Management of atrial fibrillation in patients with chronic kidney disease in clinical practice: a joint European Heart Rhythm Association (EHRA) ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Europace (2020) 22, 496–505 EHRA SURVEY
doi:10.1093/europace/euz358
Management of atrial fibrillation in patients
with chronic kidney disease in clinical practice:
a joint European Heart Rhythm Association
(EHRA) and European Renal Association/
Downloaded from https://academic.oup.com/europace/article-abstract/22/3/496/5712974 by guest on 19 May 2020
European Dialysis and Transplantation
Association (ERA/EDTA) physician-based
survey
Tatjana S. Potpara 1,2*†, Charles Ferro3†, Gregory Y.H. Lip4, George A. Dan5,
Radoslaw Lenarczyk6, Francesca Mallamaci7, Alberto Ortiz8, Pantelis Sarafidis9,
Robert Ekart10, and Nikolaos Dagres 11
1
School of Medicine, Belgrade University, Visegradska 26, 11000 Belgrade, Serbia; 2Cardiology Clinic, Clinical Centre of Serbia, Belgrade, Serbia; 3Department of Renal Medicine,
University Hospitals Birmingham, Edgbaston, Birmingham, UK; 4Liverpool Centre for Cardiovascular Science, Liverpool Heart & Chest Hospital, University of Liverpool,
Liverpool, UK; 5Medicine University ‘Carol Davila’, Colentina University Hospital, Bucharest, Romania; 6First Department of Cardiology and Angiology, Silesian Centre for Heart
Disease, Curie-Sklodowskiej Str 9, 41-800 Zabrze, Poland; 7CNR-IFC, Clinical Epidemiology and Pathophysiology of Hypertension and Renal Diseases, Ospedali Riuniti, 89124
Reggio Calabria, Italy; 8IIS-Fundacion Jimenez Diaz, School of Medicine, University Autonoma of Madrid, FRIAT and REDINREN, Madrid, Spain; 9Department of Nephrology,
Hippokration Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece; 10Faculty of Medicine, Maribor University, Maribor, Slovenia; and 11Department of
Electrophysiology, Heart Center Leipzig, Leipzig, Germany
Received 4 December 2019; editorial decision 8 December 2019; accepted 13 December 2019; online publish-ahead-of-print 21 January 2020
The European Heart Rhythm Association (EHRA) and European Renal Association/European Dialysis and Transplantation Association
(ERA/EDTA) jointly conducted a physician-based survey to gain insight into the management of atrial fibrillation (AF) in patients with
chronic kidney disease (CKD) and adherence to current European Society of Cardiology AF Guidelines in contemporary clinical practice.
Physician-based survey conducted during an 8-week period using an internet-based questionnaire sent to all EHRA and ERA/EDTA mem-
bers, with voluntary and anonymous responses. Among 306 physicians (160 EHRA and 146 ERA/EDTA members; 56 countries), a multi-
disciplinary team for management of AF-CKD patients was available to only 20/300 respondents (6.7%) and 132/295 (44.7%) routinely
screened CKD patients for AF. Oral anticoagulation (OAC) use was based on individual stroke risk in mild/moderate CKD but on shared
decision-making in advanced CKD. The CHA2DS2-VASc score-based decisions were more common among cardiologists, with substantial
intra- and inter-specialty heterogeneity in the use and dosing of specific OAC drugs across CKD stages, heterogeneous strategies for
OAC monitoring (especially among nephrologists) and a modest impact of CKD on rate and rhythm control treatment decisions. The
HAS-BLED score was generally not a determinant of OAC prescribing. Our survey provided important insights into contemporary man-
agement of AF patients with CKD in clinical practice, revealing certain differences between nephrologists and cardiologists and highlighting
shared and specific knowledge gaps and unmet needs. These findings emphasize the need for streamlining the care for AF patients across
different specialties and may inform development of tailored education interventions.
䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏 䊏
Keywords European Heart Rhythm Association survey • European Renal Association/European Dialysis and Transplantation
Association • Atrial fibrillation • Chronic kidney disease • Dialysis • Oral anticoagulant therapy
* Corresponding author. Tel: þ381 11 361 6319; fax: þ381 11 361 6319. E-mail address: tanjapotpara@gmail.com; tatjana.potpara@med.bg.ac.rs
†
These authors are joint first authors.
Published on behalf of the European Society of Cardiology. All rights reserved. V
C The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.EHRA survey 497
What’s new?
Methods
• This is the first physician-based survey jointly conducted by This physician-based survey was conducted during an 8-week period
European Heart Rhythm Association and European Renal starting from 18 January 2019, using an internet-based questionnaire that
Association/European Dialysis and Transplantation Association was jointly developed by the EHRA Scientific Initiatives Committee (SIC)
to gain insight into the management of atrial fibrillation (AF) in and ERA/EDTA European Renal and Cardiovascular medicine (EURECA-
patients with chronic kidney disease (CKD). m) working group. The link to questionnaire containing 26 single- or
• The survey revealed a suboptimal interdisciplinary collabora- multiple-choice questions (see Supplementary material online) was sent
tion in the management of patients with AF and CKD, low uti- to all EHRA and ERA/EDTA members, and the response was voluntary
and anonymous. The respective members’ responses were collected by
lization of screening for AF, substantial intra- and inter-
the EHRA-SIC and EURECA-m, and then pooled together for analysis.
specialty heterogeneity in the use and dosing of specific oral
anticoagulant (OAC) drugs across CKD stages, heterogeneous
Statistical analysis
Downloaded from https://academic.oup.com/europace/article-abstract/22/3/496/5712974 by guest on 19 May 2020
strategies for monitoring of patients taking OAC, especially
The values are shown as numbers and percentages. In case of missing
among nephrologists, and a modest impact of CKD severity
data for a particular question, the number of available responses is shown
on arrhythmia-directed treatment decisions. as n/N, where N is the total number of respondents. Owing to the obser-
• Our survey provided important insights into contemporary
vational survey design, only descriptive statistical analyses were con-
management of AF patients with CKD, highlighting shared and ducted, and two-sided P-value of 20 years, whereas more EHRA respondents were fellows in
training.
to the CKD-related platelet dysfunction.1,2
The EHRA respondents were more frequently seeing AF patients
Thromboembolic events associated with AF can be effectively pre-
with CKD not on dialysis, whereas ERA/EDTA respondents were
vented using oral anticoagulant therapy (OAC), either a non-vitamin
more commonly seeing patients on renal replacement therapy (i.e.
K antagonist oral anticoagulant (NOAC) or vitamin K antagonists
dialysis or renal transplant), Table 1.
(VKAs).3 However, the risks and benefit of specific therapies or inter-
ventions may be substantially altered in the presence of advanced
Interdisciplinary collaboration in
CKD. For example, the risk of OAC-related bleeding increases with
increasing severity of CKD. Reduced renal function may also facilitate the management of patients with
the occurrence of drug adverse effects, owing to slower drug elimina- atrial fibrillation and chronic
tion resulting in increased plasma levels,2,4 and patients with AF and kidney disease
CKD have increased risk of peri-procedural complications with car- A structured multidisciplinary team for the management of patients
diovascular invasive procedures such as, for example, percutaneous with AF and CKD was available to only 20/300 respondents (6.7%),
coronary intervention or AF catheter ablation.2 but 160 respondents (53.3%) were closely collaborating with physi-
Patients with end-stage CKD are commonly excluded from cians of another specialty (Figure 2A). Overall, 73 respondents
randomized clinical trials (RCTs) of OAC for stroke prevention in (24.3%) stated that a multidisciplinary team was neither available nor
AF, and the high-quality evidence to inform the management of such planned, and this response was significantly more frequent among
patients in daily clinical practice is missing. The European Heart ERA/EDTA respondents (Figure 2A).
Rhythm Association (EHRA) and European Renal Association/
European Dialysis and Transplantation Association (ERA/EDTA) The means of renal function assessment
jointly conducted a physician-based survey with the aim to gain in- in routine practice
sight into the management of AF in patients with CKD and adherence For the purpose of routine assessment of renal function, most EHRA
to current European Society of Cardiology (ESC) Guidelines for AF respondents were using the Cockcroft-Gault equation to estimate
management in contemporary clinical practice. creatinine clearance (CrCl), whereas ERA/EDTA respondents mostly498 T.S. Potpara et al.
Downloaded from https://academic.oup.com/europace/article-abstract/22/3/496/5712974 by guest on 19 May 2020
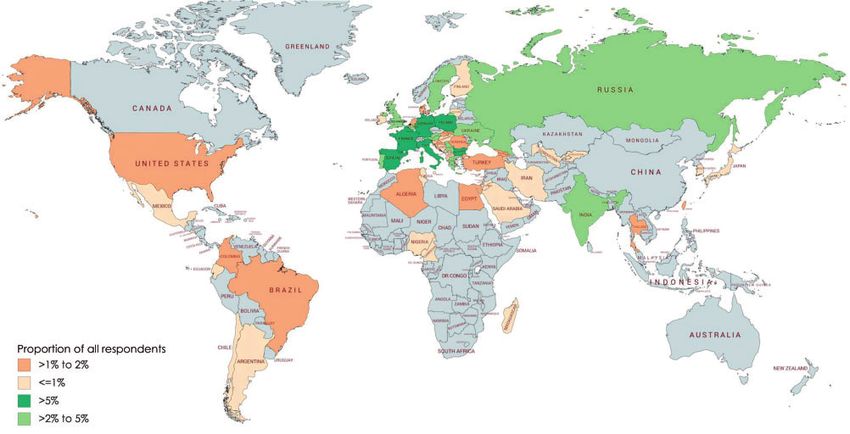
Figure 1 Geographic distribution of respondents to the EHRA-ERA survey on the management of patients with AF and CKD. AF, atrial fibrillation;
CKD, chronic kidney disease; EHRA, European Heart Rhythm Association; EP, electrophysiology; ERA, European Renal Association.
preferred the Chronic Kidney Disease Epidemiology Collaboration Holter-monitoring, an implantable cardiac monitor, or cardiac im-
(CKD-EPI) equation to estimate glomerular filtration rate (eGFR), plantable electronic device memory readings (Figure 3C).
Figure 2B. Similar preferences were observed in the assessment of re-
nal function for OAC-related decision-making (e.g. eligibility for
Stroke prevention strategies in patients
NOACs, dose selection), Figure 2C.
with atrial fibrillation and chronic kidney
Screening for atrial fibrillation among disease
chronic kidney disease patients A small proportion of respondents of both specialties would rou-
Overall, 132/295 respondents (44.7%) would routinely screen for tinely use OAC for the prevention of AF-related stroke in all AF
the presence of AF in all CKD patients at their first presentation, 68/ patients irrespective of estimated individual patient stroke risk and
295 (23.1%) would screen for AF only in selected CKD patients, and CKD severity (Figure 4). Increased individual stroke risk (as estimated
95/295 respondents (32.2%) would not screen for AF among CKD by the CHA2DS2-VASc score value of >_1 in males or >_2 in females)
patients (Figure 3A). Compared with ERA/EDTA respondents, EHRA was the most common threshold for OAC use in AF patients with a
respondents would more frequently screen for AF only in selected CKD of Stage 2 (68.0% of the cardiologist and 27.4% of the nephrolo-
CKD patients (Figure 3A). gists). With increasing severity of CKD, the use of OAC was more
The approaches to screening for AF during follow-up were commonly based on shared informed decision-making than the
broadly similar to those selected for patient’s first presentation stroke risk alone, especially for patients on renal replacement therapy
(Figure 3B). Overall, screening for AF was most likely in patients with (i.e. dialysis), Figure 4, bottom panel. Overall, treatment decision-mak-
symptoms suggestive of a cardiac arrhythmia or those with a history ing regarding OAC use was more often based on the patient’s
of arrhythmias (Figure 3A and B). More ERA/EDTA respondents CHA2DS2-VASc score value among cardiologists compared with
would screen for AF among patients on dialysis or those with a work- nephrologists.
ing kidney transplant compared with EHRA respondents (Figure 3A The risk of bleeding, as estimated by the HAS-BLED score, was
and B). generally not a determinant of OAC prescribing among most physi-
The most common screening techniques were a single 12-lead cians of both specialties, whereas only a few respondents would con-
electrocardiogram (ECG) recording (240/288 respondents, 83.3%) sider using aspirin or left atrial appendage occlusion for stroke
or >_24-h Holter monitoring (181/288, 62.8%), see Figure 3C. The prevention in patients with a HAS-BLED score of >_3.
ERA/EDTA respondents more frequently chose pulse palpation, Regarding AF patients on haemodialysis, 12.2% of the responding
whereas EHRA respondents more frequently opted for a cardiac cardiologists and 4.3% of nephrologists would refrain from treatment
rhythm monitoring strategy using a handheld device, telemetry, decision-making for stroke prevention, and as many as 32.4% ofEHRA survey 499
Table 1 Characteristics of the study population
Parameter All (n 5 306), EHRA (n 5 160), ERA/EDTA P-value
N (%) N (%) (n 5 146), N (%)
....................................................................................................................................................................................................................
Respondents’ affiliation (health care facility type)
Public 98 (32.0) 66 (41.3) 32 (21.9)500 T.S. Potpara et al.
(A) Structured muldisciplinary team 83/160, 77/140, PEHRA survey 501
N = 23/23
(A) Screening for AF among paents with EHRA ERA Selected CKD paents N = 43/45
CKD at their first presentaon With symptoms suggesve of 95.7%
67/137, arrhythmias 95.4%
65/158, 48.9%
41.1% 47/137, On AADs 60.9%
45/158, 48/158, 62.8%
34.3%
28.5% 23/137, 30.4%
Known history of arrhythmias 87.0%
16.8% 83.7%
P = 0.1809 P = 0.017 P = 0.4716 Known history of CV disease 65.2%
39.5%
In all CKD paents In selected CKD paents No roune screen for With a working kidney transplant 21.7%
4.7%
cardiac arrhythmias in CKD
paents On dialysis 69.6%
18.6%
N = 132/295 (44.7%) N = 68/295 (23.1%) N = 95/295 (32.2%)
Downloaded from https://academic.oup.com/europace/article-abstract/22/3/496/5712974 by guest on 19 May 2020
N = 34/34
(B) Screening for AF among paents with CKD Selected CKD paents N = 51/58
during follow-up
With symptoms suggesve of 94.1%
61/158, 54/136, 58/158, 96.1%
47/136, arrhythmias
38.6% 39.7% 36.7% 34.6% 70.6%
34/136, 39/158, On AADs 68.6%
25.0% 24.7%
Known history of arrhythmias 76.5%
86.3%
P = 0.8474 P = 0.031 P = 0.0635 Known history of CV disease 61.8%
54.9%
With a working kidney transplant 17.7%
In all CKD paents In selected CKD paents No roune screen for 2.0%
cardiac arrhythmias in CKD
On dialysis 58.8%
paents 21.6%
N = 115/294 (39.1%) N = 92/294 (31.3%) N = 86/294 (29.3%)
N = 135/146
(C) AF screening modalies N = 153/160
91/135,
67.4% P502 T.S. Potpara et al.
Stage 3 (eGFR 30-59 mL/min/1.73m2) EHRA Stage 3 (eGFR 30-59 mL/min/1.73m2) ERA
SPAF strategies per CKD severity Stage 4 (eGFR 15-29 mL/min/1.73m2) EHRA Stage 4 (eGFR 15-29 mL/min/1.73m2) ERA
68.0%
Stage 5 (eGFR =2f VASc>=2m or >=3f ==3 making
On haemodialysis EHRA On haemodialysis ERA
On peritoneal dialysis EHRA On peritoneal dialysis ERA
53.0%
46.0%
45.3%
37.2%
32.4%
24.8%
18.9%
14.9%
12.2%
11.1%
9.4%
9.4%
7.4%
6.1%
6.1%
5.1%
5.1%
5.1%
5.1%
4.3%
4.3%
4.3%
4.1%
3.4%
3.4%
3.4%
3.4%
2.7%
2.7%
2.6%
1.4%
1.4%
1.4%
1.4%
0.9%
0.7%
OAC rounely in all OAC if CHA2DS2- OAC if CHA2DS2- OAC if HAS-BLED OAC if HAS-BLED OAC if HAS-BLED Preferably shared Other Not applicable
paents with AF VASc>=1m or >=2f VASc>=2m or >=3f ==3 making
Figure 4 Stroke prevention strategies in patients with AF and CKD. AF, atrial fibrillation; CKD, chronic kidney disease; eGFR, estimated glomerular
filtration rate; EHRA, European Heart Rhythm Association; ERA, European Renal Association; f, female; m, male; OAC, oral anticoagulation; SPAF,
stroke prevention in AF.
nephrologists rather opted for various case finding strategies in se- Guidelines (Class I, Level of Evidence B), whereas systematic ECG
lected CKD patients with symptoms or history of arrhythmia), (iii) screening for AF may be considered in patients aged >75 years, or
OAC treatment decisions being driven by individual patient stroke those at high stroke risk (IIb, B).8 Nevertheless, 32% of physicians in
risk and patient’s preferences (i.e. shared decision-making) rather our survey would not routinely screen for AF in CKD patients and
than the estimated risk of bleeding, (iv) substantial intra- and inter- 23% would screen for AF only in CKD patients with symptoms or a
specialty heterogeneity in the use and dosing of specific OAC drugs history of arrhythmia. When screening for AF, nephrologist most
across the CKD stages, (v) heterogeneous strategies for monitoring commonly opted for pulse palpation or a single ECG recording,
of patients taking a NOAC, especially among nephrologists, and (vi) a whereas cardiologists predominantly used a single ECG recording or
modest impact of the presence and severity of CKD on rate and Holter monitoring, likely owing to different availability of heart
rhythm control treatment decisions. rhythm monitoring tools.
Only 6.7% of participants in our survey had a multidisciplinary The use of OAC for stroke prevention in our survey was generally
team available for treatment decisions and management of patients guided by patient’s stroke risk and CKD severity, and not the risk of
with AF and CKD. Although 53% of participants were closely collab- bleeding, in line with all major international AF guidelines.3 The HAS-
orating with another specialty, there was still a significant proportion BLED score was generally not a determinant of OAC prescribing,
of cardiologists and nephrologists (40% overall) not having any struc- consistent with contemporary studies.9,10 Indeed, the HAS-BLED
tured collaboration. A recent EHRA/ESC survey of cardiologists, neu- score was designed to draw attention to modifiable bleeding risk fac-
rologists, and general practitioners or family physicians managing tors and to flag up the ‘high risk’ patients for early follow-up.11
patients with AF in six European countries also showed that >50% of The proportion of physicians who would prefer shared decision-
participants regarded the interdisciplinary collaboration suboptimal.5 making increased with increasing severity of CKD (Figure 4), and
In a recent prospective study, a multidisciplinary pathway in the man- there was a preference towards the use of VKAs and apixaban or
agement of patients with AF was associated with reduced hospital ad- edoxaban (and, to some extent, rivaroxaban) over dabigatran in
mission and length of hospitalization compared with usual care,6 and patients with severe CKD or on dialysis. Similar to an earlier EHRA
integrated multidisciplinary care for AF patients has been associated electrophysiology network centre-based survey conducted in
with significantly reduced all-cause mortality and cardiovascular 2015,12 the thresholds for lower/reduced NOAC doses were highly
hospitalizations.7 variable in the present study, altogether reflecting a persistent knowl-
Opportunistic screening by pulse palpation or electrocardio- edge gap regarding NOAC dosing in patients with mild to moderate
graphic (ECG) rhythm strip is recommended in 2016 ESC AF CKD and lack of high-quality evidence to inform the use of (N)OACEHRA survey 503
134/164 EHRA 109/146 ERA
VKA use in CKD+AF paents 50.7% 49.5%
P = 0.554 P = 0.053 P = 0.411 P = 0.980 P = 0.797 P = 0.914 P = 0.865
14.9% 14.2% 14.7%
8.3% 11.0% 8.2% 7.3%
3.0% 4.6% 6.7% 4.6%
2.2%
Not applicable Never in severe CKD or on Reduced dose only in Reduced dose only if Reduced dose only if Reduced dose only if No CKD-related dose
dialysis dialysis paents eGFR/CrCl504 T.S. Potpara et al.
133/160 EHRA 104/146 ERA
The influence of CKD on the choice of rate or rhythm control
53.4%
34.6% P = 0.556
P = 0.039
P = 0.941 P = 0.117
20.2% 19.6% 16.4% 13.5% P = 0.064
P = 0.007 9.8% 9.0% 8.7% 6.8% 6.7%
1.5%
No impact Rate control is my primary Rate control if eGFR/CrClEHRA survey 505
patients with AF across different specialties and may inform develop- 6. Ptaszek LM, Baugh CW, Lubitz SA, Ruskin JN, Ha G, Forsch M et al. Impact of a
multidisciplinary treatment pathway for atrial fibrillation in the emergency de-
ment of tailored education interventions.
partment on hospital admissions and length of stay: results of a multi-center
study. J Am Heart Assoc 2019;8:e012656.
7. Gallagher C, Elliott AD, Wong CX, Rangnekar G, Middeldorp ME, Mahajan R
Supplementary material et al. Integrated care in atrial fibrillation: a systematic review and meta-analysis.
Heart 2017;103:1947–53.
8. Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B et al. 2016 ESC
Supplementary material is available at Europace online. Guidelines for the management of atrial fibrillation developed in collaboration
with EACTS. Europace 2016;18:1609–78.
Acknowledgements 9. Boriani G, Proietti M, Laroche C, Fauchier L, Marin F, Nabauer M et al.; EORP-
The production of this document is under the responsibility of the AF Long-Term General Registry Investigators. Contemporary stroke prevention
strategies in 11 096 European patients with atrial fibrillation: a report from the
Scientific Initiatives Committee of the European Heart Rhythm EURObservational Research Programme on Atrial Fibrillation (EORP-AF) Long-
Association: Tatjana S. Potpara (Chair), Radoslaw Lenarczyk (Co- Term General Registry. Europace 2018;20:747–57.
Downloaded from https://academic.oup.com/europace/article-abstract/22/3/496/5712974 by guest on 19 May 2020
Chair), Giulio Conte, Gheorghe Andrei Dan, Michal M. Farkowski, 10. Potpara TS, Dan GA, Trendafilova E, Goda A, Kusljugic Z, Manola S et al.;
BALKAN-AF Investigators. Stroke prevention in atrial fibrillation and ‘real world’
Malcolm Finlay, Estelle Gandjbakhch, Konstantinos E. Iliodromitis, adherence to guidelines in the Balkan Region: the BALKAN-AF Survey. Sci Rep
Kristine Jubele, Deirdre A. Lane, Eloi Marijon, Francisco Marin, Frits 2016;6:20432.
Prinzen, and Daniel Scherr. This work was also planned as part of 11. Lip GYH, Banerjee A, Boriani G, Chiang CE, Fargo R, Freedman B et al.
Antithrombotic therapy for atrial fibrillation: CHEST Guideline and Expert Panel
the activity of the European Renal and Cardiovascular Medicine Report. Chest 2018;154:1121–201.
(EURECAm) working group of the European Renal Association– 12. Potpara TS, Lenarczyk R, Larsen TB, Deharo JC, Chen J, Dagres N. Management
European Dialysis and Transplantation Association (ERA-EDTA). of atrial fibrillation in patients with chronic kidney disease in Europe Results of
the European Heart Rhythm Association Survey. Europace 2015;17:1862–7.
Conflict of interest: none declared. 13. Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz
MD et al. Comparison of the efficacy and safety of new oral anticoagulants with
warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials.
References Lancet 2014;383:955–62.
1. Potpara TS, Ferro CJ, Lip G. Use of oral anticoagulants in patients with atrial fi- 14. Steffel J, Verhamme P, Potpara TS, Albaladejo P, Antz M, Desteghe L et al.;
brillation and renal dysfunction. Nat Rev Nephrol 2018;14:337–51. ESC Scientific Document Group. The 2018 European Heart Rhythm
2. Boriani G, Savelieva I, Dan GA, Deharo JC, Ferro C, Israel CW et al. Chronic Association Practical Guide on the use of non-vitamin K antagonist oral antico-
kidney disease in patients with cardiac rhythm disturbances or implantable elec- agulants in patients with atrial fibrillation: executive summary. Europace 2018;
trical devices: clinical significance and implications for decision making—a posi- 20:1231–42.
tion paper of the European Heart Rhythm Association endorsed by the Heart 15. Harel Z, Chertow GM, Shah PS, Harel S, Dorian P, Yan AT et al. Warfarin and
Rhythm Society and the Asia Pacific Heart Rhythm Society. Europace 2015;17: the risk of stroke and bleeding in patients with atrial fibrillation receiving dialysis:
1169–96. a systematic review and meta-analysis. Can J Cardiol 2017;33:737–46.
3. Lip GYH, Freedman B, De Caterina R, Potpara TS. Stroke prevention in atrial fi- 16. Siontis KC, Zhang X, Eckard A, Bhave N, Schaubel DE, He K et al. Outcomes as-
brillation: past, present and future. Thromb Haemost 2017;117:1230–9. sociated with apixaban use in patients with end-stage kidney disease and atrial fi-
4. Potpara TS, Jokic V, Dagres N, Larsen TB, Lane DA, Hindricks G et al. Non-vita- brillation in the United States. Circulation 2018;138:1519–29.
min K oral anticoagulant drugs for stroke prevention in patients with atrial fibril- 17. Coleman CI, Kreutz R, Sood NA, Bunz TJ, Eriksson D, Meinecke AK et al.
lation and chronic kidney disease. Curr Med Chem 2016;23:2055–69. Rivaroxaban versus warfarin in patients with nonvalvular atrial fibrillation and se-
5. Heidbuchel H, Dagres N, Antz M, Kuck KH, Lazure P, Murray S et al. Major vere kidney disease or undergoing hemodialysis. Am J Med 2019;132:1078–83.
knowledge gaps and system barriers to guideline implementation among 18. Fernandez-Prado R, Castillo-Rodriguez E, Velez-Arribas FJ, Gracia-Iguacel C,
European physicians treating patients with atrial fibrillation: a European Society Ortiz A. Creatinine clearance is not equal to glomerular filtration rate and
of Cardiology international educational needs assessment. Europace 2018;20: Cockcroft-Gault equation is not equal to CKD-EPI collaboration equation. Am J
1919–28. Med 2016;129:1259–63.
Corrigendum doi:10.1093/europace/euz365
.......................................................................................................................................................
Corrigendum to: 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias
[Europace 2019;21:1143–4]
In this expert consensus statement, Figure 5 has been modified for clarity to illustrate the inner loop and to include a supporting reference
in the figure legend. Please refer to the text of subsection 8.3.1 “Entrainment Mapping: Overview” and the references for further discussion.
The figure is shown correctly below and has been corrected online.
C 2020 The Heart Rhythm Society; the European Heart Rhythm Association, a registered branch of the European Society of Cardiology; the Asia Pacific Heart Rhythm Society;
V
and the Latin American Heart Rhythm Society. Published by Elsevier Inc./Oxford University Press/Wiley. This article is published under the Creative Commons CC-BY license.You can also read