Managing thyrotoxicosis in the acute medical setting
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
44 Acute Medicine 2018; 17(1): 44-48
Review Article
Managing thyrotoxicosis in the acute
medical setting
Thyrotoxicosis is common and can present in although symptomatic management can be instigated
numerous ways with patients exhibiting a myriad in the acute setting. Table 1 summarises the causes
of symptoms and signs. It affects around 1 in 2000 of thyrotoxicosis.
people annually in Europe1. The thyroid gland In the acute setting, it is important to recognise
produces two thyroid hormones - thyroxine (T4) that elderly patients with thyrotoxicosis may have a
and triiodothyronine (T3). Thyroxine is inactive and subtle presentation with fewer typical symptoms and
is converted by the tissues and organs that need it signs; apathy and apparent depression may be the only
into tri-iodothyronine. In health, the production of clinical features. In any patient, symptoms of rapid
these thyroid hormones is tightly regulated by the onset (1-2 days duration) are more likely to suggest
secretion of thyroid stimulating hormone (TSH; a diagnosis of thyroiditis rather than GD or nodular
thyrotropin) from the pituitary gland. The term thyroid disease. All patients with unexplained weight
‘thyrotoxicosis’ refers to the clinical manifestations loss, tachycardia or atrial fibrillation (AF) should
of hyperthyroidism. have a diagnosis of thyrotoxicosis considered.
Linking clinical presentation to Clinical features of hyperthyroidism
aetiology Symptoms of thyrotoxicosis are often nonspecific
The commonest cause of hyperthyroidism in and patients may present in numerous ways2,4,5. In
the UK is Graves’ disease (GD), which accounts GD, onset is often gradual and poorly defined; most
for around 75% of cases of thyrotoxicosis2. GD individuals have felt unwell for 3 to 6 months before
exhibits a particularly strong female preponderance they seek medical attention. If the onset of thyrotoxic
(F:M, 6:1), in common with other autoimmune symptoms is rapid or can be pinned down to a single
disorders. It usually presents between 30-50 years day or a few days, the diagnosis is much more likely
of age, but can occur in both sexes and at any age. to be thyroiditis.
Other common causes are a single toxic nodule or a In GD, the commonest precipitant of
multinodular goitre, and together, GD and nodular thyrotoxicosis, weight loss (despite an increase in
thyroid disease account for well over 90% of all cases appetite) is found in most patients. In a minority,
of hyperthyroidism. Nodular thyroid disease is more the increase in appetite coupled with the free
often seen with advancing age. Histologically these availability of calorie-dense food, leads to weight
nodules are follicular adenomas and excess thyroid gain. Pervasive exhaustion is common but patients
hormone is secreted in an unregulated manner. Rarer may find this alternates with periods of restlessness
causes of thyrotoxicosis include subacute, silent and hyperactivity. Heat intolerance is a typical feature
or post-partum thyroiditis; these conditions occur and sweating at night is characteristic. Poor sleep with
when inflammatory destruction of thyroid follicles mental overactivity and physical hyperkinesis is often
causes a release of preformed thyroid hormones into found. Palpitations at rest or on minimal exertion or
the circulation, resulting in transient thyrotoxicosis. shortness of breath during light exercise are common
Subacute thyroiditis is usually caused by a viral at all ages. Intestinal transit-time is shortened, leading
infection and is characterised by fever and pain or to more frequent defecation. Menstrual bleeding may
thyroid tenderness. Painless thyroiditis can occur
during or after treatment with lithium, cytokines (e.g. Table 1. Causes of Thyrotoxicosis
interferon alpha), tyrosine kinase inhibitor therapy, Causes of thyrotoxicosis
highly active retroviral therapy or in the postpartum Autoimmune thyroid disease
C Napier
MBBS MRCP (UK) period and appears with differing frequency between •• Graves’ disease
Endocrine Unit, Royal studied populations3. A destructive (but nevertheless Nodular thyroid disease
Victoria Infirmary, painless) thyroiditis occurs in 5-10% of patients on •• Solitary toxic nodule
Queen Victoria Road, amiodarone3. Abnormal thyroid biochemistry (with •• Multinodular goitre
Newcastle Upon Tyne, Thyroiditis
or without symptoms) is becoming more common
NE1 4LP •• Viral
UK with the wider use of biological therapies to treat
cancer or other conditions. Almost all patients with •• Post-partum
Email: c.napier2@newcastle.
•• Drug-induced
ac.uk thyroiditis should be referred for endocrine input,
© 2018 Rila Publications Ltd.Acute Medicine 2018; 17(1): 44-48 45
Managing thyrotoxicosis in the acute medical setting
Table 2. Symptoms and Signs of Thyrotoxicosis
Symptoms and signs of thyrotoxicosis
SYMPTOMS SIGNS
Tremor Tremor
Palpitations Palmar erythema
Fatigue Onycholysis
Heat intolerance Tachycardia
Weight loss Atrial fibrillation
Breathlessness Brisk reflexes
Increased frequency of defecation Orbitopathy* – proptosis, eyelid retraction
Anxiety Goitre – smooth or nodular
Muscle aches Thyroid bruit
Menstrual disturbance Hypertension and signs of cardiac failure
Weight loss
Pretibial myxoedema*
*Signs only seen in Graves’ disease
be light, decreased in frequency, or absent. Thyroid plaques on the shin or dorsum of the foot. Signs of
tenderness or pain is not a feature. Less commonly GO include lid retraction, lid or conjunctival redness,
reported symptoms are thirst, nausea, generalised itch, periorbital oedema and proptosis. Rare signs of GD
and hair loss. In 5–10% of people, the first symptoms include chorea, onycholysis, or acropachy of the nails.
are due to Graves’ orbitopathy (GO) with itchy,
gritty, or watering eyes, or an abnormal appearance6. Investigations in hyperthyroidism
Thyrotoxicosis with extra-thyroidal features, such as Hyperthyroidism can be easily and quickly
orbitopathy or pretibial myxoedema, is pathognomic confirmed on biochemical testing with elevation
of GD. In the elderly, there may be little to suggest a of one or both serum-free thyroid hormones (FT3,
diagnosis of hyperthyroidism, or the onset of AF may FT4) together with a low or undetectable TSH.
precipitate a cardiac presentation with dyspnea and/ Serum TSH measurement has the highest sensitivity
or congestion. and specificity of any single blood test used in the
Table 2 lists the symptoms and signs of evaluation of suspected thyrotoxicosis and should
thyrotoxicosis. During clinical assessment, a thyrotoxic be used as an initial screening test3. However, when
patient may struggle to sit still, with constant fidgeting there is strong clinical suspicion of thyrotoxicosis,
and apparent anxiety or apprehension. The face, neck, it is much more pragmatic to combine TSH testing
and upper chest wall may be flushed. The palms may with measurement of free thyroid hormones for
be warm and sweaty, with a symmetrical fine tremor diagnostic accuracy3. About 5% of subjects, most
when hands are outstretched. In GD, a smooth, diffuse commonly elderly, present with elevation of FT3
goitre can be visible or palpable, with a systolic phase alone, with normal FT4 and undetectable TSH -
bruit audible over the gland due to increased blood this ‘T3 thyrotoxicosis’ is often a manifestation of
flow. In nodular thyroid disease, a discrete nodule or relatively mild hyperthyroidism. Elevation of free T4
uneven, multinodular goitre may be easily palpable. alone, with normal free T3 and undetectable TSH,
Patients with subacute thyroiditis may complain of may be found in someone with co-existing major
tenderness on palpation. In all thyrotoxic patients, illness (a combination of thyrotoxicosis and sick-
tachycardia (unless beta-blockers are already being euthyroid syndrome), but is also typical of iodine-
taken) and rapid atrial fibrillation may be present, with induced thyrotoxicosis or exogenous levothyroxine
an elevated systolic blood pressure. Hepatomegaly use. If there is doubt about the chronicity or severity
or splenomegaly may be found. Hyperreflexia is of symptoms, then it is good practice to repeat the
common and proximal musculature can be weak. abnormal thyroid function tests after a short period,
Late features of thyrotoxicosis are frank spasticity as a rapid fluctuation may be the clue to the diagnosis
and pseudobulbar paresis. Rapid onset of severe and of destructive (silent) thyroiditis. If the TSH is low
generalized muscle weakness should raise suspicion but still detectable, the diagnosis is almost certainly
of the possibility of hypokalemic periodic paralysis, a not GD and further investigations are needed7.
syndrome most common in men of Asian descent that Individuals with a persistently undetectable TSH
is precipitated by thyrotoxicosis. but normal free thyroid hormones (in the absence
In GD, pretibial myxoedema (infiltrative of pituitary disease and drug effects) are said to have
dermopathy) is usually manifest as discrete violaceous subclinical hyperthyroidism (SH) and need further
© 2018 Rila Publications Ltd.46 Acute Medicine 2018; 17(1): 44-48
Managing thyrotoxicosis in the acute medical setting
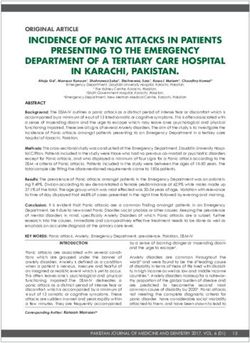
negative or if a nodular thyroid is found on palpation,
Symptoms or signs of thyrotoxicosis but the decision about the indication for imaging
and optimum imaging modality should ideally be
left until the time of endocrine review. Although
an ultrasound examination may demonstrate a
single nodule or a multinodular goitre, radionuclide
imaging with either technetium (99 Tc) or iodide
If TSH low or undetectable with elevated (123 I) is often more useful because it gives practical
FT4 +/- FT3 data regarding the presence and distribution of
functioning thyroid tissue.
Other investigations, often routinely done on
medical admission, will be worthwhile depending
upon the clinical situation and likely treatment
plan. An ECG should be documented in all
Start beta
Refer to thyrotoxic patients with tachycardia and a more
blockers if
endocrinology; detailed cardiac evaluation should be performed in
symptomatic or
send TRAb those with AF. A full blood count with a white cell
tachycardic*
differential at baseline is helpful if antithyroid drug
(ATD) treatment may be instigated in the future.
A pregnancy test should be documented in women
of childbearing age and a negative pregnancy test is
absolutely mandatory if radioiodine treatment is later
Discharge unless features of thyroid storm the chosen treatment modality.
or clinically unwell** In thyrotoxic patients, microcytosis, elevation
of serum alkaline phosphatase, and mildly deranged
Figure 1. Algorithm for Managing Suspected liver enzymes are often found on biochemical testing;
Thyrotoxicosis on the Acute Medical Unit
* If any contraindications to beta blockade, diltiazem can
mild hypercalcemia can also be present.
be used as an alternative Figure 1 outlines a suggested algorithm for the
** Patients with AF will need consideration re. investigation of patients with suspected thyrotoxicosis.
anticoagulation
Managing hyperthyroidism
investigation (i.e., serum thyroid antibodies, Holter
monitor, DEXA bone scan)7. There is little clear Symptomatic management
evidence to guide treatment in this situation and All thyrotoxic patients should gain symptomatic
intervention depends on the degree of SH and the benefit from beta blockade (Propranolol 40mg TDS
sequelae7,8 - the presence of atrial fibrillation or or Propranolol LA 80mg daily); this is contraindicated
established osteoporosis will mean patients are more in those with asthma and caution should be exercised
likely to warrant treatment. in patients with diabetes where beta blockade can
In the setting of clear extrathyroidal signs of GD, mask the symptoms of hypoglycaemia. If beta
no further testing beyond free thyroid hormones and blockade is contraindicated, diltiazem can be used in
TSH is necessary. In the absence of features of GO thyrotoxic patients with tachycardia.
or pretibial myxoedema, it is useful to attempt to
secure an aetiological diagnosis. The gold-standard Treatment
test is a highly sensitive TSHR-stimulating antibody The treatment options for hyperthyroidism
assay or TSH receptor antibodies (TRAb)4,5. Other secondary to GD or nodular thyroid disease include
serum antibody tests, including indirect assay of ATDs (Carbimazole or Propylthiouracil in the
TSH-stimulating antibodies by TSH-binding UK), radioiodine therapy, or thyroid surgery. Each
inhibitory immunoglobulin (TBI or TBII) or TPO modality has its own pros and cons, and patient
antibody assay can be employed to confirm GD preference is frequently a deciding factor. Decisions
(TPO antibodies are also positive in autoimmune regarding treatment should be taken in conjunction
hypothyroidism). with the endocrine team and are usually made at
the time of endocrine review. The pathway for
Imaging this will vary between secondary and tertiary care
Imaging of the thyroid should not be routinely settings; some acute medicals units can rapidly access
requested for all patients, even in the presence of endocrine telephone advice or review, whereas
a goitre. It is often beneficial if the antibody test is others will refer for outpatient clinic follow-up.
© 2018 Rila Publications Ltd.Acute Medicine 2018; 17(1): 44-48 47
Managing thyrotoxicosis in the acute medical setting
ATDs should only be started in conjunction with admitted for close monitoring, supportive care and
endocrine input – mainly to ensure robust (verbal urgent endocrine input. In addition, those patients
and written) warnings regarding the rare but serious with significant tachycardia, AF or features of
and potentially lethal risk of agranulocytosis with cardiac failure will require a short admission until
Carbimazole (CBZ) or Propylthiouracil (PTU). any concern regarding cardiovascular instability has
This thionamide-induced agranulocytosis occurs in resolved.
around 1 in 300 people9: symptoms include a sore
throat and mouth ulcers and those affected will Special considerations
often have a high fever. Patients should be warned to
stop the ATD immediately in the presence of these Subclinical hyperthyroidism
symptoms and have a full blood count taken on the A number of patients may be found to have a low
same day. Agranulocytosis is most likely to occur in serum TSH (particularly if TSH testing is performed
the early months after starting treatment. without specific clinical indication) – this, in
Liaising with the endocrine team will also help conjunction with normal levels of free thyroid
ensure that patients have a timely follow-up plan in hormones, is defined as subclinical hyperthyroidism
place; those who start ATDS can become rapidly eu- (SH). Depending on the TSH assay cut-off value
or hypothyroid within a matter of weeks. The pros and the iodine intake of the population, SH may be
and cons of ATD treatment vs. radioactive iodine vs. found in up to 10% of the population10. SH can be
surgery will be discussed at the time of endocrine caused by endogenous thyroid disease, drug effects
review. If patients opt to complete a course of ATD and nonthyroidal illness. A low or undetectable TSH
therapy, then block and replace vs. a dose-titration is associated with significant morbidity and mortality
regimen will be decided upon. in longitudinal epidemiological surveys7. There
Thyrotoxicosis in the context of thyroiditis is is a paucity of evidence to guide the assessment or
transient. Patients are likely to have a hyperthyroid management of patients with SH, but they should
phase followed by a hypothyroid phase and then be flagged for repeat biochemical assessment; if
spontaneous resolution. Patients with subacute TFTs remain abnormal, a referral to endocrinology
thyroiditis may have pain and fever - analgesia is appropriate. It is useful to assess for other causes
(NSAIDs will be most effective) should be of a low TSH including non-thyroidal illness, drugs
administered and a short course of systemic steroids that suppress TSH (glucocorticoids, dopaminergic
may be helpful: advice on this can be taken from the medication, or octreotide) and drugs that alter
endocrine team. ATDs are ineffective. thyroid hormone secretion (amiodarone, lithium
The management of drug-induced thyrotoxicosis or iodine-containing contrast dyes). If a cause is not
is more complex and is best managed by endocrinology found, TFTs should be repeated in 3-6 months (or
(in conjunction with the cardiology team in the earlier if the patient is elderly or has cardiovascular
case of amiodarone-induced thyrotoxicosis). Other disease. If non-thyroidal illness is suspected to be
drugs may produce a self-limiting thyroiditis or a the cause, it would be appropriate to arrange repeat
more complex picture – a joint decision regarding testing after a shorter interval11.
management can be taken by the endocrine team in
conjunction with the specialist prescribing the drug. Drug-induced thyroid dysregulation
Amiodarone-induced thyrotoxicosis (AIT) –
When to admit encompassing ‘type I’, where excess thyroid
The vast majority of thyrotoxic patients will not hormone is synthesised and released, and ‘type II’,
require hospital admission, and can be safely when a destructive thyroiditis prompts the release of
discharged once beta blockade has been instigated. preformed thyroid hormone - occurs in around 20%
The decision on when to admit should be based upon of patients on the drug. Distinguishing between
clinical features rather than serum biochemistry. type I and type II can be challenging: each subtype
Free thyroid hormone levels above the upper limit requires tailored management and endocrine input
of the reference range are one indicator of severe should be sought. Patients on lithium can present
hyperthyroidism, but should not alone prompt with hypothyroidism or thyrotoxicosis (via the effect
admission. of lithium on thyroid cells, or by inducing painless
Many patients who present with thyrotoxicosis thyroiditis)12. More recently, the increasing use of
will be tachycardic; this alone is not an indication immune-checkpoint inhibitors in the management
for acute admission, although a cardiovascular of cancer has resulted in greater numbers of patients
examination should be performed and an ECG presenting with drug-induced thyroid dysfunction
should be documented. Patients with clinical features (thyrotoxicosis can be secondary to thyroiditis or
which are suspicious of a thyroid storm should be Graves’ disease). In drug-induced thyrotoxicosis,
© 2018 Rila Publications Ltd.48 Acute Medicine 2018; 17(1): 44-48
Managing thyrotoxicosis in the acute medical setting
the precipitating drug should not necessarily be include hypertension, congestive cardiac failure
stopped; endocrine input is paramount to ensure an and thyroid storm14and obstetric complications may
appropriate management plan is promptly instigated. occur. The longer the duration of uncontrolled
hyperthyroidism, the higher the likelihood of a
Thyroid storm detrimental impact on maternal and foetal outcome.
A thyroid storm is a rare but life threatening Pregnant women with suspected hyperthyroidism
condition. Signs include fever, tachycardia, agitation should be urgently referred to medical obstetrics
and altered mental state, deranged liver function tests team or endocrinology for prompt assessment.
and features of cardiac failure. It can be precipitated Not all cases of apparent hyperthyroidism in
by infection, surgery, trauma childbirth or poor pregnancy are pathological - high levels of ß human
compliance to treatment. chorionic gonadotrophin can lead to ‘gestational
hyperthyroidism’, with absent TSH receptor
Pregnant women antibodies, no extrathyroidal features and no goitre;
Untreated hyperthyroidism in pregnancy this will resolve by 20 weeks gestation.
poses serious risks to both mother and baby. If
uncontrolled, restricted foetal growth and low Conflict of Interest
birthweight is likely13,14. Maternal sequelae can Nothing to declare.
References
1. Garmendia Madariaga A et al; The incidence and prevalence of on Diagnosis and Treatment of Endogenous Subclinical
thyroid dysfunction in Europe: a meta-analysis. J Clin Endocrinol Hyperthyroidism. Eur Thyroid J 2015; 4(3):149-63.
Metab 2014; 99(3):923-31. 9. Watanabe N et al; Antithyroid-drug induced hematopoietic
2. Vaidya B and Pearce SHS; Diagnosis and management of damage: a retrospective cohort study of agranulocytosis and
thyrotoxicosis. BMJ 2014; 349:g5218. pancytopenia involving 50,385 patients with Graves’ disease.
3. Ross DS et al; American Thyroid Association Guidelines for JCEM 2012; 97:E49-53.
Diagnosis and Management of Hyperthyroidism and Other 10. Carle A et al; Management of Endocrine Disease: Subclinical
Causes of Thyrotoxicosis. Thyroid 2016; 26(10):1343-1421. thyrotoxicosis: prevalence, causes and choice of therapy. EJE 2017;
4. Burch HB and Cooper DS; Management of Graves’ Disease: A 176:325-337.
Review. JAMA 2015; 314(23):2544-54. 11. NICE CKS Hyperthyroidism June 2016 Accessed via www.cks.
5. Smith TJ and Hegedüs L; Graves’ Disease. N Engl J Med 2016; nice.org.uk [November 2017].
375(16):1552-1565. 12. Pearce EN et al; Thyroiditis. N Engl J Med 2003; 348(26):2646-
6. Mitchell AL et al; Diagnosis of Graves’ orbitopathy (DiaGO): results 2655.
of a pilot study to assess the utility of an office tool for practicing 13. Laurberg P et al; Management of Graves’ hyperthyroidism in
endocrinologists. J Clin Endocrinol Metab 2015; 100(3):E458-62. pregnancy: Focus on both maternal and foetal thyroid function,
7. Mitchell AL and Pearce SHS; How should we treat patients with and caution against surgical thyroidectomy in pregnancy. Eur Jour
low serum thyrotropin concentrations? Clin Endocrinol 2010; Endocrinol 2009; 160(1):1-8.
72(3):292-6. 14. Rivkees SA and Mandel SJ; Thyroid disease in pregnancy. Horm
8. Biondi B et al; The 2015 European Thyroid Association Guidelines Res Paediatr 2011; 76 (supp.1):91-96.
© 2018 Rila Publications Ltd.You can also read