Innovating Women's Reproductive Health and Pregnancy Therapeutics - November 2018 - Jefferies
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Innovating Women’s Reproductive
Health and Pregnancy Therapeutics
November 2018
NASDAQ:OBSV | SIX:OBSN
DISCLAIMER
Matters discussed in this presentation may constitute forward-looking statements. The forward-looking statements contained in this
presentation reflect our views as of the date of this presentation about future events and are subject to risks, uncertainties,
assumptions, and changes in circumstances that may cause our actual results, performance, or achievements to differ significantly
from those expressed or implied in any forward-looking statement. Although we believe that the expectations reflected in the
forward-looking statements are reasonable, we cannot guarantee future events, results, performance, or achievements. Some of
the key factors that could cause actual results to differ from our expectations include our plans to develop and potentially
commercialize our product candidates; our planned clinical trials and preclinical studies for our product candidates; the timing of
and our ability to obtain and maintain regulatory approvals for our product candidates; the extent of clinical trials potentially required
for our product candidates; the clinical utility and market acceptance of our product candidates; our commercialization, marketing
and manufacturing capabilities and strategy; our intellectual property position; and our ability to identify and in-license additional
product candidates. For further information regarding these risks, uncertainties and other factors that could cause our actual results
to differ from our expectations, you should read our Annual Report on Form 20-F for the year ended December 31, 2017, as filed
with the Securities and Exchange Commission on March 9, 2018 and our other filings it makes with the Securities and Exchange
Commission from time to time. We expressly disclaim any obligation to update or revise the information herein, including the
forward-looking statements, except as required by law. Please also note that this presentation does not constitute an offer to sell or
a solicitation of an offer to buy any securities.
This presentation concerns products that are under clinical investigation and which have not yet been approved for marketing by the
U.S. Food and Drug Administration. It is currently limited by federal law to investigational use, and no representation is made as to
its safety or effectiveness for the purposes for which it is being investigated. The trademarks included herein are the property of the
owners thereof and are used for reference purposes only. Such use should not be construed as an endorsement of such products.
This presentation also contains estimates and other statistical data made by independent parties and by us relating to market size
and growth and other data about our industry. This data involves a number of assumptions and limitations, and you are cautioned
not to give undue weight to such estimates. In addition, projections, assumptions and estimates of our future performance and the
future performance of the markets in which we operate are necessarily subject to a high degree of uncertainty and risk.
2
A B O U T O B S E VA
Strategic Focus
(Women ages 15 - 49)
Uterine Fibroids
ObsEva is a clinical stage
biopharmaceutical company Endometriosis
dedicated exclusively to
women’s health.
Infertility - ART
We are passionately focused on
addressing serious, quality-of-life
impacting conditions and Preterm Labor
reproductive challenges faced by
women around the world. Preeclampsia
Ticker: OBSV (NASDAQ), OBSN (SIX) Headquarters: Geneva, Switzerland U.S. office: Boston MA, Employees: 45
3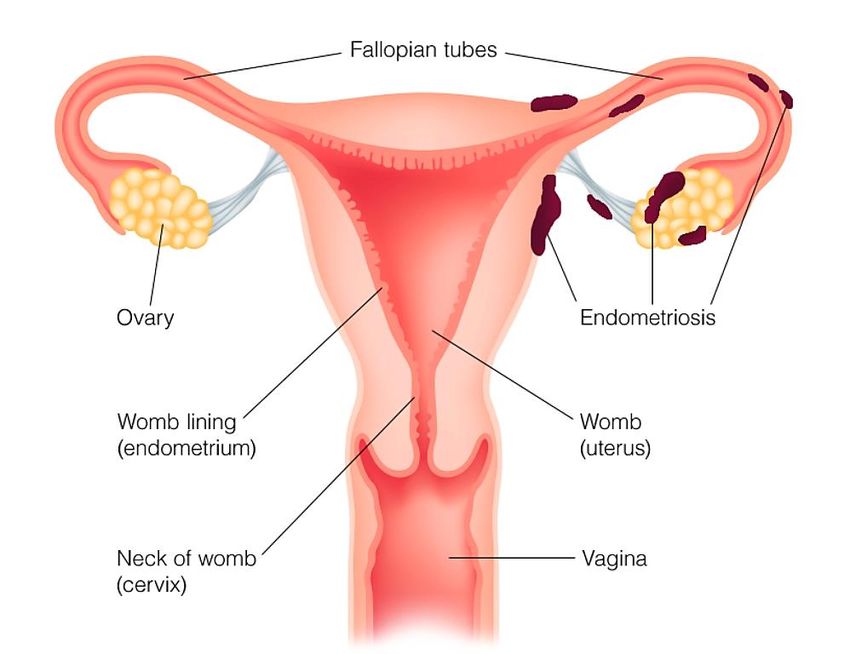
LEADERSHIP
Ernest Loumaye, MD, PhD Tim Adams Jean-Pierre Gotteland, PhD Elke Bestel, MD Ben T.G. Tan, MSc
Co-founder & Chief Financial Officer Chief Scientific Officer Chief Medical Officer Vice President,
Chief Executive Officer Commercial & BD
4
C O M PA N Y H I G H L I G H T S
• Three NCE’s focused on Women’s Health/Fertility Addressing Major Unmet Need
• Compounds with 1st/best in class potential addressing significant markets
Nolasiban for IVF in Phase 3
Linzagolix (OBE2109) for endometriosis & uterine fibroids in Phase 3
OBE022 for PTL in Phase 2
• Own worldwide rights for all (ex Linzagolix in Asia)
IP protection for all up to late 2030’s
Retaining commercial rights
• Value creating events in 2019
Finalize US trial design and begin US IVF development program 2019
Nolasiban Prepare commercial operations in EU & US 2019
Primary endpoint pregnancy results from EU IMPLANT4 in IVF Q4 2019
Planned EU MAA submission for IVF Q4 2019
Phase 3 US & EU endometriosis Start Q1 2019
Linzagolix
6 Month US & EU Phase 3 PRIMROSE 1 and 2 Results in uterine fibroids H2 2019
Interim efficacy from Phase 2a PROLONG in PTL Q1 2019
OBE022
Complete PROLONG follow-up and move to Phase 2b H2 2019
5
ROBUST PIPELINE
PRODUCT CANDIDATE PRECLINICAL PHASE 1 PHASE 2 PHASE 3 STATUS & NEXT COMMERCIAL
MILESTONE RIGHTS
IVF: IMPLANT2 EU *** Primary endpoint data
Phase 3 IMPLANT 4
NOLASIBAN & EU MAA filing Q4 2019
Oral oxytocin IVF: IMPLANT4 EU Worldwide
receptor antagonist **
US IMPLANT 3 Phase 3
IVF: IMPLANT3 US Initiation 2019
Phase 2b EDEWEISS
Complete
Endometriosis: EDELWEISS ** FDA EOP2 Meeting Q4
LINZAGOLIX* 2018 & initiate Phase 3
(OBE2109) Q1 2019 Worldwide
Oral GnRH receptor US/EU Phase 3 ex-Asia
antagonist PRIMROSE 1 & 2
Enrolling
Uterine Fibroids: PRIMROSE 1 & 2
6 month Primary Endpoint
Data H2 2019
EU Phase 2a PROLONG
OBE022
Oral PGF2α receptor Preterm Labor: PROLONG Worldwide
Interim Efficacy
antagonist Q1 2019
* Kissei developing for Asia
** Week 12 primary and secondary endpoints met in June 2018
*** Week 10 pregnancy, primary endpoint met in February 2018
6
NOLASIBAN (OBE001) Improving In Vitro Fertilization Outcomes

NOLASIBAN (OBE001)
O R A L O X Y T O C I N R E C E P T O R A N TA G O N I S T T O I M P R O V E I V F O U T C O M E S
Nolasiban AT-A-GLANCE Nolasiban INDICATIONS
• Oxytocin Receptor Antagonist In Vitro Fertilization (IVF)
• Licensed from Merck Serono • Market size: >2.01M ART/IVF cycles/year globally
(~230K in US in 2015, ~680K in Europe in 2013 and
• IP Protection to late 30’s ~400K in Japan in 2015)
• ART cycle cost: $10-20K+ in the US, € 4-10K in the
EU and $3-6K in Japan
• Estimated global sales of fertility drugs > $ 2.5B
NOLASIBAN
Well-characterized profile; Phase 2 clinical trial completed; EU Phase 3 completed
>650 subjects Orally active - tmax at 2h; t1/2= 12h; Single oral 900mg
exposed Well tolerated High bioavailability optimal dose
* Source: IQVIA’s MIDAS Data Tool , 2018.
8
I N F E R T I L I T Y: A G L O B A L P U B L I C H E A LT H I S S U E , B U T
I V F I S C O S T LY A N D N O T E F F I C I E N T E N O U G H
• Infertility – a health & societal issue
9% of women 20-44 affected globally
Ageing population problematic
• Too few healthy babies Japan: ~1.6 million
women aged 20-44
Despite good quality embryos & using best practice (9% of 18 million)
transfer techniques, IVF success rate not optimal
• IVF comes with a significant cost
Couples often self fund U.S.: ~7.7 million
women aged 15-44
Japan: ~1.6 million
women aged 20-44
Payers see an unacceptably (12.1% of 64mn) (9% of 18 million)
(CDC 2015)
high multiple pregnancy rate Europe: ~7.2 million
Society pays a higher cost women aged 20-44
(9% of 80 million)
per healthy baby
* WHO infertility website, April 2018.
http://www.who.int/reproductivehealth/topics/infertility/perspective/en/
9
NOLASIBAN: MECHANISM OF ACTION
I N C R E A S I N G C L I N I C A L P R E G N A N C Y A N D L I V E B I R T H R AT E
Nolasiban
Functional Oxytocin receptors
are expressed in human non-
pregnant uterus on:
• Myometrium smooth muscle cells
• Uterus arteries smooth muscle cells
• Endometrium glandular epithelial cells
10NOLASIBAN: IMPLANT2 PHASE 3 CLINICAL
T R I A L P R O TO C O L
Main Study Follow-Up
• Age Range: 18-36 Primary Analysis
• Fresh D3 and D5 SET
• Max 1 prior failed IVF 10 week
• P4 ≤ 4.7 nmol/L on day of 1 month
hCG pregnancy rate
• Vaginal progesterone for
luteal support 900 mg, n=380 Not preg. FU
D3 or
SCREENING IVF/ICSI
D5 SET*
7–8 months 6 months
Placebo, n=380 Preg. Preg. FU Neonatal FU
Randomize Live Birth
Target enrollment of 760 patients
*SET = Single Embryo Transfer 41 fertility centers in 9 European countries
11NOLASIBAN: IMPLANT2
F O R T H E T R E AT M E N T O F I N F E R T I L I T Y
IMPLANT 2:
• EU phase 3, randomized, double blind, clinical trial assessing Nolasiban compared to placebo for
improving the rate of pregnancy in patients undergoing IVF or ICSI due to low fertility
Initial data released in February 2018
• Met primary endpoint of increase in 10 week on-going pregnancy rate
Additional data released in October 2018
• Significant improvement in live birth rate vs. placebo
• ASRM data showed lower miscarriage rate
12I M P L A N T 2 : P R I M A RY E F F I C A C Y E N D P O I N T
P O O L E D D AY 3 A N D D AY 5 S E T
Pooled D3 and D5
Nolasiban
Placebo Increase p
900 mg
n 390 388
Ongoing
pregnancy rate 28.5% 35.6% 7.1% 0.031
at 10 weeks
• Absolute 7.1% increase compared to placebo with > 5% considered
clinically meaningful
• Relative 25% increase compared to placebo
13N O L A S I B A N : I M P L A N T 2 : S E C O N D A RY E F F I C A C Y
ENDPOINT
S U B G R O U P E F F I C A C Y A N A LY S E S : I N D I V I D U A L D 3 A N D D 5 S E T
D3 D5
Nolasiban Nolasiban
Placebo Delta p Placebo Delta p
900 mg 900 mg
N 194 194 196 194
Ongoing pregnancy
22.2% 25.3% 3.1% 0.477 34.7% 45.9% 11.2% 0.034
rate at 10 weeks
Live birth rate 22.7% 24.7% 2.5% 0.552 33.2% 44.8% 11.6% 0.025
• Live Birth Rate increased by a relative 33% after SET at day 5
14NOLASIBAN: PREGNANCY OUTCOMES AND SAFETY
I N I V F PAT I E N T S
C U M U L AT I V E D ATA F R O M 2 P L A C E B O - C O N T R O L L E D R A N D O M I Z E D
TRIALS
Nolasiban Placebo
(n=570) (n=455)
Positive pregnancy test (Day 14 post-OPU) 274 (48.1%) 188 (41.3%)
Pregnancy loss (≤ week 10) 61 (22.3%*) 53 (28.2%*)
Ectopic pregnancy 3 (1.1%*) 5 (2.7%*)
Ongoing pregnancy at week 10 post-ET 213 (37.4%) 130 (28.6%)
Pregnancy loss (week 10 to 24) 6 (2.8%**) 3 (2.3%**)
Fetus/neonate with Serious Adverse Event 15 (7.0%**) 9 (6.9%**)
Congenital malformations 11 (5.2%**) 7 (5.4%**)
* % of positive pregnancy test at 14 days post-OPU
** % of ongoing pregnancy at week 10
15N O L A S I B A N E N A B L E S U S TO D E L I V E R M O R E
B A B I E S AT L O W E R C O S T
• Nolasiban can deliver 1/3 more babies
Day 5 SET increases LBR by 11.6%,
a 33% relative increase
No evidence of tolerability or safety issues
Reduced miscarriage rate, no increase in congenital malformation Japan: ~1.6 illion
women aged 20-44
• Potential to lower cost of obtaining a baby (9% of 18 million)
Targeting more babies delivered at same total IVF costs
No incremental cost due to side effects
Estimated IVF cycle cost reduction $4-20 K depending on country
• Potential to lower healthcare costs
Reduce use of DET (Double Embryo Transfer)
Lower incidence of multiple pregnancies
Avoids mother/infant costs related to delivery and neonatal care
Avoids long term costs related to development and chronic health of twins, triplets, or more
16N O L A S I B A N : M A R K E T S T R AT E G Y
LEAN COMMERCIAL INFRASTRUCTURE FOCUSED ON SMALL
NUMBER OF ART CLINICS IN THE U.S. AND EU
UNITED STATES
• ~500 ART Clinics in the U.S.
• Clusters
EUROPE
• ~906 ART Clinics in EU 5
17LINZAGOLIX (OBE2109) Potential Best in Class Oral GnRH antagonist Indications: Endometriosis and Uterine Fibroids
ENDOMETRIOSIS AND UTERINE FIBROIDS
R E D U C I N G E S T R O G E N A L L E V I AT E S S Y M P T O M S
Endometriosis Uterine Fibroids
Symptoms: pelvic pain and infertility Symptoms: heavy menstrual bleeding,
pelvic pressure/pain, and dysmenorrhea
19UNMET MEDICAL NEED IN ENDOMETRIOSIS &
UTERINE FIBROIDS THERAPY
LARGE U.S. MARKET SIZE EXISTING TREATMENTS
Endometriosis
• 2.5 million women diagnosed and
Oral Contraceptives/NSAID’s/Opioids
treated annually
• Limited symptom reduction
• Seeking to unlock another 2.5 million
undiagnosed due to non-specific LUPRON® Injections (GnRH agonist)
symptoms and invasive laparoscopy • Not ideal for younger, chronic population
• Associated with initial symptom flares
• Full estrogen suppression
Uterine Fibroids • ABT* mandatory > 6 months
• 4 million women diagnosed and Surgical Interventions
treated annually • Avoid hysterectomy to preserve fertility & integrity
• Approximately 200,000 surgeries • High rate of reconcurrence after conservative surgery
(Hysterectomy) annually
* Low dose Add Back Therapy (ABT) = estradiol/norethindrone acetate - tablet 1.0 mg/ 0.5 mg
20LINZAGOLIX
P O T E N T I A L B E S T - I N - C L A S S , O R A L , G N R H R E C E P T O R A N TA G O N I S T
Linzagolix AT-A-GLANCE Linzagolix INDICATIONS
• GnRH oral receptor antagonist Uterine Fibroids
• Symptoms: heavy menstrual
• OBE2109 (KLH-2109)
bleeding and abdominal pain
• Licensed from Kissei (WW rights, excludes • Primary goal is to reduce/eliminate
Asia) bleeding
• IP protection to late 2030’s Endometriosis
• > 1600 female subjects exposed to date • Symptoms: pain and infertility
• Primary goal is to alleviate pain
21B E N E F I T S O F G n R H A N TA G O N I S T S V S A G O N I S T S
Allows for
partial or full
estrogen
• Competitively suppression
based on
preventing endogenous Immediate need
GnRH from binding and action
activating its pituitary No initial flare Rapid
Reversibility
receptor & worsening
of symptoms
• Contrasting with GnRH More suitable
agonists, inducing for chronic
neither downregulation, therapy
nor desensitization of
the receptors Oral dosing
enhances Consistent
patient PK/PD
compliance
22
22LINZAGOLIX (OBE2109) PHASE 2B CLINICAL TRIAL
( E D E LW E I S S ) I N E N D O M E T R I O S I S PAT I E N T S
Primary endpoint:
VRS pain score Key secondary
responder rate endpoint: BMD**
June 2018 September 2018
12 weeks
Placebo 12 weeks
8–14 weeks 50 mg daily 50 mg daily 24 weeks
LEAD-IN 75 mg daily 75 mg daily FOLLOW-UP
100 mg daily 100 mg daily
200 mg daily 200 mg daily Optional
extension
75 mg daily* * Titrated dose 50–100 mg 6 m + 6m f-up
* Titration after 12 weeks based on E2 serum level at weeks 4 and 8
Enrollment 328 patients • 50 sites in US (n=177) • 14 sites in EU (n= 151)
**BMD: Bone Mineral Density
23L I N Z A G O L I X : P H A S E 2 B E D E LW E I S S T R I A L
F O R T H E T R E AT M E N T O F E N D O M E T R I O S I S
E D E LW E I S S :
• Phase 2b, randomized, double blind, placebo controlled clinical trial designed to evaluate the safety
and efficacy of multiple doses of Linzagolix
12 week data was released in June 2018
• Met primary endpoint of increased response rates on 0-3 VRS pain scale
24-week data was released in September 2018
• Pain response rates continued to increase, minimal BMD decline from baseline as expected
75mg w/o ABT and 200mg with ABT are the Doses Targeted For Phase 3 Development
24L I N Z A G O L I X : E D E LW E I S S P R I M A RY E N D P O I N T
O V E R A L L P E LV I C PA I N R E S P O N D E R A N A LY S I S AT W 1 2 / W 2 4
% of subjects with ≥ 30% reduction of Mean Overall Pelvic Pain Score (0-3 VRS)
Baseline Change Placebo/
Placebo 50 mg FD 75 mg FD 75 mg TD 100 mg FD 200 mg FD
VRS score for 100 mg FD
(N=53) (N=49) (N=56) (N=58) (N=51) (N=56)
Overall Pain (N=53)
Week 24 (n) - 36 40 48 45 39 44
≥ 30% reduction (%) - 63.9 52.5 70.8 66.7 66.7 77.3
Week 12
≥ 30% reduction (%) 34.5 - 49.4 61.5 56.4 56.3
95% CI 22.38, 49.09 - 34.92, 63.90 51.76, 70.38 41.59, 70.17 42.28, 69.42
Odds Ratio - - 1.85 3.03 2.45 2.45
95% CI - - 0.791, 4.317 1.469, 6.239 1.049, 5.741 1.069, 5.593
p-value
- - 0.155 0.003 0.039 0.034
vs. Placebo
25L I N Z A G O L I X : E D E LW E I S S S E C O N D A RY E N D P O I N T
N M P P R E S P O N D E R A N A LY S I S
% of subjects with ≥ 30% reduction of Mean NMPP score (0-3 VRS)
Change from Placebo/
Placebo 50 mg FD 75 mg FD 75 mg TD 100 mg FD 200 mg FD
Baseline 100 mg FD
(N=53) (N=49) (N=56) (N=58) (N=51) (N=56)
VRS score for NMPP (N=53)
Week 24 (n) - 35 45 48 24 55 44
≥ 30% reduction (%) - 60.0 50.0 72.9 64.4 64.1 72.7
Week 12
≥ 30% reduction (%) 37.1 - 46.2 58.5 61.5 47.7
95% CI 24.58, 51.67 - 32.13, 60.97 48.72, 67.58 46.51, 74.54 34.20, 61.50
Odds Ratio - - 1.46 2.38 2.70 1.54
95% CI - - 0.628, 3.383 1.170, 4.859 1.156, 6.318 0.682, 3.496
p-value
- - 0.380 0.017 0.022 0.297
vs. placebo
26L I N Z A G O L I X : E D E LW E I S S A D D I T I O N A L O U T C O M E S
7 5 M G T O 2 0 0 M G S I G N I F I C A N T LY A N D C O N S I S T E N T LY I M P R O V E D
A S S O C I AT E D S Y M P T O M S
Efficacy
Other patient symptoms (VRS):
• Dyschezia
• Dyspareunia (statistical significance at the 200mg dose)
Patient Well Being assessed by the following:
• Endometriosis Health Profile-30 score;
• Patient Global Impression of Change scale (PGIC);
• Patient Global Impression of Severity (PGIS);
• Activity impairment score; and
• Modified Biberoglu & Behrman score
Tolerability
Placebo Linzagolix Linzagolix Linzagolix Linzagolix
(N=55) 50 mg; (N=49) 75 mg FD/TD; (N=114) 100 mg; (N=52) 200 mg; (N=57)
HOT FLUSH 6 (10.9) 7 (14.3) 22 (19.3) 14 (26.9) 24 (42.1)
27L I N Z A G O L I X : E D E LW E I S S C H A N G E I N B O N E M I N E R A L
DENSITY (BMD)
MEAN % CHANGE FROM BASELINE TO MONTH 6
Lumbar Spine To t a l H i p Femoral Neck
1
0.5
0
-0.5
Plc
-1
Plc/ 100 mg2
-1.5 50 mg
-1.6% lower bound CI for 75mg 75 mg FD
-2
75 mg TD
-2.2% Cutoff requiring ABT
-2.5 100 mg
200 mg
-3
-3.6% lower bound CI for 200mg
28LINZAGOLIX, GIVING WOMEN WITH ENDOMETRIOSIS THEIR
LIVES BACK
A L L E V I AT I N G S Y M P T O M S W H I L E M I N I M I Z I N G F U T U R E H E A LT H R I S K S
• Effective at reducing pain
Effective at reducing menstrual & non-menstrual pain
Effective at reducing pain during intercourse (dyspareunia) and during defecation (dyschezia)
• Potential improvement in how she feels
Improvement of “well being”
Allow couples to live more “normally”
• ABT needed only in minority of patients
Nearly ¾ patients may achieve significant symptom relief with linzagolix 75 mg once daily, no need for
ABT to protect BMD
ABT boxed warning – low probability, but potentially very severe health consequences and
contraindicated for women at risk for thrombosis
ABT may increase bleeding/spotting
Option for ABT with linzagolix 200 mg once daily only when necessary
29LINZAGOLIX: PRIMROSE 1 & 2
P H A S E 3 C L I N I C A L T R I A L S F O R T H E T R E AT M E N T O F
UTERINE FIBROIDS
Primary endpoint:
Responder-HMB Reduction
8–14 weeks 24 weeks
H2:19 28 weeks
16-OBE2109-008 24 weeks Placebo + placebo add-back
100% US sites
n = 100 Placebo + placebo add-back 200mg + add-back
n = 100 100mg + placebo add-back 100mg + placebo add-back
24w follow-up
n = 100 Screening 100 mg + add-back 100 mg + add-back
n = 100 200 mg + placebo add-back 200 mg + add-back
n = 100 200 mg + add-back 200 mg + add-back
16-OBE2109-009
70% Europe
30% US sites n = 100 Placebo + placebo add-back 200mg + add-back
n = 100 100mg + placebo add-back 100mg + placebo add-back
24w follow-up
n = 100 Screening 100 mg + add-back 100 mg + add-back
n = 100 200 mg + placebo add-back 200 mg + add-back
n = 100 200 mg + add-back 200 mg + add-back
• IND granted in April 2017
• Currently recruiting • Aiming at supporting the registration of two regimens of administration
30OBE022 Treating Preterm Labor
OBE022
PO TEN TIAL FIR ST- IN - C L ASS, O R AL AN D SEL EC TIVE PG F2 Α
R E C E P T O R A N TA G O N I S T F O R P R E T E R M L A B O R ( P T L )
OBE022 AT-A-GLANCE OBE022 INDICATION
• Prostaglandin F2α (FP) receptor antagonist Preterm labor (GA 24-34 week)
• Incidence: USA: 500,000; EU: 500,000;
• Licensed from Merck Serono Asia: 6,900,000
• Composition of matter protection through • Economic burden for premature infants:
~$26Bin the US ($16.9B in infant medical
2037 with PTE
care)
32B L O C K I N G P G F 2 Α R E C E P TO R H A S P O T E N T I A L TO
T R E AT P T L W I T H I M P R O V E D S A F E T Y O V E R N S A I D S
Phospholipids Phospholipids
‘Inflammation’
ArachidonicAcid Prostaglandins ArachidonicAcid
PGHS-1/2 = COX1/2
Indomethacin Cytokines PGHS-1/2 = COX1/2
Chemokines
PGH2 PGH2
OBE022
PGE2 PGF2α PGE2 PGF2α
EP1 EP2 EP1 EP2
FP FP
EP3 EP4 EP3 EP4
UTERUS: UTERUS:
CONTRACT RELAX CONTRACT CONTRACT RELAX CONTRACT
kidney, brain, vascular smooth muscle PGF2α contracts the myometrium and
RUPTURE PGF2α metabolites rise in amniotic fluid
Vasoconstriction of ductus arteriosus, before and during labor
renal and mesenteric arteries
Platelet aggregation inhibition CONTRACT PGF2α upregulates enzymes causing
cervix dilatation and membrane rupture
DILATE
33O B E 0 2 2 : P R O L O N G P H 2 A S T U D Y ( PA R T S A A N D B )
Preliminary safety Final Part A Main study end End of Infant FU
& PK analysis Main analysis
Part A Dosing for 7d Maternal + neonatal FU 24-month Infant FU
Up to 8 patients
Open-label: Atosiban + OBE022
Final Part B
Main analysis
Part B Dosing for 7d Maternal + neonatal FU 24-month Infant FU
up to 60 patients + up to 60 patients
• Double-blind: Atosiban + OBE022 vs Atosiban + PLACEBO
• Part A concluded in Q3 18
• Part B initiated in Q4 18
34C O M PA N Y H I G H L I G H T S
• Three NCE’s focused on Women’s Health/Fertility Addressing Major Unmet Need
• Compounds with 1st/best in class potential addressing significant markets
Nolasiban for IVF in Phase 3
Linzagolix (OBE2109) for endometriosis & uterine fibroids in Phase 3
OBE022 for PTL in Phase 2
• Own worldwide rights for all (ex Linzagolix in Asia)
IP protection for all up to late 2030’s
Retaining commercial rights
• Value creating events in 2019
Finalize US trial design and begin US IVF development program 2019
Nolasiban Prepare commercial operations in EU & US 2019
Primary endpoint pregnancy results from EU IMPLANT4 in IVF Q4 2019
Planned EU MAA submission for IVF Q4 2019
Phase 3 US & EU endometriosis Start Q1 2019
Linzagolix
6 Month US & EU Phase 3 PRIMROSE 1 and 2 Results in uterine fibroids H2 2019
Interim efficacy from Phase 2a PROLONG in PTL Q1 2019
OBE022
Complete PROLONG follow-up and move to Phase 2b H2 2019
35THANK YOU
November 2018
NASDAQ:OBSV | SIX:OBSNYou can also read