Radiosensitivity Translates Into Excellent Local Control in Extremity Myxoid Liposarcoma
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Original Article
Radiosensitivity Translates Into
Excellent Local Control in Extremity
Myxoid Liposarcoma
A Comparison With Other Soft Tissue Sarcomas
Peter W. M. Chung, MB, ChB1,6; Benjamin M. Deheshi, MD2,3,6; Peter C. Ferguson, MD2,3,6;
Jay S. Wunder, MD2,3,6; Anthony M. Griffin, MSc3; Charles N. Catton, MD1,6; Robert S. Bell, MD2,3,6;
Lawrence M. White, MD5,6; Rita A. Kandel, MD4,6; and Brian O’Sullivan, MD1,6
BACKGROUND: Myxoid liposarcoma has been reported to be more radiosensitive compared with other
soft tissue sarcomas (STS). The authors report the results of multidisciplinary treatment of extremity myx-
oid liposarcoma compared with a contemporary cohort of other STS subtypes with an emphasis on the
role of radiotherapy (RT) in improving local control. METHODS: Between 1989 and 2004, 691 patients were
identified from a prospective STS database who underwent combined management for localized extremity
STS and were followed for a minimum of 12 months or until death. All patients underwent surgery together
with pre or postoperative RT, depending on their presenting characteristics and resection margins. Demo-
graphics and outcomes were compared between patients with myxoid liposarcoma and other STS sub-
types (other-STS). RESULTS: Of 691 patients, 88 patients had myxoid liposarcoma and 603 had other STS
subtypes (other-STS). Median age was 48 and 60 years for the myxoid liposarcoma and other-STS groups,
respectively. Median follow-up was 86 and 61 months, respectively. For myxoid liposarcoma and other-STS
groups, preoperative RT was used in 57% versus 61% of patients and postoperative RT in 43% versus 39%,
respectively. The 5-year local recurrence-free survival was 97.7% for patients with myxoid liposarcoma com-
pared with 89.6% for patients with other-STS tumors (P ¼ .008). High-grade tumors were present in 7%
and 59% of myxoid liposarcoma and other-STS patients, respectively (P ¼ .0003). Two myxoid liposarcoma
patients with local recurrence had positive resection margins, whereas only 33% of patients in the other-
STS group who developed a local recurrence had positive resection margins. No patients with myxoid lipo-
sarcoma required amputation as primary management, whereas 8 (1.3%) required amputation as primary
management in the other-STS group. Systemic disease control was superior in myxoid liposarcoma com-
pared with other-STS patients, with 5-year overall and metastasis-free survival rates of 93.9% versus 76.4%
(P ¼ .0008) and 89.1% versus 66.0% (P ¼ .0001) respectively. Of 12 myxoid liposarcoma patients with dis-
tant metastases, 7 appeared in nonpulmonary sites. In comparison, 205 (34%) patients with other-STS
tumors developed systemic disease but 78% had pulmonary metastases. CONCLUSIONS: Multidisciplinary
management of extremity STS achieves high rates of local control. Myxoid liposarcoma is associated with
Corresponding author: Peter W. M. Chung, MB, ChB, Princess Margaret Hospital, Radiation Oncology, 610 University Ave, Toronto, Ontario M5G
2M9 Canada; Fax: (416) 946-4442; peter.chung@rmp.uhn.on.ca
1
Radiation Oncology, Princess Margaret Hospital, Toronto, Ontario, Canada; 2Surgical Oncology, Princess Margaret Hospital, Toronto, Ontario, Can-
ada; 3Division of Orthopaedic Surgery, Mount Sinai Hospital, Toronto, Ontario, Canada; 4Department of Pathology, Mount Sinai Hospital, Toronto,
Ontario, Canada; 5Medical Imaging, Mount Sinai Hospital, Toronto, Ontario, Canada; 6University of Toronto, Toronto, Ontario, Canada
Presented, in part, at the 48th Annual Meeting of ASTRO, Philadelphia, Pennsylvania, November 5–29, 2006.
Received: September 23, 2008; Revised: December 23, 2008; Accepted: December 31, 2008
Published online: May 26, 2009 V
C 2009 American Cancer Society
DOI: 10.1002/cncr.24375, www.interscience.wiley.com
3254 Cancer July 15, 2009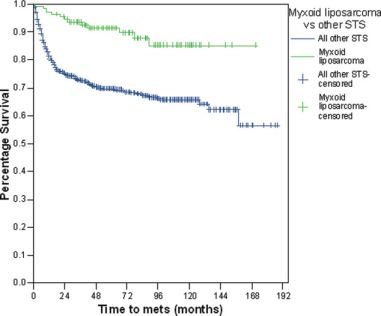
Local Control of Myxoid Liposarcoma/Chung et al
higher rates of local control compared with other STS subtypes, after combined surgery and radiation, sug-
gesting a particular radiosensitivity that can be exploited to improve oncologic outcome in appropriate
cases. Cancer 2009;115:3254–61. V C 2009 American Cancer Society.
KEY WORDS: myxoid liposarcoma, radiotherapy, local control, combined modality therapy, surgery.
Soft tissue sarcomas (STS) of the extremity are a heter- METHODS AND MATERIALS
ogeneous group of tumors with differing pathologies that The research ethics board approved this study. From our
clinically behave in a similar fashion. With the exception prospectively collected institutional database, 691
of certain pediatric and chemotherapy-sensitive histologi- patients who had surgical treatment and RT at our center,
cal subtypes, surgery plays a predominant role in the local between 1989 and 2004, for localized extremity STS
management of extremity STS.1 Radiotherapy (RT) has were identified. Patients were excluded if: chemotherapy
been shown to be an important adjunctive treatment and was a part of their treatment (n ¼ 75), they had meta-
improves local control rates over those seen with conserva- static disease at diagnosis, they had either dermatofibro-
tive surgery alone, particularly when ‘wide’ resection mar- sarcoma protuberans or well-differentiated liposarcoma.
gins cannot be obtained.2,3 Local control in extremity Patients who underwent initial surgery elsewhere before
STS would be expected to be around 90% overall with referral, usually in the form of an unplanned exci-
this approach.2 sion,13,14 and were referred for definitive management,
Myxoid liposarcoma is a common variant of liposar- were included if they were treated with further conserva-
coma and has a characteristic t(12:16) translocation that is tive surgery and RT at our center. In this setting, the
shared with myxoid/round cell liposarcoma (a higher ‘management policy’ evolved over time but currently,
grade variant with more aggressive biology4). Myxoid lip- patients would generally have preoperative RT and re-
osarcoma has a peculiar characteristic of extrapulmonary excision unless it was anticipated that excision with wide
metastasis5 not commonly seen in other STS subtypes margins could be achieved and, thus, RT was not likely
but appears to have a relatively favorable prognosis.6,7 to be needed. All patients had their pathology reviewed to
Although some studies have suggested that myxoid lipo- confirm the diagnosis and subtype of STS. The grade of
sarcoma may be relatively responsive to RT more than STS was assigned according to a 3-tier system. Myxoid
other types of STS, with high rates of regression and even liposarcoma patients were assigned a minimum of grade
reports of complete clinical response,8,9 others have 2, and if there was evidence of 5% or more round cell
reported high rates of local relapse overall; but, it is component within the specimen, then they were assigned
unclear that all appropriate patients received combined grade 3. Staging included full history and examination
management with surgery and RT in these studies.10,11 together with cross sectional imaging of the extremity
Pitson et al previously demonstrated an objective response (usually magnetic resonance imaging [MRI]). Thoracic
of myxoid liposarcoma to RT in the preoperative set- computed tomography (CT) scans were obtained and
ting.12 Thus adjunctive RT might translate into improve- other imaging was done at the discretion of the clinician.
ment in local control for myxoid liposarcoma patients Patients with locally recurrent disease and no distant me-
compared with other adult STS subtypes treated in a simi- tastases were included as long as the intent of manage-
lar manner. ment was conservative surgery and RT.
The aim of this retrospective study was to compare Patients were treated with limb conserving surgical
the outcomes of multidisciplinary treatment of a cohort of methods whenever possible. RT was used as an adjunct
myxoid liposarcoma patients with a contemporary group whenever surgical resection could not be achieved with
consisting of other STS subtypes (other-STS) treated in a wide negative margins (usually defined as a minimum of 2
standardized manner with particular emphasis on the role cm). Resections were categorized as complete excision
of RT in local control. with microscopic negative margins (R0), excision with
Cancer July 15, 2009 3255Original Article
microscopic positive margins (R1) or excision with gross Table 1. Patient and Treatment Characteristics
positive margins (R2). External beam RT was delivered in
Characteristics Myxoid All Other P
the preoperative setting (50 Gy) or postoperatively (60-66 Liposarcoma STS
Gy). In some cases, in the setting of positive margins after n 5 88 n 5 603
preoperative RT and surgery, a postoperative boost of up No. (%) No. (%)
to 16 Gy was delivered. The timing of RT evolved over Median age, y 48 [16, 86] 60 [15, 95] .0001
the period under study as postoperative RT was more [minimum, maximum]
commonly delivered up to 1994. From 1994-1997, a Sex .25
Male 52 (59) 314 (52)
national randomized clinical trial (NCIC SR2) of pre ver- Female 36 (41) 289 (48)
sus postoperative RT was conducted and influenced the Median size, cm 8.0 [2.5, 36] 7.5 [1, 39.5] .51
[minimum, maximum]
timing of RT for patients who participated in this trial.
Subsequent to this, preoperative RT became more com- Grade .0002*
1 0 84
mon. After treatment, patients were followed on a stand- 2 82 myxoid alone 161
ard schedule every 3 months to 6 months for the first 3 3 6 with round cell 358
years (high-grade patients were seen every 3 months), 6 Depth .65
Superficial 13 (15) 105 (17)
monthly until Year 5, and then annually until 10 years. At
Deep 75 (85) 498 (83)
each follow-up visit, physical examination and chest x-ray
Radiotherapy .57
were performed, and other imaging was done at the dis- Preoperative 41 (47) 317 (52.5)
cretion of the physician. Minimum follow-up was 12 Postoperative 38 (43) 234 (39)
Preoperative 1 9 (10) 52 (8.5)
months. Postoperative boost
Prior surgery (unplanned excision) .35
No 58 (66) 362 (60)
Statistical Methods Yes 30 (34) 241 (40)
Local recurrence-free survival, metastasis-free survival, Margin status after final surgery .34
Negative (R0) 71 (81) 459 (76)
and overall survival were estimated using the Kaplan- Positive (R1) 17 (19) 144 (24)
Meier method. Survival time was calculated from the date Positive (R2) 0 (0) 7 (1.2)
Amputation 0 (0) 8 (1.3)
of definitive surgery for the primary tumor. Differences in
survival were compared using the log-rank test. A p-value
ofLocal Control of Myxoid Liposarcoma/Chung et al
Table 2. Oncologic Outcomes
Outcome Myxoid Liposarcoma, All Other STS, P
n 5 88 n 5 603
No. (%) No. (%)
Current status
Alive, no evidence of disease 73 (83) 376 (65)
Alive with evidence of disease 5 (6) 73 (11)
Deceased (nonsarcoma related) 3 (3) 35 (6)
DOD 7 (8) 119 (18)
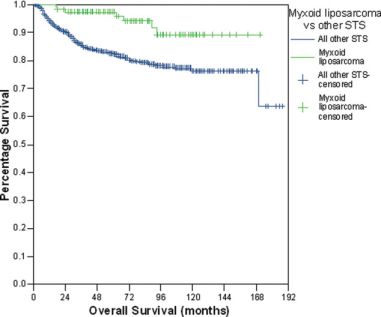
5-Year overall survival 93.9% 76.4% .0008
Local recurrence
Preoperative radiation 0/41 (0) 32/317 (10)
Preoperative 1 postoperative boost 1/9 (11) 10/52 (19)
Postoperative radiation 1/38 (3) 18/234 (8)
5-Year LR-free survival 97.7% 89.6% .008
Metastases 12 (13.6) 205 (34)
5-Year metastasis-free survival 89.1% 66% .0001
STS indicates soft tissue sarcoma; DOD, dead of disease; LR, local recurrence.
FIGURE 1. Overall survival myxoid liposarcoma versus other FIGURE 2. Metastasis-free survival myxoid liposarcoma ver-
STS subtypes (P ¼ .0008). sus other STS subtypes (P ¼ .0001).
The corresponding RT treatments in the other-STS group Overall survival at 5 years (Fig. 1) was 93.9% for the
were 52.5%, 8.5%, and 39%, respectively. myxoid liposarcoma group and 76.4% for the other-STS
group (p < .01). Not surprisingly, metastatic disease
developed more frequently in patients who were in the
other-STS group, in keeping with the larger proportion of
Outcomes patients with high-grade disease in that group. Metastasis-
Median follow-up was 86 months for the myxoid liposar- free survival at 5 years (Fig. 2) was 89.1% and 66.0% for
coma group and 61 months for the other-STS group. The the myxoid liposarcoma and other-STS groups, respec-
main oncological outcomes are shown in Table 2. tively (P < .01).
Cancer July 15, 2009 3257Original Article
Overall, 5-year local relapse-free survival was 97.7% types of STS, and although some historical series reported
for the myxoid liposarcoma group and 89.6% for other- high rates of local recurrence (up to 33%) in patients
STS patients. treated with surgery alone,6,19 other small series have
When patients with locally recurrent disease were noted good local control with the addition of RT.17,20,21
excluded, local recurrence-free rates were 98% for the In 1 such study of 10 patients, even in the presence of
myxoid liposarcoma group and 91% for the other-STS marginal or intralesional excisions without further sur-
group (P ¼ .02) at 5 years. gery, the addition of RT resulted in excellent local control
Of patients with local recurrence, both in the other- with no local relapses at mean follow-up of 58 months,
STS group had positive margins (and both patients had suggesting that the radiosensitivity of the tumor improved
grade 2 disease), whereas 33% (20 of 60) in the other-STS local control.22 Another more recent series examining
group had positive margins. combined modality therapy reported 100% local control
Overall, 12 (13.6%) myxoid liposarcoma developed in 9 patients with positive margins, 99% local control in
metastatic disease and 2 had multiple sites involved 91 patients with negative margins, and only 87% local
including mediastinum, spine, lung, and bone. Of 10 control in 25 patients where the margin status was
myxoid liposarcoma patients who developed a solitary site unknown.23 In our series, we did not have any patients
of metastatic disease, 4 had pulmonary metastases, 2 with gross positive margins (R2 resections) in the other-
intra-abdominal disease, 3 a soft tissue metastasis, and 1 a STS group, but there were 7 (1.2%) patients within the
spinal bone metastasis. Subsequently, 6 of these patients other-STS group who had R2 resections. We were not
developed further metastases. In contrast, of those in the able to distinguish patients with narrow but microscopi-
other-STS group who developed metastases, 78% (160 of cally negative margins of excision compared with those
205) had pulmonary metastases. with a more widely negative excision as all were coded as
R0. Of myxoid liposarcoma patients in our study, 17
had positive margins, of whom only 2 had local recur-
DISCUSSION rence (compared with 20 of 60 of other-STS patients).
Patients with extremity STS, managed at our center with Although the local control in myxoid liposarcoma
combined surgery and RT, had excellent local control patients is excellent, we believe our data confirm the
rates (90%) that compare favorably with other large se- need for adequate local surgery resulting in negative mar-
ries reported in the literature.15 In a recently published se- gins whenever possible because only those myxoid lipo-
ries of 279 patients undergoing primary treatment for sarcoma patients with positive resection margins
STS, the local recurrence rate was reported to be 16%.16 recurred locally.
Although the myxoid liposarcoma and other-STS Although the sensitivity of myxoid liposarcoma to
groups were comparable, the overall 5-year local disease RT was first reported more than 70 years ago and has
control for patients with myxoid liposarcoma treated with been described by others,8,24,25 only recently has objective
surgery and RT was exceptional. We hypothesized that the evidence of this response been reported. Pitson et al com-
radiosensitivity of myxoid liposarcoma would facilitate pared patients with myxoid liposarcoma to a group with
improved local control in patients treated with combined malignant fibrous histiocytoma who were both treated
surgery and RT. The results of this study support our with preoperative RT.12 Using MRI, before and after RT,
theory as myxoid liposarcoma patients treated with (neo)- a proportional reduction of 59% in median tumor vol-
adjuvant RT had 98% 5-year local control compared with ume was measured in myxoid liposarcoma patients. The
90% for other-STS patients. mechanism by which this volume reduction occurs is
Reports of patients with well-differentiated liposar- unknown but could be due to a particular cellular suscep-
coma, which generally requires surgery alone without RT, tibility or loss of tumor stroma. The TLS-CHOP (FUS-
and pleomorphic liposarcoma, which may have a higher DDIT3) translocation, which is commonly present in
rate of local recurrence, even when treated with adjuvant myxoid liposarcoma, and the resulting fusion protein play
RT, have been included together with myxoid liposar- a central role in formation of these tumors. These mutant
oma.17,18 Myxoid liposarcoma may be distinct from other fusion proteins involving CHOP fail to allow growth
3258 Cancer July 15, 2009Local Control of Myxoid Liposarcoma/Chung et al
arrest in response to radiation and may, thereby, lead to
the radiosensitivity typical of myxoid liposarcoma tumor
cells. It must be noted that while the presence of this trans-
location may aid the diagnosis of myxoid liposarcoma, it
has not been shown, at least thus far, to have prognostic
significance.26 This tendency to respond to RT is not only
important when planning combined treatment, but it
appears to increase the likelihood of local control for myx-
oid liposarcoma compared with other STS subtypes.
Many of our patients were treated with preoperative
(neoadjuvant) RT, which has been shown to result in the
same level of local control as postoperative (adjuvant) RT
in STS patients.27 An advantage of preoperative RT over
postoperative RT may be to limit late morbidity, particu-
larly in patients with large tumors as the smaller treatment
volumes and lower doses delivered in preoperative RT
may result in better functional outcome with less fibro-
sis28 as well as reduction in risk of bone fracture.29
Although the use of preoperative RT in STS patients has
not been universally adopted, its use in myxoid liposar-
coma patients may be preferable for several reasons. First,
preoperative RT would be expected to cause a large reduc-
tion in tumor volume, which may, in turn, allow less mor-
bid surgery, resulting in improved functional outcomes
without compromising local control. Second, preopera-
tive RT facilitates surgical sparing of critical structures ad-
jacent to the tumor margin. Even in the setting of
‘‘planned’’ positive margins after preoperative RT, where
the tumor does not shrink away from a vital structure after
preoperative RT, for example, after epineural dissection
of a major motor nerve, local control rates do not appear
to be significantly reduced.30 This may be particularly rel-
evant in the setting of myxoid liposarcoma as such tumors
frequently arise in intermuscular locations and may
involve neurovascular bundles.31 An example of the type
of response that may be seen with preoperative RT in
myxoid liposarcoma is shown in Figure 3.
Patients with myxoid liposarcoma generally have a
good prognosis and have the potential to gain maximum
benefit from strategies that minimize the long-term conse- FIGURE 3. Axial fat suppressed fast spin-echo T2-weighted
quences of RT. With modern RT techniques, such as in- (A) MR in a 55-year-old male patient with a myxoid liposar-
coma of the posterior compartment of the left thigh (arrows
tensity-modulated radiotherapy, further benefit might be in A). Corresponding axial fat suppressed fast spin-echo T2-
derived from reducing the normal tissue volume that weighted (B) MR images show dramatic reduction in the size
of the lesion post radiation therapy (arrows in B).
receives high doses while maintaining optimal local con-
trol. This may be advantageous in the preoperative set-
ting, but it may be more applicable in the postoperative
Cancer July 15, 2009 3259Original Article
setting since limiting the volume of normal tissue exposed In summary, we found excellent rates of local con-
to the higher doses of RT used with the aforementioned trol for STS patients treated with surgery and RT. Patients
highly conformal RT techniques might be expected to with myxoid liposarcoma treated at our center had signifi-
reduce the severity of late toxicity in these patients.32 cantly lower rates of local and distant failure compared
As with all retrospective data, patient selection sig- with other STS subtypes. Improved local control in myx-
nificantly influences outcome, as is the case in our 2 oid liposarcoma might well be due to its radiosensitivity,
patient cohorts. One might speculate that including while a lower rate of metastasis may be a reflection of the
patients with locally recurrent disease may reduce the relatively low numbers of patients with high-grade disease
apparent local control rate for other-STS patients, espe- in the myxoid liposarcoma cohort as well as the high rate
cially because this group had a larger proportion of of local control. It has been recognized that particular sub-
patients with locally recurrent disease at initial presenta- types of STS may have specific characteristics; myxoid lip-
tion. However, even after excluding these patients, the osarcoma is 1 such subtype, and the data presented here
local control rate was 90% for the other-STS group. suggest that its radio-responsiveness translates into excel-
For patients who underwent ‘unplanned’ excision of a lent local control when RT is appropriately applied.
sarcoma elsewhere with positive margins before referral,
our policy is for further re-excision as these patients are
at significant risk of local recurrence even with the addi- Conflict of Interest Disclosures
tion of RT. Our group and others have reported high The authors made no disclosures.
rates (59%) of residual disease following ‘unplanned’
excisions, which provides evidence to support this treat- References
ment algorithm.13,14,33,34 We do not believe that this
1. Wunder JS, Nielsen TO, Maki RG, O’Sullivan B, Alman
should be a significant confounding factor as the propor- BA. Opportunities for improving the therapeutic ratio for
tion of patients referred after ‘unplanned’ excisions and patients with sarcoma. [Comment in: Lancet Oncol.
their subsequent management was similar in both 2007;8:667-8; author reply 668-9.] [Erratum in: Lancet
Oncol. 2007;8:670]. Lancet Oncology. 2007;8:513-524.
patient groups.
2. Strander H, Turesson I, Cavallin-Stahl E. A systematic
The unusual metastatic disease pattern in myxoid
overview of radiation therapy effects in soft tissue sarcomas.
liposarcoma has previously been documented with predi- Acta Oncologica. 2003;42:516-531.
lection for intra-abdominal/retroperitoneal sites6,7,35,36 in 3. Enneking WF, Spanier SS, Goodman MA. A system for
addition to osseous metastases most commonly involving the surgical staging of musculoskeletal sarcoma. Clin Orthop
the spine.5 In our series, metastatic disease developed in Relat Res. 1980; Nov-Dec:106-120.
14% of patients, and over half of these were in nonpulmo- 4. Antonescu CR, Elahi A, Humphrey M, et al. Specificity of
TLS-CHOP rearrangement for classic myxoid/round cell
nary sites. Although the pattern of distant metastasis is not liposarcoma: absence in predominantly myxoid well-differ-
unusual for this disease, the incidence was relatively low in entiated liposarcomas. J Mol Diagn. 2000;2:132-138.
our myxoid liposarcoma patients. This may be a reflection 5. Schwab JH, Boland P, Guo T, et al. Skeletal metastases in
of the small number of patients with a round cell compo- myxoid liposarcoma: an unusual pattern of distant spread.
nent (which appears to confer greater metastatic poten- Ann Surg Oncol. 2007;14:1507-1514.
tial21) in our cohort, but it could also be related to the 6. Chang HR, Hajdu SI, Collin C, Brennan MF. The prog-
nostic value of histologic subtypes in primary extremity lip-
high rate of local disease control. One investigation of osarcoma. Cancer. 1989;64:1514-1520.
patients with liposarcoma reported a 22% incidence of 7. Spillane AJ, Fisher C, Thomas JM. Myxoid liposarcoma–
distant metastasis in myxoid liposarcoma compared with the frequency and the natural history of nonpulmonary soft
over 40% in pleomorphic liposarcoma.18 Given the rela- tissue metastases. Ann Surg Oncol. 1999;6:389-394.
tively atypical metastatic pattern in myxoid liposarcoma 8. Edland RW. Liposarcoma. A retrospective study of fifteen
cases, a review of the literature and a discussion of radiosen-
compared with other sarcomas, it has been recommended
sitivity. Am J Roentgenol Radium Ther Nucl Med.
that patients with myxoid liposarcoma should have rou- 1968;103:778-791.
tine staging and follow-up to include abdominopelvic CT 9. Reitan JB, Kaalhus O. Radiotherapy of liposarcomas. Br J
scans and imaging of the spine.5,23 Radiol. 1980;53:969-975.
3260 Cancer July 15, 2009Local Control of Myxoid Liposarcoma/Chung et al
10. Ten Heuvel SE, Hoekstra HJ, van Ginkel RJ, Bastiaannet E, 24. Ewing J. Fascial sarcoma and intermuscular myxoliposar-
Suurmeijer AJ. Clinicopathologic prognostic factors in myx- coma. Arch Surg. 1935;31:507-520.
oid liposarcoma: a retrospective study of 49 patients with 25. Shiu MH, Chu F, Castro EB, Hajdu SI, Fortner JH.
long-term follow-up. Ann Surg Oncol. 2007;14:222-229. Results of surgical and radiation therapy in the treatment
11. Fiore M, Grosso F, Lo Vullo S, et al. Myxoid/round cell of liposarcoma arising in an extremity. Am J Roentgenol Ra-
and pleomorphic liposarcomas: prognostic factors and sur- dium Ther Nucl Med. 1975;123:577-582.
vival in a series of patients treated at a single institution. 26. Antonescu CR, Tschernyavsky SJ, Decuseara R, et al. Prog-
Cancer. 2007;109:2522-2531. nostic impact of P53 status, TLS-CHOP fusion transcript
12. Pitson G, Robinson P, Wilke D, et al. Radiation response: structure, and histological grade in myxoid liposarcoma: a
an additional unique signature of myxoid liposarcoma. Int J molecular and clinicopathologic study of 82 cases. Clin
Radiat Oncol Biol Phys. 2004;60:522-526. Cancer Res. 2001;7:3977-3987.
13. Noria S, Davis A, Kandel R, et al. Residual disease follow- 27. O’Sullivan B, Davis AM, Turcotte R, et al. Preoperative
ing unplanned excision of soft-tissue sarcoma of an extrem- versus postoperative radiotherapy in soft-tissue sarcoma of
ity. J Bone Joint Surg Am. 1996;78:650-655. the limbs: a randomised trial.[see comment]. Lancet.
14. Davis AM, Kandel RA, Wunder JS, et al. The impact of 2002;359:2235-2241.
residual disease on local recurrence in patients treated by 28. Davis AM, O’Sullivan B, Turcotte R, et al. Late radiation
initial unplanned resection for soft tissue sarcoma of the morbidity following randomization to preoperative versus
extremity. J Surg Oncol. 1997;66:81-87. postoperative radiotherapy in extremity soft tissue sarcoma.
15. Weitz J, Antonescu CR, Brennan MF. Localized extremity Radiother Oncol. 2005;75:48-53.
soft tissue sarcoma: improved knowledge with unchanged 29. Holt GE, Griffin AM, Pintilie M, et al. Fractures following
survival over time. J Clin Oncol. 2003;21:2719-2725. radiotherapy and limb-salvage surgery for lower extremity
16. Fiore M, Casali PG, Miceli R, et al. Prognostic effect of re- soft-tissue sarcomas. A comparison of high-dose and low-
excision in adult soft tissue sarcoma of the extremity. Ann dose radiotherapy. J Bone Joint Surg Am. 2005;87:315-319.
Surg Oncol.. 2006;13:110-117. 30. Gerrand CH, Wunder JS, Kandel RA, et al. Classification
17. Spittle MF, Newton KA, Mackenzie DH. Liposarcoma. A of positive margins after resection of soft-tissue sarcoma of
review of 60 cases. Br J Cancer. 1970;24:696-704. the limb predicts the risk of local recurrence.[see comment].
J Bone Joint Surg Br. 2001;83:1149-1155.
18. Zagars GK, Goswitz MS, Pollack A. Liposarcoma: outcome
and prognostic factors following conservation surgery and 31. Clarkson PW, Griffin AM, Catton CN, et al. Epineural
radiation therapy. Int J Radiat Oncol Biol Phys. 1996;36: dissection is a safe technique that facilitates limb salvage
311-319. surgery. Clin Orthop Relat Res. 2005;438:92-96.
19. Azumi N, Curtis J, Kempson RL, Hendrickson MR. Atypi- 32. Griffin AM, Euler CI, Sharpe MB, et al. Radiation plan-
cal and malignant neoplasms showing lipomatous differen- ning comparison for superficial tissue avoidance in radio-
tiation. A study of 111 cases. Am J Surg Pathol. 1987;11: therapy for soft tissue sarcoma of the lower extremity. Int J
161-183. Radiat Oncol Biol Phys. 2007;67:847-856.
20. Evans HL. Liposarcoma: a study of 55 cases with a reassess- 33. Zagars GK, Ballo MT, Pisters PW, et al. Surgical margins
ment of its classification. Am J Surg Pathol. 1979;3:507-523. and reresection in the management of patients with soft tis-
sue sarcoma using conservative surgery and radiation ther-
21. Kilpatrick SE, Doyon J, Choong PF, Sim FH, Nascimento
apy. Cancer. 2003;97:2544-2553.
AG. The clinicopathologic spectrum of myxoid and round
cell liposarcoma. A study of 95 cases. Cancer. 1996;77: 34. Chandrasekar CR, Wafa H, Grimer RJ, et al. The effect of
1450-1458. an unplanned excision of a soft-tissue sarcoma on progno-
sis. J Bone Joint Surg Br. 2008;90:203-208.
22. Hatano H, Ogose A, Hotta T, et al. Treatment of myxoid
liposarcoma by marginal or intralesional resection combined 35. Pearlstone DB, Pisters PW, Bold RJ, et al. Patterns of re-
with radiotherapy. Anticancer Res. 2003;23:3045-3049. currence in extremity liposarcoma: implications for staging
and follow-up. Cancer. 1999;85:85-92.
23. Guadagnolo BA, Zagars GK, Ballo MT, et al. Excellent local
control rates and distinctive patterns of failure in myxoid lip- 36. Estourgie SH, Nielsen GP, Ott MJ. Metastatic patterns of
osarcoma treated with conservation surgery and radiotherapy. extremity myxoid liposarcoma and their outcome. J Surg
Int J Radiat Oncol Biol Phys. 2008;70:760-765. Oncol. 2002;80:89-93.
Cancer July 15, 2009 3261You can also read

















































