Making changes to community urgent care services - Right care, right place, first time - Pre-consultation business case Barking and Dagenham ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Making changes to
community urgent care
services
Pre-consultation business case
Barking and Dagenham, Havering and
Redbridge (BHR) clinical commissioning
groups (CCG)
May 2018
Right care, right place,
first time
1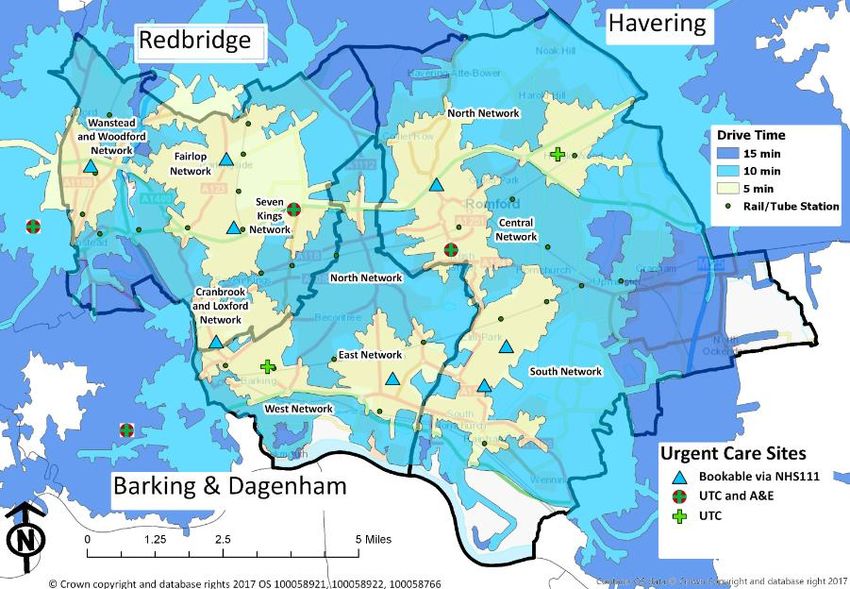
Contents
1.0 Executive summary 3
2.0 Context 4
Community urgent care review 4
Aims and objectives 4
Scope of this review 4
Current urgent care service offer 5
Service location map 5
Urgent and emergency care service usage 5
Primary care 6
Wound care 8
National context 8
Financial context 10
2.0 Case for change 12
What is urgent care? 12
BHR vision for urgent and emergency care 12
Variation in existing community urgent care services 12
Duplicate attendances 12
3.0 Engagement to date - urgent care co-design and research 16
Learning from our engagement 17
4.0 Options development and selection 18
5.0 Context for our options 20
Click or call before you come in - bookability 20
Consistent elements which will exist regardless of this proposed service change 20
Options for public consultation 22
What the future will look like 25
6.0 Proposed consultation process 27
Engagement plan for the next stage 27
Consultation process 27
Summary of the key stages of the consultation process and indicative timeline 28
7.0 Annex 1 - Case for change 29
8.0 Annex 2 - Variation in existing community urgent care services 29
9.0 Annex 3 - Current urgent and emergency care services 33
10.0 Annex 4 - Options appraisal 36
11.0 Annex 5 - Selected option description, activity shifts and savings profiles 43
12.0 Annex 6 - Consultation requirements 45
13.0 Glossary 47
2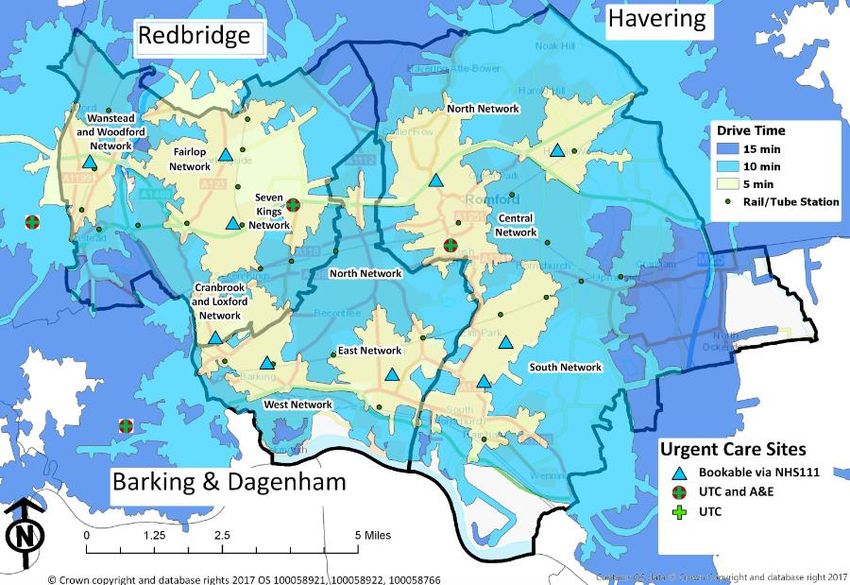
1.0 Executive summary
This draft pre consultation business case sets out the vision and options for future delivery of
community urgent care across Barking and Dagenham, Havering and Redbridge (BHR).
The document sets out the case for change, which was agreed through Governing Bodies in July
2017 and based on what we have learnt from the system and our people.
The case concerns the provision of walk-in centres, GP out of hours and GP access hubs with a
move to bookable activity through NHS 111 and provision of urgent treatment centres (UTC)
which will provide for walk-in and bookable services.
The clinical commissioning groups (CCGs) cannot leave the system as it is currently. Doing
nothing is not an option for the following reasons:
Local people have told us it’s too complicated and we want to provide services that are
easier to access and use
To do nothing is unaffordable. All urgent and emergency care service models illustrate
that doing nothing would cost us £2.57m per year above our current spend of £35.77m
If we do nothing then the profile of increasing demand and high levels of duplication
seen at all of our urgent care service and in our A&E departments will continue.
Ultimately, doing nothing will not help us resolve the challenges in our urgent and emergency
care system and will not ease the pressure on our emergency department, leading to an un-
sustainable model of care for our population. We need to deliver a simpler, cost-effective system
that meets our future needs.
Two options have been developed for the future model (detailed in section 5.0) and the proposal
is that we share these with our public in a formal consultation to determine the best fit for the
future.
Both options also include a move towards booked appointments for urgent care needs, building
on call or click before you come in. They will utilise NHS 111 as a way for us to help people
get the right care, right place, first time.
Audits have demonstrated that people are attending, and being seen in, A&E for conditions that
can be managed in an urgent treatment centre or in the community. We are currently working
with providers in the system to strengthen the streaming in the Urgent treatment Centres and
ensure that we maximise the attendances that can appropriately be seen in this setting. This will
reduce the number of patients seen in A&E and ensure that our performance is improved. This
activity shift is closely linked to the community urgent care review but not formally part of the
scope of this work.
Option 1 would see 12 sites in total, with four Urgent Treatment Centres open within Barking and
Dagenham, Havering and Redbridge (2 on hospital sites, and 2 in the community), plus eight
locations for booked community urgent care services. This option would save £1.07 million a year
and was our highest scoring option.
Option 2 would see 12 sites in total, with two UTCs within our area on our hospital sites,
although local people may still use those in our neighbouring boroughs (Newham and Whipps
Cross). Plus there will be 10 places to be booked when your own GP practice is closed and you
have an urgent health need. This option would save £1.19 million a year - £117,589 a year more
than Option 1, but despite this scored less overall than option 1.
During our engagement work we have consistently been given a clear message that urgent and
emergency care services are confusing. We feel both options will help us to address this critical
issue - and future-proof urgent care.
3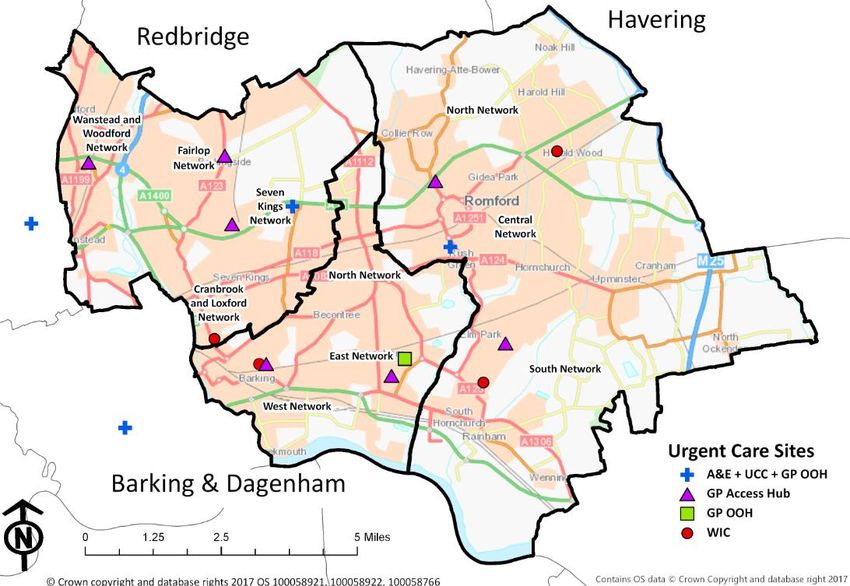
2.0 Context
Urgent and emergency care (UEC) has been a key challenge for our health economy for many
years with a background that includes:
A complex urgent and emergency care system with duplication and fragmentation across
services.
A challenged health economy that is struggling to manage increasing demand, partially
driven through population and health profile changes.
Key performance targets, particularly in accident and emergency, not being met.
In Barking and Dagenham, Havering and Redbridge (BHR), as with other parts of England,
increasing numbers of people are using NHS services every year. The current urgent and
emergency care system does not provide a good experience for patients as it can lead to a long
wait to see a GP or in accident and emergency (A&E), and also puts increasing pressure on our
hard-working frontline staff and clinicians.
Community urgent care review
Aims and objectives
The aims of the community urgent care review are to:
Improve patient experience including provision of a clear and defined service offer so
that patients can be confident about where to go for treatment, e.g. illness, injury,
urgent or emergency.
Improve quality including safety, consistency and right care, right place, first time – for
example this will this will support management of patients within the community.
Ensure services are designed to support the changing profile of population growth.
Support delivery of the urgent and emergency care performance targets.
Support system and financial sustainability.
Achieve an integrated service that works more effectively with 111, primary, community
and acute care services (in line with national requirements)
The objectives for the BHR proposals for community urgent care services were set out in the
case for change and summarised below:
Simplify the system for patients - provide a clear and defined service structure so that
patients can be confident about where to go for treatment, e.g. illness/ injury, urgent or
emergency need, and to reduce duplication and inappropriate attendances.
Move towards bookable appointments - the national requirement is bookable from
8am-8pm daily.
Consistent assessment -
Consistent assessment and re-direction when booking and at the front door of
services where people walk in, such as A&E.
Appointments bookable through centralised systems (phone and online) to
increase self-care and remove inappropriate appointments.
Plan for the changing profile of population growth.
Provide more local services, this being an opportunity to review the location of where
and how services are delivered.
Improved provision for children (newborn - 18 years) as they represent the greatest
proportion of attendance growth.
Scope of this review
The focus of this review is on the community based urgent care services:
GP out of hours service (GP OOH)
Primary care access hubs (or GP access hubs)
Walk-in centres (WICs).
4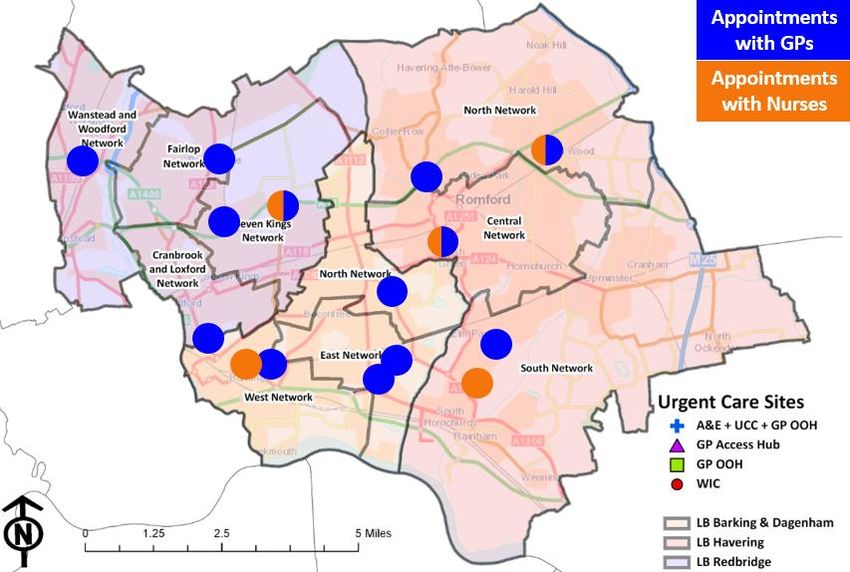
In 2017/18 these services alone delivered over 171,467 appointments which is 40% of the total
urgent and emergency care activity of 421,627.
Whilst the Urgent Care Centres (UCCs) at King George Hospital and at Queen’s Hospital do offer
a GP led/delivered service, the purpose of these co-located services is to manage patients who
present at A&E and are not suitable for an A&E attendance. There are separate plans in place to
bring these services up to the UTC specification.
This consultation is not about emergency care services or changes to A&E services at Queen’s,
King George, Whipps Cross or Newham hospitals - all of which serve our residents.
Current urgent care service offer
People in Barking and Dagenham, Havering and Redbridge are able to use a range of different
services when they feel they need medical advice urgently, but when it is not an emergency.
These include:
Pharmacists
General practice
NHS 111
Primary care access hubs (or GP access hubs)
GP out of hours service (GP OOH)
Urgent Care Centres (UCCs).
Descriptions of these services can be found in annex 3.
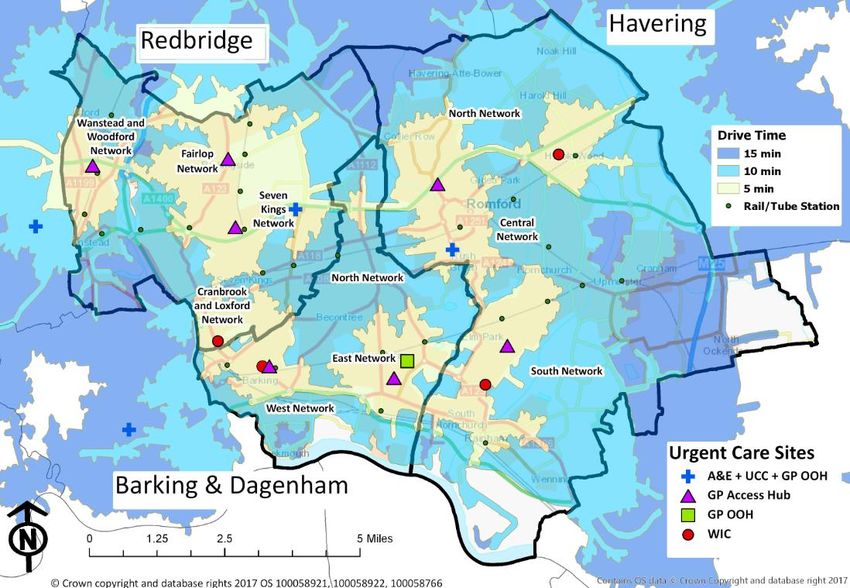
Service location map
The map below shows the locations of our urgent and emergency care services.
Urgent and emergency care service usage
Over the last few years A&E activity has consistently increased. Our latest analysis shows this is
generally in line with population growth. However, most of the increase in A&E activity has
occurred during the 'in hours’ period (8am and 6pm), which creates a bottle neck and pressure
points, resulting in poor A&E performance and an emergency team which is unable to cope with
so many people turning up over a short timeframe.
In the same piece of analysis, activity ‘in hours’ at community urgent care services has not
increased, which, when compared to population growth and the increase seen at the A&E and
UCC, means the community urgent care services are being used relatively less. This is in line
with messages from the public during our engagement work: that some people use A&E because
5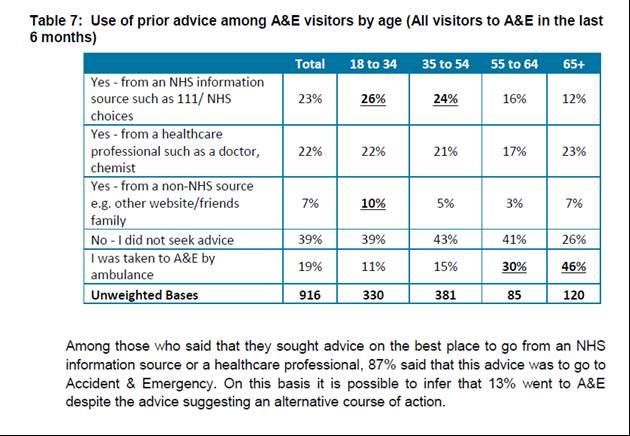
it is seen as a reliable 24/7 service where their issue will be resolved, even if they have to wait for
hours, and that the rest of the community urgent care being offered is too confusing.
Over the next 15 years, the population of Barking and Dagenham, Havering and Redbridge is
expected to grow by 143,000 extra people, with population growth expected to follow the large-
scale housing developments planned in Ilford, Barking town centres, Romford, Rainham, Beam
Park and Barking Riverside. That’s a 19% increase, and equivalent to the size of Basildon.
If the trends described above continue in line with this enhanced level of population growth and
within the context of our financial position, this would create a completely unsustainable model of
care unless we change the service offered in order to manage this.
Doing nothing would not support our A&E departments, and inevitably lead to an unsustainable
model of care for our population.
A&E activity has grown by 2.54% since April 2016 as seen in the figure below. This is above
population growth for the same period by 1.15%. It should be noted that, from September 2017,
A&E activity has been in line with plan.
Primary care
Across BHR there are 124 General Practices:
44 practices in Redbridge
44 practices in Havering
36 Practices in Barking and Dagenham
Practices should be open for bookable appointments between 8am - 6.30pm Monday to Friday;
although across BHR there is still is some variation in practice e.g. a small number of practices
don’t open until 8.30am and some practices still operate with half day closures once a week.
Significant progress has been made in improving access to General Practice over the last few
years. However in our 2016 research survey, 33% of those surveyed in A&E said they had been
unable to get a timely appointment with their GP. Local GPs and stakeholders tell us that the
current model in primary care is unsustainable. The primary care workload is increasing, and will
do further with the ageing population, meaning practices can find it difficult to deliver the quality of
care their patients need.
6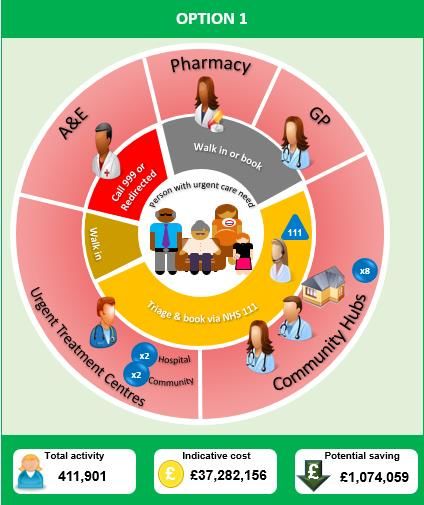
Our workforce is stretched, with recruitment and retention of staff challenging. To put this in
context BHR has some of the lowest rates of GPs per 1,000 population in London, with 0.44-0.47
GPs for every 1,000 registered patients compared to a London average of 0.55. The Practice
Nursing picture is slightly better with 0.14-0.22 Nurses per 1,000 population compared to a
London average of 0.2. Traditionally, outer London has found it harder to attract newly qualified
GPs than inner London. It is difficult both to recruit and retain salaried GPs and to attract GP
partners in BHR, as well as other members of the primary care workforce.
Patient behaviour also contributes to the increasing GP workload. Some patients still feel they
need to see their GP for minor illnesses such as coughs and colds when another professional
such as a community pharmacist could provide that care. Other people seek an appointment with
their own GP, as well as seeking contact with professionals in urgent care - in our engagement
survey 37% of people reported they had seen their GP with the same issue before attending
A&E. Sometimes this is because their symptoms worsen, but it can also be due to initially
attending an urgent care setting which could not meet their needs, to ‘check’ their treatment is
correct, for further reassurance, or to seek a prescription to ‘cure’ the illness e.g. antibiotics or
paracetamol. As we reported in our case for change, a Barking and Dagenham (B&D) GP
practice audited attendances outside of the practice for 1 week. The greatest number of patients
attending different services on the same day had a final outcome of having been prescribed
antibiotics. GPs anecdotally report patients seeking antibiotics outside of the practice as a clinical
concern and a driver of duplication.
In March 2018 BHR CCGs carried out a survey of GP practices to better understand the primary
care role in the wider current urgent care patient pathway. Practices were asked to complete a
short questionnaire to provide some of the primary care context. 46 practices responded to the
survey - a 38% response rate. The results of this survey demonstrate the key role that primary
care play in the delivery of urgent care.
Highlights from responding practices include:
100% of practices provide access to same day appointments
45% practices triage their same day appointments and this may be undertaken by anyone
in the practice from a GP 48% to receptionists 43%
70% of practices undertake injury management - examples of this were:
Road
Road
traffic
accident
traffic
accident
83% reported in the survey that their voicemail refers patients via NHS 111 to the GP out
of hours service when the practice is closed for the day, 17% did not respond to this
question
85% practices advertise the access hubs - using a range of methods such as text
messaging, posters/leaflets, Jayex boards/TV screens, standard letters and on the
practice website
7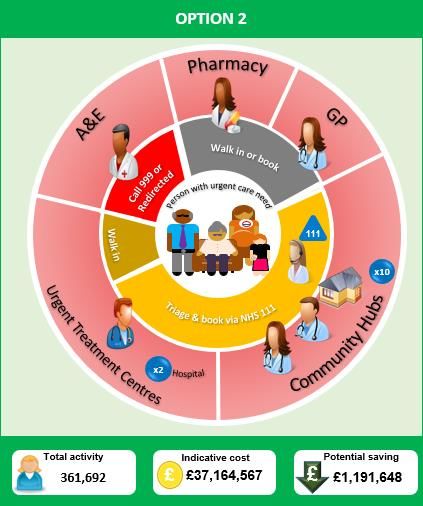
Wound care
The CCGs are in the process of reviewing wound care – the review scope includes
Lymphedema, complex wound care and simple wound care. It is likely that these three service
will be improved through three separate projects. The simple wound care service is currently
delivered by a range of providers across BHR including individual GP practices via a local
incentive scheme to a borough wide contract in Havering with the Hurley group, who also provide
the walk in centres (WIC) for the borough. During spring/summer 2018 the CCGs will undertake
patient engagement on the simple wound care and the feedback will be used to inform future
provision. Given this review is in place, the modelling for the community urgent care review has
removed all wound care activity from the baselines as it will be re-provided as part of this project.
National context
NHS England’s Next Steps on the NHS Five Year Forward View (5YFV) explains how the 5YFV’s
goals will be implemented over the next two years. Urgent and Emergency Care (UEC) is one of
the NHS’s main national service improvement priorities, focussing on improving national A&E
performance whilst making access to services clearer for patients.
As part of the NHS Five Year Forward View and subsequent updates, including the Urgent and
Emergency Care Review, NHS England (NHSE) have introduced a new set of key deliverables
for urgent and emergency care in 2017/18 and 2018/19 which includes:
Achievement of the ‘4 hour target’
Comprehensive front-door clinical streaming
Specialist mental health care in accident and emergency departments (A&E)
Integrated urgent care (IUC) - an enhanced NHS 111 service which means more people
will speak to a clinician and receive a booked appointment where appropriate
An enhanced primary care offer which will deliver a bookable general practice service
from 8am - 8pm seven days a week
Standardise non-acute services - including urgent care centres (UCCs), minor injury units
(MIU) and urgent treatment centres (UTCs).
This business case sets out the CCGs proposals for standardising non-acute services, including
upgrading UCCs and walk in centres to Urgent Treatment Centres or a bookable service.
Developing an Integrated Urgent Care (IUC) system
The review of community urgent care services is one of the programmes that is being taken
forward to develop an integrated urgent care system.
Integrated Urgent Care (IUC) - A better NHS 111 - providing clinical advice, triage and booking.
NHS England see NHS 111 as a key part of providing patients with integrated urgent care, which
is how they describe the way different services will link up to help people in need of urgent same-
day care and advice.
There are some aspects to the current NHS 111 service which would be promoted as part of the
model as they underpin the proposed changes:
Clinical advice service (or CAS) - allows NHS 111 health advisors to fast-track transfer
children aged under 1 and people aged 65 and older to a GP or other health professional
for advice and assessment.
Bookability - for those who do need to come into one of our services, our local NHS 111
service can already book appointments at some of our existing community urgent care
services, and we plan to add more, meaning just one call to NHS 111 would be the only
action required to access urgent care.
Interpretation services - NHS 111 is supported by two interpretation services:
8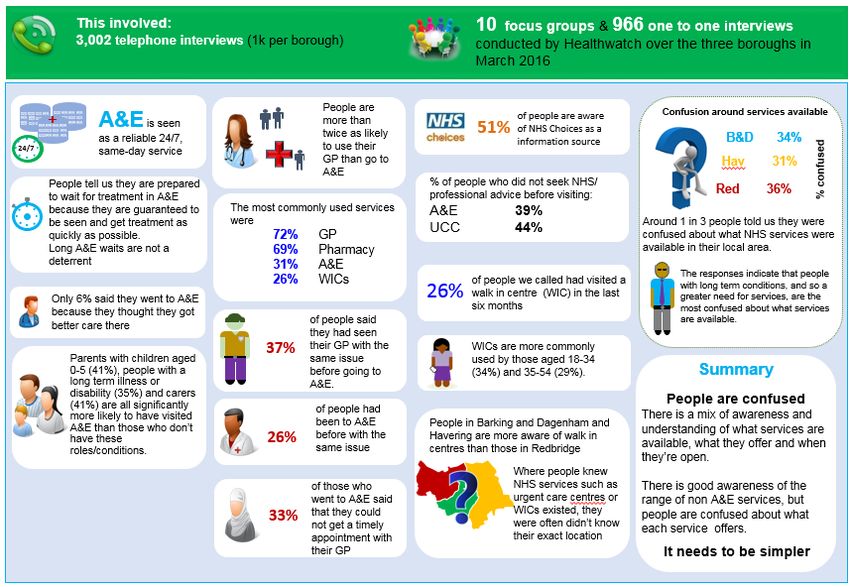
Languages - there is a confidential interpreter service available in many
languages. The caller needs to simply mention the language they wish to use
when the NHS 111 operator answers the call line. NHS 111 patient information
leaflets are available at NHS choices in several languages.
British sign language (BSL) - NHS 111 offers a video relay service that enables a
video call to a British Sign Language (BSL) interpreter. The BSL interpreter will call
NHS 111 to enable a real-time conversation with the NHS 111 adviser via the
interpreter. This requires a webcam, a modern computer and a good broadband
connection to use this service. Visit NHS 111 BSL interpreter service for more
details, including an online user guide. http://interpreternow.co.uk/nhs111
Out of hours - available 6.30pm - 8am weekdays and all weekend when most core
services are closed:
Dental (Smile service) - NHS 111 can be used to access the dental service who can:
Assess the dental issue or problem
Make referrals to an Out of Hours Dental service
Look up urgent care services that provide dental treatment
Offer self-care advice.
Prescriptions out of hours (PURM) - if a repeat prescription is required, for items
that have previously been prescribed via an NHS prescription, NHS 111 can be used
to access a pharmacy service who can:
Assess symptoms and provide clinical advice
Refer to a pharmacy that provides access to urgent medicines for
assessment and potentially the supply of medicines.
The CCGs are already making improvements to our local NHS 111 service so it provides more
than just advice and signposting to services now and in the future. We have introduced a Clinical
Advice Service (or CAS) which allows NHS 111 health advisors to fast-track transfer children
aged under 1 and people aged 65 and older to a GP or other health professional for advice and
assessment. As a result of this pilot, currently over 50% of people now speak to a clinician on the
phone after calling NHS 111.
In future, people may also be booked into an appointment with their own GP, and this is being
tested in other parts of the country now. An online version of NHS 111 and a digital app are also
being tested in other parts of London.
Urgent treatment centres (UTCs)
The case for change for community urgent care services, which was agreed at July 2017
Governing Bodies meeting, reflects feedback from the public, both at a local and national level,
that there is a confusing mix of urgent care services that they find difficulty in navigating:
From the outset of our review of urgent treatment services in the NHS, our patients and the public
told us of the confusing mix of walk-in centres, minor injuries units and urgent care centres, in
addition to numerous GP health centres and surgeries offering varied levels of core and extended
service. Within and between these services, there is a confusing variation in opening times, in the
types of staff present and what diagnostics may be available.
Source: core principles and standards for UTCs https://www.england.nhs.uk/wp-content/uploads/2017/07/urgent-
treatment-centres%E2%80%93principles-standards.pdf
NHSE have published a core set of standards and principles for urgent treatment centres (UTC)
to establish as much commonality as possible across services, and offer a consistent route to
access urgent appointments offered within 4 hours and those booked through NHS 111,
ambulance services and general practice. NHS England expects us to have UTCs in place by
December 2019, if not sooner.
The core principles for UTCs include:
9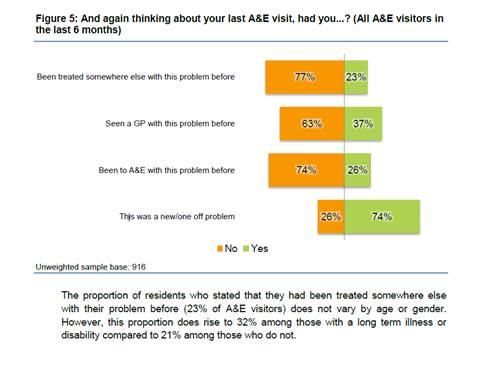
a) Having access to urgent treatment centres that are open at least 12 hours a day, GP-
led, staffed by GPs, nurses and other clinicians, with access to simple diagnostics, e.g.
urinalysis, echocardiogram (ECG) and in some cases simple x-rays.
b) Have a consistent route to access urgent appointments offered within 4 hours and
booked through NHS 111, ambulance services and general practice. A walk-in access
option will also be retained.
c) Increasingly be able to access routine and same-day appointments and out-of-hours
general practice for both urgent and routine appointments, at the same facility and where
geographically appropriate.
d) Know that the urgent treatment centre is part of locally integrated urgent and
emergency care services working in conjunction with the ambulance service, NHS 111,
local GPs, hospital A&E services and other local providers.
NHS England expect commissioners to have UTCs in place by December 2019 or sooner.
We have looked at our existing walk in services and compared them to the UTC national
standard:
South Hornchurch Walk-in service is only open for 6 hours a day and significant
investment would be required to open this site for 12 hours a day, every day of the year
and make the other improvements needed to meet the standard.
Most people who use Loxford Polyclinic already book appointments rather than walk in.
Fewer people use Loxford compared to the numbers seen at the other walk-in services in
our area, and significant investment would be required to meet the UTC standard.
Based on the existing provision of diagnostics, it may be possible for Harold Wood
Polyclinic and Barking Community Hospital to become UTCs, and this is included within
one of the options.
UTCs will help reduce the pressure on our busy A&E departments, releasing capacity to treat
those people requiring immediate emergency care when life or long term health is at risk.
Audits have demonstrated that people are attending, and being seen in, A&E for conditions that
can be managed in an urgent treatment centre or in the community. We are currently working
with providers in the system to strengthen the streaming in the urgent treatment centres and
ensure that we maximise the attendances that can appropriately be seen in this setting. This will
reduce the number of patients seen in A&E and ensure that our performance is improved. This
activity shift is closely linked to the community urgent care review but not formally part of the
scope of this work.
Financial context
Nationally, the NHS is facing a challenging time as demand for services is growing - an
increasing and ageing population coupled with more people living with long term health
conditions, such as diabetes - placing further pressure on already stretched services and
finances.
The CCGs faced specific challenges to our budgets for 2017/18, and we reached a point where
we did not have enough money to continue buying all the services in the way we had done
previously. To achieve financial balance during the year we needed to address a financial
shortfall of £55m, which is just over 5% of our total annual joint budget of just over £1 billion. The
CCGs delivered £32.2 million in savings in 2017/18 (against a £55 million savings target).
2018/19 will be just as tough as we’re currently aiming to deliver £45 million savings to achieve
financial balance.
To achieve financial balance this year we have, therefore, had to maintain very close focus on
where we are using our funds, reducing spending in some areas of our health budget to ensure
we are making the most effective use of every penny that goes into our local NHS, all while
making sure local people can access the healthcare which is most needed and that people with
equal need have equal opportunity to access treatments.
10The CCGs have set up specific groups of key clinical and senior staff to ensure that our focus is
maintained on making the most effective and efficient use of the CCGs’ resources and securing
the required budgetary savings.
We are not alone in needing to carry out major reviews of where money is spent. CCGs all over
the country are now looking at how they can use limited resources responsibly to make sure the
NHS in their areas is able to focus on those most in need, whilst remaining in financial balance.
The CCGs remain totally committed to ensuring that we are commissioning the best health
services we can for local patients and residents within the money we are allocated, and will
continue to work with patients and stakeholders on the difficult decisions we need to take to
achieve this.
We spent £14.3 million on community urgent care in 2017/18. Too many of our existing urgent
care services provide similar care at the same time. It’s confusing for patients, and not the best
use of our limited NHS resources.
112.0 Case for change
What is urgent care?
The CCGs worked with Healthwatch in 2016 to create local definitions to help explain the
difference between urgent and emergency care:
Urgent care is care needed the same day. This could include anything from cuts, minor injuries,
wound infections or tonsillitis, urinary infections, mild fevers, etc.
Urgent care is not emergency care which is provided in a medical emergency when life or long
term health is at risk. For example, this could include serious injuries or blood loss, chest pains,
choking or blacking out.
BHR vision for urgent and emergency care
The BHR vision for urgent and emergency care is:
Health and social care partners across BHR want local people to receive the right care, in the
right place, first time. If they do need to be admitted to hospital, we will get them home safely and
quickly, with the right support to help them to recover their independence. No time will be wasted.
Our ambition is to radically transform local urgent and emergency care services, removing
barriers between health and social care, and between organisations.
Variation in existing community urgent care services
• There are a number of variations across our community urgent care services, including
inconsistencies in:
access routes
service names / branding
opening times
diagnostic provision
skill mix
digital integration
• This complexity and variation within the system leads to:
duplicate attendances for the same health need
poor patient experience
multiple transfers of care
wasted time and resources for both patients and staff
poor value for money
all of the above ultimately leading to a likelihood of poorer clinical outcomes
Some of the evidence for duplicate attendances and patients not being seen in the most
appropriate place first time is given below. The forms of variation across urgent and emergency
care services are described in more detail in the case for change (annex 1) with more detail
within annex 2.
Duplicate attendances
We know that some NHS capacity is wasted due to duplicate or repeat attendances for the same
health need.
Some of this is caused by the variation in services, which can mean people’s first choice service
cannot meet their health needs due to the different staff types, diagnostics or technology in place.
12However some of this is also driven by patient behaviour and the perceived need to seek a
second opinion.
Our IT systems are unconnected which means we cannot quantify the full extent of duplication
that exists. However, where we can compare datasets (approx. 50% of urgent care attendances),
the level of duplicate attendances was just over 5%, with most of these within 24 hours of the first
attendance at 3.3%.
The highest number of attendances was one person attending 6 services within 72 hours.
Clinical audits have demonstrated a higher rate of duplication. In a clinical audit of 300 WIC
attendance records, the following examples of duplication were observed:
• 23% of cases would have been better seen by their own GP as the WIC could not
manage their need.
• 17% could have been managed by a pharmacist (conjunctivitis/ simple pains /
gastroenteritis / ear nose and throat (ENT) symptoms such as ear pain).
• 7% of cases were for a second opinion. This was a combination of patients with chronic
conditions seeking second opinion or those seeking help after trying a new medication
only for a few days.
• 10% of cases were referred onto the emergency department (ED) (deep vein
thrombosis (DVT) / some fractures / chest pains).
• 44% of cases were appropriate and fully managed at the WIC.
This means 40% of these cases were potentially duplicated appointments where ED, primary
care or other urgent care services and a further 17% could have been managed by pharmacy.
In our engagement work people reported attending multiple times for the same need.
Of those attending A&E:
• 39% sought no advice before attending A&E.
• 37% had seen their GP with the same issue.
• 26% had been to A&E before with same issue.
Parents reported a slightly different profile:
• 37% of parents who attended A&E had seen a GP previously for the same issue.
• 25% had previously been to A&E with the same issue.
The following diagram shows
excerpts from the BMG
telephone survey:
13The following picture shows 45% of people sought advice before going to A&E from various
sources including NHS 111, a GP or a pharmacist. This indicates multiple attendances for the
same need. Although the survey was not able to analyse whether they were correctly advised to
go to A&E, 87% said that the advice they were given was to go to Accident & Emergency. It is
possible to infer from this that the other 13% went to A&E despite the advice suggesting an
alternative course of action.
A much lower percentage of people sought advice before going to a hub or WIC (31% for a hub,
34% for a WIC) compared with A&E and UCCs (60%). This could be down to the confidence in
or awareness of these services by those giving advice.
The re-direction trial at Queen’s hospital demonstrated up to 30% of A&E presentations do not
require a same day urgent care service.
Do nothing
The CCGs cannot leave the system as it is currently. Doing nothing is not an option for the
following reasons:
Local people have told us it’s too complicated and we want to provide services that are
easier to access and use.
To do nothing is unaffordable. All urgent and emergency care service models illustrate
that doing nothing would cost us £2.57m per year above our current spend of £35.77m.
If we do nothing then the profile of increasing demand and high levels of duplication
seen at all of our urgent care service and in our A&E departments will continue.
Ultimately, doing nothing will not help us resolve the challenges in our urgent and emergency
care system and will not ease the pressure on our emergency department, leading to an un-
sustainable model of care for our population. We need to deliver a simpler, cost-effective system
that meets our future needs.
14Drive time analysis for ‘do nothing’:
The CCGs believe that the case for change is strong based on the results of our engagement
exercise, financial and activity analysis, the need to strengthen urgent care services to reduce
pressure on our hospital sites and the need to develop a sustainable integrated urgent care
service going forward that builds on national and local developments.
153.0 Engagement to date - urgent care co-design and research
Over the last two years we have undertaken several engagement exercises with stakeholders
and patient representatives to gather views on how we can transform urgent care services.
This includes the Barking and Dagenham, Havering and Redbridge (BHR) urgent care
conference held on 1 July 2015 and engagement with the CCG patient engagement forums, a
comprehensive UEC co-design research survey which included many patient events.
We have talked extensively to local residents to find out their views on local community urgent
care services. Our research study involved more than 4,000 people and included a telephone
survey, 10 focus groups and 2 workshops.
Residents told us that the wide range of services available is confusing and means they don’t
know which service to choose. Even finding the right service is complicated, with different
numbers, different opening hours and a mix of walk-in services or pre-bookable appointments to
choose from. People said they can’t always get a same-day appointment with their own GP, so
some will head to A&E instead of using an alternative, more appropriate service. Some people
say the long waits do not deter them as they think of A&E as reliable service.
The info graphic below outlines the key messages from the 2016 urgent care research:
The clear message from all of this engagement is that all stakeholder groups view urgent care as
complex and confusing and endorse the need to look at simplifying the pathway.
This year, the Healthwatch organisations in all three of our boroughs worked with us to talk with
local people about some of our emerging ideas. They spoke with more than 500 people - a mix of
parents, young adults (15-24) and older people aged 65 and over as these groups are our
biggest users of urgent care services.
16A report on the findings is available on our websites alongside the other documents supporting
this consultation.
While most people can confidently describe the difference between ‘urgent care’ and ‘emergency
care’, it’s clear more needs to be done to help people feel confident to make the right choices for
their urgent health needs. Simplifying the system and providing better support and advice through
NHS 111, as well from your local pharmacist, will help patients.
While patients would prefer to see their own GP, there is support for more appointments within
the local community (at a GP hub or bookable service) when your own GP is not available.
There’s also good recognition of the role of pharmacies in providing expert advice for minor
illnesses.
People welcomed news of the improvements to NHS 111 and felt this would make it easier to get
health advice quickly, to book an urgent appointment and would reduce the number of people
who go to A&E when they have a minor illness or minor injury. But people told us we need to do
more to raise awareness what NHS 111 can now help with.
Learning from our engagement
Services are confusing and vary across our three boroughs. People have told us they want it to
be simpler to get the urgent care or advice they need quickly and in a timely way.
We know that the mix of services is confusing, both for patients and many professionals too. This
can mean people aren’t seen in the most appropriate place first time. That can be frustrating as it
means extra travel, longer waits and delays in getting the help required.
Also, services are not consistent across different A&E departments. Some patients might have a
telephone assessment before they see or speak to a doctor or nurse; others are booked in for a
detailed assessment; and then some people can just walk into others, regardless of the level of
urgent care need.
This isn’t fair, and so we want to make sure that all services prioritise those in most need in a
consistent way.
174.0 Options development and selection
The options appraisal process was completed in 3 stages and overseen by a programme board,
with membership including a lay member, an independent clinical lead, public health, primary
care, finance, communications and engagement and estates.
1. Scenario generation - to generate our scenarios we looked at all the information that was
available to us including:
Patient feedback including our huge research study and engagement programme
National requirements and regional studies and examples, including guidance on making
it easier for local people to get help in the right place, first time
Data and analysis on our services and how they are used
Population growth estimates for the next 3 years.
Using this information, we modelled different scenarios and tested them against our priority
themes.
2. Scenario appraisal - the scenarios were appraised in two stages:
a) The ‘affordability test’ - the CCG finance team completed a financial evaluation of the
modelling of each scenario. Only scenarios that are estimated within the ‘do nothing’
forecast value are scored against the non-financial criteria.
b) Non-financial criteria scoring process where a scenario scoring panel, consisting of
Programme Board members and joined by an additional Lay Member (Audit Chair), the
Quality Manager and Contract Manager from the Commissioning Support Unit, was formed
to score the scenarios which passed the affordability test.
The scenario scoring panel evaluated each scenario against the following criteria:
Patient experience
Clinical quality
Deliverability
Efficiency.
3. Option selection - When setting the scenario shortlisting process, the programme board
agreed that the top 4 scoring scenarios with a minimum score of five would be recommended
for consultation. However, when reviewing the final scores, the programme board and
financial recovery programme delivery meeting (FRPDM) agreed to recommend to financial
recovery programme board (FRPB) and Governing Bodies (GB) that only the top two highest
scoring scenarios would be recommended as options for consultation on the basis that no
18additional benefits to either the public or CCGs could be identified for the scenarios which
scored in third, fourth or fifth place. ‘Do nothing’ scored 3.30 and was excluded on this basis.
195.0 Context for our options
Both of our options enhance current services in line with the standards set out in the
government’s NHS Five Year Forward View plan which we are required to implement.
In response to the need to simplify the pathway, our options have just two points of access and a
common name for services:
Bookable services accessed through NHS 111
Urgent Treatment Centres (UTCs).
Click or call before you come in - bookability
When developing the scenarios we have considered how we could help to address the critical
issue of confusion, and how we can help people access the right care, right place, first time.
Call or click before you come in was an idea first developed in 2015 during our time as a
vanguard site. As this model was supported by stakeholders and local people and is used
nationally, we have continued to build on this when developing our models.
Both options also include a move towards booked appointments for urgent care needs, building
on click or call before you come in. Both of our options will utilise NHS 111 as a way for us to
help people get the right care, right place, first time. The message to our population would be to
click or call before you come in, resulting in shorter times spent in our waiting rooms and fewer
handoffs. People who come in for a booked appointment following click or call would be seen at
their appointment time, rather than the current commitment to see people within 4 hours of arrival
at our urgent and emergency services.
‘Click’ or ‘Call’ before you ‘Come in’
‘Click’ - NHS111 online to provide support and information. This will help people to self-
care and book urgent appointments when needed. NHS 111 on-line is being tested
elsewhere now, and there are other systems being tested across the country.
‘Call’ - NHS 111 telephone line for those who need more advice and reassurance or to
book an appointment to come in if this is required.
‘Come in’ - Urgent Treatment Centres (UTCs) where patients who need to come in can
access urgent care.
Consistent elements which will exist regardless of this proposed service change
Integrated Urgent Care - ‘the smart call to make’, providing clinical advice, triage and booking.
There are some key aspects to the current NHS 111 service which would be promoted as part of
the model:
Clinical advice service (or CAS) - for those who will benefit from telephone advice
Bookability - for those who do need to come into one of our services, NHS 111 will book
an appointment at one of our community urgent care services
Interpretation services
Out-of-hours dental and prescription services (6.30pm - 8am).
Urgent Treatment Centres (UTCs)
Both urgent care centres at King George and Queens Hospitals will be upgraded to the new
national UTC specification. The main difference between our current UCCs and the UTC
specification is that the centres would have:
access to simple diagnostics
bookable services via NHS 111
These enhancements are being addressed as part of this year’s winter plan.
20UTCs will have access to simple diagnostics, such as blood tests and simple x-rays, as well as
treatment for ailments like wound closure and management of minor head and eye injuries. Staff
will also be able to issue e-prescriptions and repeat prescriptions.
The CCGs are proposing two options for public consultation. We know that both options will
mean we need to plan how we tell people about the changes and about how they can get help
and care in the future so that they understand and feel confident when we are ready to make the
changes. We believe each option would mean we could deliver improved care for local people in
the future and meet our ambitions for the community urgent care.
21Options for public consultation
Option 1 - would see 12 sites in total – with
four Urgent Treatment Centres open within
Barking and Dagenham, Havering and
Redbridge (2 on hospital sites, and 2 in the
community), plus eight locations for booked
community urgent care services.
Our existing Urgent Care Centres at King
George and Queen’s Hospitals will be
upgraded and become Urgent Treatment
Centres in line with national policy. These will
see patients who walk in or who are booked
into a timed appointment by NHS 111.
As well as the two existing Urgent Care
Centres, people could also continue to walk
into Barking Community Hospital and Harold
Wood Polyclinic, and facilities at these
locations would be upgraded to become
community Urgent Treatment Centres.
This would mean there would be four
locations (including the hospital UTCs) in
Barking and Dagenham, Havering and Redbridge where you can walk in and be seen as well as book an
appointment by calling NHS 111.
There will also be eight community urgent care services across the area where you can be booked in
following a call to NHS 111. You will be seen within a maximum of 30 minutes of your appointment time.
All sites (including UTCs) would have bookable appointments through NHS 111.
Financial modelling results conclude that this option would save £1.07 million a year.
Option 1 - map of
services and drive time
analysis for services
within the BHR
geography:
22Option 2 would mean 12 sites in total –
with two UTCs within our area on the
hospital sites (although local people may
still use those in our neighbouring
boroughs Newham and Whipps Cross).
Plus there will be 10 more places to be
booked when your own GP practice is
closed and you have an urgent health
need.
Under option 2, the Urgent Treatment
Centres at King George and Queen’s
Hospitals would be the only places you
could walk in without making a call first or
getting an appointment.
By calling NHS 111, you would be booked
a timed appointment at 10 community
urgent care service locations across
Barking and Dagenham, Havering and
Redbridge. These would include Harold
Wood Polyclinic, South Hornchurch Health
Centre, Loxford Polyclinic and Barking
Community Hospital.
All sites would have bookable
appointments through NHS 111.
Financial modelling results suggests that this option would save £1.19 million a year - £117,589 a year
more than Option 1.
Option 2 - map
of services and
drive time
analysis for
services within
the BHR
geography:
23Option comparison
Option 1 Option 2
Service provision Twelve sites in total: Twelve sites in total:
Four UTCs (walk in and bookable access) Two UTCS (walk in and bookable access)
Bookable appointments via NHS 111 at 8 locations Bookable appointments via NHS 111 at 10 community urgent care
for booked community urgent care services service locations across Barking and Dagenham, Havering and
Redbridge. These would include Harold Wood Polyclinic, South
Hornchurch Health Centre, Loxford Polyclinic and Barking
Community Hospital.
Scenario scoring panel Quality score Quality score
scores
Total score
Total score
Deliverability
Deliverability
£ score
£ score
experience
experience
Efficiency
Efficiency
Clinical
Clinical
Patient
Patient
1.80 1.50 1.32 1.40 1.34 7.36 2.00 1.18 1.30 1.14 1.38 7.00
Benefits Managing the 4 hour A&E wait - greater capacity for Greater savings - the modelling estimates that this scenario saves
diagnostics to support minor injury management away £117,589 more than option 1.
from the main hospital sites and closer to home.
70% bookable capacity – this both allows for the
management of injuries as walk-in whilst reflecting a
sensitivity analysis of people’s compliance with the click/
call/ come in message.
Risks Patient behaviour does not follow the modelling Patient behaviour does not follow the modelling assumptions - i.e. where
assumptions - i.e. where WICs become bookable services WICs become bookable services (Harold Wood Polyclinic, South
(Loxford and South Hornchurch) that 70% of patients will Hornchurch Health Centre, Loxford Polyclinic and Barking Community
book appointments Hospital) that 100% of patients will book appointments.
There is no UTC facility in B&D.
24What the future will look like
We want to make it easier for local people to access help for urgent health needs. We want
people to click or call before they come in, and to trust the advice they receive about what to do
or where to go when they have an injury or illness.
We know that both options will mean we need to plan how we tell people about the changes so
that they understand and feel confident about where to go for help when we are ready to make
the changes.
In general we will not be closing existing services, but will be changing the way services are
accessed from the existing locations. The only exception is Grays Court in Dagenham as the
Council own this building and have alternative plans for its use in the future (subject to
confirmation from London borough of Barking & Dagenham).
We will enhance our existing Urgent Care Centres to meet the new national Urgent Treatment
Centres specification, and offer more pre-booked appointments with GPs and nurses in
community locations away from hospital sites.
Both of these changes will help to reduce the pressure on our busy A&E departments, and will
reduce waiting times for patients.
Local services will be designed to meet the growing and changing population of our three
boroughs, but we will make sure we get better value for money from local NHS services by
removing duplication and helping residents receive the right care in the right place, first time.
In the future, people will receive a more consistent quality assessment of their health needs
before they see a clinician, whether it’s by NHS 111 or as they walk into any of our UTCs. This
will help to address the issues of perceived vs urgent care need and help people get the right
care in the right place, first time, with those with the most serious needs seen as a priority - not
on the basis of who called or turned up first.
We’ll continue to build on improvements to NHS 111 and to the way that different services and
organisations link up to share information including electronic health records. This will improve
the quality of the care patients receive and tackle the challenge of those who visit several
services for the same issue. National tools such as the summary care record will be used.
A digital future for healthcare
Advances in digital technology are already making it easier to get health advice and services
online. Across London, doctors and patients are talking via Skype and we’ve seen the launch of
the ‘GP at Hand’ virtual NHS service. In our own area, GPs from NHS 111 are using video
consultations with care homes when a resident is unwell so staff can care for them safely in the
home and avoid an often unnecessary journey by ambulance to A&E.
Both of our options will allow patients to access urgent care on-line, which will include access to
clinical advice and the ability to book an appointment at the right place for their needs for those
who need it.
In future, it will be easier and quicker to get help from a health professional without needing to go
into a busy health centre and see someone. Many people won’t even need to leave their home,
as they’ll get advice through their phone, smartphone, tablet or PC.
People won’t waste time sitting in a waiting room, and if they do need to see someone they will
be booked an appointment at the right place for their needs. Appointments will fit around an
25individual’s life and responsibilities, such as work, collecting children from school or other caring
responsibilities.
We will make sure services and organisations link up to share information including electronic
health records. This will improve the quality of care patients receive.
We think moving away from walk-in services will make it easier for local people to get help with
urgent health needs. We will make it easier to call (and, in future, click), get clinical advice from
home and be guided to the right place for the care needed.
266.0 Proposed consultation process
Engagement plan for the next stage
The CCGs will be seeking views through online surveys or at events that we attend, and we will
ensure personal information is kept secure and confidential and will only be used to help us
analyse the feedback we receive.
When the consultation closes, we will read and consider all the responses we receive.
We will use feedback to write a report for the three CCGs’ decision-making Governing Bodies to
consider, alongside any other evidence and/or information available. This includes the equality
impact assessment (EQIA). The Governing Bodies will make a decision about what to do.
Responses on behalf of an organisation or for those who represent the public (as an MP,
Councillor or similar) may be made available for the public to look at. Where an individual
responds in a personal capacity, we will not publish the name or response in full but may instead
use some of what is said to show particular points of view.
For responders who request to be kept up to date and provide contact details when completing
the questionnaire, we will email updates to keep them informed.
Any comments on our proposals must be received by 5pm on 21 August 2018.
Consultation process
We propose the following:
A 12 week, three-borough consultation, running from 29 May to 21 August 2018.
Online consultation in line with previous successful Spending Money Wisely consultations
Consultation to be promoted through social media and other established channels, through
media releases, posters, and advertisements, and via newsletters, stakeholders and existing
forums.
Printed copies of a flyer (written in plain English) promoting the consultation to be widely
circulated throughout the three boroughs
Present at the BHR patient engagement forums (PEF).
Actively engage with Healthwatch and other local stakeholders.
Attend meetings with local stakeholders as requested.
Proactively engage the voluntary and community sector
Key stakeholders identified, with a targeted focus on hard to reach groups, parents of young
children and young adults as high or frequent users of UEC services
27Summary of the key stages of the consultation process and indicative timeline
The timeline for the following stages (e.g. route to contract, market testing, procurement and
mobilisation of the new service) will be developed and released following the consultation
decision making stage.
287.0 Annex 1 - Case for change
Community urgent
care case for change_July 2017.pdf
8.0 Annex 2 - Variation in existing community urgent care services
Access routes - people can access services by calling NHS 111, various call centres or at some
services it is possible to simply walk in.
29Variation in service names / branding – there are many descriptions for our community urgent
care services, despite common services being offered, e.g. treatment of minor ailments or minor
injuries:
Variation and duplication of opening hours
Across all urgent and emergency care services, there is plenty of access available
covering 24 hours a day seven days a week. Variation does exist even within services of
the same type, e.g. for walk in centres:
Loxford: 8am - 8pm
Harold Wood: 8am - 8pm
South Hornchurch: Monday to Fridays 10:00 - 14:00 and 15:00 - 19:00; Saturday
and Sundays 10:00 - 14:00
Barking community hospital: Monday to Fridays 7am-10pm; Saturday and
Sundays 8am - 8pm
UEC services week day opening hours:
30UEC services week opening hours:
Variation in diagnostics – and, again, this even occurs in services with the same
name:
Walk-in centre Loxford: urinalysis
Walk-in centre South Hornchurch: urinalysis, blood glucose
Walk-in centre Harold Wood: urinalysis, blood glucose, phlebotomy, simple
x-ray
Walk-in centre Barking community hospital: urinalysis, phlebotomy, simple
x-ray, ECGs.
31 Skill mix - there is no consistent staffing model in place with a mix of nursing and
medical workforce delivering the service. This can be an issue if people attend a
service and the skill required to deliver their needs are not available there. The
diagram below shows this variation:
D
i
g
Digital integration - we have lots of community urgent care services, but few are
digitally connected. This means medical records or care plans are not always
available. This has a direct impact on patient care as clinical decision-making is
improved where clinical history is available.
Even where the same system is used by multiple services (Adastra) it is not
connected across the system.
329.0 Annex 3 - Current urgent and emergency care services
People in Barking and Dagenham, Havering and Redbridge are able to use a range of different
services when they feel they need medical advice urgently, but when it is not an emergency.
Service location map
The map below shows the locations of our urgent and emergency care services:
Descriptions of current services
Pharmacists
Daily, about 1.6 million people visit a pharmacy in England. There are around 140 community
pharmacies across Barking and Dagenham, Havering and Redbridge, located in high streets,
supermarkets and local shopping centres.
Community pharmacists (or chemists) dispense and check prescriptions and provide advice to
patients on medicines that have been prescribed for them. They can also provide advice on
minor illnesses and staying healthy. You can find out more on the NHS Choices website or by
talking to your local community pharmacist.
General practice
GP practices offer same-day urgent appointments and will continue to do so. These are the best
place for you to be seen, especially if you have an ongoing medical condition or health need.
NHS 111
NHS 111 is the NHS non-emergency telephone number where you can speak to a highly trained
adviser, supported by healthcare professionals. It is available 24 hours a day, 365 days a year.
Calls are free from landlines and mobile phones. There is also a free text-phone service and a
confidential translator service which is available in many languages.
33You can also read