Management of chronic testicular pain due to thoracolumbar junction syndrome: A pilot study - Urofrance
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Progrès en urologie (2020) 30, 114—118
Disponible en ligne sur
ScienceDirect
www.sciencedirect.com
ORIGINAL ARTICLE
Management of chronic testicular pain due
to thoracolumbar junction syndrome: A
pilot study
La prise en charge de la douleur testiculaire chronique due a un syndrome de
charniere thoraco-lombaire : étude pilote
F. Aoun a,b,∗, E. Malek c, D. Kazan b, S. Albisinni d,
A. Peltier a, R. Bollens e, T. Roumeguère d
a
Urology department, Institut Jules Bordet, Université Libre de Bruxelles, Brussels, Belgium
b
Urology department, Hôtel Dieu de France, Université Saint-Joseph, Lebanon
c
Osteopathic Medicine department, Levant Hospital, Lebanon
d
Urology department, Cliniques Universitaires de Bruxelles, hôpital Erasme, Université Libre
de Bruxelles, Brussels, Belgium
e
Urology department, Centre Hospitalier de Wallonie picarde, Belgium
Received 17 June 2019; accepted 14 December 2019
Available online 21 January 2020
KEYWORDS Summary
Orchialgia; Introduction. — Thoracolumbar dysfunction (TLD) had been evoked as a possible etiology of
Testicular pain; chronic testicular pain. Our study investigated the efficacy of osteopathic diagnosis and treat-
Vertebral; ment of TLD in men with chronic testicular pain.
Thoraco-lumbar Methods. — Patients suffering from testicular pain were examined for thoracolumbar dysfunc-
syndrome; tion and enrolled in a prospective trial if they have both conditions. Following standardized
Maigne syndrome examination, all patients were prescribed 1 to 3 osteopathic treatment sessions, usually at
weekly interval. Treatment success was evaluated using the Visual Analog scale and durability
was assessed by regular follow-up. Patient satisfaction was also assessed. Comparison of pain
improvement was done using Wilcoxon matched-pairs signed-ranks test. Logistic regression was
used to assess for risk factors of success. A P < 0.001 was used for significance.
Result. — Out of 62 patients enrolled, 41 patients (median age 32 years, IQR 24—37) were suf-
fering from chronic testicular pain and TLD. 37 of the 41 participants completed the treatment
and follow-up according to the plan. Patients underwent a median of 2 osteopathic treatment
sessions (range 1—3). Overall, pain disappeared completely in 25 patients (67.5%) and improve-
ment was noted in 7 patients (18.9%). After initial improvement, two patients experienced
relapse at their last visit (5.4%). Five patients (13.5%) had no improvement of their symptoms
∗ Corresponding author.
E-mail address: fouad.aoun@bordet.be (F. Aoun).
https://doi.org/10.1016/j.purol.2019.12.002
1166-7087/© 2019 Elsevier Masson SAS. All rights reserved.
Management of chronic testicular pain due to thoracolumbar junction 115
after osteopathic treatment. Statistically, improvement was significant with a P < 0.001 and on
logistic regression, site of pain and duration of pain were the sole predictors of failure.
Conclusion. — TLD is a pathology that should be considered in the differential diagnosis in
patients with chronic testicular pain and osteopathic manipulation of the spine appears to
be an effective treatment option.
© 2019 Elsevier Masson SAS. All rights reserved.
MOTS CLÉS Résumé
Orchialgie ; Introduction. — La douleur testiculaire chronique peut être un symptôme d’un dérangement
Douleur testiculaire ; intervertébral minime au niveau de la charnière thoraco-lombaire. Le but de notre étude est
Manipulation d’examiner l’efficacité à moyen terme d’une manipulation ostéopathique particulière de la
ostéopathique ; colonne vertébrale sur la douleur testiculaire.
Vertébrale ; Méthodes. — Les patients souffrant d’une douleur testiculaire chronique ont été examinés à la
Syndrome de Maigne ; recherche des critères d’un syndrome de charnière thoraco-lombaire. Les patients répondants
Dérangement aux critères du diagnostic ont bénéficié d’une manipulation ostéopathique vertébrale par un
intervertébral médecin expérimenté avec une évaluation de la douleur par l’échelle visuelle analogique avant
minime ; la session, juste après la session et à chaque mois par la suite. La satisfaction du patient a été
Charnière également examinée. La comparaison a été faite en utilisant le test de Wilcoxon et les facteurs
thoraco-lombaire prédicteurs ont été étudiés grâce à une étude multivariée.
Résultat. — Sur les 62 patients examinés, 41 patients répondaient aux critères diagnostic et
37 patients ont été inclus. La douleur a disparu complètement chez 67,5 % des patients et une
amélioration a été notée chez 18,9 %. Deux patients ont rechuté par la suite (5,4 %). La douleur
a persisté chez 13,5 % des patients. Les facteurs prédicteurs de rechute et de non-amélioration
étaient une durée prolongée des symptômes et une douleur limitée à la paroi scrotale.
Conclusion. — La douleur testiculaire chronique est souvent due à un dérangement inter-
vertébral minime et répond bien à une manipulation ostéopathique vertébrale bien conduite.
© 2019 Elsevier Masson SAS. Tous droits réservés.
Introduction intervertebral dysfunction at the thoracolumbar junction,
and causes pain in the low back, hip, groin, testicles and
Chronic testicular pain is defined as intermittent or constant lower abdomen [5]. A limited number of case reports in the
scrotal or intra-scrotal pain, lasting for 3 months or longer, literature demonstrated an improvement of testicular pain
usually mild in intensity but bothersome to the patient [1]. after treating the thoracolumbar dysfunction [6—9].
It is not an infrequent cause of consultation in the urology Herein, we investigated the efficacy of osteopathic diag-
clinics and often the patient is not satisfied by the care given nosis and treatment of thoracolumbar dysfunction for men
and the physician is frustrated by the absence of an apparent with chronic testicular pain.
etiology and an efficacious treatment [2].
Patient’s complaint is not limited to the testicle only
as the pain may involve other parts of the scrotal content
including the epididymis, the spermatic cord and/or the
Materials and methods
scrotal skin. Physical exam, urine analysis/culture and
Patients
duplex scrotal ultrasound are mandatory to rule out
reversible causes of pain such as tumor, infection, injury, After obtaining the institutional review board approval from
varicocele, spermatocele or infection. Treatment of this our center, a total of 62 patients presenting to our clinic
problem remains a therapeutic dilemma in the absence of suffering from chronic testicular pain were first included.
an underlying cause. All patients underwent a standard urologic and osteopathic
The mechanism of testicular pain is not fully under- examination by the same investigator (FA). Anamnesis was
stood, but in general involves nociceptors, that are somatic taken focusing on the onset, duration, severity (graded on
nerves in the genital branch of the genitofemoral and the a 0—10 scale on the Visual Analog Scale), and location of
ilioinguinal nerves, as well as autonomic branches from pain including points of radiation. Activities that exacer-
the parasympathetic ganglia of T10—12 for the testis, and bate or improve the pain such as voiding, bowel movements,
T10—L1 for the epididymis and vas deferens [3,4]. Thora- sexual or physical activity, prolonged sitting or supine posi-
columbar junction syndrome occurs as a result of a minor tion were noted. Imaging and previous medical treatment
116 F. Aoun et al.
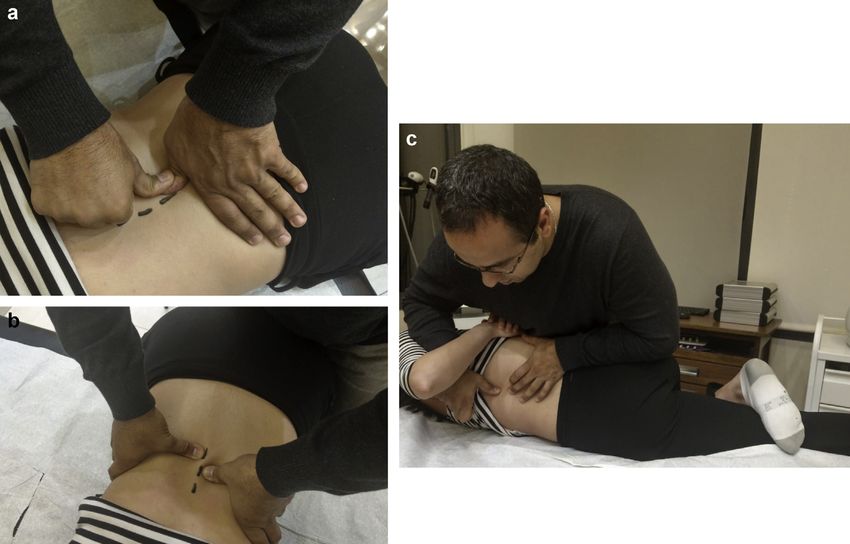
Figure 1. Patient is positioned prone (a—b) and left contra-lateral decubitus (c). Various maneuvers are performed to stress the motion
segment and elicit pain under examination: extension by slowly applied pressure on the spinous processes, torque, by pressure applied to
the sides of the spinous processes and pressure on the facet joint.
and care were also examined. Past surgeries, trauma and After selection, the severity of the pain was graded using
infection involving the back, inguinal, scrotal, pelvic or the Visual Analog Scale. Patients were then presented to
retroperitoneal areas were also noted. Lumbar pain was cha- a physician with an osteopathy training (EM) who evaluated
racterized as well if present. Physical examination focusing again the severity of the pain using the same scale. A clinical
on the genitalia, groin and lumbar spine was systematically history was taken, with particular attention to life style and
performed. The aim of the physical exam was to identify any musculoskeletal and back symptoms/injuries, followed by a
anatomic causes to the pain and to confirm the presence of systematic examination (sacroiliac joint and thoracolumbar
a thoracolumbar dysfunction. The diagnosis of thoracolum- junction mobility, tenderness on back palpation, posture,
bar dysfunction was based upon physical examination that range of motion of the hips, spine).
should reveal severe limitation of the passive and active
range of motion of the lumbar spine, tenderness at the T12- Osteopathic treatment
L1, L5-S1 and L4-L5 intervertebral spaces and at the T12,
L1, L4 and L5 spinous processes. On the ipsilateral side, the Each patient was prescribed 1 to 3 treatment sessions, usu-
maneuver of lateral pressure against the spinous process at ally at weekly interval, each lasting 15 minutes. All manip-
the level of T12-L1, the pinch-roll test and the posterior ulations were performed in the same standardized manner
iliac crest point sign should be positive (Fig. 1). Additional by the same operator. An office care including 15 minutes
urine analysis/culture and duplex scrotal ultrasound of the of manual flexion-distraction and/or high-velocity, low-
scrotum was ordered to all these patients. amplitude adjustments to palpated restrictions in the lower
thoracic and lumbar regions as tolerated by the patient was
performed. No instruments were used during the session. No
Study inclusion specific physical exercises were needed for home care. How-
ever, patients were advised to avoid provocative movements
Patients having chronic testicular pain and a thoracolumbar and demonstrated lumbar spine sparing strategies for daily
dysfunction were included. Patients with acute or sub-acute activities. Patients were assessed after the first session to
testicular pain (less than 3 months) and a thoracolumbar decide if further sessions were needed. The protocol of the
dysfunction were excluded (n = 19) and re-included if the study was to perform 3 sessions and if pain persists the osteo-
pain lasted more than 3 months despite medical therapy pathic manipulation was considered as a failed treatment
(n = 11). Patients with chronic testicular pain and no thora- and no further osteopathic manipulation was advised.
columbar dysfunction were excluded (n = 3). Patients with
any related cause of pain were excluded. These included Evaluation
inguinal hernia (n = 3), pudendal neuralgia (n = 1), varicocele
(n = 1), prior hernia repair (n = 2), prior vasectomy surgery After the end of the session, the severity of pain was
(n = 1), infection (n = 1) and spermatocele (n = 1). assessed by the osteopath using the same scale of pain (EM).Management of chronic testicular pain due to thoracolumbar junction 117
This allows comparison between the patient’s pretreatment testis (18 months and 72 months, respectively). On multi-
and post-treatment perceptions of pain, which is the only variate analysis, only the site of pain (Chi2 : 18.03, P = 0.001)
important measure at this time. Patients were seen one and duration of symptoms (OR 0.72, 95%CI 0.58—0.90,
week after the session by the physician (FA) to assess the P = 0.004) were associated with failure. Age, BMI and sever-
severity of pain and decide if further sessions were needed. ity of pain were not predictors for treatment failure. The
Patients were then followed-up by regular interval (1 month, treatment was well tolerated; patients were satisfied in
and then every three months) and questioned in person or 78.1% of cases and recommend the treatment to other per-
in writing on their pain and satisfaction with the treatment. son suffering from the same condition in 80.1% of cases
Patient satisfaction with the treatment was assessed by the (Tables 1—3).
following two questions: ‘‘if they were satisfied with the
treatment’’ and if they ‘‘recommend the treatment for oth-
ers suffering from the same condition’’. Cure was defined as Discussion
a pain scoring 0 on EVA scale. Improvement was considered
if a decrease > 1 point on EVA scale. This pilot study describes thoracolumbar junction dys-
function in patients with chronic testicular pain and
Statistical analysis the diagnostic approach and treatment they received.
Comparison of pain improvement was done using Wilcoxon
matched-pairs signed-ranks test. Logistic regression was Table 1 Baseline patient characteristics.
used to assess for risk factors of success. The studied varia- Number of patients 41
bles were the site of pain, duration of symptoms, age and
severity of pain. A P < 0.001 was used for significance. Age (years) median (IQR) 32 (24—37)
Site of pain
Head of the epididymis 25
Results Head and tail of the epididymis 2
Scrotal skin 2
A total of 41 patients were included (median age 32 years, Testicle and head of the epididymis 6
IQR 24—37). Pain was limited to the head of the epididymis Testicle only 6
(n = 25), head and tail of the epididymis (n = 2), scrotal skin Duration of symptoms (months) median 4 (3—12)
(n = 2), testicle (n = 6), testicle and head of the epididymis (IQR)
(n = 6). The pain irradiated to the inner part of the thigh Osteopathic treatment sessions median 2 (1—3)
in 8 patients, to the groin in 6 patients, and to both in 4 (IQR)
patients. Lumbar pain was present in 9 patients only. Visual Analog scale before the first session 4 (3—5)
Duration of symptoms ranged from 3 months up to median (IQR)
6 years (median 4 months, mean 10 months and IQR VAS—E median (IQR) 6 (5—7)
3—12 months). All these patients had previously been VAS p median (IQR) 4 (4—5)
treated by nonsteroidal anti-inflammatory drugs, mus- VAS pp median (IQR) 1 (0—2)
cle relaxant, antidepressants, anticonvulsants, narcotics VAS after 2 days median (IQR) 1 (0—2)
and/or antibiotics without improvement. VAS at 1 month median (IQR) 0 (0—1)
The median Visual Analog scale was 4 (IQR 3—5) before VAS at 3 months median (IQR) 0 (0—1)
the first session. Four patients included initially did not
complete the treatment as planned. A total of 37 patients
completed treatment as planned. Patients underwent a Table 2 Association between site of pain and success.
median of 2 osteopathic treatment sessions (range 1—3). Site Failure Success
After the first session, pain disappeared completely
in 14 patients (37.8%). Pain improved significantly in Head and tail of the epididymis 0 2
10 patients (27.1%). A second session was needed for 23 Head of the epididymis and testicle 3 1
patients (62.2%). After the second session, pain disap- Head of the epididymis 2 25
peared completely in 9 patients (24.3%) and improved in 7 Scrotal skin 2 0
patients (18.9%). A third session was needed for 14 patients Testicle 2 4
(37.8%). After the third session, pain disappeared com- 2 : 18.03; P = 0.001.
pletely in 2 patients (5.4%) and improved in 7 patients
(18.9%). Improvement after the first, second and third ses-
sions was statistically significant (P < 0.001).
Median follow-up was 8 months, (mean 10 months, IQR Table 3 Univariate logistic regression exploring risk
5—14 months). At the last follow-up, pain disappeared com- factors for success.
pletely in 25 patients (67.5%) and improvement was noted in
7 patients (18.9%). After initial improvement, two patients OR 95%CI P-value
experienced pain relapse at their last visit (5.4%). Five Age 0.99 0.90—1.09 0.85
patients (13.5%) had no improvement of their symptoms Duration of pain 0.72 0.58—0.90 0.004
after osteopathic treatment: Two patients had a scrotal skin VAS 0.58 0.28—1.19 0.14
pain; three patients had long lasting pain limited to the118 F. Aoun et al.
Thoracolumbar junction dysfunction was present in all but the small number of patients, the absence of a control arm
3 patients with chronic testicular pain unrelated to other and a relatively short follow-up.
etiologies (93.3%). Osteopathic manipulations of the spine
resulted in a significant improvement of testicular pain and
complete resolution rate as high as 67%. Conclusion
Thoracolumbar junction syndrome was first described by
Robert Maigne as a minor intervertebral dysfunction of the Thoracolumbar junction syndrome is a pathology that should
mobile segment of the thoracolumbar junction which con- be considered in the differential diagnosis in patients with
sists of the intervertebral disc, ligaments and the facet chronic testicular pain. Physician should be familiar with the
joints [10]. Minor intervertebral dysfunction causes pain in above mentioned syndrome and should be able to diagnose
the corresponding metamere (Fig. 1). Afferent innervation and refer for management. The osteopathic treatment of
of the scrotum originates via somatic nerves in the genital thoracolumbar dysfunction relieves testicular pain in the
branch of the genitofemoral nerve, ilioinguinal nerves and majority of cases especially if pain is limited to the head
autonomic branches from T10-L1 parasympathetic ganglia. of the epididymis and is of short duration.
The genitofemoral and ilioinguinal nerves provide anterior
scrotal wall and thigh innervation. The posterior scrotal
wall is innervated via the perineal branches of the puden- Disclosure of interest
dal nerve. Signs can be found in the same dermatome,
myotome and sclerotome as the spinal dysfunction. There- The authors declare that they have no competing interest.
fore, patients may complain of pain in the scrotal skin,
epididymis, spermatic cord, and testis. The pain can be felt
also on the medial part of the thigh, the groin or lower back References
[11,12]. Physical examination is regarded as the keystone for
diagnosis of thoracolumbar junction syndrome and should be [1] Calixte N, Brahmbhatt J, Parekattil S. Chronic testicular and
groin pain: pathway to relief. Curr Urol Rep 2017;18:83,
mastered by the urologist.
http://dx.doi.org/10.1007/s11934-017-0722-7.
Our study is a good example showing that clinical exam-
[2] Quallich SA, Arslanian-Engoren C. Chronic testicular
ination is very important when evaluating patients with pain in adult men: an integrative literature review. Am
chronic testicular pain. When examining the thoracolumbar J Mens Health 2013;7:402—13, http://dx.doi.org/10.
junction, one must always look carefully for tender points 1177/1557988313476732.
upon palpation of spinous processes, transverse process and [3] Kumar P, Mehta V, Nargund VH. Clinical management
facet joints. Urologist should look for tenderness at the pos- of chronic testicular pain. Urol Int 2010;84:125—31,
terior iliac crest and perform correctly the pinch-roll test http://dx.doi.org/10.1159/000277587.
described above. Our study demonstrated clearly that clini- [4] Parekattil SJ, Gudeloglu A, Brahmbhatt JV, Priola KB,
cal assessment is reliable, reproducible and can be done by Vieweg J, Allan RW. Trifecta nerve complex: potential
anatomical basis for microsurgical denervation of the sper-
the trained urologist.
matic cord for chronic orchialgia. J Urol 2013;190:265—70,
Thoracolumbar junction syndrome is particularly respon-
http://dx.doi.org/10.1016/j.juro.2013.01.045.
sive to spinal manipulative therapy [10]. When performed [5] Kozera K, Ciszek B. Posterior branches of lum-
properly, no further treatment is required in most cases bar spinal nerves - part I: anatomy and functional
as demonstrated in our study. The aim of manipulation is importance. Ortop Traumatol Rehabil 2016;18:1—10,
to restore normal mobility to a hypomobile vertebral seg- http://dx.doi.org/10.5604/15093492.1198827.
ment. Long term relief after osteopathic treatment was not [6] Doubleday KL, Kulig K, Landel R. Treatment of testicular pain
assessed in our study due to limited follow-up. Urologist using conservative management of the thoracolumbar spine: a
should keep in mind that thoracolumbar junction syndrome case report. Arch Phys Med Rehabil 2003;84:1903—5.
is the result of trauma to the spine at that level, efforts, [7] Fortin JD. Thoracolumbar syndrome in athletes. Pain Phys
2003;6:373—5.
bad postures, and/or repeated micro-trauma. Despite the
[8] Delavierre D, Rigaud J, Sibert L, Labat J-J. Evaluation of
small number of relapses in our series, relapses could be
chronic pelvic and perineal pain. Prog Urol 2010;20:865—71,
seen more frequently if long term follow-up was performed. http://dx.doi.org/10.1016/j.purol.2010.08.066.
That’s why, life style modification, correction and counsel- [9] Rowell RM, Rylander SJ. Low-back pain, leg pain, and
ing of bad posture, and strengthening spine muscles are chronic idiopathic testicular pain treated with chiro-
mandatory. practic care. J Altern Complement Med 2012;18:420—2,
Of note, five patients did not respond to osteopathic http://dx.doi.org/10.1089/acm.2010.0698.
manipulation. Two patients had a scrotal skin pain that is [10] Maigne R. Dorsolumbar origin of certain low lumbalgias. Role
probably mediated by the pudendal nerve and should be of interapophyseal articulations and of the posterior branches
treated accordingly. One patient did have a pudendal nerve of spinal nerves. Rev Rhum Mal Osteoartic 1974;41:781—9.
[11] Delavierre D, Rigaud J, Sibert L, Labat J-J. Symptomatic
infiltration and not > 50% improvement on EVA scale. The
approach to referred chronic pelvic and perineal pain
remaining three patients had a long lasting history of scro-
and posterior ramus syndrome. Prog Urol 2010;20:990—4,
tal pain and more severe pain on the Analog Visual Scale http://dx.doi.org/10.1016/j.purol.2010.08.071.
and could represent intrinsic neurologic changes (defini- [12] Delavierre D, Rigaud J, Sibert L, Labat J-J. Definitions,
tive?) more difficult to treat. An infiltration of the posterior classifications and terminology of chronic pelvic and per-
articular process at the level of Ll was attempted without ineal pain. Prog Urol 2010;20:853—64, http://dx.doi.org/10.
any change in testicular pain. Finally, our study is limited by 1016/j.purol.2010.08.070.You can also read

















































