K, Theriault G, Satoh T, Mimura M, Miyaoka
castration, sex hormones, beta-amyloid, memory and depres- H et al. Validity of the Center for Epidemiologic Studies
sion in men. Psychoneuroendocrinology 2004; 29: 1071–1081. Depression Scale as a screening instrument of major depres-
17 Beer TM, Bland LB, Bussiere JR, Neiss MB, Wersinger EM, sive disorder among Japanese workers. Am J Ind Med 2007; 50:
Garzotto M et al. Testosterone loss and estradiol administra- 8–12.
tion modify memory in men. J Urol 2006; 175: 130–135. 31 Beekman AT, Deeg DJ, Van Limbeek J, Braam AW, De Vries
18 Wang C, Swerdloff RS, Iranmanesh A, Dobs A, Snyder PJ, MZ, Van Tilburg W. Criterion validity of the Center for
Cunningham G et al. Testosterone Gel Study Group. Trans- Epidemiologic Studies Depression scale (CES-D): results from
dermal testosterone gel improves sexual function, mood, a community-based sample of older subjects in The Nether-
muscle strength, and body composition parameters in hypo- lands. Psychol Med 1997; 27: 231–235.
gonadal men. J Clin Endocrinol Metab 2000; 85: 2839–2853. 32 Delhez M, Hansenne M, Legros JJ. Andropause and psycho-
19 Baba K, Yajima M, Carrier S, Morgan DM, Nunes L, Lue TF pathology: minor symptoms rather than pathological ones.
et al. Delayed testosterone replacement restores nitric oxide Psychoneuroendocrinology 2003; 28: 863–874.
International Journal of Impotence ResearchYou can also read