Improving Effects of Peripheral Nerve Decompression Microsurgery of Lower Limbs in Patients with Diabetic Peripheral Neuropathy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

brain
sciences
Article
Improving Effects of Peripheral Nerve Decompression
Microsurgery of Lower Limbs in Patients with Diabetic
Peripheral Neuropathy
Fukai Ma † , Guangyu Wang † , Yiwei Wu, Bingran Xie and Wenchuan Zhang *
Department of Neurosurgery, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University
School of Medicine, Shanghai 200011, China; fkma@fudan.edu.cn (F.M.)
* Correspondence: zhangwench88@sjtu.edu.cn
† These authors contributed equally to this work.
Abstract: Background: Peripheral nerve decompression microsurgery can relieve nerve entrapment
and improve the symptoms of DPN. However, postoperative tissue adhesion will produce new
pressure on the nerves, affecting the surgical efficacy. In this study, a nerve conduit was used in the
peripheral nerve decompression microsurgery to prevent postoperative adhesions, and the role of the
nerve conduit in surgical nerve decompression was explored. Methods: A total of 69 patients with
DPN were recruited and randomly divided into three groups: the nerve conduit group, conventional
surgery group, and control group. Two weeks before surgery and 6 months after surgery, patients in
each group were clinically tested using the visual analog scale (VAS) score, neurophysiological test,
Toronto clinical scoring system (TCSS) score, and two-point discrimination (2-PD) test. Results: The
patients’ symptoms in the nerve conduit group were relieved to varying degrees, and the relief rate
reached 90.9%; the treatment efficacy was higher than that in the other groups. The postoperative
nerve conduction velocity (NCV) in the two surgical groups was significantly higher than that before
the surgery, and the difference between the nerve conduit group and the conventional surgery
group was statistically significant (p < 0.05). For the 2-PD test, there was a statistically significant
difference between the two surgical groups (p < 0.05). The TCSS score in the two surgical groups
Citation: Ma, F.; Wang, G.; Wu, Y.;
was significantly higher than that in the control group (p < 0.01). There was a significant difference
Xie, B.; Zhang, W. Improving Effects
in the TCSS scores between the nerve conduit group and the conventional surgery group (p < 0.05).
of Peripheral Nerve Decompression
Conclusions: The nerve conduit could further improve the efficacy of peripheral nerve decompression
Microsurgery of Lower Limbs in
Patients with Diabetic Peripheral
microsurgery in the treatment of DPN.
Neuropathy. Brain Sci. 2023, 13, 558.
https://doi.org/10.3390/ Keywords: diabetic peripheral neuropathy; peripheral nerve decompression microsurgery; nerve conduit
brainsci13040558
Academic Editors: Marco Luigetti
and Thomas M. Kinfe
1. Introduction
Received: 26 February 2023 Diabetic peripheral neuropathy (DPN) is one of the most common chronic compli-
Revised: 17 March 2023 cations of diabetes, with an incidence rate of as high as 50–60% [1,2]. It is also the main
Accepted: 24 March 2023 cause of foot ulcers, infections, and amputations [3,4]. DPN has long been considered
Published: 26 March 2023
“progressive and irreversible”. It is mainly manifested as pain, numbness, and paresthesia
in the glove-sock-like distribution area at the end of the extremities, seriously influencing
the patients’ quality of life, and results in a heavy social burden [5–7]. In recent years, it
Copyright: © 2023 by the authors.
has generally been demonstrated to be the result of a combination of factors including
Licensee MDPI, Basel, Switzerland. long-term hyperglycemia caused by metabolic disorders, microcirculation disorders, and
This article is an open access article neuroischemia, and hypoxia [8]. The pathogenesis of DPN is complex and remains unclear.
distributed under the terms and It involves changes in osmotic pressure, glycation end products, neuromicroangiopathy,
conditions of the Creative Commons autoimmune responses, oxidative stress responses, and deficiencies of neurotrophic and
Attribution (CC BY) license (https:// nerve growth factors.
creativecommons.org/licenses/by/ Traditional treatment of DPN mainly includes controlling blood sugar and analgesia,
4.0/). metabolic regulation, and improvement in the microcirculation, in order to eliminate ischemia
Brain Sci. 2023, 13, 558. https://doi.org/10.3390/brainsci13040558 https://www.mdpi.com/journal/brainsci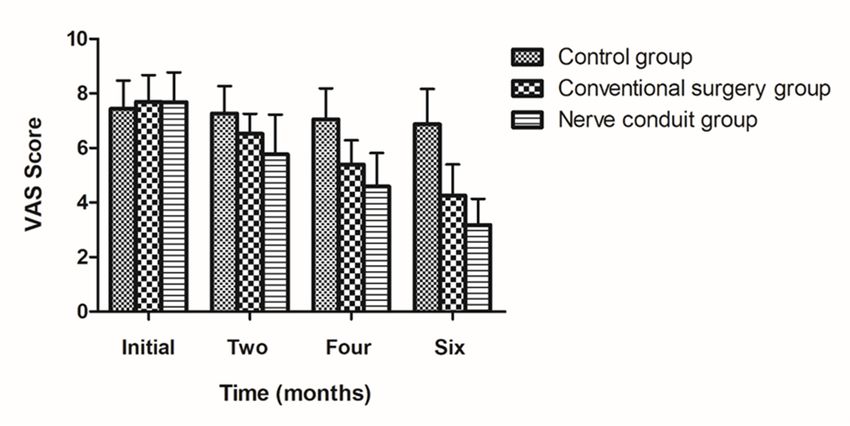
Brain Sci. 2023, 13, 558 2 of 12
and hypoxia as well as enhance nerve conduction function [9]. Other methods have also
been reported such as the consumption of antioxidants, supplementation of nerve growth
factors, and the administration of immunosuppressants [10,11]. However, there is currently
no specific and satisfactory therapeutic method in clinical practice [12]. Professor Dellon
found that the sensitivity of peripheral nerves to compression increased during diabetes,
and demonstrated that the symptoms of DPN were caused by nerve compression, and after
taking the lead in the treatment of DPN with peripheral nerve decompression microsurgery,
the surgery was effective, and the course of DPN changed [13]. In recent years, according
to Dellon et al.’s findings [14,15], several hospitals have applied peripheral nerve decom-
pression microsurgery to treat DPN. Satisfactory efficacy of peripheral nerve decompression
microsurgery assists patients with DPN to restore their feelings and relieve pain [16].
However, after surgery, nerves may adhere to the surrounding tissues, hindering the
extension of the axons to the distal end. At the late stage, it may cause new compression on
the nerve, affecting the recovery of nerve function, and the symptoms are not significantly
improved, and new symptoms may even occur [17]. To prevent the adherence of nerves to
the surrounding tissue or the scar tissue formation caused by recompression of nerves, in
the present study, we used a nerve conduit to wrap the nerve after surgery. Six months after
the surgery, the effects of the nerve conduit were evaluated by the Toronto clinical scoring
system (TCSS) score, visual analog scale (VAS) pain score, neuronal electrophysiology, and
two-point discrimination (2-PD) test.
2. Materials and Methods
2.1. General Data
A total of 69 patients who were diagnosed with type 2 diabetes and treated in the
Ninth People’s Hospital Affiliated with Shanghai Jiaotong University School of Medicine
(Shanghai, China) between March 2019 and March 2022 were enrolled. The study popu-
lation included 35 males and 34 females, with the mean age of 63.8 ± 10.7 years old, the
time of diagnosis of type 2 diabetes was 10.4 ± 4.7 years, and the time to onset of DPN
symptoms was 15.9 ± 7.6 months. Patients presented with spontaneous neuralgia below
the knees and on the bottom of the foot with sensory disturbance. Electromyography (EMG)
confirmed peripheral neuropathy in the lower limbs. Neural Tinel’s sign was positive,
and patients had no severe edema of the feet. Peripheral neuropathy in the lower limbs
caused by cervical and lumbar spine lesions, infectious polyneuritis, chronic alcoholism,
drug poisoning, thyroid disease, tumors, cerebrovascular sequelae, and peripheral vascular
disease were excluded in all patients. Patients were randomly divided into three groups:
the nerve conduit group, conventional surgery group, and control group including 23 cases
in each group. Patients in each group had not received regular treatment for more than
3 months before the experiment. After the start of the experiment, all patients received reg-
ular diabetic treatment, hemoglobin A1c (HbA1c) ≤ 7.5%. In the nerve conduit group and
conventional surgery group, the fasting blood glucose was controlled at about 8 mmol/L
for at least 2 weeks before surgery. This study was conducted in accordance with the
Declaration of Helsinki.
2.2. Treatment Method
The nerve conduit was obtained from Beijing TianXinFu Medical Appliance Co., Ltd.
(Beijing, China). The diameter of the nerve conduit was 3 mm, with the length of 1.3 cm.
Control group program: epalrestat, lipoic acid capsules, beraprost sodium tablets, and
mecobal tablets. Conventional surgery group plan: the classic Dellon lower extremity triple
nerve decompression surgery was performed, and three incisions were made in the lower
extremity: the first surgical incision was located 1.5 cm below the fibular head, a 2.5 cm
oblique incision was made, and the main trunk of the common peroneal nerve was exposed.
The fascia and the peroneus longus tendon were incised to fully expose the superficial
and deep branches of the common peroneal nerve, in which a part of the tendon was cut
at the nerve entrapment site to release the common peroneal nerve, and the epineurium
Brain Sci. 2023, 13, 558 3 of 12
was released along the surface of the common peroneal nerve. Then, a longitudinal 2.5 cm
incision was made on the first and second toes of the dorsum of the foot, the deep peroneal
nerve was freed by incising the skin subcutaneously, and the deep peroneal epineurium
was released throughout the distal end. Finally, an arc-shaped incision was made at
the tarsal canal, about 6 cm in length, in which the skin and flexor retinaculum were
incised, the posterior tibial artery, vein, and their branches were separated and protected,
and the tibial nerve and its branches were separated below it. This was freed and fully
decompressed along the direction of the nerve, and the epineurium was released along
the nerve surface. For the nerve conduit group, after the nerve was decompressed, it was
wrapped by the nerve conduit. Neurolysis and decompression surgeries were performed
under a microscope. Data on the lower extremity with the most serious symptoms were
collected. This was a prospective randomized two-blind trial. The following test was
completed by the same researcher who was blinded to the treatment.
2.3. TCSS Score
TCSS scores were calculated for patients 2 weeks before surgery and 6 months after
surgery. The TCSS score is basically composed of three parts: neurological symptoms, neu-
ral reflexes, and sensory function scores; neurological symptoms include lower extremity
numbness, pain, needle-like sensation, fatigue, unsteady walking, in which 0 and 1 point is
considered for the absence and presence of neurological symptoms, respectively, in total
accounting for 6 points; nerve reflexes include ankle and knee reflexes, in which both sides
are scored separately, involving 2 points for disappearance of reflexes, 1 point for weakened
reflexes, and 0 point for normal reflexes, in total accounting for 8 points; sensory function
includes pain, temperature, touch pressure, vibration, and position sense of the big toe,
involving 1 point for abnormality and 0 point for normality, in total accounting for 5 points.
The total score was 19 points.
2.4. VAS Score Measurement
The patients’ level of spontaneous pain was evaluated using the VAS score measure-
ment. The VAS is one of the oldest and most reliable scales for measuring the severity of
pain [18]. Two weeks before surgery and every 2 months after surgery, pain was assessed
by the VAS score, the pain level gradually increased from 0 to 10 points, and the curative
effect was assessed by the decrease in the VAS score after treatment.
2.5. Nerve Conduction Velocity (NCV)
An electromyograph (model DK-2740; Medtronic Co., Ltd., Copenhagen, Denmark)
was used to detect NCV, in a quiet indoor environment, at a room temperature of 25 ◦ C and
skin temperature of 30 ◦ C. Stimulation and recording were performed by the compliant
surface electrodes. The NCVs of the common peroneal nerve and tibial nerve were recorded
for the three groups 2 weeks before surgery and 6 months after surgery [19].
2.6. 2-PD Test
2-PD discrimination is the ability to discern that two nearby objects touching the skin
are truly two distinct points, and not one. A baseline two-point discriminator (Fabrication
Enterprises, New York, NY, USA) was used to perform the 2-PD test on patients 2 weeks
before surgery and 6 months after treatment. During the neurological examination, patients
were asked to close their eyes to avoid bias in the results. Two points of the skin of the
hallux palm were stimulated with the separated feet of a two-point limen tool, applying
pressure on the skin. If the patient could feel two points, the distance between the two feet
could be shortened by adjusting the tool until the patient could feel one point, then, the
distance was recorded. In this study, the great toe two-point discrimination of the hallux
palm was higher than 9 mm [20].
the distance was recorded. In this study, the great toe two-point discrimination of the h
lux palm was higher than 9 mm [20].
2.7. Statistical Analysis
Brain Sci. 2023, 13, 558 4 of 12
SPSS 13.0 software (IBM, Armonk, NY, USA) was used to perform statistical analys
Data were presented as the mean ± standard deviation (x ± s) and analyzed using t
paired
2.7.sample
Statisticalt-test, covariance analysis, and repeated measures analysis of varian
Analysis
(ANOVA). p < 0.05 was
SPSS 13.0 software considered as statistically
(IBM, Armonk, NY, USA) wassignificant.
used to perform statistical analysis.
Data were presented as the mean ± standard deviation (x ± s) and analyzed using the
3. Results
paired sample t-test, covariance analysis, and repeated measures analysis of variance
(ANOVA). p < 0.05 was considered as statistically significant.
3.1. General Data
3. Results
All 69 patients successfully completed the surgery (Figure 1), and in the review p
3.1. General
cess, one patient Data
in the nerve conduit group was excluded from the study due to the lo
All 69 patients successfullyas
to follow-up. It was recorded completed
effectivetheifsurgery (Figureexperienced
the patient 1), and in the review process,
a relief of sympto
one patient in the nerve conduit group was excluded from the study due to the loss to
(Tablefollow-up.
1). The remission rate in
It was recorded as the nerve
effective conduit
if the patientgroup, conventional
experienced a relief of surgery
symptoms group, a
control group
(Table wasremission
1). The 90.9%, 82.6%,
rate in and 26.1%,
the nerve respectively
conduit (Table 2). The
group, conventional surgical
surgery group,efficacy
the nerve conduit group was the highest among the three groups (Table 2). No periphe
and control group was 90.9%, 82.6%, and 26.1%, respectively (Table 2). The surgical
nerveefficacy
injuryinoccurred
the nerve after
conduit group was
surgery, thethe highest among
incisions the threewell,
were healed groupsand(Table
no 2). No or amp
ulcer
peripheral nerve injury occurred after surgery, the incisions were healed well, and no ulcer
tation was found. One patient in the nerve conduit group underwent surgery again a
or amputation was found. One patient in the nerve conduit group underwent surgery
monthsagainafter
at 6 the recurrence
months of symptoms.
after the recurrence It was Itfound
of symptoms. that that
was found the the
nervenerveconduit
conduit was co
pletely
wasdegraded
completelywhen thewhen
degraded patient underwent
the patient surgery
underwent again.
surgery again.
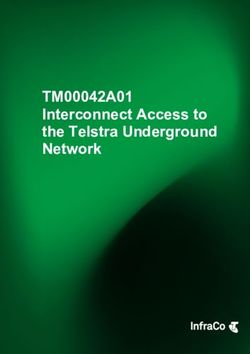
Figure 1. Illustration of the nerve conduit and incisions. (A) Photograph of the nerve conduit. (B) Pho-
tograph of the third surgical incision. (C) Photograph of the first surgical incision. (D) Photograph of
the second surgical incision.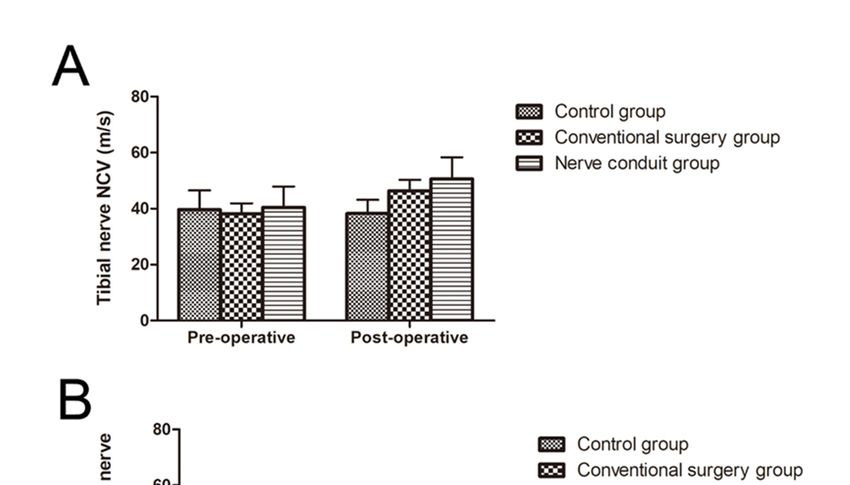
Brain Sci. 2023, 13, 558 5 of 12
Brain Sci. 2023, 13, 558 5 of 12
Figure 1. Illustration of the nerve conduit and incisions. (A) Photograph of the nerve conduit. (B)
Photograph of the thirdand
Table 1. Demographic surgical incision.
clinical features(C) Photograph
of patients of thegroups.
in different first surgical incision. (D) Photo-
graph of the second surgical incision.
Nerve Conduit Conventional
Control Group
Group Surgery Group
Table 1. Demographic and clinical features of patients in different groups.
Mean age (years old) 66.8 ± 9.9 62.4 ± 10.4 62.2 ± 11.5
Female, n Nerve10 Conduit Conventional
12 12
Male, n 13 11 Control
11 Group
Group Surgery Group
Duration of diabetes (years) 9.74 ± 4.3 11.35 ± 4.7 10.2 ± 5.0
Mean ageof(years
Duration old)
pain (months) 66.8
16.3 ±± 8.6
9.9 62.4
18.2 ±
± 10.4
7.7 62.2
13.1 ± ±5.411.5
Female, n 10 12 12
Male, n of the curative effect13
Table 2. Comparison among the three groups11[n (%)]. 11
Duration of diabetes (years) 9.74 ± 4.3 11.35 ± 4.7 10.2 ± 5.0
N Efficient Invalid
Duration of pain (months) 16.3 ± 8.6 18.2 ± 7.7 13.1 ± 5.4
Nerve conduit group 22 20 (90.9) 2 (9.1)
Conventional surgery group 23 19 (82.6) 4 (17.4)
Table 2. Comparison of the curative effect among the three groups [n (%)].
Control group 23 6 (26.1) 17 (73.9)
N Efficient Invalid
3.2.Nerve
TCSS Score
conduit group 22 20 (90.9) 2 (9.1)
TCSS scores
Conventional were calculated
surgery group for the
23 statuses of 2 19
weeks before surgery and46(17.4)
(82.6) months
after surgery. The average preoperative TCSS score in the nerve conduit group was
Control group 23 6 (26.1) 17 (73.9)
16.14 ± 1.81 points, 8.32 ± 1.64 points after treatment, and the difference was statistically
significant (p < 0.05). The average preoperative TCSS score in the conventional surgery
3.2.group
TCSSwasScore
15.83 ± 2.01 points, 9.57 ± 2.25 points after surgery, and the difference was
TCSS scores
statistically were calculated
significant (p < 0.05).forThe
theaverage
statusesTCSS
of 2 weeks before
score in surgery
the control and 6was
group months
16.09
after ± 1.9 points
surgery. before treatment,
The average preoperative ± 2.31score
15.48 TCSS pointsinafter
thetreatment, and the
nerve conduit difference
group was 16.14
waspoints,
± 1.81 not statistically significant
8.32 ± 1.64 (p > 0.05).
points after The above-mentioned
treatment, and the differenceresults
was suggest that the
statistically signif-
curative effect in the two surgical groups was better than that in the control group. There
icant (p < 0.05). The average preoperative TCSS score in the conventional surgery group
was a significant difference between the two surgical groups before and after treatment
was 15.83 ± 2.01 points, 9.57 ± 2.25 points after surgery, and the difference was statistically
(p < 0.05), and it was revealed that the surgical efficacy in the two surgical groups was
significant (p 0.05). TheTCSS
post-operative above-mentioned
scores in differentresults
groups. suggest that the curative effect in
the two surgical groups was better than that in the control group. There was a significant
Nerve Conduit Conventional
difference between the two surgical Surgery
groupsGroupbefore andControl
afterGroup P (1,
treatment (p < 2)
0.05), and it
Group
was revealed that the surgical
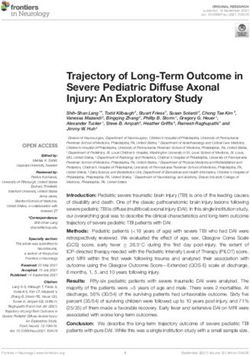
Pre-operative efficacy 15.83
16.14 ± 1.81 in the
± two
2.01 surgical groups
16.09 ± 1.9 was greater than that in
P1 < 0.05
the control group
Post-operative (Table 3) (Figure
8.32 ± 1.64 2). 9.57 ± 2.25 15.48 ± 2.31 P2 < 0.01
P1: Nerve conduit group vs. conventional surgery group; P2: Conventional surgery group vs. control group.
Figure 2. The figure displays the records of the TCSS scores in all groups (mean ± SD).
Figure 2. The figure displays the records of the TCSS scores in all groups (mean ± SD).
Brain Sci. 2023, 13, 558 6 of 12
Brain Sci. 2023, 13, 558 6 of 12
Table 3. Pre- and post-operative TCSS scores in different groups.
Nerve Conduit Conventional Sur-
3.3. VAS Score Control Group P (1, 2)
Group gery Group
According to the degree of improvement in the patients’ symptoms, the VAS score
Pre-operative
was 16.14
used to evaluate the ± 1.81
pain level before15.83 ± 2.01
and after treatment. 16.09
There±was
1.9 no significant
P1 < 0.05
Post-operative
difference in the preoperative VAS score among the three groups. The VAS score in 0.05). Thereperiod.
was a The
VAS statistically
score in the significant difference
conventional in thegroup
surgery VAS score
was between
betweenthe thatnerve conduit
in the nervegroup
conduitandgroup
andthetheconventional surgery
control group. Thegroup
VAS(pscore
< 0.05).
in The
the above-mentioned
two surgery groups results suggest
was that nervelower
significantly
decompression surgery could reduce symptoms in patients, especially with
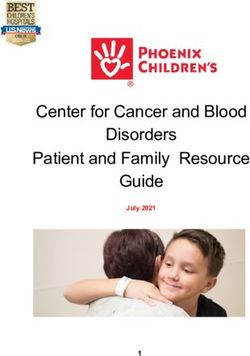
than that in the control group at 6 months after surgery (p < 0.01). At 6 months after sur- the application
of a nerve conduit (Table 4) (Figure 3).
gery, the VAS score in the nerve conduit group decreased from 7.68 ± 1.09 to 3.18 ± 0.96
points
Tablebefore and after
4. Comparison surgery,
of VAS scores atand the difference
different was statistically
time points among significant (p < 0.05).
the three groups.
The VAS score in the conventional surgery group decreased from 7.7 ± 0.97 to 4.26 ± 1.14
Postoperative
points before and after surgery. In comparison, there was no significant difference
Baseline P (1, 2) in the
2 Months 4 Months 6 Months
control group before and at 6 months after surgery for the VAS score (p > 0.05). There was
Nerve conduit
a statistically
group significant difference in the VAS score between the nerve conduit group and
7.68 ± 1.09 5.77 ± 1.45 4.59 ± 1.22 3.18 ± 0.96 P1 < 0.05
the conventional
Conventional surgery group (p < 0.05). The above-mentioned results suggest that nerve
7.7 ± 0.97 6.52 ± 0.73 5.39 ± 0.89 4.26 ± 1.14 P2 < 0.01
decompression
surgery group surgery could reduce symptoms in patients, especially with the applica-
tion Control
of a nerve
group conduit
7.43 ±(Table
1.04 4) (Figure
7.26 ± 1.013). 7.04 ± 1.15 6.87 ± 1.29
P1: Nerve conduit group vs. conventional surgery group; P2: Conventional surgery group vs. control group.
Figure 3. The figure illustrate the results of the VAS levels at different time points for each group
Figure 3. The figure illustrate the results of the VAS levels at different time points for each group
(mean ± SD).
(mean ± SD).
3.4. Electrophysiological Evaluation
The NCVs of 68 patients were recorded. As presented in Table 5, different degrees
of improved NCV could be observed in the majority of patients with DPN in the nerve
conduit group and conventional surgery group. The NCV in the nerve conduit group was
40.4 ± 7.5 m/s before surgery and 50.6 ± 7.8 m/s after surgery for the tibial nerve, and2 Months 4 Months 6 Months
Nerve conduit
7.68 ± 1.09 5.77 ± 1.45 4.59 ± 1.22 3.18 ± 0.96 P1 < 0.05
group
Conventional sur-
7.7 ± 0.97 6.52 ± 0.73 5.39 ± 0.89 4.26 ± 1.14 P2 < 0.01
Brain Sci. 2023, 13, 558 gery group 7 of 12
Control group 7.43 ± 1.04 7.26 ± 1.01 7.04 ± 1.15 6.87 ± 1.29
P1: Nerve conduit group vs. conventional surgery group; P2: Conventional surgery group vs. con-
trol38.9 ± 7.5 m/s before surgery and 52 ± 7.3 m/s after surgery for the common peroneal
group.
nerve, which was the highest velocity among all groups, indicating that the NCV of
3.4.patients after surgeryEvaluation
Electrophysiological was significantly higher than that before surgery (p < 0.05). At
6 months after nerve decompression surgery, the NCV in the conventional surgery group
The NCVs of 68 patients were recorded. As presented in Table 5, different degrees of
increased from 38.1 to 46.3 m/s for the tibial nerve, and 37.2 to 48 m/s for the common
improved
peronealNCV
nerve,could
whichbe observed
was in the
higher than thatmajority of patients
in the control with
group and DPN
lower in that
than the nerve
in the con-
duit group
nerve and group,
conduit conventional
and the surgery
differencegroup. The NCVsignificant
was statistically in the nerve conduit
(p < 0.05) group
(Figure 4). was
40.4 ± 7.5 m/s before surgery and 50.6 ± 7.8 m/s after surgery for the tibial nerve, and 38.9
Table
± 7.5 m/s Comparison
5. before of NCV
surgery andbefore
52 and
± 7.3after
m/s surgery
after among
surgerythe for
threethe
groups.
common peroneal nerve,
which was the highest velocity among all groups, indicating that the NCV of patients after
Nerve Conduit Group Conventional Surgery Group Control Group P
surgery was significantly higher than that before surgery (p < 0.05). At 6 months after nerve
Pre-Operative Post-Operative Pre-Operative Post-Operative Pre-Operative Post-Operative
decompression surgery, the NCV in the conventional surgery group increased from 38.1
Posterior P1 < 0.05,
40.4 ± 7.47 to 46.3
50.56 ± 7.78
m/s 38.1 ± 3.81
for the tibial nerve, and 46.35 ± 3.93
37.2 ± 6.88
39.64for
to 48 m/s the common 38.24 ±peroneal
4.93
tibial nerve P2nerve,
< 0.01 which
Common was higher than that in the control group and lower than that in the nerve conduit group,
P1 < 0.05,
peroneal 38.91 ± 7.48 and the ± 7.28
51.96difference 37.18 ±
was statistically
4.87 ± 6.33
significant
48.03 (p38.7 ± 6.15 (Figure
< 0.05) 4).± 5.17
38.01
P2 < 0.01
nerve
P1: Nerve conduit group vs. conventional surgery group; P2: Conventional surgery group vs. control group.
Figure 4. Pre-operative and post-operative NCVs of patients in all groups (mean ± SD). (A) Nerve
conduction velocity of the tibial nerve. (B) Nerve conduction velocity of the common peroneal nerve.
3.5. 2-PD Test
In the two surgical groups, the 2-PD values significantly decreased half a year after
surgery compared with those before surgery (p < 0.05). In the control group, however, no
significant change in 2-PD values was noted after half a year (p > 0.05). Compared with the
control group, the difference in 2-PD values before and after surgery in the two surgicaltibial 40.4 ± 7.47 50.56 ± 7.78 38.1 ± 3.81 46.35 ± 3.93 39.64 ± 6.88 38.24 ± 4.93
P2 < 0.01
nerve
Common
P1 < 0.05,
peroneal 38.91 ± 7.48 51.96 ± 7.28 37.18 ± 4.87 48.03 ± 6.33 38.7 ± 6.15 38.01 ± 5.17
P2 < 0.01
nerve
Brain Sci. 2023, 13, 558 8 of 12
P1: Nerve conduit group vs. conventional surgery group; P2: Conventional surgery group vs. con-
trol group.
groups was statistically significant (p < 0.05). Compared with the conventional surgery
3.5.group,
2-PD the
Testdifference in 2-PD values before and after treatment in the nerve conduit group
showed
In theatwo
better improvement,
surgical groups,and
the the
2-PDdifference was statistically
values significantly significant
decreased (p a
half < year
0.05) after
(Table 6 and Figure 5).
surgery compared with those before surgery (p < 0.05). In the control group, however, no
significant change
Table 6. Results in 2-PD
of the 2-PDtestvalues was groups.
in the three noted after half a year (p > 0.05). Compared with
the control group, the difference in 2-PD values before and after surgery in the two surgi-
Nerve Conduit
cal groups was statistically significantConventional
(p < 0.05). Compared
Controlwith
Groupthe conventional
P (1, 2) surgery
Group Surgery Group
group, the difference in 2-PD values before and after treatment in the nerve conduit group
Pre-operative 14.05 ± 1.7 ± 1.5 ± 1.43
showed a better improvement, and the13.61 difference was13.7
statistically P1 < 0.05
significant (p < 0.05)
Post-operative 7.05 ± 1.25 8.22 ± 1.78 13.26 ± 2.34 P2 < 0.01
(Table 6 and Figure 5).
P1: Nerve conduit group vs. conventional surgery group; P2: Conventional surgery group vs. control group.
Figure
Figure 5. Diagramofof2-PD
5. Diagram 2-PDtests
tests showing
showing the
thechanges
changesinin
thethe
three groups
three (mean
groups ± SD).
(mean ± SD).
4. Discussion
Table 6. Results of the 2-PD test in the three groups.
It is noteworthy that DPN is a frequent complication of diabetes and a major cause of
Nerve
morbidity and increased ConduitandConventional
mortality, has been shown Sur-
to be associated with significant
reductions in the overallGroup
quality of life, increased
Control Group P (1, 2)
levels of anxiety and depression, sleep
gery Group
impairment, and greater gait variability [21–23]. In the absence of effective treatment,
Pre-operative 14.05 ± 1.7 13.61 ± 1.5 13.7 ± 1.43 P1 < 0.05
patients with diabetes may develop to progressive and irreversible loss of foot sensation,
Post-operative 7.05 ± 1.25 8.22 ± 1.78 13.26 ± 2.34
which may further lead to loss of balance in walking, easy falling and injuries, and even
P2 < 0.01
P1:fractures.
Nerve conduit group vs. conventional surgery group; P2: Conventional surgery group
At the same time, DPN patients are prone to various painless injuries including vs. con-
trolscalds,
group.foot ulcers, infections, gangrene, and even amputation, seriously influencing the
patients’ quality of life [24–26].
Under normal circumstances, blood sugar enters the nerves to provide energy and
is converted into fructose. A high blood sugar level causes fructose accumulation in the
peripheral nerves of diabetic patients. The molecular formula of fructose determines its
tendency to bind water. Therefore, water is sucked into the nerve, causing the nerve to
swell, expanding its volume, stimulating the axons to swell, and is easy to compress [24,27].
An excessive amount of fructose impedes axoplasmic transport, thereby hindering the
transport of lipoproteins that are essential for nerve maintenance and repair, leading
to demyelinate lesions, which are also chronic pathological consequences of elevated
intraneural pressure [28,29]. The formation of terminal glycosylation products in the
peripheral nerves and non-enzymatic glucose, combined with the intraneural collagen,
may reduce nerve elasticity, increase tension, and decrease the sliding properties [30].
Thus, anatomical and physiological properties of the nerve make itself more susceptible
to compression. There are multiple anatomical stenoses on the pathways of peripheral
nerves supplying the fingers and toes from the spinal cord such as the common peroneal
nerve through the peroneal canal and the tibial nerve through the tarsal canal [31]. ForBrain Sci. 2023, 13, 558 9 of 12
diabetic patients, when the swollen nerve is compressed through the anatomical stenosis of
the limb, long-term chronic entrapment leads to epineurial microvascular ischemia and
aggravated demyelination of peripheral nerves, forming a vicious circle and corresponding
clinical symptoms [32].
In the present study, peripheral nerve decompression microsurgery was applied to
relieve nerve compression at the site of anatomical stenosis [33]. Before surgery, there was
no significant difference in gender, age, time of diagnosis, and fasting blood glucose level
among the three groups (Table 1) (p > 0.05). In addition, patients in the nerve conduit
group exhibited good postoperative results after the repair of peripheral nerves observed
using a minimally invasive microscope, and their feelings were satisfactory. The TCSS
score is a method for the diagnosis and prognosis of DPN through patient complaints
and physical examination, and its high efficiency was previously confirmed [34]. The
TCSS score can evaluate the severity of DPN and can also be used as an index for the
evaluation of postoperative treatment efficacy. The results of the present study showed that
the TCSS score was higher in the nerve conduit group than that in the other two groups,
and the difference was statistically significant. Electrodiagnostic testing was not only used
to identify patients eligible for surgery, but was also utilized as an objective marker to
follow the progress of large nerve fiber function [19,35]. The present study revealed that
NCVs were consistent with the TCSS scores. In this study, a higher rate of surgical efficacy
was found in the nerve conduit group compared with that in the other two groups (Table 2).
Peripheral nerve decompression microsurgery can relieve nerve entrapment, restore
axonal transport and blood supply in the nerve, relieve numbness and pain, and promote
tissue repair, while it cannot eliminate peripheral neuropathy caused by abnormal glucose
metabolism. Therefore, insulin should still be used to control blood sugar stability and to
improve metabolic disorders in diabetic patients postoperatively.
In the present study, the diabetic peripheral nerve decompression microsurgery was
utilized as a minimally invasive fibrous neurosurgery with short operation time and less
pain for the patient [36]. Diabetic patients with typical symptoms of peripheral neuropathy
such as pain, numbness, paresthesia, and the peripheral neuropathy caused by other
factors were excluded. When the diagnosis of DPN is confirmed by neurophysiological
examination, nerve decompression can be performed [37]. During surgery, it was found
that the nerves were significantly compressed when passing through the above-mentioned
channels. In addition, it was revealed that the nerves became pale yellow in the surgery,
and their texture was softer than that of the normal nerves. It was considered that the
nerves were compressed for a long time, and degenerated under the state of hyperglycemia.
After incision of the epineurium, there was pale yellow fluid. The intraneural effusion
was presumed due to compressed ischemia–hypoxic neurodegeneration and nerve edema,
leading to local exudation, which in turn increased the intraneural pressure.
The ligament or fibrous tissue was cut to release the compressed part on the nerve
pathway, the compression on the nerve was removed, the blood supply of the nerve was
restored, and the nerve was allowed to slide with the movement of the adjacent joints, so
the symptoms of numbness and pain were relieved [38]. With the prolongation of the time
course of lesion development, necrosis of the innervated muscles may gradually occur,
which may finally be fibrous tissues, and the nerve damage is irreversible [39]. Therefore,
we recommend patients undergo surgery when they experience tingling and numbness in
the feet. If a patient waits until there is muscle degeneration and necrosis, it is difficult to
recover with surgery. In the present study, the follow-up results showed that peripheral
nerve decompression in patients with DPN could alter the natural history of DPN, resulting
in sensory recovery as well as a relief in symptoms such as burning, pain, and numbness.
In this study, we used a nerve conduit to protect the nerves in the surgical area during
surgery, which could prevent the recurrence of nerve compression due to tissue adhesion
after surgery. The nerve conduit manly consists of collagen extracted from bovine Achilles
tendon tissue, and it is one of the most appropriate peripheral nerve repair materials.
A collagen material is mainly recognized as a natural polymer material with excellentBrain Sci. 2023, 13, 558 10 of 12
biocompatibility and biosafety [40–42]. When collagen scaffolds are used for the repair of
peripheral nerve defects, they can maintain a scaffolding effect for a long-time, which is
conducive to the growth and proliferation of nerve cells and gradually form new tissues
to achieve the purpose of tissue repair and regeneration [43,44]. At the same time, the
implanted material is an exogenous substance to the body, and if the implantation time
is very long, it can easily cause a foreign body reaction in the tissue. Therefore, the
degradation time is one of the major factors determining whether the product can meet
the requirements of scaffolds for tissue engineering [45]. In one patient who underwent
surgery 6 months later, we found that the nerve sheath was completely absorbed and
degraded. The collagen scaffold used in this study has degradable properties, making it
appropriate for tissue regeneration. In addition, it has a special pore structure that meets
the requirements for cell growth and nutrient transport, thereby facilitating organizational
reconstruction. However, there were some limitations in the study. In future works, we will
enroll a greater number of patients and evaluate the long-term prognosis of the patients.
Furthermore, serial sensory conduction will be tested in future works, which may provide
more objectivity and credibility to the conclusions.
5. Conclusions
In summary, the results of this study confirmed that peripheral nerve decompression
microsurgery in the lower extremity was effective for patients with DPN. Based on the
current data, intraoperative application of the nerve conduit can further improve the
efficacy of peripheral nerve decompression microsurgery in the treatment of DPN. This
method may be a new treatment option for patients with DPN who cannot achieve adequate
symptom relief via medications.
Author Contributions: Conceptualization, F.M. and W.Z.; Methodology, Y.W.; Software, Y.W.; Valida-
tion, G.W.; Formal analysis, B.X.; Investigation, F.M. and B.X.; Writing—original draft, F.M. and G.W.;
Writing—review & editing, G.W.; Visualization, G.W.; Supervision, W.Z.; funding acquisition, W.Z.
All authors have read and agreed to the published version of the manuscript.
Funding: This research was funded by the Shanghai Huangpu District Industrial Support Fund
(XK2020010).
Institutional Review Board Statement: The study was conducted in accordance with the Declaration
of Helsinki, and approved by the Review Board of Shanghai Ninth People’s Hospital, Shanghai
Jiaotong University School of Medicine Ethics Committee (SH9H-T252-2).
Informed Consent Statement: Informed consent was obtained from all subjects involved in the
study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement: The data that support the findings of this study are available upon
request to the corresponding author.
Acknowledgments: Financial support for this project was provided by the Shanghai Huangpu
District Industrial Support Fund (XK2020010).
Conflicts of Interest: The authors declare no competing interests.
References
1. Sangiorgio, L.; Iemmolo, R.; Le Moli, R.; Grasso, G.; Lunetta, M. Diabetic neuropathy: Prevalence, concordance between clinical
and electrophysiological testing and impact of risk factors. Panminerva Med. 1997, 39, 1–5. [PubMed]
2. Chitneni, A.; Rupp, A.; Ghorayeb, J. Early Detection of Diabetic Peripheral Neuropathy by fMRI: An Evidence-Based Review.
Brain Sci. 2022, 12, 557. [CrossRef] [PubMed]
3. Petit, W.A., Jr.; Upender, R.P. Medical evaluation and treatment of diabetic peripheral neuropathy. Clin. Podiatr. Med. Surg. 2003,
20, 671–688. [CrossRef]
4. Boulton, A.J.; Vinik, A.I.; Arezzo, J.C.; Bril, V.; Feldman, E.L.; Freeman, R.; Malik, R.A.; Maser, R.E.; Sosenko, J.M.; Ziegler, D.
Diabetic neuropathies: A statement by the American Diabetes Association. Diabetes Care 2005, 28, 956–962. [CrossRef]
5. Ponirakis, G.; Elhadd, T.; Al Ozairi, E. Prevalence and risk factors for diabetic peripheral neuropathy, neuropathic pain and foot
ulceration in the Arabian Gulf region. J. Diabetes Investig. 2022, 13, 1551–1559. [CrossRef] [PubMed]Brain Sci. 2023, 13, 558 11 of 12
6. Siemionow, M.; Zielinski, M.; Sari, A. Comparison of clinical evaluation and neurosensory testing in the early diagnosis of
superimposed entrapment neuropathy in diabetic patients. Ann. Plast. Surg. 2006, 57, 41–49. [CrossRef]
7. Zhang, W.; Chen, L. A Nomogram for Predicting the Possibility of Peripheral Neuropathy in Patients with Type 2 Diabetes
Mellitus. Brain Sci. 2022, 12, 1328. [CrossRef]
8. Caffee, H.H. Treatment of diabetic neuropathy by decompression of the posterior tibial nerve. Plast. Reconstr. Surg. 2000, 106,
813–815. [CrossRef]
9. Hagedorn, J.M.; Engle, A.M.; George, T.K.; Karri, J.; Abdullah, N.; Ovrom, E.; Bocanegra-Becerra, J.E.; D’Souza, R.S. An overview
of painful diabetic peripheral neuropathy: Diagnosis and treatment advancements. Diabetes Res. Clin. Pract. 2022, 188, 109928.
[CrossRef]
10. Zhang, A.; Wang, Q.; Liu, M.; Tan, M.; Zhang, X.; Wu, R. Efficacy and safety of Mudan granules for painful diabetic peripheral
neuropathy: A protocol for a double-blind randomized controlled trial. Medicine 2022, 101, e28896. [CrossRef]
11. Putz, Z.; Tordai, D.; Hajdú, N.; Vági, O.E.; Kempler, M.; Békeffy, M.; Körei, A.E.; Istenes, I.; Horváth, V.; Stoian, A.P.; et al. Vitamin
D in the Prevention and Treatment of Diabetic Neuropathy. Clin. Ther. 2022, 44, 813–823. [CrossRef] [PubMed]
12. Ren, L.; Guo, R.; Fu, G.; Zhang, J.; Wang, Q. The efficacy and safety of massage adjuvant therapy in the treatment of diabetic
peripheral neuropathy: A protocol for systematic review and meta-analysis of randomized controlled trials. Medicine 2022, 101,
e29032. [CrossRef] [PubMed]
13. Dellon, A.L. The Dellon approach to neurolysis in the neuropathy patient with chronic nerve compression. Handchir. Mikrochir.
Plast. Chir. 2008, 40, 351–360. [CrossRef] [PubMed]
14. Dellon, A.L. Treatment of symptomatic diabetic neuropathy by surgical decompression of multiple peripheral nerves. Plast.
Reconstr. Surg. 1992, 89, 689–697, discussion 698–689. [CrossRef] [PubMed]
15. Aszmann, O.C.; Kress, K.M.; Dellon, A.L. Results of decompression of peripheral nerves in diabetics: A prospective, blinded
study. Plast. Reconstr. Surg. 2000, 106, 816–822. [CrossRef]
16. Aszmann, O.; Tassler, P.L.; Dellon, A.L. Changing the natural history of diabetic neuropathy: Incidence of ulcer/amputation in
the contralateral limb of patients with a unilateral nerve decompression procedure. Ann. Plast. Surg. 2004, 53, 517–522. [CrossRef]
17. Wang, S.L.; Liu, X.L.; Kang, Z.C.; Wang, Y.S. Platelet-rich plasma promotes peripheral nerve regeneration after sciatic nerve injury.
Neural Regen. Res. 2023, 18, 375–381. [CrossRef]
18. Scott, J.; Huskisson, E.C. Graphic representation of pain. Pain 1976, 2, 175–184. [CrossRef]
19. Onde, M.E.; Ozge, A.; Senol, M.G.; Togrol, E.; Ozdag, F.; Saracoglu, M.; Misirli, H. The sensitivity of clinical diagnostic methods
in the diagnosis of diabetic neuropathy. J. Int. Med. Res. 2008, 36, 63–70. [CrossRef]
20. Bril, V.; Perkins, B.A. Validation of the Toronto Clinical Scoring System for diabetic polyneuropathy. Diabetes Care 2002, 25,
2048–2052. [CrossRef]
21. Malik, R.A. Novel mechanisms of pain in painful diabetic neuropathy. Nat. Rev. Endocrinol. 2022, 18, 459–460. [CrossRef]
[PubMed]
22. Trepman, E.; Nihal, A.; Pinzur, M.S. Current topics review: Charcot neuroarthropathy of the foot and ankle. Foot Ankle Int. 2005,
26, 46–63. [CrossRef]
23. Daeschler, S.C.; Pennekamp, A.; Tsilingiris, D.; Bursacovschi, C.; Aman, M.; Eisa, A.; Boecker, A.; Klimitz, F.; Stolle, A.; Kopf,
S.; et al. Effect of Surgical Release of Entrapped Peripheral Nerves in Sensorimotor Diabetic Neuropathy on Pain and Sensory
Dysfunction-Study Protocol of a Prospective, Controlled Clinical Trial. J. Pers. Med. 2023, 13, 348. [CrossRef] [PubMed]
24. Wang, D.; Lee, K.Y.; Lee, D.; Kagan, Z.B.; Bradley, K. Low-Intensity 10 kHz Spinal Cord Stimulation Reduces Behavioral and
Neural Hypersensitivity in a Rat Model of Painful Diabetic Neuropathy. J. Pain Res. 2022, 15, 1503–1513. [CrossRef] [PubMed]
25. Harris, M.; Eastman, R.; Cowie, C. Symptoms of sensory neuropathy in adults with NIDDM in the U.S. population. Diabetes Care
1993, 16, 1446–1452. [CrossRef] [PubMed]
26. Liao, C.; Li, S.; Nie, X.; Tian, Y.; Zhang, W. Triple-nerve decompression surgery for the treatment of painful diabetic peripheral
neuropathy in lower extremities: A study protocol for a randomized controlled trial. Front. Neurol. 2022, 13, 1067346. [CrossRef]
27. Jakobsen, J. Peripheral nerves in early experimental diabetes: Expansion of the endoneurial space as a cause of increased water
content. Diabetologia 1978, 14, 113–119. [CrossRef]
28. Gouveri, E.; Papanas, N. The Emerging Role of Continuous Glucose Monitoring in the Management of Diabetic Peripheral
Neuropathy: A Narrative Review. Diabetes Ther. 2022, 13, 931–952. [CrossRef]
29. Nishimura, T.; Hirata, H.; Tsujii, M.; Iida, R.; Hoki, Y.; Iino, T.; Ogawa, S.; Uchida, A. Pathomechanism of entrapment neuropathy
in diabetic and nondiabetic rats reared in wire cages. Histol. Histopathol. 2008, 23, 157–166.
30. Reyes-Pardo, H.; Sánchez-Herrera, D.P.; Santillán, M. On the effects of diabetes mellitus on the mechanical properties of DRG
sensory neurons and their possible relation with diabetic neuropathy. Phys. Biol. 2022, 19, 046002. [CrossRef]
31. Boulton, A.J.; Malik, R.A.; Arezzo, J.C.; Sosenko, J.M. Diabetic somatic neuropathies. Diabetes Care 2004, 27, 1458–1486. [CrossRef]
[PubMed]
32. Dellon, A.L. Diabetic neuropathy: Review of a surgical approach to restore sensation, relieve pain, and prevent ulceration and
amputation. Foot Ankle Int. 2004, 25, 749–755. [CrossRef] [PubMed]
33. Trignano, E.; Fallico, N.; Chen, H.C.; Faenza, M.; Bolognini, A.; Armenti, A.; Di Pompeo, F.S.; Rubino, C.; Campus, G.V. Evaluation
of peripheral microcirculation improvement of foot after tarsal tunnel release in diabetic patients by transcutaneous oximetry.
Microsurgery 2016, 36, 37–41. [CrossRef] [PubMed]Brain Sci. 2023, 13, 558 12 of 12
34. Sinnreich, M.; Taylor, B.V.; Dyck, P.J. Diabetic neuropathies. Classification, clinical features, and pathophysiological basis.
Neurologist 2005, 11, 63–79. [CrossRef]
35. Koo, Y.S.; Cho, C.S.; Kim, B.J. Pitfalls in using electrophysiological studies to diagnose neuromuscular disorders. J. Clin. Neurol.
2012, 8, 1–14. [CrossRef] [PubMed]
36. Dellon, A.L. Preventing foot ulceration and amputation by decompressing peripheral nerves in patients with diabetic neuropathy.
Ostomy Wound Manag. 2002, 48, 36–45.
37. Wang, Q.; Guo, Z.L.; Yu, Y.B.; Yang, W.Q.; Zhang, L. Two-Point Discrimination Predicts Pain Relief after Lower Limb Nerve
Decompression for Painful Diabetic Peripheral Neuropathy. Plast. Reconstr. Surg. 2018, 141, 397e–403e. [CrossRef]
38. Zhong, W.; Yang, M.; Zhang, W.; Visocchi, M.; Chen, X.; Liao, C. Improved neural microcirculation and regeneration after
peripheral nerve decompression in DPN rats. Neurol. Res. 2017, 39, 285–291. [CrossRef]
39. Mu, Z.P.; Wang, Y.G.; Li, C.Q.; Lv, W.S.; Wang, B.; Jing, Z.H.; Song, X.J.; Lun, Y.; Qiu, M.Y.; Ma, X.L. Association Between Tumor
Necrosis Factor-α and Diabetic Peripheral Neuropathy in Patients with Type 2 Diabetes: A Meta-Analysis. Mol. Neurobiol. 2017,
54, 983–996. [CrossRef]
40. Nair, M.; Johal, R.K.; Hamaia, S.W.; Best, S.M.; Cameron, R.E. Tunable bioactivity and mechanics of collagen-based tissue
engineering constructs: A comparison of EDC-NHS, genipin and TG2 crosslinkers. Biomaterials 2020, 254, 120109. [CrossRef]
41. Depalle, B.; McGilvery, C.M.; Nobakhti, S.; Aldegaither, N.; Shefelbine, S.J.; Porter, A.E. Osteopontin regulates type I collagen
fibril formation in bone tissue. Acta Biomater. 2021, 120, 194–202. [CrossRef] [PubMed]
42. Maher, M.; Castilho, M.; Yue, Z.; Glattauer, V.; Hughes, T.C.; Ramshaw, J.A.M.; Wallace, G.G. Shaping collagen for engineering
hard tissues: Towards a printomics approach. Acta Biomater. 2021, 131, 41–61. [CrossRef]
43. Hwangbo, H.; Kim, W.; Kim, G.H. Lotus-Root-Like Microchanneled Collagen Scaffold. ACS Appl. Mater. Interfaces 2021, 13,
12656–12667. [CrossRef]
44. Xin, L.; Lin, X.; Pan, Y.; Zheng, X.; Shi, L.; Zhang, Y.; Ma, L.; Gao, C.; Zhang, S. A collagen scaffold loaded with human umbilical
cord-derived mesenchymal stem cells facilitates endometrial regeneration and restores fertility. Acta Biomater. 2019, 92, 160–171.
[CrossRef] [PubMed]
45. Ma, F.; Xiao, Z.; Chen, B.; Hou, X.; Han, J.; Zhao, Y.; Dai, J.; Xu, R. Accelerating proliferation of neural stem/progenitor
cells in collagen sponges immobilized with engineered basic fibroblast growth factor for nervous system tissue engineering.
Biomacromolecules 2014, 15, 1062–1068. [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual
author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to
people or property resulting from any ideas, methods, instructions or products referred to in the content.You can also read