Management of sickle cell disease - Mariane de Montalembert Service de Pédiatrie Générale, Necker Enfants Malades, Paris Centre de Référence des ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Management of sickle cell disease
Mariane de Montalembert
Service de Pédiatrie Générale, Necker Enfants Malades, Paris
Centre de Référence des Syndromes Drépanocytaires majeurs
Labex GR-Ex
RoFSED
mariane.demontal@aphp.fr
Definition-Epidemiology
Autosomal recessive disease characterized by the presence of hemoglobine S (HbS)
(b6 Glu> Val)
- In homozygous status on both b-globine alleles (HbSS disease)
- Associated with HbC on the other b-globine allele (HbSC disease)
- Associated with b-thalassemia on the other b-globine allele (HbS/b-thalassemia)
- More rarely, associated with another mutation of b-globine gene
Rees DC et al. Lancet 2010
Sickle cell disease syndromes
A% S% A 2% F% Hb g/l MCV fl
SS 0 S N 0 - 20 60 -100 N
SC 0 S=C N 0-5 100 -130 N
S b0 thal 0 S 5 - 10 80 -100 < 80
S b+ thal A < S 5 - 20 70-110 < 80
AS A > S N N N N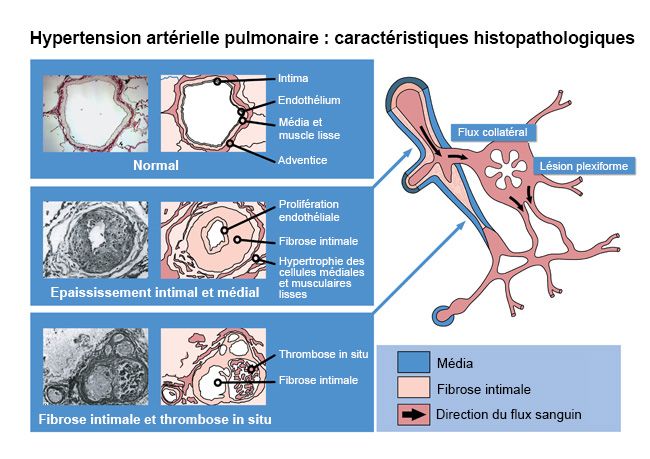
Newborn Screening
Conventional methods
Isoelectric focusing (IEF)
manual
lower cost Confirmatory tests
- IEF
- HPLC
- HPLC - Capillary electrophoresis
- Capillary electrophoresis
semi-automated
highest cost (kits)
70-80.000 tests/year
Innovative high throughput methods Autopuncher
Maldi-Tof
Mass spectrometry (MALDI-TOF)
fully automated
high cost of material
no reagents 2-300.000 tests/year
Courtesy of Jacques Elion
µExpert Centres
nFirst-line centres
¥Second-line centres
µ Paris area 5636
n Lille 133
IdF 2015 FKP SCD
n Rouen –Le Havre –
Evreux – Amiens –
¥ second-line centres
N pts
(75, 77, 78, 91, 92, 93, 94, 95) : 1548 13 Lisieux 208
191
incidence 1/14056n Rennes-Brest-Caen 671/649
n Nantes-Angers 89
n Poitiers-Orléans-Tours
DOM-TOM 116
µ Lyon – Marseille
µ Guadeloupe – Martinique n Clermont-Fd –
Limoges – St Etienne 434
2109 160 ¥ Grenoble 14
n Bordeaux
Mayotte
107
¥ Nimes 14
n Mayotte – Réunion n Guyane ¥ Nice 31
n Montpellier
174 255 n Toulouse
82 45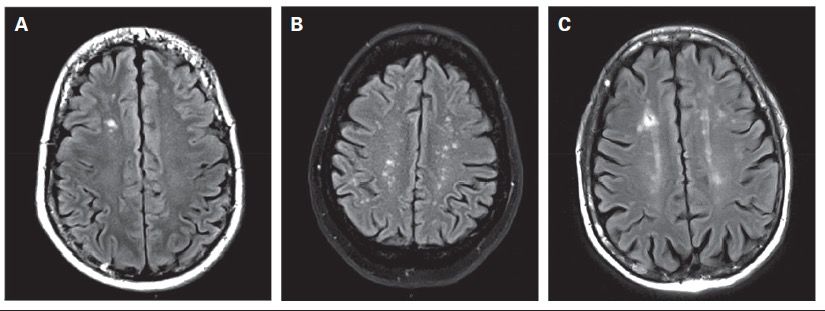
Pathophysiology
Hypoxia reoxygenation
Inflammation
Increased RBC adhesion
Haemolysis
NO
Endothelial dysfunction
Red cell
dehydration
Platelet activation HbS/HbF
Polymerization of
deoxhHbS Reproduced from Stuart MJ, Nagel RL. Lancet.
Sickling 2004;364:1343-60 © 2004, with permission from Elsevier.
Modified by M de Montalembert.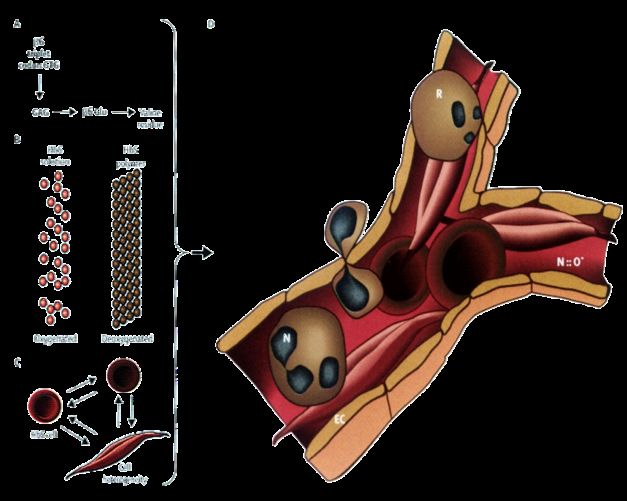
Inflammation implicated
in vaso-occlusive crises
Enhanced understanding of endothelial activation points to new therapies
Platelet
ESL RBC
E-selectin
aMb2 integrin
Neutrophil
Role of adherent sickle erythrocytes
Endothelial Cell Activation _
E- and P-Selectin expression
Inflammatory Endothelial integrin activation Leukocyte Sickle Erythrocyte
Leukocyte
Cytokine ICAM-1, VCAM secretion Adhesion to Adhesion to
Activation
Secretion Endothelium Leukocytes
Platelet Activation
Vasoocclusion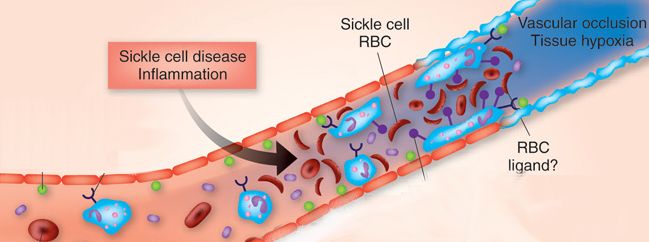
Des complications aiguës et une évolution chronique
Red cell sickling Red cell sickling
Chronic inflammation
Intimal hyperplasia
Impaired NO-induced vasodilation
Spleen dysfunction infection
sequestration
Vasocclusion: pain
Vasoocclusion: pain Vasculopathy: stroke, PHT, renal disease..
Median life expectancy in male patients
with homozygous sickle cell disease is increasing
years
Daily peni: 1986
Neonatal screening:
70 1988 58
50 42
HC: 1995
14.3
TCD: 1998
10
1973 1994 2014 Adapted from
Elmariah H, Am J Hematol 2014
Indeed, the disease remains severe
in many patients
Morbidity of SCA is high:
ü chronic pain, unpredictable painful events,
ü organ failure, neurocognitive defects (silent infarcts)
ü multiple drugs (transfusion, chelation)
Median age at death at:
ü38 yrs M, 42 yrs F (USA, Lanzkron,
Public Health Report 2013)
ü37 yrs (France, Ngo, ASH 2014)
There is a sub-population of highly severe patients,
needing early intensification of treatmentCauses of death in SCD adult patients
Ngo S, ASH 2014, abstract 2715
• Cohort of 2478 patients followed-up in one French center
• 96 deaths between 2001-2013
• Median age at death: 36 yrs
• Main causes:
– Acute organ failure in a context of chronic organ impairment (22,9%)
– ACS (16,7%)
– Infection (16,7%)
– Cerebral hemorrhage (10,4%)
– Drug overdose (7,3%)
– Acute right heart failure (5,2%)
– Delayed hemolytic transfusion reaction (4,2%)
– 6 deaths during pregnancy
– History of kidney failure (p=0,01) and positive irregular antibodies (p=0,04)
risk factors for premature deathAxes prioritaires de la prise en charge d’un patient drépanocytaire adulte • Prise en charge optimale des complications, surtout de la douleur • Prévention des complications aiguës et chroniques • Mise en place d’un traitement de fond si nécessaire • Prise en compte des répercussions psychologiques et sociales
Management of complications
infection
CV
Severe vasocclusion: pain
Vicious circle !
ACS, stroke,..
Worsening
of chronic anemiaVaso-occlusive crises
• Incidence: # 30 VOC /100 pt-yrs (personal data), but
– highly variable according to patients
• Increased by: cold, dehydration, infection, hypoxia,
stress…
• Pain, decreased motility, local inflammatory signs,
fever
– Long bones +++: femur, humerus
– Vertebrae
– Ribs (risk of ACS)Management of acute pain
Prevention
– Hydration
– Eviction of cold, dehydration,…
– NSAID unless contraindicated
– Acetaminophen, tramadol, codein if > 12yrs
Treatment
- Shortened time in trial
- Hydration
- Opioids
- Regular and continuous assessment of pain and relief
- Encourage non pharmacological and psychological
support Ballas SK et al
Hematol/oncol Clin N Am 2005A frequent pitfall in diagnosis in SCD patients:
acute bone pain
Vasooclusive crisis (VOC)
?
Ostemyelitis
Key messages
• Neutrophils, CRP weakly discriminant between VOC
and infection
• Rx useless
•Ultrasonography helpful; MRI?
•Salmonella are frequently responsible for osteomyelitis
•Treatment of osteomyelitis need high dosages of antibiotics• Jeune fille SS de 22 ans, hospitalisée pour NEJM 2005; 352:2425 douleurs dos et MI. • A l’arrivée, auscultation pulmonaire nle, RxThorax : opacités LIG, SatO2: 100% • Persistance douleur malgré morphine; à H5, Sat O2 : 76% • H10, Sat O2: 40%, intubation, • Transfusion simple puis échange, ATB large spectre, NO • Décès à H48
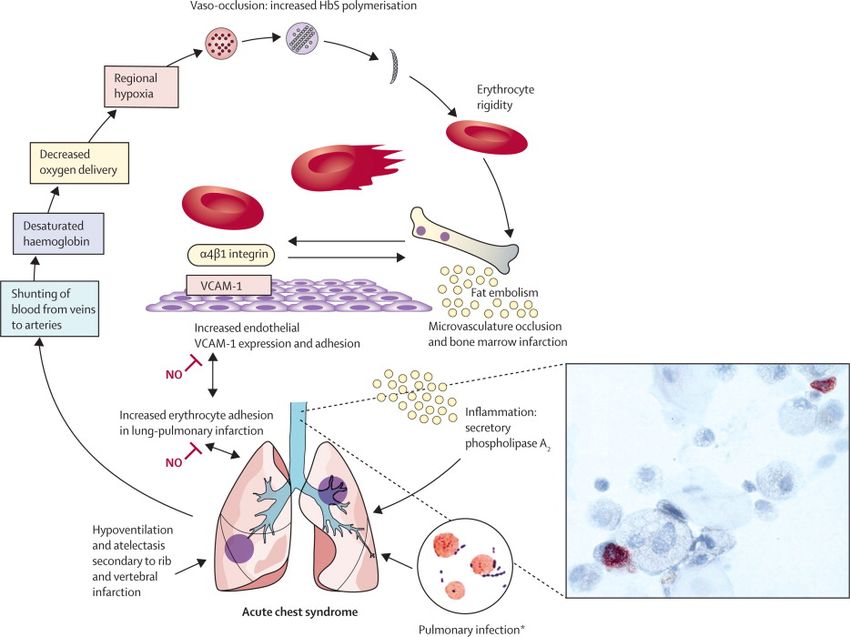
Management of acute chest syndrome
1. Diagnosis
Fever and/or acute respiratory symptoms accompanied by a
new pulmonary infiltrate on X-ray
2. Multiple causes
Infection
Pain
Pulmonary embolism
Hypoventilation…
3. Treatment
In intensive care unit
Adequate pain relief
Non invasive ventilation
Antibiotics
Consider transfusion or exchange transfusion
Consider Hydroxycarbamide for preventing a
recurrence
Howard J, et al. Br J Haematol 2015.
Rees DC et al. Lancet 2010Les complications infectieuses L’asplénie fonctionnelle est responsable d’une vulnérabilité aux germes encapsulés. Toute q > 38°5 impose une ATB probabiliste active contre le Pneumocoque Pneumopathies Amoxicilline en première intention + macrolide : d’emblée si STA ou germe atypique suspecté, secondairement si pas d’évolution favorable sous amoxicilline Risque d’évolution vers STA Ostéomyélites Diagnostic difficile: intérêt de l’IRM Fréquence des salmonelles Recherche de porte d’entrée : dents, voies bilaires, KT Septicémies Peuvent être fulminantes Germes les plus fréquents : pneumocoque, E. Coli, salmonelles, staph doré
Management of acute worsening of chronic anemia
Median baseline Hb in patients with HbSS and HbS/b0-thalassemia is 8± 1 g/dL (retics ≈200 G/l)
Baseline Hb higher in patients with HbSC and HbS/b+-thalassemia
Worsening anemia may be related to
- acute splenic sequestration in children, hypersplenism
- transient aplastic crisis secondary to Parvovirus B19 infection
- hyperhemolyis related to acute infection or painful crisis
- delayed hemolytic transfusion reaction
Decision to transfuse relies on:
- Hb level and retics response
- Clinical tolerance of anemia
-Past history of allo-immunization and/or blood group genotype
Transfusion will match as close as possible patient’s extensively phenotyped blood group
And will bring Hb level close to its baseline level (Risk of increasing blood viscosity)Epidemiology of neurological complications in SCD
• Overt stroke: 1.02/100 pt-years between
2 and 5 yrs (Ohene-Frempong K, 1998)
• Moya-Moya (progressive stenosis of distal ICA +
abnormal network of collaterals) :
20% in children with strokes (Moritani T, 2004)
• Silent cerebral infarcts
u21.8% SS children aged 6 to 19 yrs (Pegelow CH, 2002)
u 37% SS children by their 14th birthday (Bernaudin F, 2011)
Related with cognitive impairments (DeBaun MR, 2012)Classic example of cerebral
vasculopathy in SCD
Intracranial segment of left internal carotid artery in a HbS/HbS patient
who had a stroke: lumen entirely filled with proliferated intima
The proliferated intima was considered the likely primary event which
led to formation of thrombi
Merkel KH et al. Stroke 1978;9:45–52Epidemiology
c
• Overt strokes
0.0040 Hemorrhagic CVA
0.0035
Hazard function
0.0030
0.0025 Ischemic CVA
0.0020
0.0015
0.0010
10 20 30 40 50
Age (years)
Ohene-Frempong K, Blood 1998
Prevalence 11% by 20 yrs of age in SS patients
Maximal incidence (1.02 per 100 patient/yr) in SS children aged 2-5 yrsInfarctus cérébraux silencieux chez des patients adultes drépanocytaires
Calvet D, et al. Blood advances 2017Priapisme
– complication fréquente: 6% des enfants
42% des adultes
– deux modes :
– les priapismes intermittents,
spontanément résolutifs en moins de 3 h
– les priapismes aigus
– Protocole de prise en charge de priapisme :
– traitement per os par EffortilÒ (étiléfrine) dès
que les épisodes intermittents apparaissentTraitement de priapisme aigu – si < à 3 heures : injection en intracaverneux, 0.6 ml d’une amp. d’EffortilÒ à répéter 20 min plus tard si la détumescence ne se produit pas. – si > à 3 heures : drainer les corps caverneux , il s’agit d’évacuer par écoulement le sang, sans aspirer ni laver, puis d’injecter l’EffortilÒ. – Échange transfusionnel
Complications chroniques de la drépanocytose
Ware RE, et al. Lancet 2017Hypertension artérielle pulmonaire • Associée à un phénotype hémolytique (anémie, élévation LDH, ulcère de jambe, priapisme) • Echo coeur : tricuspid regurgitant jet velocity ≥2.5 m/sec • Gladwin NEJM 2004: présente chez 30% des patients • Facteur de risque de décès (rate ratio, 10.1; 95% confidence interval 2.2 to 47.0; P
Prothèse totale de hanche
Douleur
Raideur
50% de descellements septiques
ou aseptiques à 5 ansCan we decrease mortality in young adults with SCD?
Recommended exams to be performed annually
0-1 yr 2 yrs 3-5 yrs 6-9 yrs 10-15 yrs 16-18 yrs
Physical examination
Transcutaneous O2 sat
Laboratory tests*
Assessment of
adherence to tt and
appointments
TCD
Liver/gallbladder
ultrasound
Academic
performance
Pulmonary function
tests
Hip x-ray
ECG
Ophthalmological
evaluation**
* CBC, liver profile, electrolytes, BUN, creatinine, µalbuminuria, ferritin if transfused, calcium metabolism,
parvovirus B19 serology until positive. ** Since the age of 6 yrs if Hb SC disease.
de Montalembert, Am J Hematol 2011.Increased survival rate in adults under Hydroxyurea treatment Steinberg MH, J Am Med Assoc. 2003 Voskaridou E, Blood 2010
Mechanisms of action of HU
Rees DC, Haematologica 2001Hydroxyurea and ACE could limit worsening of renal impairment
Multivariate determinants of albuminuria
- HU use= OR: 0,28 (95% CI: 0,11-0,75), p=0,01
Laurin, Nephrol Dial Transplant 2014
Bartolucci, JASN 2015Indications for hydroxycarbamide (HC)
2 current options
To select indications
To propose HC to all
patients, whatever
the severity of their - Recurrent VOC and or ACS (RCT)
disease - After a period of transfusion
Yawn BP et al, JAMA and normalization of TCD in patients
2014 having had abnormal TCD
and having normal MRI (RCT)
- Baseline Hb level < 7 g/dl
- Renal impairment
- Hypoxemia
- Multiple cerebral silent infarcts
- Conditional velocities on TCD
RCT: based on randomized controlled trial3 VOC/yr
> 2 ACS Stroke
Hb < 7g/dL
Abnormal Silent cerebral infarct
TCD
HU
Minimal tt of 6-9 mo
rial
t
SIT
↓ VOC/ACS : Failure
success
Start chronic transfusion switch to HU
TWiTCH trial
Look for HLA-id. sibling
Yes No
HSTC Chronic transfusion +
chelation
EHA, Stockholm 2013Deaths observed in the
international survey
Gluckman et al, Blood 2016
1000 SCD patients transplanted with HLA-id sibling
Ø 846 children: median age at HSCT: 9 yrs (0,3-16)
Ø 154 adults: median age at HSCT: 20 yrs (16-54)
OS (%) EFS (%) Graft a GVH (%) C GVH (%)
rejection
(%)
92.9 91.4 2.3 14.8 14.3
70 deaths:
Ø infection: 14
Ø GVHD: 9
Ø toxicity: 9
Ø hemorrhage: 3
Ø secondary malignancy: 2
Ø no specified cause: 33Myelo-ablative HLA-matched sibling
transplants in SCD
Walters Panepinto Bernaudin Locatelli Mahesh- Lucarelli Dedeken
-wari
year 2000 2007 2007 2013 2014 2014 2014
Median F.U. 4.8 (3.2-7.9) 5.1 (0.25- 6 (1.6-17.5) 5.8 (1- 3 (1.3-9) 7.7 (0.4-21.3)
(yrs) 14.8) 12.5)
N 50 67 87 160 16 42 50
Conditioning BU,CY, ATG BU, CY, other BU, CY, BU, other BU, CY, ATG BU, CY, other BU, CY, ATG >
or ATG>1992 1991
CAMPATH
Age yrs 3.3-15.9 2-27 2-22 1.2-19.3 2-16 0.9-31.8
Primary 98 100 97.6 94
engraftment %
Graft rejection 10 15 3 [>1992] 0 0 8
%
Acute GVHD % 10 GII: 11.6 GII: 13 GI-II: 30 GI-II: 12
G III-IV: 8.1 G III-IV: 0 GIII-IV: 17.5 G III-IV : 10
Chronic GVHD 22 12.6 0 5 20
%
Death % 6 3 5 > 2000 3 0 9 6
DFS% 84 85 95>2000 92 100 91 85.6Non myelo-ablative HLA-matched sibling
transplants in SCD
Bhatia Krishnamurti Hsieh King
Reduced toxicity Reduced intensity conditioning
year 2014 2008 2014 2015
Median F.U. (yrs) 2.9 (0.4-7.5) 4 (2-8,5) 3.4 (1- 8.6) 3.4 (0.7-11.8)
N 18 7 30 43 SCD + 9 thal
Conditioning BU, Flu alemtuzumab BU, Flu, ATG, TLI Alemtuzumab, TBI(300 Alemtuzumab,
cGy), sirolimus Flu, melphalan
Age (yrs) 2.3-20.2 6-18 17-65 0.8-20. 3
Primary 100 100 87 96
engraftment%
Graft rejection% 0 14 (N=1) 13 2
Acute GVHD% GII-IV: 17 GII: 14 (N=1) 0 GI-III: 23
G III-IV : 11
Chronic GVHD% 11 14 (N=1) 0 13
Death% 0 0 3 7
TR-infections N=6 Continued
Sirolimus-toxicity N=5 immunosuppr.
Continued N=3
immunosuppr.= N=10
EFS% 100 86% 87 91Outcome of patients receiving haplo-identical hematopoietic
stem cell transplant
N Median OS% Rejection DFS% GVH% TRM%
age (yrs) %
Bolanos- 14 22 100 43 57 0 0
Meade
(2012)
Dallas 8 9 75 38 38 38cGVH 25
(2013)
De la Fuente 13 SCD + 10 94 6 12.5aGVH 6
(2015)
3 TM 6.3cGVH
Dedhin 5 26.4 100 60 13.6
(2016)
7 18.1 28.5aGVH
22 10 86.4 9.1 81.8 18.2aGVH+cGVHRibeil JA, …Leboulch P and Cavazzana M, NEJM 2017; 376: 848-55
Early screening
Improving life expectancy Effective treatments
needs
And !
Patient’s adhesionDiscontinuation of chronic blood transfusions after
transition to adult care?
A retrospective analysis of 22 SCD patients (10 males, 12 females) with childhood stroke who were
referred to adult programmes between 1993 and 2009
Results
● Patients who were non-compliant with blood transfusion or who refused to be maintained on
chronic transfusions were hospitalized for painful crises 5.7 ± 5.00 times annually
● All 5 patients who refused to be maintained on chronic blood transfusions died within
3 years after transition
One third of patients with SCD and stroke died within 3 years of transition
to adult care due to discontinuation or poor compliance with
blood transfusion regimens
Slide created by Bart Biemond for the GIS, March 2012
Ballas SK. Blood. 2010;116:[abstract 1629].High rate of non observance in adolescents
and young adults
369 patients in France, median age 35 ±12 yrs (Foïs E, et al. Hematologie 2013;19:5
1/3 patients take HU 1 day/ 2
Reasons for non compliance:
Ø omission (39 %)
Ø tiredness (13 %)
Ø side effects (9 %) % of omission according to treatment
60% 57%
50%
40% 35%
32%
30%
20%
10%
0%
HU Folic acid otherSome references… • La Revue de Médecine interne. Mai 2015. 36, Supp. Au n°5, S1-5S54. • Yawn BP, Buchanan GR, Afenyi-Annan AN, et al. Management of sickle cell disease. Summary of the 2014 Evidence-Based Report by Expert Panel Members. JAMA 2014; 321: 1033-1048. • Howard J, Hart N, Roberts-Harewood M, et al. Guideline on the management of acute chest syndrome in sickle cell disease. Br J Haematol 2015; 169: 492-505. • Ware RE, de Montalembert M, Tshilolo L, Abboud M. Sickle cell disease. Lancet 2017; 390: 311-23
Un adulte porteur d’une drépanocytose homozygote, déjà hospitalisé à 2 reprises dans l’année précédente, se présente aux urgences pour une crise douloureuse avec douleurs dorsales EVA à 9/10 : Q1 -Le délai de prise en charge du patient doit être court, de l’ordre de 30 minutes -Le traitement débute par l’administration d’un antalgique de palier 2 - La radio de thorax doit être systématique - L’examen clinique doit être succinct, pour éviter de mobiliser le malade, en raison de la douleur, et sera complété quand cette douleur aura diminué - L’utilisation de dérivés morphiniques lors des hospitalisations est fréquemment responsable d’une toxicomanie
Au 3ème jour d’hospitalisation, apparition d’une fièvre à 38,80C, sans point d’appel clinique : Q2 -En première intention, il faut considérer que la fièvre est probablement liée à la crise vaso-occlusive osseuse -La radio standard osseuse est utile -Les voies d’abord vasculaires, même en périphérie, représentent une porte d’entrée septique possible -L’existence d’une hyperleucocytose à 16600/dL dont 9600 polynucléaires et d’une C-réactive protéine à 172 sont en faveur d’une infection bactérienne - Dans tous les cas, l’antibiothérapie instituée doit être active sur le pneumocoque, même si le patient est à jour de la vaccination anti- pneumococcique
Q3 Une polypnée est constatée, et l’auscultation retrouve des râles crépitants de la base droite : -Une saturation de 97% sous oxygénothérapie de 3 l/min est rassurante -La kinésithérapie respiratoire incitative doit être instituée car elle a fait la preuve de son efficacité dans la prévention et le traitement du syndrome thoracique aigu -Atteinte pulmonaire bilatérale ou installation rapide des symptômes pulmonaires représentent des signes de gravité d’un syndrome thoracique aigu -Le manque d’habitude des équipes paramédicales dans les modalités de surveillance d’un syndrome thoracique aigu peuvent représenter une indication à transfert dans une unité de soins continus
• Un patient drépanocytaire SS de 25 ans arrive aux urgences pour une crise vaso-occlusive osseuse touchant les humérus et les tibias. Il n'y a pas de facteur déclenchant évident retrouvé si ce n'est un épisode de diarrhée il y a 48 heure qui a cédé spontanément. • Ses antécédents sont les suivant: priapisme dans l'enfance, un syndrome thoracique aigu sans critère de gravité, il y a 2 ans (le patient fut perdu de vu depuis). Il n'a pas été cholécystectomisé. Son traitement de fond comporte uniquement de l'acide folique. Il est à jour de ses vaccinations. • Il est fébrile à 38,2°C. L'auscultation pulmonaire est normale, fréquence respiratoire à 18/min. pression artérielle 110/60 mm Hg. Les leucocytes sont à 20 000/mm3 dont 18 000/mm3 polynucléaires neutrophiles, Hb 7,7 g/dl (Hb de base à 8,5 g/dl), Plaquette 550 000/mm3, CRP 200 mg/L.
Q1/ Quelle est votre prise en charge aux urgences la première heure? (0 à plusieurs bonnes réponses possibles) • Antalgie par morphine IV • Débuter des antibiotiques type céphalosporines de 3° génération • Hydrater le patient en IV • Transfuser le patient en culots globulaires • Réaliser des hémocultures et un examen bactériologique urinaire
Q2/ Après 7 jours d'hospitalisation, les douleurs se sont localisées depuis 2 jours sur le tibia où vous sentez une voussure sur la crête tibiale, très douloureuse à la palpation. La zone est très inflammatoire. Il existe des pics fébriles le soir à 39°C. Vous suspectez une ostéomyélite. Quel est votre attitude? (0 à plusieurs bonnes réponses possibles) • Je débute des antibiotiques couvrant le staphylocoque et les bacilles gram négatifs • Je prélève des hémocultures • Je tente une ponction à l'aveugle de la zone prétibiale à visée bactériologique • Je transfère le patient en réanimation • J'envisage une transfusion globulaire
Q3/ Finalement une hémoculture est positive pour salmonella sp sensible. Quel diagnostic retenez-vous et quelle est votre prise en charge ? • Il s'agit probablement d'une ostéomyélite du tibia à salmonelle • Il s'agit probablement d'une crise localisée associée à une gastroentérite à salmonelle • Il faut rechercher une porte d'entrée digestive par une coloscopie • Il faut réaliser systématiquement une échographie biliaire • Un traitement par fluoroquinolone d'environ 6 semaines sera proposé
You can also read