2020 Symposia Series 1 - Practicing Clinicians Exchange
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
2020 Symposia Series 1
Optimizing Outcomes in Moderate to Severe Asthma: Utilizing Biologic Therapy for Individualized Treatment
Learning Objectives
• Recognize phenotypic variations and subtypes that can characterize
uncontrolled asthma
• Identify indications for add-on biologic therapy based on disease- and
patient-centered factors
• Implement techniques to increase treatment adherence for improved
patient outcomes
3
GINA Guidance on Asthma in the Context of COVID-19
• Avoid spirometry in patients with confirmed or suspected COVID-19
‒ If community transmission of the virus is occurring, postpone spirometry and
peak flow measurement within healthcare facilities unless urgently needed
‒ Follow contact and droplet precautions
• Avoid nebulizers whenever possible
‒ Pressurized MDI via spacer is preferred during severe exacerbations, with a
mouthpiece or tightly fitting face mask if required
• Use strict infection control measures if aerosol-generating procedures are needed
‒ Examples: nebulization, oxygen therapy (including with nasal prongs), sputum
induction, manual ventilation, noninvasive ventilation, and intubation
GINA = Global Initiative for Asthma; MDI = metered-dose inhaler.
Global Initiative for Asthma. www.ginasthma.org. Accessed Apr 23, 2020. 4Asthma Is a Common Chronic Lung Disorder • Affects 19.0 million (7.7%) US adults and 5.5 million (7.5%) US children under the age of 18 • A heterogeneous disease ‒ Typically begins in childhood ‒ Can also develop in adulthood, predominantly in women over the age of 40 • Significant economic burden in the US—over a 5-year period (2008-2013), asthma was the cause of: ‒ $3 billion in losses due to missed work/school ‒ $29 billion due to asthma-related morbidity ‒ $50.3 billion in medical costs Centers for Disease Control and Prevention. www.cdc.gov/nchs/fastats/asthma.htm. Accessed Apr 24, 2020; Nurmagambetov T, et al. Ann Am Thorac Soc. 2018;15:348-356; Sood A, et al. Ann Am Thorac Soc. 2013;10:188-197. 5
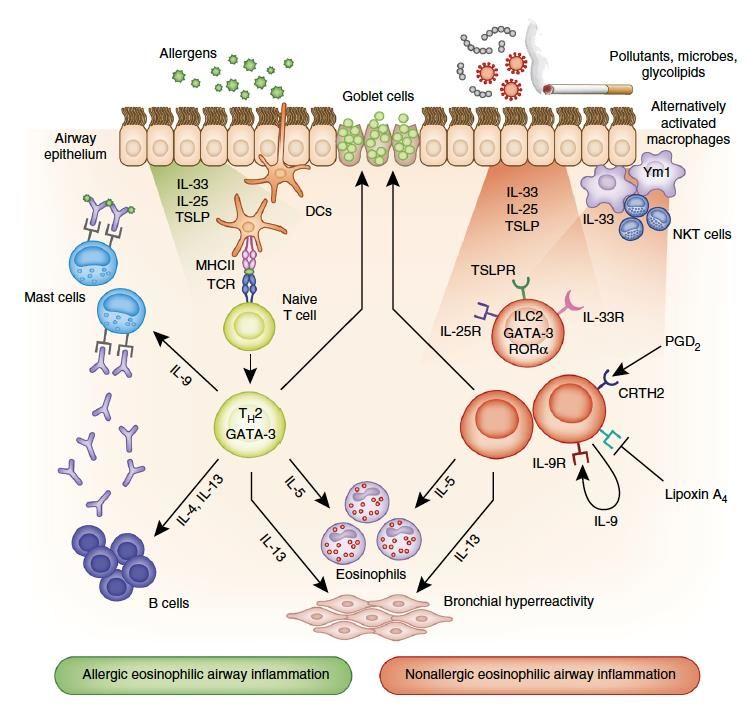
Asthma Is Highly Heterogeneous
and Driven by Inflammation
Type 2 Inflammation
• Asthma is caused by chronic airway FeNO
inflammation, which may lead to:
‒ Airway hyperresponsiveness NO
NO
‒ Obstruction/airflow limitation
• Type 2 inflammation is characterized by
presence of IL-4, IL-5, IL-13, and eosinophils
• Non-type 2 inflammation includes neutrophilic,
IgE
mixed, and paucigranulocytic inflammation
(few cells)
DC = dendritic cell; TH2 = T-helper type 2; NKT = natural killer T cell;
TSLP = thymic stromal lymphopoietin.
Israel E, et al. N Engl J Med. 2017;377:965-976; Lambrecht BN, et al. Nat Immunol.
2015;16:45-56; National Heart, Lung, and Blood Institute.
www.ncbi.nlm.nih.gov/books/NBK7232/pdf/ From Lambrecht BN, et al. Nat Immunol. 2015;16:45-56.
Bookshelf_NBK7232.pdf. Accessed Apr 24, 2020. 6Asthma Phenotypes
Phenotype Description
Allergic asthma Most easily recognized; often starts in childhood; associated with history of allergic disease;
sputum often has eosinophilic airway involvement; responds well to ICS treatment
Late-onset asthma Adult-onset, particularly in women; nonallergic; often requires higher doses of ICS or is
refractory to corticosteroids; has sputum eosinophilia; may coexist with chronic rhinosinusitis
with nasal polyps
Asthma with fixed In patients with long-standing asthma, fixed airflow limitation may develop due to airway
airflow limitation remodeling
Asthma with obesity Prominent respiratory symptoms associated with obesity; little eosinophilic airway
inflammation
Asthma-COPD Persistent airflow limitation with clinical features of both asthma and COPD
overlap
Chung KF, et al. Eur Respir J. 2014;43:343-373; Global Initiative for Asthma. www.ginasthma.org. Accessed Apr 23, 2020. 7Evidence-based Asthma Guidelines
• National Asthma Education and
Prevention Program Expert Panel Report-3
‒ 2007
• Global Initiative for Asthma
‒ Updated 2020
• National Asthma Education and Prevention
Program Expert Panel Report-4
‒ TBA
8Case Study: Amelia
• African American woman, age 52
• Editor at a major publishing house
• BMI: 25 kg/m2
• Married with 3 children
• Family history of elevated cholesterol and heart disease
• Medical history
‒ High LDL-C, managed with atorvastatin
‒ Hypothyroidism, managed with thyroxine replacement
‒ Chronic rhinosinusitis with nasal polyps, managed with intranasal
steroids
LDL = low-density lipoprotein cholesterol. 9Case Study (cont’d): Amelia Was Diagnosed With Asthma 1 Year Ago
• Initially presented 1 year ago with Physical Exam
wheezing and shortness of breath Pulmonary Clear to auscultation
Moderate wheeze on forced
‒ After exercising expiration
‒ With exposure to cigarette smoke ENT No polyps visible
or strong perfumes PFT Results
‒ Sometimes awakened at night FEV1/FVC ratio 69%
• Complained of chest tightness that FEV1 59% of predicted
worsened when walking the dog Bronchodilator FEV1 by 15% and 300 mL
response
• Based on clinical and PFT findings,
• An increase in FEV1 by ≥200 mL and ≥12% after
Amelia was diagnosed with asthma using albuterol confirms a diagnosis of asthma
FVC = forced vital capacity; PFT = pulmonary function test; SpO2 = peripheral capillary oxygen saturation. 10Differentiating Asthma From Other Disorders
Age Condition Findings
40+ years Bronchiectasis Productive cough, recurrent infections
Cardiac failure Dyspnea with exertion, nocturnal symptoms
Central airway obstruction Dyspnea, unresponsive to bronchodilators
COPD Cough, sputum, dyspnea on exertion, smoking or noxious
exposure
GERD Heartburn, epigastric or chest pain, dry cough
Hyperventilation, dysfunctional Dizziness, paresthesia, sighing
breathing
Medication-related cough Treatment with ACE inhibitor
Parenchymal lung disease Dyspnea with exertion, nonproductive cough, finger clubbing
Pulmonary embolism Sudden onset of dyspnea, chest pain
Vocal cord dysfunction Dyspnea, inspiratory wheezing (stridor)
Each of these may also be found together with asthma.
ACE = angiotensin converting enzyme.
Global Initiative for Asthma. www.ginasthma.org. Accessed Apr 23, 2020. 11GINA: Stepwise Management for Pharmacotherapy
Symptoms most
Short course OCS may be needed
days, waking ≥1x
for severely uncontrolled asthma
per week, or low
Symptoms most lung function
days, or waking STEP 5
Symptoms ≥2x per month, ≥1x per week
Symptoms High-dose
butGoals of Management: GINA Global Strategy
• Long-term management goals Control-based Asthma Management Cycle:
At Every Patient Visit
‒ Achieve good symptom control and
maintain normal activity levels
Assess
‒ Eliminate future risk of exacerbations,
fixed airflow limitation, and AEs
‒ Avoid use of OCS as daily controller
• Also important Review Adjust
‒ Take patient’s own goals into account Response Treatment
‒ Manage comorbidities, consult other
specialists as needed
AE = adverse event; OCS = oral corticosteroid.
Global Initiative for Asthma. www.ginasthma.org. Accessed Apr 23, 2020. 13Case Study (cont’d): Amelia’s Asthma Treatment History
• At diagnosis, started on daily low-dose ICS maintenance therapy; prescribed an albuterol
inhaler for rescue therapy (GINA step 2)
• Stepped up over the next 12 months due to insufficient control of her asthma symptoms
Amelia is currently being treated at GINA Step 4
• Fluticasone/salmeterol DPI, 1 inhalation of 250 µg/50 µg, twice daily (medium dosage)
• Albuterol rescue inhaler as needed
• Last week, on a cold dry evening when the fireplace was in use, she had an exacerbation
‒ Had chest tightening, wheezing, and trouble breathing; albuterol did not help
‒ Went to the ED, where she received a bronchodilator and a prednisone burst and was
told to follow up with you
DPI = dry powder inhaler. 14How to Assess Asthma Control
• According to GINA, “the level of asthma control is the extent to which the
manifestations of asthma can be observed in the patient, or have been
reduced or removed by treatment”
‒ Assessed retrospectively after a trial of asthma controller(s)
for ≤3 months
• Asthma control includes both:
‒ Symptom control (current clinical control) and
‒ Eliminating future risk, particularly exacerbations
Global Initiative for Asthma. www.ginasthma.org. Accessed Apr 23, 2020. Louie S. Consultant. 2018;58:336-342. 15Case Study (cont’d): Assessing Amelia’s Asthma
Control Using the ACT™
• Can be self- In the past 4 weeks… 1 2 3 4 5 SCORE
administered 1. How much time did your asthma keep
you from getting as much done at work, All Most Some A little None 3
• Possible total school, or home?
2. How often have you had shortness of >1x per 3 to 6x per 1 to 2x per
score of 25 breath? day
1x per day
week week
Not at all 2
• If total score is 3. How often did your asthma symptoms
wake you up at night or earlier than usual in ≥4 nights
2 to 3
1x per
≤19, asthma is the morning? per week
nights per
week
week
1x or 2x Not at all 1
not controlled 4. How often have you used your rescue
≥3x per 1 to 2x per 2 or 3x per
inhaler or nebulizer (such as albuterol)? ≤1x week Not at all 2
day day week
5. How would you rate your asthma control Not
Poorly Somewhat Well Completely
during the past 4 weeks? controlled
controlled controlled controlled controlled 1
at all
TOTAL 9
Copyright 2002, by QualityMetric Incorporated. Asthma Control Test is a trademark of QualityMetric Incorporated.
Nathan RA, et al. J Allergy Clin Immunol. 2004;113:59-65. 16Case Study (cont’d): Amelia’s Asthma Action Plan—
A Strategy to Address Short-term Changes
DOING WELL (Green Zone) Use these daily controller medicines:
You have all of these: Medicine How Much How Often/When
• You prescribe Amelia a • Breathing well Peak flow:
ICS-LABA 2 inhalations Once in AM, once in PM
• No cough or wheeze 440 to 351
• Sleep through the night
peak flow meter as part • Can work and play
For asthma with exercise: Albuterol; 1 inhalation, then wait 1 min & take
another
of her action plan CAUTION (Yellow Zone) Continue with green zone medicine and add:
• You show her how to You have any of these:
• First signs of a cold
Medicine How Much How Often/When
Albuterol 1 inhalation 1x, then wait 1 min and take another
• Exposure to known trigger
use it and instruct her • Cough CALL YOUR ASTHMA CARE PROVIDER.
• Mild wheeze Peak flow:
on how to interpret the • Tight chest 350 to 220
• Coughing at night
results based on her
DANGER (Red Zone) Take these medicines and call your provider now:
personal best result of Your asthma is getting worse fast: Medicine How Much How Often/When
• Medicine not helping
440 L/min • Breathing hard and fast
Albuterol 1 inhalation 1x, then wait 1 min and take another
• Nose opens wide Peak flow:
• Trouble speaking Prednisone 3 10-mg tablets 1x a day for 5 days
Below 220
• Ribs show (in children)
CALL YOUR ASTHMA CARE PROVIDER RIGHT AWAY.
If you cannot contact your provider, go directly to the ED.
DO NOT WAIT.
Asthma and Allergy Foundation of America. www.aafa.org/asthma-treatment-action-plan. Accessed Apr 24, 2020; Gibson PG, et al.
Thorax. 2004;59:94-99. 17Role of the Asthma Action Plan • A written asthma action plan helps patients recognize and respond to worsening asthma in the short term • Should include when, how, and for how long to increase treatment and when to seek medical help • Supports patient education and provides a consistent approach • It is also important for patients to understand and avoid potential triggers to prevent exacerbations Asthma and Allergy Foundation of America. www.aafa.org/asthma-treatment-action-plan. Accessed Apr 24, 2020; Gibson PG, et al. Thorax. 2004;59:94-99. 18
Risk Factors That Increase the Likelihood of Exacerbations
• Uncontrolled asthma symptoms • Major psychological or socioeconomic problems
• Frequent SABA use • Exposures
‒ Mortality increased if more than one 200-dose ‒ Smoking, allergen exposure (if sensitized)
canister used/month • Comorbidities
• Suboptimal ICS ‒ Obesity, chronic rhinosinusitis, confirmed
‒ Not prescribed, poor adherence, incorrect food allergy
inhaler technique • Pregnancy
• Low FEV1 • History of being intubated or in ICU for asthma
‒ Especially ifBefore Considering Any Step Up in Treatment
• Assess whether the following problems may be the cause of persistent
symptoms or exacerbations:
‒ Incorrect inhaler technique
‒ Poor adherence
‒ Persistent exposure to agents such as allergens, tobacco smoke, air
pollution, or to medications such as β-blockers or NSAIDs
‒ Comorbidities that might contribute to respiratory symptoms and poor QoL
‒ Incorrect diagnosis
QoL = quality of life.
Global Initiative for Asthma. www.ginasthma.org. Accessed Apr 23, 2020. 20It’s Important to Teach Good Inhaler Technique:
Errors Are Common and a Major Risk for Poor Control
Common errors with inhaler techniques
MDI DPI BAMDI MDI + spacer
60%
48%
Mean Percentage
50% 45% 44% 46% 46%
37% 39% 38%
40% 33% 34%
30% 32% 33%
29%
30%
22%
20% 18%
10%
0%
0%
• Not exhaling fully before inhaling the medication is a common error with traditional MDIs and DPIs
BAMDI = breath-actuated metered-dose inhaler.
Sanchis J, et al. Chest. 2016;150:394-406. 21Case Study (cont’d): Investigating Risk Factors That Could
Contribute to Poor Control
Before stepping up treatment, you asked Amelia:
• Has she been using her inhaler as directed? (yes)
• Can she demonstrate proper inhaler technique right now? (she does)
• Has she had any problems with allergies? (no, she has never had allergies)
• Has she been exposed to any new irritants (yes, smoke from the fireplace, cold air); these
may have triggered her recent exacerbation
Management plan: Move from GINA Step 4 to GINA Step 5
• You increase her dosage of fluticasone/salmeterol to 1 inhalation of 500 µg/50 µg, twice
daily (high-dose ICS, salmeterol dose unchanged)
• You add the LAMA tiotropium to her regimen 3 weeks later because her symptoms are still
not controlled
22Case Study (cont’d): 4 Weeks Later, Amelia Has Another
Asthma Exacerbation, Leading to Hospitalization
• Four weeks after you last saw Amelia, she had a respiratory infection but
didn’t notify you at the time
• Coughing, wheezing, and chest tightness worsened
‒ Used the albuterol rescue inhaler but still had trouble breathing
‒ Self-monitored peak flow was 200 L/min
• She went to the ED and was admitted to the hospital due to continued
wheezing and physical exhaustion despite bronchodilator therapy
• Given a prednisone burst and was discharged with a 14-day taper
23Risks Associated With OCS Use
• AEs are particularly common and problematic with long-term use of OCS
Adverse Effects of Long-term OCS Use
Obesity Hypertension
Diabetes Adrenal suppression
Osteoporosis Depression
Cataracts Anxiety
• Frequent short-term use of OCS is associated with sleep disturbances and
increased risk of infection, fracture, and thromboembolism
Global Initiative for Asthma. www.ginasthma.org. Accessed Apr 23, 2020. 24GINA Control-based Asthma Management Cycle
• Confirm diagnosis
• Symptom control, risk factors
Assess (including lung function)
• Comorbidities
• Inhaler technique, adherence
• Patient goals
• Symptoms • Medications
• Exacerbations
Review Adjust • Nonpharmacologic
• AEs Response Treatment approaches
• Patient satisfaction • Modifiable risk factors
• Lung function • Education & skills
training
Global Initiative for Asthma. www.ginasthma.org. Accessed Apr 23, 2020. 25Case Study (Cont’d): You Refer Amelia to an Asthma Specialist • After she is discharged, Amelia notifies you that she was admitted to the hospital • You decide to refer her to an asthma specialist When To Consider Referral • Difficulty confirming asthma diagnosis • Persistent uncontrolled asthma or frequent exacerbations • Evidence of, or risk for, significant treatment-related AEs (systemic corticosteroids) • Suspected occupational asthma • Symptoms suggesting complications or subtypes of asthma • Any risk factors for asthma-related death Global Initiative for Asthma. www.ginasthma.org. Accessed Apr 23, 2020. 26
Assessing Whether a Patient Has Type 2 or Non-Type 2
Inflammation
• Type 2 inflammation should be considered if the patient has any of the
following while on high-dose ICS or daily OCS*:
Blood eosinophils ≥150/µL and/or
FeNO ≥20 ppb and/or
Sputum eosinophils ≥2% and/or
Asthma is clinically allergen-driven (allergen-specific IgE)
*OCS often suppresses markers of type 2 inflammation; these tests should be performed before starting OCS or on the lowest possible dose.
Global Initiative for Asthma. www.ginasthma.org. Accessed Apr 24, 2020. 27Case Study (cont’d): Amelia Is Evaluated by an Asthma Specialist
• Asthma specialist confirms: Laboratory Results
‒ Asthma as the diagnosis Parameter Amelia’s Results Reference
‒ Adherence and inhaler FEV1/FVC 65% ≥70%
technique FEV1 58% of predicted ≥80% of predicted
• Further evaluates markers
Total serum IgE 85 IU/mLCase Study (cont’d):
Next Steps in Amelia’s Stepwise Management
STEP 5 Evidence of Type 2 Inflammation No Evidence of Type 2 Inflammation
High-dose ICS-LABA
• Consider clinical type 2 phenotype for • Add-on treatment options include:
Refer for phenotypic which specific add-on treatment is − Tiotropium
assessment ±
available
add-on therapy, − Leukotriene modifier
eg, tiotropium, anti-IgE, • Add-on biologic options include:
anti-IL5/5R, anti-IL4R − Low-dose macrolide
‒ Anti-IgE
− Low-dose OCS (≤7.5 mg/day
‒ Anti-IL-5/5R prednisone equivalent)
Add low-dose OCS
but consider side ‒ Anti-IL-4R/IL-13R − Consider bronchial thermoplasty
effects
with registry enrollment
Additional steps
• Healthy diet • Manage emotional stress
• Vaccinations • Pulmonary rehab
Global Initiative for Asthma. www.ginasthma.org. Accessed Apr 23, 2020; Israel E, et al. N Engl J Med. 2017;377:965-976. 29Biologic Targets in Severe Asthma
Dupilumab Dupilumab
IL-4R/
IL-13R IL-4R
IL-4 IL-13
APC Th0 Cell Th2 Cell B Cell
Mepolizumab IL-5
Reslizumab
IgE
Benralizumab
IL-5R Omalizumab
Eosinophil
APC = antigen-presenting cell.
Adapted from: Bice JB, et al. Ann Allergy Asthma Immunol. 2014;112:108-115; Ziegler SF, et al. Nat Immunol. 2010;11:289-293. 30How Do Biologics Improve Asthma Control? • Prevent exacerbations • Reduce symptoms • Improve lung function • Decrease need for systemic corticosteroids Busse WW. Allergol Int. 2019;68:158-166; Cataldo D, et al. J Asthma. 2020;1-11. 31
Anti-IgE Biologic: Omalizumab
Indication(s) Warnings and Precautions Most Common AEs
• Moderate to severe persistent asthma in patients • Anaphylaxis • Muscle aches
≥6 years with: • Hypersensitivity reactions • Joint aches
‒ Positive skin test or in vitro reactivity to • Malignancy • Fatigue
perennial aeroallergen • Acute asthma symptoms • Injection site reaction
‒ Symptoms inadequately controlled with ICS • Abrupt corticosteroid reduction • Severe allergic
• Chronic idiopathic urticaria in patients ≥12 years who • Eosinophilic conditions reactions (rare)
remain symptomatic despite H1 antihistamine • Fever, arthralgia, rash
treatment • Parasitic (helminth) infection
• Because of the risk of anaphylaxis, omalizumab must be administered in a clinic or infusion center, and patients taking it
should carry an epinephrine pen auto-injector
Cleveland Clinic. my.clevelandclinic.org/health/treatments/17711-biologic-therapy-for-severe-asthma. Accessed Apr 24, 2020; Jackson K, et al. Expert
Rev Clin Immunol. 2020;16:311-319; US Food and Drug Administration. www.accessdata.fda.gov/scripts/cder/daf/index.cfm. Accessed Apr 24, 2020. 32Anti-IL-4R/IL-13R Biologic: Dupilumab
Indication(s) Warnings and Precautions Most Common AEs
• Maintenance Rx in patients ≥12 years with moderate • Hypersensitivity reactions • Sore throat
to severe asthma with: • Conjunctivitis and keratitis • Injection site reaction
‒ An eosinophilic phenotype or • Eosinophilic conditions • Elevated eosinophil
‒ OCS-dependent asthma • Acute asthma symptoms or level
• Maintenance Rx in adults with inadequately controlled deteriorating disease • Severe allergic
chronic rhinosinusitis with nasal polyposis • Abrupt reduction of reactions (rare)
• Treatment of patients ≥12 years with moderate to severe corticosteroid dosage
atopic dermatitis not adequately controlled with topical • Parasitic (helminth)
prescription therapies or when those therapies are not infections
advisable
• Based on clinical trial experience, dupilumab is typically used in patients with eosinophils ≥150 cells/µ L
• Is administered subcutaneously and can be given as a self-injection at home
Busse WW. Allergol Int. 2019;68:158-166; Cleveland Clinic. my.clevelandclinic.org/health/treatments/17711-biologic-therapy-for-severe-asthma.
Accessed Apr 24, 2020; US Food and Drug Administration. www.accessdata.fda.gov/scripts/cder/daf/index.cfm. Accessed Apr 24, 2020. 33Anti-IL-5R Biologic: Benralizumab
Indication(s) Warnings and Precautions Most Common AEs
• Maintenance Rx of patients • Hypersensitivity reactions • Headache
≥12 years with severe asthma and with • Acute asthma symptoms or • Sore throat
an eosinophilic phenotype deteriorating disease • Severe allergic
• Abrupt reduction of corticosteroid reaction (rare)
dosage
• Parasitic (helminth) infections
• Based on clinical trial experience, benralizumab is typically used in patients with eosinophils ≥300 cells/µL
• Is administered subcutaneously and can be given as a self-injection at home
Busse WW. Allergol Int. 2019;68:158-166; Cleveland Clinic. my.clevelandclinic.org/health/treatments/17711-biologic-therapy-for-severe-asthma.
Accessed Apr 24, 2020; US Food and Drug Administration. www.accessdata.fda.gov/scripts/cder/daf/index.cfm. Accessed Apr 24, 2020. 34Anti-IL-5 Biologic: Mepolizumab
Indication(s) Warnings and Precautions Most Common AEs
• Maintenance Rx of patients • Hypersensitivity reactions • Headaches
≥6 years with severe asthma and with • Acute asthma symptoms or • Injection site reactions
an eosinophilic phenotype deteriorating disease • Back pain
• Rx of adults with eosinophilic • Opportunistic infections: herpes • Weakness
granulomatosis with polyangiitis zoster • Fatigue
• Abrupt reduction of corticosteroid • Severe allergic
dosage reactions (rare)
• Parasitic (helminth) infections
• Based on clinical trial experience, mepolizumab is typically used in patients with eosinophils ≥150 cells/µL
• Is administered subcutaneously and can be given as a self-injection at home
Busse WW. Allergol Int. 2019;68:158-166; Cleveland Clinic. my.clevelandclinic.org/health/treatments/17711-biologic-therapy-for-severe-asthma.
Accessed Apr 24, 2020; Emma R, et al. Ther Adv Respir Dis. 2018;12:1753466618808490; US Food and Drug Administration.
www.accessdata.fda.gov/scripts/cder/daf/index.cfm. Accessed Apr 24, 2020. 35Anti-IL-5 Biologic: Reslizumab
Indication(s) Warnings and Precautions Most Common AEs
• Maintenance Rx of patients • Anaphylaxis • Sore throat
≥18 years with severe asthma and with • Acute asthma symptoms or • Muscle aches
an eosinophilic phenotype deteriorating disease • Severe allergic
• Malignancy reactions (rare)
• Abrupt reduction of corticosteroid
dosage
• Parasitic helminth infection
• Based on clinical trial experience, reslizumab is typically used in patients with eosinophils ≥400 cells/µL
• Because of the risk of anaphylaxis, it must be administered in a clinic or infusion center
• Administration is weight-based; thus, it can be considered for obese patients, especially if eosinophil
levels remain elevated on other therapies
Busse WW. Allergol Int. 2019;68:158-166; Cleveland Clinic. my.clevelandclinic.org/health/treatments/17711-biologic-therapy-for-severe-asthma.
Accessed Apr 24, 2020; US Food and Drug Administration. www.accessdata.fda.gov/scripts/cder/daf/index.cfm. Accessed Apr 24, 2020. 36Case Conclusion
• Given Amelia’s blood eosinophilia (220 cells/µL), FeNO level (55 ppb), and history of
chronic rhinosinusitis with nasal polyps, asthma specialist recommends adding
dupilumab to current high-dose ICS-LABA, tiotropium, and intranasal steroid regimen
‒ She says that her asthma is now “well controlled” and that she’s staying in the
“green zone” of her action plan
‒ ACT score is now 21
‒ Rhinosinusitis and nasal polyposis improved
• Amelia will be evaluated every 2 weeks initially, with instructions to contact you or
the asthma specialist if symptoms worsen
• Treatment with high-dose ICS-LABA may be decreased in 3 to 6 months if she
continues to do well; tiotropium may not be needed; dupilumab to be continued
37PCE Action Plan
✓ Use an evidence-based, stepwise approach such as GINA as a guide to
control symptoms and minimize future risk
✓ Help your patients write an asthma action plan that is tailored to their
individual needs
✓ If a patient has persistent symptoms and/or exacerbations despite 2 to 3
months of controller therapy, correct common problems before stepping up
treatment
✓ Avoid long-term or frequent OCS use due to the risk of AEs
PCE Promotes Practice Change
382020 Symposia Series 1
You can also read

















































