Influence of Different Trigger Techniques on Twitch Mouth Pressure During Bilateral Anterior Magnetic Phrenic Nerve Stimulation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Influence of Different Trigger
Techniques on Twitch Mouth Pressure
During Bilateral Anterior Magnetic
Phrenic Nerve Stimulation*
Wolfram Windisch, MD; Hans-Joachim Kabitz; and Stephan Sorichter, MD
Background: The trigger has a key role when assessing the twitch mouth pressure (Tw Pmo), since
a “gentle” inspiratory or expiratory effort is needed for triggering to ensure an open glottis
during twitch, but which also guaranties only very mild changes of transdiaphragmatic pressure
following changes in lung volume.
Study objectives: To test if different trigger mechanisms cause different Tw Pmo values, if the
predefined trigger criteria were accomplished, and if the breathing maneuver during triggering
can influence the Tw Pmo.
Design: Experimental study.
Setting: Respiratory muscle and lung function laboratory of a university hospital.
Participants: Twenty healthy men (mean age, 25.6 ⴞ 1.2 years [ⴞ SD]; mean FEV1, 105.9 ⴞ 11.5% of
predicted).
Measurements: Tw Pmo produced by bilateral anterior magnetic phrenic nerve stimulation was
measured using an inspiratory flow trigger (40 mL/s), an inspiratory pressure trigger, and an
expiratory pressure trigger (3.75 mm Hg). All trigger criteria were controlled.
Results: Unusable pressure-time curves occurred in 40% during expiratory triggering, but not during
inspiratory triggering. For inspiratory pressure (flow) triggering, 10% (30%) of the predefined trigger
criteria were exceeded by 50%, indicating that a “gentle” inspiratory effort was not warranted. The
Tw Pmo was higher during inspiratory compared to expiratory triggering (analysis of variance,
p < 0.05). The Tw Pmo during inspiratory pressure and flow triggering were comparable and
significantly correlated (r ⴝ 0.70, p < 0.0001). The time between start of inspiration and trigger
release, and the pressure-time product during that period ranged widely, but this could not predict
the Tw Pmo (multiple linear regression).
Conclusions: The trigger technique influences the Tw Pmo with higher values during inspiratory
compared to expiratory triggering. Expiratory triggering more often produced unusable pressure-
time curves. Inspiratory flow and pressure triggering is comparably useful in healthy subjects, but this
might be different in patients. The trigger criteria need to be controlled to warrant a gentle breathing
effort. (CHEST 2005; 128:190 –195)
Key words: bilateral anterior magnetic phrenic nerve stimulation; diaphragm; inspiratory muscle strength; maximal
inspiratory mouth pressure; phrenic nerve stimulation; respiratory muscle testing; sniff pressure; trigger; twitch pressure
Abbreviations: fb ⫽ breathing frequency; FIn trig ⫽ inspiratory flow at triggering; FRC ⫽ functional residual capacity; PEx
trig ⫽ expiratory pressure at triggering; Pimax ⫽ maximal inspiratory mouth pressure; PIn trig ⫽ inspiratory pressure at
triggering; PTPshut-trig ⫽ pressure-time product during tshut-trig; RV ⫽ residual volume; Sn Pna ⫽ nasal pressure during a
maximal sniff; tshut-trig ⫽ time span between complete shutter occlusion and trigger impulse; Tw Pdi ⫽ twitch transdia-
phragmatic pressures; Tw Pes ⫽ twitch esophageal pressures; Tw Pmo ⫽ twitch mouth pressure; Tw Pmo ExP ⫽ twitch
mouth pressure during expiratory pressure triggering; Tw Pmo InF ⫽ twitch mouth pressure during inspiratory flow
triggering; Tw Pmo InP ⫽ twitch mouth pressure during inspiratory pressure triggering; Vt ⫽ tidal volume
T heessential
assessment of inspiratory muscle strength is
in the investigation of respiratory distur-
Pna) are the simplest and most widely used specific
diagnostic tests for quantification of global inspiratory
bances.1,2 Volitional and noninvasive tests such as the muscle strength, but it is difficult to ensure that the
measurement of maximal inspiratory mouth pressure
(Pimax) and nasal pressure during a maximal sniff (Sn Reproduction of this article is prohibited without written permission
from the American College of Chest Physicians (www.chestjournal.
org/misc/reprints.shtml).
*From the Department of Pneumology, University Hospital Correspondence to: Wolfram Windisch, MD, Department of
Freiburg, Freiberg, Germany. Pneumology, University Hospital Freiburg, Killianstrasse 5,
Manuscript received September 12, 2004; revision accepted D-79106 Freiburg, Germany; e-mail: windisch@med1.ukl.uni-
December 14, 2004. freiburg.de
190 Clinical Investigations
Downloaded From: http://journal.publications.chestnet.org/ on 03/06/2015subjects are making a truly maximal effort.3,4 In con- Table 1—Demographic Data and Parameters on Lung
trast, the measurement of twitch transdiaphragmatic Function and Volitional Tests of Inspiratory Muscle
Strength in 20 Healthy Subjects*
pressures (Tw Pdi) and twitch esophageal pressures
(Tw Pes) in response to phrenic nerve stimulation Variables Mean SD Minimum Maximum
allows the assessment of inspiratory muscle contractility Age, yr 25.6 1.2 23 28
more accurately and independently from the patience’s Weight, kg 77.0 9.0 62 103
ability to perform a maximal inspiratory effort, even in Height, cm 183.3 6.7 173 193
critically ill patients.3–5 However, these measurements Neck girth, cm 38.1 1.4 36 40
require the placement of esophageal and gastric bal- Body mass index 22.8 2.3 20.2 30.0
FEV1, % predicted 105.9 11.5 87 127
loon catheters, which is often unpleasant for the patient FVC, % predicted 103.8 10.6 87 129
and difficult to perform and, therefore, reserved to FEV1/FVC, % 81.6 7.7 68 96
some few centers that have the adequate expertise.6 – 8 Total lung capacity, % 98.7 9.3 85 115
The measurement of the twitch mouth pressure (Tw predicted
Pmo) in response to phrenic nerve stimulation has Plpeak RV, mm Hg 105.8 11.3 84.0 123.0
Plpeak FRC, mm Hg 92.3 12.0 60.0 117.0
been recognized as a valuable diagnostic tool for the Plmax1.0 RV, mm Hg 81.8 17.3 34.5 103.5
assessment of diaphragmatic strength, since it is non- Plmax1.0 FRC, mm Hg 72.0 14.3 43.5 95.3
volitional but is also noninvasive.3,6,8 Since the transdia- Sn Pna, mm Hg 87.8 11.3 65.3 104.3
phragmatic pressure is reciprocally proportional to the *Plmax1.0 ⫽ plateau Pimax sustained for 1 s; Plpeak ⫽ peak Pimax.
lung volume, it is recommended to apply the magnetic
impulse as close as possible to the functional residual
capacity (FRC).9 –11 However, the transmission of the
Pna, Pimax, and Tw Pmo were also measured (ZAN 100; ZAN
intrathoracic pressure to the mouth during measure- Gerätetechnik GmbH; Oberthulba, Germany). For Pimax, peak
ments at the relaxed FRC may be hindered by glottic and plateau pressures have been measured both at residual
closure.6,7,12 Therefore, inspiratory or expiratory effort volume (RV) and at FRC as has been described previously.17
is necessary to ensure an open glottis during phrenic
nerve stimulation, but this effort needs to be “gentle” to Tw Pmo: Recordings of Pressure and Air Flow
avoid changes in lung volume that could change the
Tw Pmo was measured using a flanged mouthpiece connected
transdiaphragmatic pressure and that also may lead to to cylinder with a shutter at its distal end that functions as a
unintentional twitch potentiation.6,11,13,14 Therefore, magnetic catch piston to completely occlude the external airway
the trigger mechanism for the release of the magnetic for 2.0 s. A steel tube of 4 cm in length and 1 mm in internal
twitch has a key role in the accurate assessment of the diameter was placed proximally of the shutter as has been
Tw Pmo. described previously,16 thereby preventing glottic closure during
the maneuver. The cylinder was connected to a pressure trans-
Both inspiratory and expiratory trigger mecha- ducer and pneumotachograph interfaced with a computer sys-
nisms have been introduced for the assessment of tem. This allowed visualization of the pressure-time curves and
the Tw Pmo.6,7,15,16 However, it is unclear if differ- displaying of the flow signal to the participant.
ences in trigger mechanisms and trigger conditions Pressure and volume calibration of the system was performed
can lead to different Tw Pmo. In addition, it is daily prior to the measurements. All measurements were per-
formed only by one specialized person with the participant in a
unclear if the subjects performed a truly gentle seated position wearing a nose clip. All pressures generated by
inspiratory or expiratory effort, since the predefined the inspiratory muscles are presented with positive numbers.
trigger criteria were not controlled in most studies.
Therefore, the aim of the present study was to test if Bilateral Anterior Magnetic Phrenic Nerve Stimulation
different trigger mechanisms cause differences in
the Tw Pmo, if the predefined trigger criteria have Bilateral anterior magnetic phrenic nerve stimulation5,18 was
performed using two magnetic stimulators (Magstim 2002; Mag-
been accomplished, and if the breathing maneuver stim; Wales, UK) at maximal output (100%). For this purpose,
during triggering can influence the Tw Pmo. two 45-mm figure-eight coils (Magstim) generating a magnetic
field of 3.2 T at maximal drive were used. Both magnetic
stimulators were triggered simultaneously; here, the impulse was
Materials and Methods automatically released by an electric signal derived from the
computer system as soon as the below-defined trigger criteria
The study protocol was approved by the Agency of Ethics of have been achieved.
Albert-Ludwig University, Freiburg, Germany, and was per- The coils were placed around the posterior border of the
formed in accordance with the ethical standards laid down 2000 sternomastoid muscle at the level of the cricoid cartilage as
in the Declaration of Helsinki. Informed written consent was previously described.16 The accurate position of the coils was
obtained from all subjects. Twenty young and healthy men warranted by slightly moving the coils until the greatest Tw Pmo
without lung or thoracic rib cage disease who did not take any amplitude was recorded.6,11,19 For measurements of the experi-
medication were studied after careful instruction (Table 1). Lung mental study design, all Tw Pmo measures were recorded by
function parameters using body plethysmography were measured performing the twitch exactly at this position, which was marked
(Masterlab-Compact Labor; Jaeger; Hochberg, Germany). Sn by a highlighter. For the purpose of holding the position, a steel
www.chestjournal.org CHEST / 128 / 1 / JULY, 2005 191
Downloaded From: http://journal.publications.chestnet.org/ on 03/06/2015bracket for fixing the coils was constructed that ensured that the breathing frequency (fb) and the Vt were calculated as the mean
angle and the position of the coils were unchanged during all of the last three breaths. The inspiratory pressure at triggering
measurements. (PIn trig) , expiratory pressure at triggering (PEx trig), and the
inspiratory flow during triggering (FIn trig) were measured to
Experimental Study Design verify if the trigger criteria were accomplished as demanded by
the target of each experiment.
To avoid twitch potentiation,11,13,14 a rest of 20 min in which the To ensure a gentle inspiratory or expiratory effort, the Tw Pmo
participant breathed quietly without speaking preceded the experi- was only accepted if the difference between the predefined and
ments after locating the correct coil position. The elapsed time measured trigger criteria did not exceed 50%. Accordingly, the
between successive maneuvers exceeded 30 s. The Tw Pmo was Tw Pmo was not accepted if the FIn trig was ⬎ 60 mL/s (trigger
recorded using three different techniques for triggering in a random criteria, 40 mL/s) during inspiratory flow triggering or if the PIn
order (experiments 1, 2, and 3). For each experiment, the Tw Pmo trig was ⬎5.625 mm Hg and if the PEx trig was ⬎5.625 mm Hg
was measured until five acceptable pressure tracings according to (trigger criteria, 3.75 mm Hg) during inspiratory and expiratory
the criteria defined below were recorded. Subsequently, the highest pressure triggering, respectively. In addition, the pressure-time
and lowest Tw Pmo measures were deleted, and the mean of the curves need to present a clear twitch reply of the diaphragm with
remaining three values was counted. The trigger was started close to a clear increase and decrease of the inspiratory pressure following
the FRC in all experiments. For this purpose, the participant was the trigger impulse.
instructed to breathe quietly and to perform a “gentle” inspiratory or
expiratory effort as the valve was closed. Statistical Analysis
Experiment 1: To assess Tw Pmo during inspiratory flow
triggering (Tw Pmo InF), the shutter was closed immediately Statistical analysis was performed using Sigma-Stat (Version
after the beginning of inspiration. The magnetic impulse was 2.03; SPSS; Chicago, IL). Data are presented as mean ⫾ SD after
initiated when the inspiratory flow of the participant reached 40 testing for normal distribution (Kolmogorov Smirnov test). Com-
mL/s. The duration of shutter occlusion lasts approximately 76 parisons between different measurements (different Tw Pmo in
ms. This time has to be taken into account when starting the experiments 1, 2, and 3) were performed using one-way analysis
trigger, since it is principally possible that the trigger release of variance. Correlation analysis was performed using the Pear-
occurs to early when the shutter is not completely closed yet. son product moment correlation. In addition, fb, FIn trig, PIn
Therefore, it was also required for triggering that the inspiratory trig, PTPshut-trig, and tshut-trig during inspiratory triggering
pressure was at least 3.75 mm Hg, which ensured that the shutter (experiments 1 and 2) were compared using the unpaired t test if
was completely closed. data were normally distributed or using the Mann-Whitney rank
Experiment 2: To assess Tw Pmo during inspiratory pressure test if data were not normally distributed. Further, the Tw Pmo
triggering (Tw Pmo InP), the shutter was closed immediately after was calculated for its predictors, which could be derived from
the beginning of inspiration. The magnetic impulse was initiated as measurement variables of the pressure-time curve using the
soon as the inspiratory pressure of the participant had reached 3.75 multiple linear regression analysis. Here, Tw Pmo was used as
mm Hg. In addition, it was also required for triggering that the dependent variable, and FIn trig, PIn trig, and PTPshut-trig or
inspiratory flow was at least 10 mL/s to avoid a pure static pressure tshut-trig were used as independent variables if an inspiratory
development. trigger was used. Accordingly, Tw Pmo was used as dependent
Experiment 3: To assess Tw Pmo during expiratory pressure variable, and PEx trig and PTPshut-trig or tshut-trig were used as
triggering (Tw Pmo ExP), the shutter was closed as soon as 95% of independent variables if an expiratory trigger was used. Statistical
the tidal volume (Vt) was exhaled. The magnetic impulse was significance was assumed at p ⬍ 0.05.
initiated as soon as the expiratory pressure had reached 3.75 mm Hg.
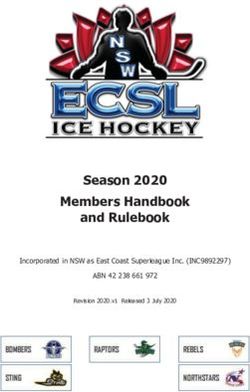
For inspiratory triggering, the Tw Pmo was regarded as the
difference between the trigger impulse and the peak pressure
(Fig 1). The beginning of inspiration was reliably detected if the Results
inspiratory volume has reached 10 mL. For expiratory triggering,
the Tw Pmo was regarded as the difference between the pressure
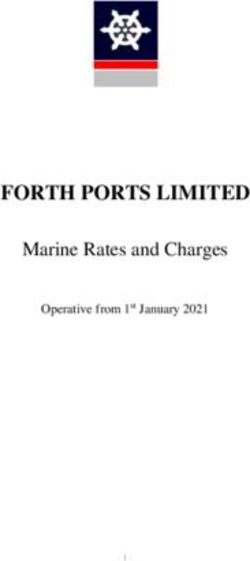
Unusable pressure-time curves without a clear
at the point of reversal of the pressure direction and the peak increase and decrease of the inspiratory pressure
pressure. The time span between complete shutter occlusion and occurred in 40% when using the expiratory trigger
trigger impulse (tshut-trig) was calculated (Fig 1). In addition, (Fig 2), but all trigger criteria could be accepted. For
the area under the pressure-time curve (pressure-time product)
during tshut-trig (PTPshut-trig) was calculated (Fig 1). The
Figure 2. Pressure-time curve of the Tw Pmo during expiratory
pressure triggering that was not accepted according to predefined
Figure 1. Assessment of Tw Pmo, tshut-trig, and PTPshut-trig. criteria.
192 Clinical Investigations
Downloaded From: http://journal.publications.chestnet.org/ on 03/06/2015Table 2—Descriptive Data of Experiments 1 and 2 (n ⴝ 20): Tw Pmo During Inspiratory Flow Trigger (Experiment 1)
and During Inspiratory Pressure Trigger (Experiment 2)
Variables Tw Pmo, mm Hg FIn trig,* mL/s PIn trig,* mm Hg tshut-trig, ms PTPshut-trig, mm Hg/s fb, min
Experiment 1
Mean 14.40 43.6 4.5 208.3 4.65 17.5
SD 3.30 2.1 0.4 67.3 1.73 4.4
Minimum 9.45 40.0 3.8 128.3 2.63 10.8
Maximum 23.03 48.3 5.3 452.0 10.50 26.5
Experiment 2
Mean 13.65 31.3 3.8 194.5 3.60 17.3
SD 2.55 7.7 0.1 83.3 1.65 4.3
Minimum 9.00 16.0 3.8 83.7 1.50 10.0
Maximum 17.78 41.7 4.5 363.3 6.75 27.0
*p ⬍ 0.001 comparing experiments 1 and 2.
inspiratory pressure triggering, 10% of the pressure- no significant predictors out of the predefined indepen-
time curves could not be accepted, since the differ- dent variables in any experiment following the multiple
ence between the predefined and measured trigger linear regression analysis.
criteria was ⬎ 50%. Accordingly, 30% of the pres-
sure-time curves could not be accepted for inspira- Discussion
tory flow triggering, but nearly all pressure-time
curves during inspiratory triggering were acceptable. There is a need of assessing inspiratory muscle
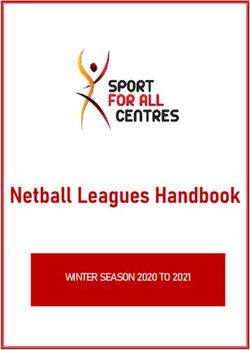
The Tw Pmo was higher when using inspiratory strength in patients with respiratory disturbances.1,2
compared to expiratory trigger techniques (Tables 2, Volitional tests are most widely used, but their inter-
3; Fig 3). The Tw Pmo InF was significantly corre- pretation is limited by the possibility of false pathologic
lated to the Tw Pmo InP (r ⫽ 0.70, p ⬍ 0.0001) and values, since these measurements are dependent from
to the Tw Pmo ExP (r ⫽ 0.67, p ⫽ 0.001). In con- the subject performing a truly maximal effort.3,4 The
trast, the Tw Pmo InP and the Tw Pmo ExP were not assessment of the Tw Pmo is easy to perform and
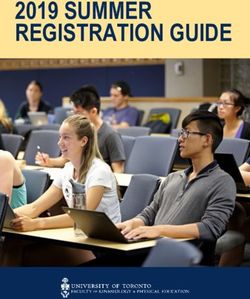
correlated (r ⫽ 0.28, p ⫽ 0.23). During inspiratory independent from the patient’s cooperation and could,
flow (Fig 4) and pressure (Fig 5) triggering, the therefore, become a worthwhile alternative. However,
inspiratory pressure increased slightly at the begin- it is still unclear which trigger should be applied,
ning of inspiration prior to triggering and subse- although triggers of 3.75 mm Hg or 40 mL/s have been
quently steepened markedly after inspiratory muscle suggested to ensure an open glottis, but also to warrant
contraction following magnetic twitch (twitch reply). a gentle inspiratory or expiratory effort.6,16
In contrast, there was a reversal of the pressure In the present study, it has been shown that a gentle
direction during expiratory triggering when switch- breathing effort could not be guarantied, since the flow
ing from gentle volitional expiration to maximal and the pressure, respectively, were ⬎ 50% of the
inspiratory diaphragm contraction (Fig 6). predefined trigger criteria in 30% during inspiratory
Although the trigger criteria of the counted pressure- flow triggering and in 10% during inspiratory pressure
time curves were consistent (Tables 2, 3), the variance triggering even in well-informed healthy subjects. This,
and range of the tshut-trig and the PTPshut-trig were however, is suggested to cause changes in lung volume
wide, indicating that the breathing maneuver occurred that need to be avoided.6,11,13,14 Therefore, a gentle
with slow and rapid increases of the flow/pressure until inspiratory effort starting from very close to the FRC
attaining the trigger threshold. However, this could not for triggering is essential and needs to be controlled
explain the variance of the Tw Pmo, since there were and monitored in all future studies.
Table 3—Descriptive Data of Experiment 3: Tw Pmo During Expiratory Pressure Trigger*
Variables Tw Pmo, mm Hg PEx trig, mm Hg Vt, L Vex/Vt, % tshut-trig, ms PTPshut-trig, mm Hg/s fb, min
Mean 12.00 3.8 0.8 95.5 211.9 3.83 17.7
SD 2.77 0.1 0.1 0.4 77.5 1.53 4.1
Min 7.20 3.8 0.6 95.0 83.7 1.35 8.9
Max 17.25 4.5 1.1 96.0 416.7 8.93 22.9
*Vex/Vt ⫽ percentage of Vt during expiratory triggering; n ⫽ 20.
www.chestjournal.org CHEST / 128 / 1 / JULY, 2005 193
Downloaded From: http://journal.publications.chestnet.org/ on 03/06/2015Figure 5. Representative pressure-time curve of the Tw Pmo
during inspiratory pressure triggering.
pressure-time curves could not be analyzed. In the
present study, expiratory but not inspiratory triggering
often produced unusable pressure-time curves without
a clear pressure maximum. The reason for this remains
Figure 3. Comparison of different Tw Pmo using different unclear, but might be attributed to the reversal of the
inspiratory and expiratory trigger techniques.
flow and pressure direction when switching from gentle
expiration to twitch-induced inspiratory diaphragm
contraction. Based on these results, inspiratory trigger-
Inspiratory trigger mechanisms produced a ing is more reliable than expiratory triggering. Accord-
higher Tw Pmo than the expiratory trigger mech- ingly, in both healthy subjects and patients with severe
anism. This might be in part attributed to tech- COPD, inspiratory but not expiratory triggering pro-
nical differences, since the Tw Pmo following duced a significant correlation between Tw Pmo and
expiratory triggering only reflects the pressure Tw Pes in former studies,7,16 favoring an inspiratory
development caused by twitch-induced diaphragm trigger for future studies. However, the Tw Pmo has
contraction, whereas the Tw Pmo following in- been shown to reliably predict Tw Pes and also Tw Pdi
spiratory triggering implies the pressure develop- both in healthy subjects6,7,20 and in patients with respi-
ment generated by the twitch-induced diaphragm ratory muscle weakness without lung disease,6 but the
contraction in addition to the preceding increasing prediction of Tw Pes from Tw Pmo is hindered by an
inspiratory pressure development during the la- impaired transmission of intrathoracic pressure to the
tency between trigger impulse and twitch reply. upper airway following airway obstruction.16
Therefore, the Tw Pmo generated by expiratory The Tw Pmo generated by flow- and pressure-
compared to inspiratory triggering reflects the driven inspiratory trigger mechanisms were compa-
twitch reply more precisely. rable and significantly correlated to each other.
Former studies have not clearly indicated how many
Figure 6. Representative pressure-time curve of the Tw Pmo
Figure 4. Representative pressure-time curve of the Tw Pmo during expiratory pressure triggering. See Table 3 for expansion
during inspiratory flow triggering. of abbreviation.
194 Clinical Investigations
Downloaded From: http://journal.publications.chestnet.org/ on 03/06/2015However, these results are valid for healthy subjects References
only, and changes in respiratory mechanics might 1 Polkey MI, Green M, Moxham J. Measurement of respiratory
lead to differences in the pressure generation prior muscle strength. Thorax 1995; 50:1131–1135
to attaining the trigger threshold. In addition, the 2 Laghi F, Tobin MJ. Disorders of the respiratory muscles.
breathing maneuver when activating the trigger was Am J Respir Crit Care Med 2003; 168:10 – 48
3 ATS/ERS statement on respiratory muscle testing. Am J
markedly different with slow and rapid increases of Respir Crit Care Med 2002; 166:518 – 624
the flow and pressure until attaining the trigger 4 ATS/ACCP statement on cardiopulmonary exercise testing.
threshold. However, no predictors derived from the Am J Respir Crit Care Med 2003; 167:211–277
pressure-time curve that indicate how fast or slow 5 Polkey MI, Moxham J. Clinical aspects of respiratory muscle
dysfunction in the critically ill. Chest 2001; 119:926 –939
the pressure increased until attaining the trigger 6 Hamnegard CH, Wragg S, Kyroussis D, et al. Mouth pressure
threshold could be identified to explain the variance in response to magnetic stimulation of the phrenic nerves.
of the Tw Pmo. Therefore, it was insubstantial for Thorax 1995; 50:620 – 624
the Tw Pmo as to how slow or how fast the trigger 7 Laghi F, Tobin MJ. Relationship between transdiaphragmatic
and mouth twitch pressures at functional residual capacity.
criteria were accomplished. Eur Respir J 1997; 10:530 –536
Further studies on influences of different trig- 8 Hughes PD, Polkey MI, Kyroussis D, et al. Measurement of
ger techniques on the Tw Pmo including both sniff nasal and diaphragm twitch mouth pressure in patients.
healthy subjects and patients with chronic lung Thorax 1998; 53:96 –100
9 Hubmayr RD, Litchy WJ, Gay PC, et al. Transdiaphragmatic
disease are required before a clear recommenda- twitch pressure: effects of lung volume and chest wall shape.
tion can be given of how the trigger should be Am Rev Respir Dis 1989; 139:647– 652
performed. Thereby, measurements of the Tw Pdi 10 Hamnegard CH, Wragg S, Mills G, et al. The effect of lung
and Tw Pes and measurements of twitch potenti- volume on transdiaphragmatic pressure. Eur Respir J 1995;
8:1532–1536
ation should be included to validate the most 11 Laghi F, Harrison MJ, Tobin MJ. Comparison of magnetic and
favorable trigger technique. electrical phrenic nerve stimulation in assessment of diaphrag-
matic contractility. J Appl Physiol 1996; 80:1731–1742
12 Similowski T, Gauthier AP, Yan S, et al. Assessment of
diaphragm function using mouth pressure twitches in chronic
Conclusion obstructive pulmonary disease patients. Am Rev Respir Dis
1993; 147:850 – 856
The measurement of the Tw Pmo is suggested to be 13 Mador MJ, Magalang UJ, Kufel TJ. Twitch potentiation
a valuable diagnostic tool for the assessment of inspira- following voluntary diaphragmatic contraction. Am J Respir
tory muscle strength. The correct application is inde- Crit Care Med 1994; 149:739 –743
14 Wragg S, Hamnegard C, Road J, et al. Potentiation of
pendent from the cooperation of the patient, but is yet diaphragmatic twitch after voluntary contraction in normal
easy to perform, which could allow a widely used subjects. Thorax 1994; 49:1234 –1237
implementation in the future. The choice of triggering 15 De Bruin PF, Watson RA, Khalil N, et al. Use of mouth
the magnetic twitch significantly influences the Tw pressure twitches induced by cervical magnetic stimulation to
assess voluntary activation of the diaphragm. Eur Respir J
Pmo with higher values during inspiratory compared to 1998; 12:672– 678
expiratory triggering. The inspiratory trigger is sug- 16 Topeli A, Laghi F, Tobin MJ. Can diaphragmatic contractility
gested to be more reliable compared to the expiratory be assessed by twitch airway pressures in patients with
trigger, favoring the inspiratory trigger for future stud- chronic obstructive pulmonary disease? Am J Respir Crit
Care Med 1999; 160:1369 –1374
ies. The trigger criteria that are designed to ensure an 17 Windisch W, Hennings E, Sorichter S, et al. Peak or plateau
open glottis and a gentle inspiratory or expiratory effort maximal inspiratory mouth pressure: which is best? Eur
need to be measured and controlled, since an increase Respir J 2004; 23:708 –713
of flow/pressure during triggering can occur causing 18 Mills GH, Kyroussis D, Hamnegard CH, et al. Bilateral
magnetic stimulation of the phrenic nerves from an antero-
changes in lung volume and transdiaphragmatic pres- lateral approach. Am J Respir Crit Care Med 1996; 154:
sure that need to be avoided. Further studies including 1099 –1105
measurement with balloon catheters are required to 19 Similowski T, Fleury B, Launois S, et al. Cervical magnetic
verify which trigger technique is most applicable and stimulation: a new painless method for bilateral phrenic nerve
useful. stimulation in conscious humans. J Appl Physiol 1989; 67:
1311–1318
ACKNOWLEDGMENT: We thank Roland Merklein (ZAN; 20 Yan S, Gauthier AP, Similowski T, et al. Evaluation of human
Oberthulba, Germany) for writing the software and for technical diaphragm contractility using mouth pressure twitches. Am
assistance. Rev Respir Dis 1992; 145:1064 –1069
www.chestjournal.org CHEST / 128 / 1 / JULY, 2005 195
Downloaded From: http://journal.publications.chestnet.org/ on 03/06/2015You can also read