IS FLEXIBLE CYSTOSCOPY NECESSARY IN THE INVESTIGATION OF NON-VISIBLE HAEMATURIA?
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Original Article
DOI:10.22374/jeleu.v4i2.124
IS FLEXIBLE CYSTOSCOPY NECESSARY IN THE INVESTIGATION OF NON-
VISIBLE HAEMATURIA?
Jennifer Nowers1, Mark O. Kitchen1,2*, Sneha Rathod1, Caroline Lipski1, Sharbathana Nageswaran1,
Shahjahan Aslam1, Anurag Golash1
1
Urology Department, University Hospitals of North Midlands NHS Trust, Staffordshire, UK; 2School of
Medicine, Keele University, Staffordshire, UK
*Author for correspondence: Mark O. Kitchen: m.o.kitchen@keele.ac.uk.
Abstract
Background: Historic evidence suggests up to 16% (approximately) of non-visible haematuria (NVH) refer-
rals result in Urological cancer diagnosis. The majority are bladder cancers, for which flexible cystoscopy is
regarded the “gold standard” diagnostic procedure. Recent changes to suspected cancer referral guidelines,
public information campaigns and reduced smoking prevalence may have changed this percentage. We
retrospectively calculated cancer detection rates from NVH referrals to assess whether flexible cystoscopy,
an invasive and morbid procedure, remains necessary.
Patients and methods: All patients referred to our University teaching hospital on a suspected (“two-
week”) cancer pathway with NVH over a 16-week period were included. Clinical and demographic data
were collected for a series of 200 patients (96 male, age range 27–92, median 68).
Results: Only eight patients had urological malignancy found (two renal and six bladder cancers). Both
renal, and four bladder cancers, were identified on imaging prior to flexible cystoscopy. Only two bladder
cancers were therefore detected by cystoscopy; one low-risk non-muscle invasive (patient has already been
discharged) and one in a patient that was unfit for treatment (died of heart failure). Only seven (3.5%) of
the patients were offered the option of not undergoing flexible cystoscopy.
Conclusion: Our analyses suggest that flexible cystoscopy is rarely of benefit in patients with NVH. We
suggest that patients should be given an accurate risk of bladder cancer diagnosis during the consent pro-
cess. We advocate that flexible cystoscopy can be avoided for the majority of NVH referrals, particularly
in patients without strong risk factors for urothelial cell carcinoma. Avoidance of flexible cystoscopy would
reduce patient risks from procedural morbidity, reduce risks of acquiring coronavirus from hospital atten-
dance, and there could be huge reductions in financial and service delivery demands in an overstretched
secondary-care service.
INTRODUCTION despite improvements in technology and vision/resolu-
tion, FC remains a user-dependent procedure, with poor
Flexible cystoscopy (FC) has been considered the
sensitivity for flat urothelial lesions such as carcinoma-
“gold standard” to visualize the bladder for several de-
in-situ (CIS).4 Therefore, it comprises only part of a
cades.1 As such, it is recommended in the investigation
multi-modal approach to haematuria investigation.
of haematuria by the National Institute for Health and
FC can be a morbid procedure, causing considerable
Care Excellence (NICE) and European Association of
(but temporary) irritative lower urinary tract symptoms
Urology (EAU) Bladder Cancer guidelines.2,3 However,
J Endolum Endourol Vol 4(2):e7–e12; June 22, 2021.
This article is distributed under the terms of the Creative Commons Attribution-
Non Commercial 4.0 International License. © Nowers, et al.
e7
Nowers_WKBK.indd 1 6/21/2021 12:23:33 PM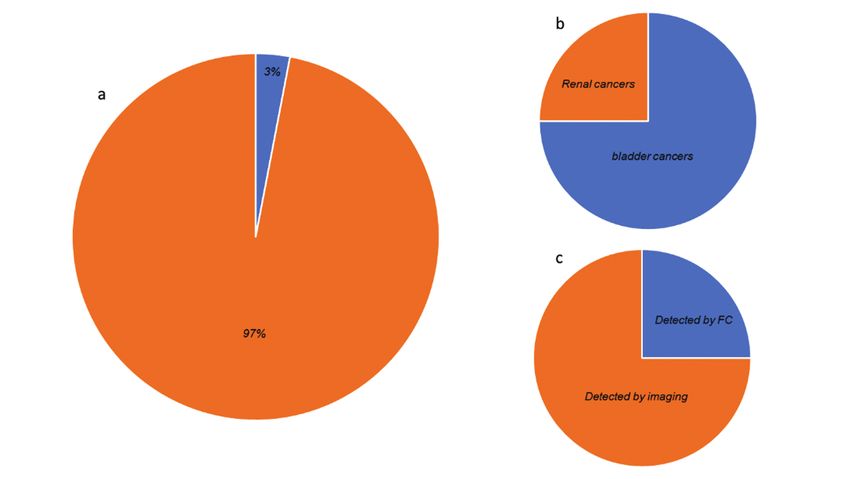
Is Flexible Cystoscopy Necessary in the Investigation of Non-Visible Haematuria?
for a significant number of patients.5 It also has at- pathway for investigation of NVH, was identified at
tributable risks of infection (up to 10%) and sepsis our tertiary cancer centre and University teaching
(Is Flexible Cystoscopy Necessary in the Investigation of Non-Visible Haematuria?
Table 1. Patient Demographics
Total Age Median Current Occupational risk Family
number range age smokers Ex-smokers factors history
Male 96 27–92 67 10 28 11 1
Female 104 31–88 68 11 20 7 2
Figure 1. Cancers found. (a) Pie-chart representation of the number of bladder cancers found in our NVH
case series: the orange segment represents no cancer found (n = 194, 97%) and the blue segment represents
bladder cancers found (n = 6, 3%). (b) Pie-chart representation of all cancers found by site: the blue segment
represents bladder cancers (n = 6) and the orange segment represents renal cancers (n = 2). (c) Pie-chart
representation of cancers identified by imaging prior to FC (bladder cancers orange segment, n = 6, and
renal cancers blue segment, n = 2).
No prostate cancers were suggested by screening Regression analyses
PSA and/or DRE (that were subsequently proven on Multivariate regression analyses did not find any
mpMRI and/or prostate biopsy). significant correlation with age, gender, smoking
Two bladder tumours were identified only by FC: in status, or occupational or family risk factors to blad-
these cases, one was a sub-centimetre solitary G1pTa der cancer diagnosis.
(patient already discharged from follow-up), and the DISCUSSION
other was a solitary 2 cm pedunculated papillary tu-
mour, however, the patient was unfit for trans-urethral There are multiple conflicting factors regarding
resection and has since died of heart failure. the need for FC in NVH patients. The risk of bladder
J Endolum Endourol Vol 4(2):e7–e12; June 22, 2021.
This article is distributed under the terms of the Creative Commons Attribution-
Non Commercial 4.0 International License. © Nowers, et al.
e9
Nowers_WKBK.indd 3 6/21/2021 12:23:33 PMIs Flexible Cystoscopy Necessary in the Investigation of Non-Visible Haematuria?
cancer missed by preliminary investigations and pa- Reassuringly, if a cancer is missed initially by US, the
tient choice (FC may be wanted for “peace of mind”), patient is likely to represent with further episodes of
compete with user-dependence, poor sensitivity, as- NVH, or with new VH, but the very low rate (Is Flexible Cystoscopy Necessary in the Investigation of Non-Visible Haematuria?
clear discussion of the low risks of finding bladder Final approval of the version to be published: JN,
cancer would prompt patients to decline FC on a risk MK, AG
versus benefit judgment, despite many patients being REFERENCES
initially keen for referral and investigation.4
Although patient safety and decreasing unnecessary 1. Samplaski MK, Jones JS. Two centuries of cystoscopy:
invasive investigations and risks are the key drivers The development of imaging, instrumentation and
to our study, there are potentially huge reductions in synergistic technologies. BJU Int. 203;103(2):154–8.
financial outlay and service demands that could be http://dx.doi.org/10.1111/j.1464-410X.2008.08244.x
made, if FC were not routinely performed for NVH 2. Bladder cancer: Diagnosis and management NICE
guideline [NG2] [Internet]. 2015 [cited 2021 Feb 04].
patients. For example, our Trust could save more than
Available from: https://www.nice.org.uk/guidance/
750 (NVH) patient appointments and an estimated
ng2/chapter/1-Recommendations#diagnosing-and-
£220,000 per year, potentially reducing waiting list
staging-bladder-cancer-2
times for visible haematuria and other urgent refer-
3. Babjuk M, Burger M, Compérat E, Gontero P,
rals, and freeing funds for other essential services.
Liedberg F, Masson-Lecomte A, et al. European As-
CONCLUSION sociation of Urology (EAU) guidelines non-muscle
invasive bladder cancer [Internet]. 2021 [cited 2021
Although it is difficult to prove from our series, the
Feb 04]. Available from: https://uroweb.org/guideline/
risks and associated procedural morbidity of FC almost
non-muscle-invasive-bladder-cancer/
certainly outweigh the potential benefits in patients 4. Jubber I, Shariat SF, Conroy S, Tan WS, Gordon PC,
with NVH, given the low prevalence of bladder cancer Lotan Y, et al. Non-visible haematuria for the detec-
and the minimal risk of missing clinically significant tion of bladder, upper tract, and kidney cancer: An
disease. The demand on over-stretched resources, and updated systematic review and meta-analysis. Eur
the need to reduce unnecessary hospital attendance Urol. 2020;77(5):583–98. http://dx.doi.org/10.1016/j.
during the global coronavirus pandemic, are also strong eururo.2019.10.010
arguments that we should not routinely perform FC for 5. Burke DM, Shackley DC, O’Reilly PH. The
patients with NVH. The authors advocate, however, community-based morbidity of flexible cystoscopy.
the use of clinical judgement in all cases and suggest BJU Int. 2002 Mar;89(4):347–9. http://dx.doi.
the risk versus the benefit is discussed with patients org/10.1046/j.1464-4096.2001.01899.x
to inform their decision-making. 6. Cusumano JA, Hermenau M, Gaitanis M, Travis M,
LaPlante KL, Tran TY, et al. Evaluation of post–flex-
FUNDING
ible cystoscopy urinary tract infection rates. Am J
N/A Health Syst Pharm. 2020;77(22):1852–8. http://dx.doi.
CONFLICTS OF INTEREST org/10.1093/ajhp/zxaa270
7. National health Service (NHS) England. COVID-19
All authors declare no conflicts of interest. hospital activity [Internet]. [cited 2021 Feb 06]. Avail-
ACKNOWLEDGEMENTS able from: https://www.england.nhs.uk/statistics/
statistical-work-areas/covid-19-hospital-activity/
N/A 8. Social Science Statistics online software [Internet].
AUTHORSHIP CREDIT [cited 2021 Mar 19]. Available from: https://www.
socscistatistics.com/
Concept and design of study: MK, AG 9. Stoke-On-Trent tobacco control strategy 2015/18
Acquisition of data, or analysis and interpretation [Internet]. [cited 2021 Feb 13]. Available from: www.
of data: MK, SR, CL, SN, AA stoke.gov.uk/download/downloads/id/788/tobacco-
Drafting the article or revising it critically for control-strategypdf.pdf
intellectual content: JN, MK 10. Tan WS, Feber A, Sarpong R, Khetrapal P, Rodney S,
Jalil R, et al. Who should be investigated for haematuria?
J Endolum Endourol Vol 4(2):e7–e12; June 22, 2021.
This article is distributed under the terms of the Creative Commons Attribution-
Non Commercial 4.0 International License. © Nowers, et al.
e11
Nowers_WKBK.indd 5 6/21/2021 12:23:33 PMIs Flexible Cystoscopy Necessary in the Investigation of Non-Visible Haematuria?
Results of a contemporary prospective observational cystourethroscopy. BJU Int. 2019 May;123(5A):E29–33.
study of 3556 patients. Eur Urol. 2018 Jul;74(1):10–14. http://dx.doi.org/10.1111/bju.14662
http://dx.doi.org/10.1016/j.eururo.2018.03.008 13. Rod JE, Oviedo-Trespalacios O, Cortes-Ramirez J.
11. Casey RG, Catto JWF, Cheng L, Cookson MS, Herr A brief-review of the risk factors for covid-19 sever-
H, Shariat S, et al. Diagnosis and management of ity. Rev Saude Publica. 2020;54:60. http://dx.doi.
urothelial carcinoma in situ of the lower urinary tract: org/10.11606/s1518-8787.2020054002481
A systematic review. Eur Urol. 2015;67(5):876–88. 14. Hrouda D, Emberton M, Hampson SJ. Written con-
http://dx.doi.org/10.1016/j.eururo.2014.10.040 sent is haphazard for minor urological procedures.
12. Clennon EK, Acevedo AM, Sajadi KP. Safety and effectiveness Br J Urol. 1997 Apr;79(4):503–4. http://dx.doi.
of zero antimicrobial prophylaxis protocol for outpatient org/10.1046/j.1464-410x.1997.00104.x
J Endolum Endourol Vol 4(2):e7–e12; June 22, 2021.
This article is distributed under the terms of the Creative Commons Attribution-
Non Commercial 4.0 International License. © Nowers, et al.
e12
Nowers_WKBK.indd 6 6/21/2021 12:23:33 PMYou can also read