Mastering the Infection Control Focused Survey - Kentucky ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Mastering the Infection Control Focused Survey June 2021
Mastering the Infection
Control Focused Survey
Shelly Maffia RN, NHA, MSN, MBA, CHC, QCP
Director of Regulatory Services
OBJECTIVES
At the conclusion of this session, the learner will:
1. Describe the procedures used by surveyors in conducting focused
infection control surveys
2. Explain changes in Infection Prevention & Control survey
procedures that will take place in upcoming annual surveys
3. Explain enhanced enforcement actions associated with infection
control citations
4. Apply strategies to prevent infection control citations
www.proactivemedicalreview.com 1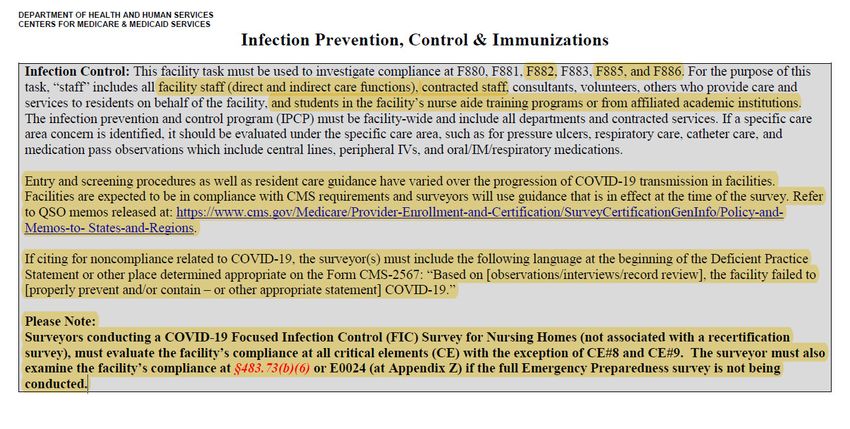
Mastering the Infection Control Focused Survey June 2021
COVID‐19 SURVEY ACTIVITIES
FOCUSED INFECTION
CONTROL (FIC) SURVEYS
• On‐site surveys to be performed within 3‐5 days of identification of 3 or more new COVID‐19
suspected & confirmed cases in a nursing home since the last weekly NHSN COVID‐19 report or one
confirmed case in a facility that was previously COVID free and other factors that may place residents’
health and safety at risk. These factors include:
• Multiple weeks with new COVID‐19 cases;
• Low staffing;
• Selection as a Special Focus Facility per Section 1819(f)(8)(B) of the Social Security Act ;
• Concerns related to conducting outbreak testing per CMS requirements; or
• Allegations or complaints which pose a risk for harm or Immediate Jeopardy to the health or safety
of residents which are related to certain areas, such a abuse or quality of care (e.g., pressure
ulcers, weight loss, depression, decline in functioning).
• Survey must start within 3‐5 days of identification by CMS/State
• Do not have to perform FIC in facilities that meet criteria if a FIC survey was conducted within previous
3 weeks
www.proactivemedicalreview.com 2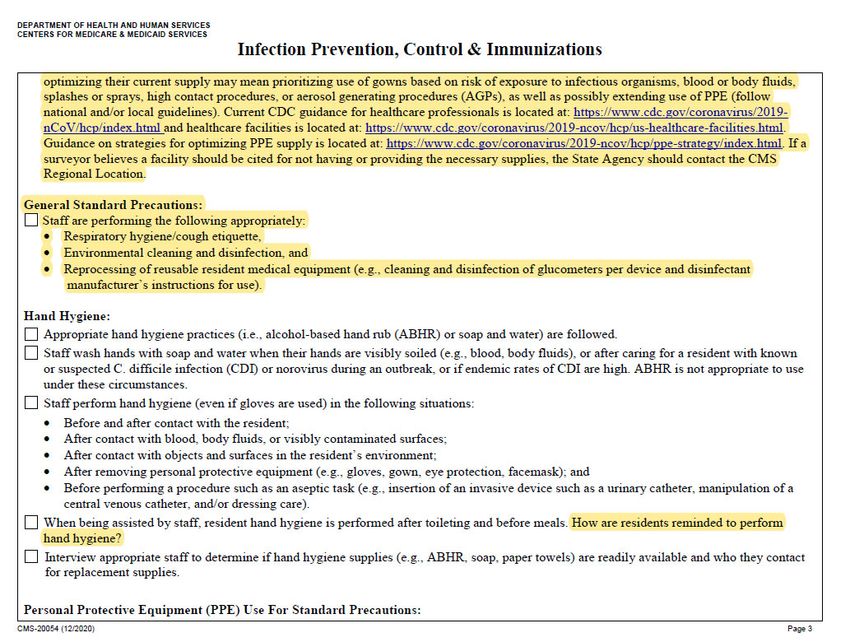
Mastering the Infection Control Focused Survey June 2021
FOCUSED INFECTION
CONTROL SURVEYS
• In FY 2021 (Oct 2020), annual focused infection control (FIC) surveys will
be conducted in 20% of nursing homes in state
• To count toward required 20%, FIC must be stand‐alone survey not
associated with recertification survey
• Any FIC conducted in FY 2021 d/t meeting outbreak criteria can count
toward meeting State’s 20%
EXPANDED SURVEY ACTIVITIES
• Prior to transitioning back to routine survey activities, states will
prioritize surveys for:
• Complaint investigations triaged as Non‐Immediate Jeopardy‐High
• Revisits of facilities with removed IJ that are still out of compliance
• Special focus facility (SFF) & SFF Candidate recertification surveys
• Recertification surveys that are greater than 15 months
• As of 5/23/21 CASPER data:
• 89.8% KY facilities 15 months overdue (255 facilities)
• 72.5% 18 months overdue (206 facilities)
• 21.5% 24 months overdue (61 facilities)
• 4.6% 27 months overdue (13 facilities)
www.proactivemedicalreview.com 3
Mastering the Infection Control Focused Survey June 2021
ENHANCED ENFORCEMENT
FOR INFECTION CONTROL DEFICIENCIES
• If no Infection Control deficiency in last year (or on last STD)
• D or E level F880 citation
• Directed Plan of Correction
• F level F880 citation
• Directed Plan of Correction
• Discretionary denial of payment for new admissions
(DOPNA) with 45 days to demonstrate compliance with
Infection Control deficiencies
ENHANCED ENFORCEMENT
FOR INFECTION CONTROL DEFICIENCIES
• If 1 Infection Control deficiency in last year (or on last STD)
• D or E level citation
• Directed Plan of Correction
• DOPNA with 45 days to demonstrate compliance with Infection
Control deficiencies
• Per instance Civil Monetary Penalty (CMP) up to $5,000
• F level citation
• Directed Plan of Correction
• DOPNA with 45 days to demonstrate compliance with Infection
Control deficiencies
• $10,000 per instance CMP
www.proactivemedicalreview.com 4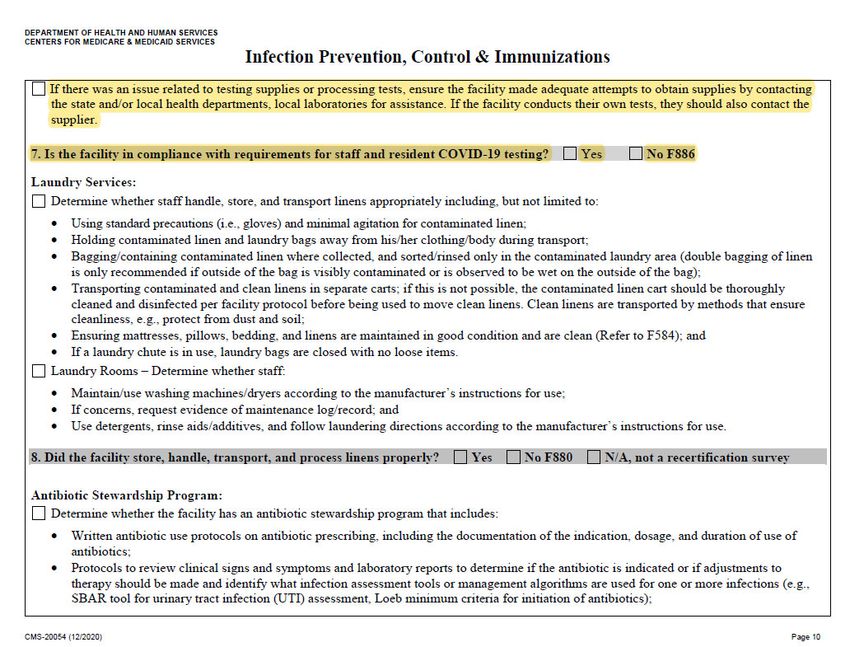
Mastering the Infection Control Focused Survey June 2021
ENHANCED ENFORCEMENT
FOR INFECTION CONTROL DEFICIENCIES
• If 2 or more Infection Control deficiency in last 2 years (or twice since 2nd to last STD)
• D or E level citation
• Directed Plan of Correction
• DOPNA with 30 days to demonstrate compliance with Infection Control deficiencies
• $15,000 Per Instance CMP (or per day CMP may be imposed, as long as the total
amount exceeds $15,000)
• F level citation
• Directed Plan of Correction
• DOPNA with 30 days to demonstrate compliance with Infection Control deficiencies
• $20,000 Per Instance CMP (or per day CMP may be imposed, as long as the total
amount exceeds $20,000)
ENHANCED ENFORCEMENT
FOR INFECTION CONTROL DEFICIENCIES
• Current Infection Control deficiency at harm level (G,H,I) regardless of past history
• Directed Plan of Correction
• DOPNA with 30 days to demonstrate compliance with Infection Control
deficiencies
• CMP imposed at highest amount option within the appropriate (non‐Immediate
Jeopardy) range in the CMP analytic tool
• Current Infection Control deficiency at Immediate Jeopardy level (J,K,L) regardless of
past history
• Mandatory remedies of Temporary Manager or Termination
• Directed Plan of Correction
• DOPNA with 15 days to demonstrate compliance with Infection Control
deficiencies
• CMP imposed at highest amount option within the appropriate (IJ) range in the
CMP analytic tool
www.proactivemedicalreview.com 5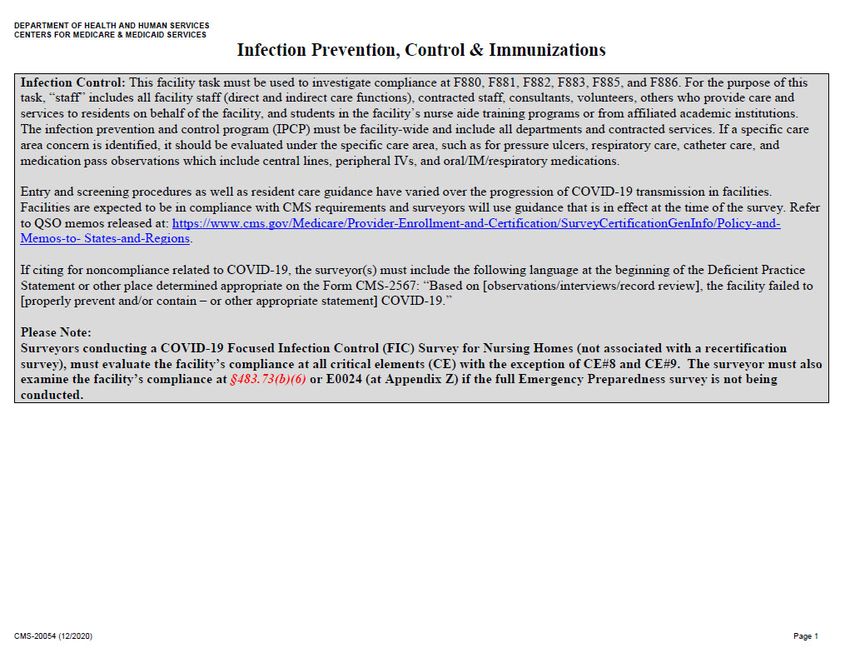
Mastering the Infection Control Focused Survey June 2021
IMPOSED REMEDIES
• Directed Plan of Correction
• A plan the State develops to require a facility to take action
within specified time frames.
• Should address all elements required for a facility developed
plan of correction
• May be imposed 15 calendar days after facility receives notice in
non‐IJ situations & 2 calendar days after notice in IJ situations
• The date the directed plan of correction is imposed does not
mean that all correction must be completed by that date.
IMPOSED REMEDIES
• Denial of Payment for all New Medicare & Medicaid Admission (DOPNA)
• May be imposed anytime facility is out of compliance, as long as facility is given
written notice 2 calendar days before effective date for IJ situations and at least 15
days before effective date in non‐IJ situations
• CMS will deny payment to facility for all new MCR admissions
• State MCD agency will deny payment to facility & CMS will deny Federal financial
participation to MCD agency for all new MCD admissions
• Mandatory DOPNA
• When not in substantial compliance 3 months after the last day of the survey
identifying deficiencies or
• When found to have substandard quality of care on last 3 consecutive standard
surveys
• Payments resume prospectively from date substantial compliance was achieved
www.proactivemedicalreview.com 6
Mastering the Infection Control Focused Survey June 2021
IMPOSED REMEDIES
• Civil Money Penalties (CMPs)
• May impose $3,050‐$10,000 per day of IJ or $50‐$3,000 per day of non‐IJ or per
instance CMP of $1,000‐$10,000 for each deficiency
• Per day CMP may start accruing on date facility was first out of compliance
• Payment is due on whichever of the following occurs first if the facility files an appeal of
the enforcement action:
• The date on which the independent informal dispute resolution process is
completed; or
• The date which is 90 calendar days after the date of the notice of imposition of the
penalty.
• If no hearing requested, due:
• 15 calendar days after time period for requesting hearing has expired if substantial
compliance achieved before hearing request was due
KY Enforcement Actions FY2021
• 90 providers received enforcement action
• 165 total enforcement actions
• 24 Directed Plan of Corrections
• 5 Discretionary Denial Payment for New Admits
• 136 Civil Money Penalties
• 77 Per Diem
• Average $13,705.04
• Average Days in Effect – 6
• 59 Per Instance
• Average $6,511.60
Source: CASPER (05/23/2021)
www.proactivemedicalreview.com 7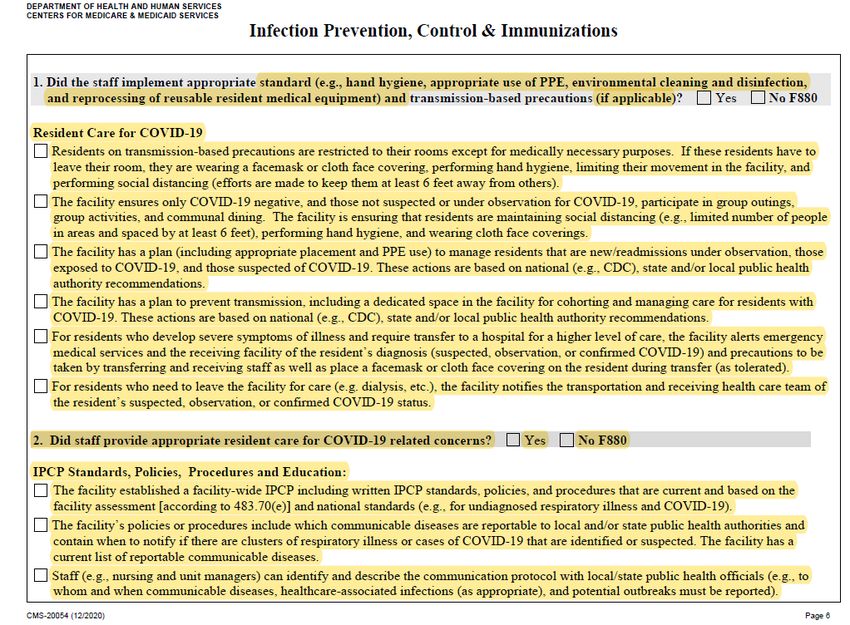
Mastering the Infection Control Focused Survey June 2021
COVID‐19 Focused Infection Control (FIC)
Survey Protocol
Offsite Planning for COVID FIC Survey
• Prior to coming onsite, surveyor will:
• Review facility reported information in NHSN
• Complaint allegations
• Identify surveyors to remain offsite to receive information from surveyor or
facility staff while onsite
www.proactivemedicalreview.com 8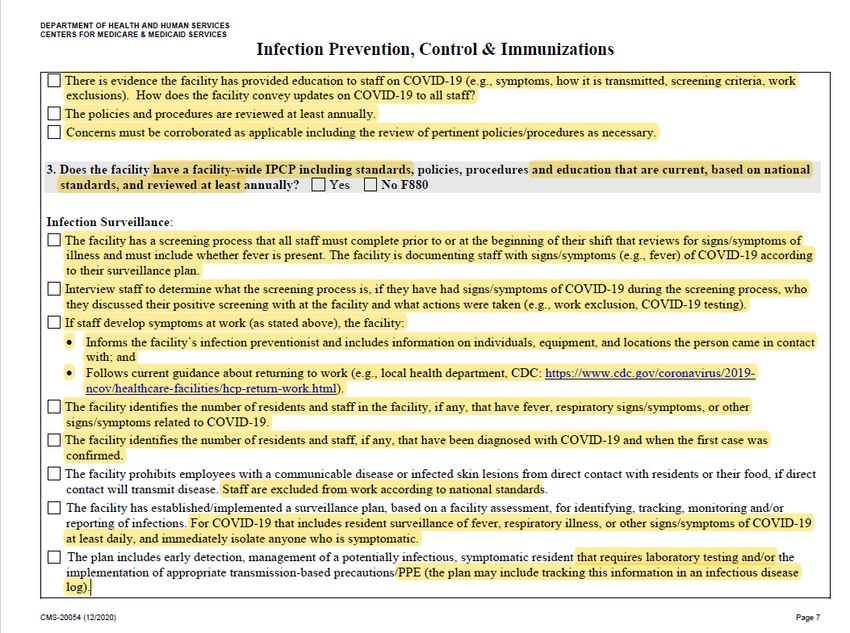
Mastering the Infection Control Focused Survey June 2021
COVID FIC Survey On-Site Activities
• Surveyor should begin the survey activity in an area with COVID‐19 negative
residents and not return to that area once positive residents have been
encountered
• Prioritize observations to key areas & activities r/t infection control
• Identify interviews/observations that need to be conducted
• Identify records that need to be reviewed onsite & those that can be sent for
offsite review
• Medical record reviews, staff & resident test results, County positivity rates may be reviewed
offsite after survey begins
• Telephone interviews
• Comprehensive review of facility P&Ps
• Review of communications to residents & families
• Will refer to & review latest CDC guidance
COVID FIC
Survey Entrance
Conference
www.proactivemedicalreview.com 9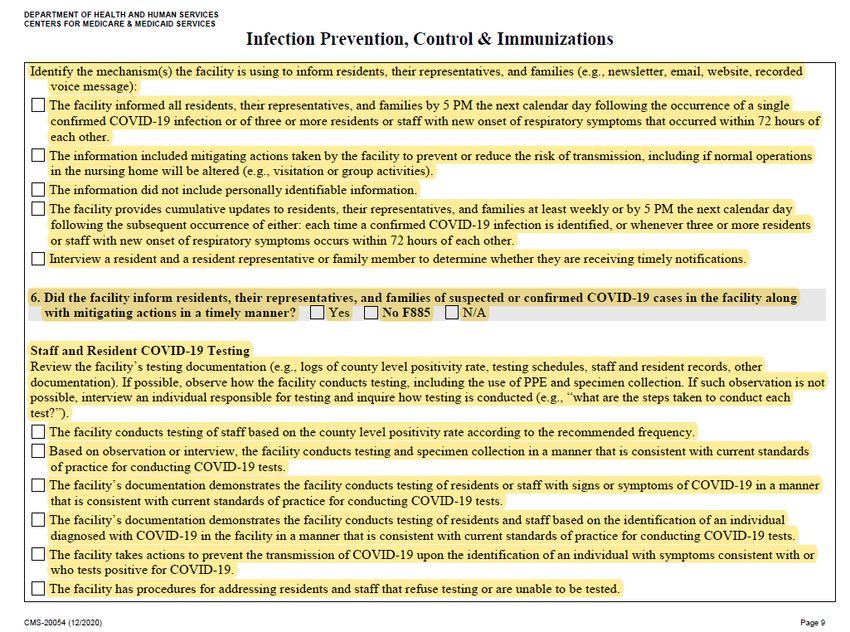
Mastering the Infection Control Focused Survey June 2021
Infection
Prevention,
Control, &
Immunization
Pathway
COVID FIC Survey Exit
• Survey exit discussions should be held by telephone or through virtual
meeting
• CMS‐2567 drafted offsite
www.proactivemedicalreview.com 10Mastering the Infection Control Focused Survey June 2021
Standard Survey
FY 2021 Recertification Surveys
• 12 facilities (4.2%) recertification surveys completed
• Oct 2020 2021 – 8 Surveys Completed
• 9 Avg Deficiencies per survey
• 15‐22 months since last surveys (those less than 18 mo received IJ r/t complaints)
• March 2021 – 2 Surveys Completed
• 3 Deficiencies for 1, SOD not available yet for other
• 25‐26 months since last survey
• April 2021 – 2 Surveys Completed
• 1 Deficiency free & No SOD available yet for the other
• 24‐26 months since last survey
Source: CASPER 05/30/2021
www.proactivemedicalreview.com 11Mastering the Infection Control Focused Survey June 2021
Changes Related to COVID-19
• Offsite Prep includes review of CDC, state/local public health information, if available, to be aware of the
COVID‐19 status of the facility
• Will ensure a surveyor(s) is assigned to and stays exclusively in the area of the facility that is used for
cohorting COVID‐19 positive or suspected positive residents when making assignments
• 2 residents who are on Transmission‐Based Precautions (suspected or confirmed COVID‐19 and for any
reason other than COVID‐19) should be included in the initial pool for the team, if available.
• If one resident is on TBP for both types of infections (COVID‐19 and non‐COVID‐19), it is acceptable to
include just the one resident
• If dining rooms are not being used during the PHE, determine whether residents are receiving assistance and
ensure room trays are reviewed
• If a surveyor is restricted to a specific area of the building (e.g., because of cohorting), the surveyor should
not be physically present with any team member.
• The surveyor should meet virtually or by telephone (on his/her own) with the team throughout the
survey.
Infection Control Task Changes Related to
COVID-19
• Sample 3 staff & 3 residents
• Will include at least 1 staff member & resident who was confirmed COVID‐19
positive or had signs or symptoms consistent with COVID‐19 (if any) & 1
resident on TBP, for purposes of determining compliance with infection
prevention and control national standards such as exclusion from work, as well
as screening, testing, and reporting.
• Sample 5 residents for influenza & pneumococcal immunizations
www.proactivemedicalreview.com 12Mastering the Infection Control Focused Survey June 2021
Entrance Conference Worksheet Changes Related to
COVID-19
• Information needed immediately upon entrance
• A list of residents who are confirmed or suspected cases of COVID‐19
• Name of facility staff responsible for IPC Program
• Entrance Conference changes
• A copy of an updated facility floor plan, if changes have been made, including COVID‐19 observation and
COVID‐19 units.
• Information Needed Within One Hour of Entrance
• List of key personnel, location, and phone numbers. Note contract staff (e.g., rehab services). Also include
the staff responsible for notifying all residents, representatives, and families of confirmed or suspected
COVID‐19 cases in the facility.
• The facility’s mechanism(s) used to inform residents, their representatives, and families of confirmed or
suspected COVID‐19 activity in the facility and mitigating actions taken by the facility to prevent or reduce
the risk of transmission, including if normal operations in the nursing home will be altered (e.g., supply the
newsletter, email, website, etc.). If the system is dependent on the resident or representative to obtain the
information themselves (e.g., website), provide the notification/information given to residents, their
representatives, and families informing them of how to obtain updates.
• Documentation related to COVID‐19 testing, which may include the facility’s testing plan, logs of county
level positivity rates, testing schedules, list of staff who have confirmed or suspected cases of COVID‐19, and
if there were testing issues, contact with state and local health departments.
Entrance Conference Worksheet Changes Related to
COVID-19
• Information needed within 4 hours of entrance
• Infection Prevention and Control Program Standards, Policies and
Procedures, to include the Surveillance Plan, Procedures to address resident
and staff who refuse testing or are unable to be tested, and Antibiotic
Stewardship Program.
• List of rooms meeting any one of the following conditions that require a variance:
• Less than the required square footage
• More than four residents
• Below ground level
• No window to outside
• No direct access to exit corridor
• EHR Information
• COVID‐19 test results
www.proactivemedicalreview.com 13Mastering the Infection Control Focused Survey June 2021
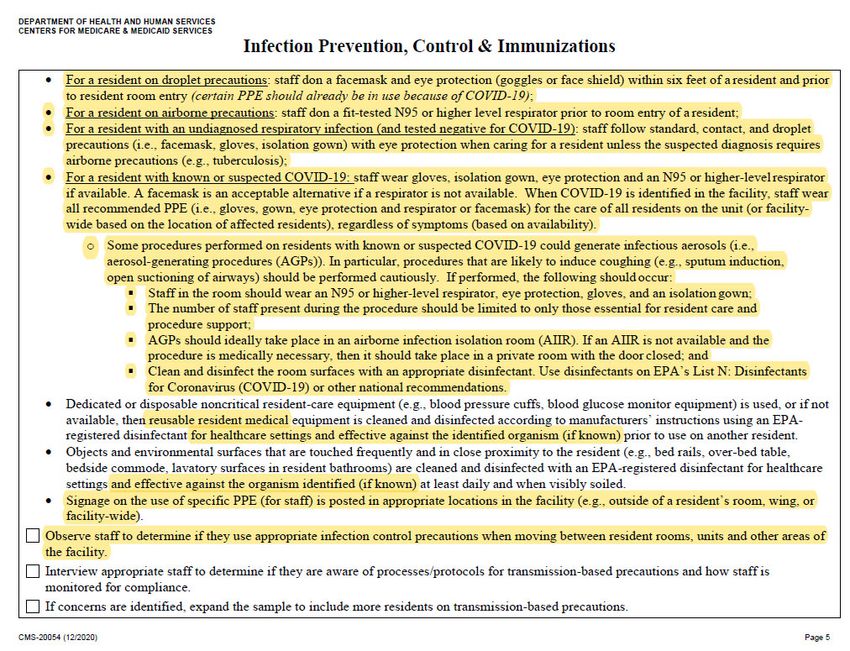
Infection Prevention, Control, & Immunization
CE Pathway Changes Related to COVID-19
Infection
Prevention,
Control, &
Immunization
CE Pathway
Changes
Related to
COVID-19
(Page 2)
www.proactivemedicalreview.com 14Mastering the Infection Control Focused Survey June 2021
Infection
Prevention,
Control, &
Immunization
CE Pathway
Changes
Related to
COVID-19
(Page 3)
Infection
Prevention,
Control, &
Immunization
CE Pathway
Changes
Related to
COVID-19
(Page 4)
www.proactivemedicalreview.com 15Mastering the Infection Control Focused Survey June 2021
Infection
Prevention,
Control, &
Immunization
CE Pathway
Changes
Related to
COVID-19
(Page 5)
Infection
Prevention,
Control, &
Immunization
CE Pathway
Changes
Related to
COVID-19
(Page 6)
www.proactivemedicalreview.com 16Mastering the Infection Control Focused Survey June 2021
Infection
Prevention,
Control, &
Immunization
CE Pathway
Changes
Related to
COVID-19
(Page 7)
Infection
Prevention,
Control, &
Immunization
CE Pathway
Changes
Related to
COVID-19
(Page 8)
www.proactivemedicalreview.com 17Mastering the Infection Control Focused Survey June 2021
Infection
Prevention,
Control, &
Immunization
CE Pathway
Changes
Related to
COVID-19
(Page 9)
Infection
Prevention,
Control, &
Immunization
CE Pathway
Changes
Related to
COVID-19
(Page 10)
www.proactivemedicalreview.com 18Mastering the Infection Control Focused Survey June 2021
Infection
Prevention,
Control, &
Immunization
CE Pathway
Changes
Related to
COVID-19
(Page 11)
CMS FAQs
• When doing STD survey, if surveyors discover facility has COVID cases, must
they combine the FIC with STD survey?
• No
• How should LTC standard recertification health surveys, and EP surveys and
LSC surveys be conducted when there are active COVID‐19 cases in the
building?
• 1 surveyor will be assigned to and stay exclusively on COVID unit
• All surveyors should use appropriate IC precautions when entering resident rooms
• Are facilities required to allow surveyors and Fire Marshals into their
facilities?
• Yes
www.proactivemedicalreview.com 19Mastering the Infection Control Focused Survey June 2021
CMS FAQs
• What protocols are in place for surveyors?
• Wear appropriate PPE
• Adhere to COVID‐19 IPC practices
• Adhere to screening protocols prior to entering
• Can a facility refuse entry to a surveyor based on results of screening
protocols?
• Surveyors should not enter if they are experiencing s/s of infection
• Are surveyors required to be tested?
• CMS encourages States to provide testing for surveyors, but does not require it
• Facilities may offer to test surveyors, but cannot require it as a condition for
entering facility
CMS FAQs
• Should the team try to minimize the number of surveyors who interact with
known COVID‐19 positive residents?
• Yes, recommend 1 surveyor to be assigned to COVID positive residents only & 1 to suspected
COVID residents or under observation & they not meet in person with other surveyors
• Does the Personal Protective Equipment (PPE) requirement for surveyors change
based on the COVID‐19 status of the facility?
• Yes
• For facilities with a COVID‐19 unit, should that unit be included in the sample
selection process?
• Yes
• During LTC standard recertification health surveys, will survey teams be permitted
to complete entrance activities by phone?
• No
www.proactivemedicalreview.com 20Mastering the Infection Control Focused Survey June 2021
CMS FAQs
• During LTC standard recertification health surveys, if the initial pool of residents
includes a COVID‐19 positive resident, could that resident be replaced with
someone who is negative?
• No
• During standard recertification surveys, will survey teams be permitted to
complete phone interviews and record reviews offsite to minimize time onsite?
• Should attempt to safely interview in the resident room, even if COVID positive or suspected
• Are there any facility tasks that need to be altered if there are COVID‐19 cases in
the building?
• Resident council group interview should be done while social distancing. If not possible, will
ask to review council minutes & follow up on concerns with a member
• If dining rooms not being used, will assess if assistance provided to those needing assistance &
observe meal for initial pool residents with weight loss, food, or hydration concerns
CMS FAQs
• During standard recertification surveys, will survey teams be permitted to
complete exit activities by phone?
• Yes, if all parties agree
• What adjustments should Life Safety Code surveyors make during the survey
process in response to COVID‐19?
• Facility Tour‐ may choose not to enter room/wings with confirmed/suspected COVID
cases
• Record Reviews – Must review Sprinkler system testing, fire extinguisher monthly
inspection, elevator testing, Emergency generator testing, daily inspections of means
of egress in areas that have undergone construction or alterations, orientation
training program r/t fire plan
• Deficiency Determination – should not cite for any areas covered in 1135 blanket
waiver https://www.cms.gov/files/document/summary‐covid‐19‐emergency‐
declaration‐waivers.pdf
www.proactivemedicalreview.com 21Mastering the Infection Control Focused Survey June 2021
NEW INFECTION CONTROL F-TAGS
NEW REPORTING REQUIREMENTS – F884
• (g) COVID‐19 Reporting. The facility must—
• (1) Electronically report information about COVID‐19 in a standardized format specified by the
Secretary. This report must include but is not limited to
• (i) Suspected and confirmed COVID‐19 infections among residents and staff, including residents
previously treated for COVID‐19;
• (ii) Total deaths and COVID‐19 deaths among residents and staff;
• (iii) Personal protective equipment and hand hygiene supplies in the facility;
• (iv) Ventilator capacity and supplies in the facility;
• (v) Resident beds and census;
• (vi) Access to COVID‐19 testing while the resident is in the facility;
• (vii) Staffing shortages; and
• (viii) Other information specified by the Secretary.
• (2) Provide the information specified in paragraph (g)(1) of this section at a frequency specified by the
Secretary, but no less than weekly to the Centers for Disease Control and Prevention’s National
Healthcare Safety Network. This information will be posted publicly by CMS to support protecting the
health and safety of residents, personnel, and the general public.
www.proactivemedicalreview.com 22Mastering the Infection Control Focused Survey June 2021
NHSN REPORTING (F884)
• Must submit through the NHSN reporting system at least every 7 days
• May choose to submit multiple times a week
• No specific day of week that reporting must be completed, but should
remain consistent with data being submitted on same day(s) each week
• Collection period should remain consistent (e.g. Mon‐Sun)
• Every Monday CMS will review the data submitted to assess if each
facility submitted data at least once in the previous 7 days.
• NHSN Enrollment & Training
• https://www.cdc.gov/nhsn/ltc/covid19/index.html
REPORTING ENFORCEMENT
• COVID‐19 Reporting to CDC (F884)
• Reviews conducted offsite by CMS Federal surveys
• State surveyors will not cite this tag
• Facilities identified as not reporting will receive F884 at
scope/severity level F & CMP imposition
• If fail to report weekly, CMS will impose a per day CMP of $1,000
for one day for the failure to report that week. CMP will increase by
$500 for each subsequent week facility fails to submit required
report (not reporting for 2 weeks= CMP total of $2,500)
www.proactivemedicalreview.com 23Mastering the Infection Control Focused Survey June 2021
F884 Citations
• COVID‐19 Reporting to CDC (F884)
• As of 05/23/2021 data in CASPER
• 4,479 Citations Nationally in FY 2021
• 69 Citations in KY in FY 2021
• From 52 facilities
Source: CASPER (05/23/2021)
Most Common Data Submission Errors
• Reporting aggregate counts
• COVID‐19 deaths > total number of deaths
• Missing data for counts
• Missing or incomplete reporting in one or more pathway
• Number of ventilators missing or 0 in facilities that identified they have
ventilator units/beds
www.proactivemedicalreview.com 24Mastering the Infection Control Focused Survey June 2021
REPORTING ISSUES
• Try to connect and report to NSHN on a daily basis (if you are
having difficulties reporting on a weekly basis, as required by
CMS), even if each attempt is unsuccessful. After unsuccessful
attempts, request technical assistance from NHSN.
• Maintain thorough records of all attempts to connect, report,
and receive technical assistance.
• If you receive an F‐tag and/or CMP, submit the matter to
independent informal dispute resolution (IIDR) within the
permitted time‐frame and include all documentation and details.
• Submit a separate IIDR request for each 2567, even if the supporting
documentation is the same.
NEW REPORTING REQUIREMENTS – F885
• (3) Inform residents, their representatives, and families of those residing in facilities
by 5 p.m. the next calendar day following the occurrence of either a single
confirmed infection of COVID‐19, or three or more residents or staff with new‐
onset of respiratory symptoms occurring within 72 hours of each other. This
information must—
• (i) Not include personally identifiable information;
• (ii) Include information on mitigating actions implemented to prevent or reduce
the risk of transmission, including if normal operations of the facility will be
altered; and
• (iii) Include any cumulative updates for residents, their representatives, and
families at least weekly or by 5 p.m. the next calendar day following the
subsequent occurrence of either: each time a confirmed infection of COVID‐19
is identified, or whenever three or more residents or staff with new onset of
respiratory symptoms occur within 72 hours of each other
www.proactivemedicalreview.com 25Mastering the Infection Control Focused Survey June 2021
REPORTING ENFORCEMENT
• COVID‐19 Reporting to Residents, Representatives,
Families (F885)
• Reviews included in on‐site COVID focused surveys
• Facilities identified as not reporting will receive F885 at
scope/severity level F
• Can notify through email listservs, website postings, paper
notification, and/or recorded telephone calls
F885 Citations
• COVID‐19 Reporting to Residents, Representatives, Families
(F885)
• As of 05/23/2021 data in CASPER
• 390 citations nationally in FY 2021
• 2 Citations in KY in FY 2021
• 1 D level
• 1 F level
Source: CASPER (05/23/2021)
www.proactivemedicalreview.com 26Mastering the Infection Control Focused Survey June 2021
F885 Citation
• Failed to ensure timely notification of families of positive COVID results for 4
residents.
• Building sent emails to corporate to update website with positive results and one
occasion email sent on Friday and website not updated till Mon and facility did not
send email with 7/24 + results to corporate to update until 7/28. (they had previously
sent memo to families notifying them that communication of + cases will occur on the
website)
• Resident was tested 7/21 r/t potential exposure. Resident DC home on 7/22
and facility did not inform family of pending test d/t exposure. 7/23 received
confirmation of positive test. Family not notified until 7/24
• Logs of recorded calls to residents and families revealed COVID update calls
were not made with each new confirmed case
COVID TESTING REQUIREMENTS – F886
• § 483.80(h) COVID‐19 Testing. The LTC facility must test residents and facility staff, including
individuals providing services under arrangement and volunteers, for COVID‐19. At a minimum, for all
residents and facility staff, including individuals providing services under arrangement and volunteers,
the LTC facility must:
• (1) Conduct testing based on parameters set forth by the Secretary, including but not limited to:
• (i) Testing frequency;
• (ii) The identification of any individual specified in this paragraph diagnosed with COVID19 in the facility;
• (iii) The identification of any individual specified in this paragraph with symptoms consistent with COVID‐19
or with known or suspected exposure to COVID‐19;
• (iv) The criteria for conducting testing of asymptomatic individuals specified in this paragraph, such as the
positivity rate of COVID‐19 in a county;
• (v) The response time for test results; and
• (vi) Other factors specified by the Secretary that help identify and prevent the transmission of COVID‐19.
• (2) Conduct testing in a manner that is consistent with current standards of practice for conducting
COVID‐19 tests;
Source: https://www.cms.gov/files/document/qso‐20‐38‐nh.pdf
www.proactivemedicalreview.com 27Mastering the Infection Control Focused Survey June 2021
COVID TESTING REQUIREMENTS
DEFINITONS
• Fully Vaccinated
• Refers to a person who is ≥2 weeks following receipt of the second dose in a 2‐
dose series, or ≥2 weeks following receipt of one dose of a single‐dose vaccine.
• Unvaccinated
• Refers to a person who does not fit the definition of “fully vaccinated,”
including people whose vaccination status is not known, for the purposes of
this guidance.
COVID TESTING REQUIREMENTS
County Positivity Rates: https://data.cms.gov/stories/s/COVID‐19‐Nursing‐Home‐Data/bkwz‐xpvg
Source: https://www.cms.gov/files/document/qso‐20‐38‐nh.pdf
www.proactivemedicalreview.com 28Mastering the Infection Control Focused Survey June 2021
COVID TESTING REQUIREMENTS
County Positivity Rates: https://data.cms.gov/stories/s/COVID‐19‐Nursing‐Home‐Data/bkwz‐xpvg
Source: https://www.cms.gov/files/document/qso‐20‐38‐nh.pdf
COVID TESTING REQUIREMENTS – F886
• (3) For each instance of testing:
• (i) Document that testing was completed and the results of each staff test; and
• (ii) Document in the resident records that testing was offered, completed (as appropriate
to the resident’s testing status), and the results of each test.
• (4) Upon the identification of an individual specified in this paragraph with
symptoms consistent with COVID‐19, or who tests positive for COVID‐19, take
actions to prevent the transmission of COVID‐19.
• (5) Have procedures for addressing residents and staff, including individuals
providing services under arrangement and volunteers, who refuse testing or are
unable to be tested.
• (6) When necessary, such as in emergencies due to testing supply shortages,
contact state and local health departments to assist in testing efforts, such as
obtaining testing supplies or processing test results.
www.proactivemedicalreview.com 29Mastering the Infection Control Focused Survey June 2021
F886 Citations
• COVID‐19 Testing Residents & Staff
• As of 05/23/21 data in CASPER
• 658 citations nationally in FY 2021
• 6 Citation in KY in FY 2021
• 1 E level
• 5 F level
Source: CASPER (05/23/2021)
F886 Citation Examples
• Failed to provide twice weekly testing to staff based on county
positivity rate.
• Facility was only testing when staff showed s/s or suspicion of COVID
• Facility testing weekly rather than twice per week per county positivity
rate
www.proactivemedicalreview.com 30Mastering the Infection Control Focused Survey June 2021
F887 COVID Immunization
• The LTC facility must develop and implement policies and procedures to
ensure all the following:
i. When COVID‐19 vaccine is available to the facility, each resident and staff member
is offered the COVID‐19 vaccine unless the immunization is medically
contraindicated or the resident or staff member has already been immunized;
ii. Before offering COVID‐19 vaccine, all staff members are provided with education
regarding the benefits and risks and potential side effects associated with the
vaccine;
iii. Before offering COVID‐19 vaccine, each resident or the resident representative
receives education regarding the benefits and risks and potential side effects
associated with the COVID‐19 vaccine;
iv. In situations where COVID‐19 vaccination requires multiple doses, the resident,
resident representative, or staff member is provided with current information
regarding those additional doses, including any changes in the benefits or risks and
potential side effects, associated with the COVID‐19 vaccine, before requesting
consent for administration of any additional doses
Source: https://www.cms.gov/files/document/qso‐21‐19‐nh.pdf
F887 COVID Immunization (continued)
• The LTC facility must develop and implement policies and procedures to ensure all the
following:
v. The resident, resident representative, or staff member has the opportunity to accept or refuse a
COVID‐19 vaccine, and change their decision; and
vi. The resident's medical record includes documentation that indicates, at a minimum, the
following:
A. That the resident or resident representative was provided education regarding the benefits and potential
risks associated with COVID‐19 vaccine; and
B. Each dose of COVID‐19 vaccine administered to the resident, or
C. If the resident did not receive the COVID‐19 vaccine due to medical contraindications or refusal.
vii. The facility maintains documentation related to staff COVID‐19 vaccination that includes at a
minimum, the following:
A. That staff were provided education regarding the benefits and potential risks associated with COVID‐19
vaccine;
B. Staff were offered the COVID‐19 vaccine or information on obtaining COVID‐19 vaccine; and
C. The COVID‐19 vaccine status of staff and related information as indicated by NHSN.
viii. The COVID‐19 vaccine status of residents and staff, including total numbers of residents and staff,
numbers of residents and staff vaccinated, numbers of each dose of COVID19 vaccine received,
and COVID‐19 vaccination adverse events; and
ix. (ix) Therapeutics administered to residents for treatment of COVID‐19
Source: https://www.cms.gov/files/document/qso‐21‐19‐nh.pdf
www.proactivemedicalreview.com 31Mastering the Infection Control Focused Survey June 2021
F882 Infection Preventionist
• The facility must designate one or more individual(s) as the infection
preventionist(s) (IP)(s) who are responsible for the facility’s IPCP.
• The IP must:
• Have primary professional training in nursing, medical technology,
microbiology, epidemiology, or other related field;
• Be qualified by education, training, experience or certification;
• Work at least part‐time at the facility; and
• Have completed specialized training in infection prevention and control.
• Be a member of & report to QAPI committee on the IPCP on a regular basis
Infection Preventionist Specialized Training
• CMS & CDC "Nursing Home • Covers core activities of IPCP,
Infection Preventionist Training recommended practices,
Course“ implementation resources
• 19 hours CE credits & certificate
https://www.train.org/cdctrain/traini of completion
ng_plan/3814 • Completion of course will
provide the required specialized
training
www.proactivemedicalreview.com 32Mastering the Infection Control Focused Survey June 2021
F880 Infection Control
• §483.80 Infection Control
• The facility must establish and maintain an infection prevention and control program
designed to provide a safe, sanitary and comfortable environment and to help
prevent the development and transmission of communicable diseases and
infections.
• System for preventing, identifying, reporting, investigating, and controlling infections and
communicable diseases
• Written standards, policies, & procedures for the program
• System for recording incidents and corrective actions taken
• Handling of linen
• Annual review & update of IPCP
• Antibiotic stewardship program (see F881)
Source: Appendix PP State Operations Manual Pg. 634‐661
F880 Citations
www.proactivemedicalreview.com 33Mastering the Infection Control Focused Survey June 2021
F880 Citations
• As of 05/23/2021 data in CASPER
• 9,016 citations nationally in FY 2020
• 6,996 citations nationally in FY 2021
• 49 Citation in KY in FY 2021(1 IJ)
• Cited in 4 of the 12 annual surveys completed
Source: CASPER (05/23/2021)
F880 KY Immediate Jeopardy Citation
• Facility noted to have 88 COVID + residents & 10 COVID deaths
• The facility's failure to implement their COVID‐19 Action Plan, their Infection Control Policy, and the Health
Department's recommendations resulted in a failure to provide a safe and sanitary environment to help
prevent the development and transmission of communicable disease and infections, resulting in residents
being exposed to COVID‐19
• No signage on elevator on floor to alert staff it was a COVID‐19 positive unit, no PPE obviously
available, & no PPE disposal receptacle near elevator. Staff were not wearing gloves, masks, gowns, &
shoe coverings
• In green zone floor, staff were wearing N95, no eye protection, & only 2 hand sanitizer dispensers
were on opposite ends of hallways
• On Memory care unit, there were 6 + residents. No signage on rooms to indicate they were in droplet
precautions, no PPE available, & no PPE disposal receptacle in hall or in resident rooms. Resident’s
who were COVID + were cohorting with COVID negative residents. Staff were not wearing eye
protection. Staff observed with cloth mask on and masks below noses. Staff floating from COVID unit
to the unit, which also housed COVID negative residents and sharing equipment between the units
www.proactivemedicalreview.com 34Mastering the Infection Control Focused Survey June 2021
FY 2021 F880 KY CITATIONS –
Complaint or FIC
• The State Surveyor entered the main entrance of the facility to
conduct a FICS. The Staff Member posted at the Main Entrance of the
facility took the Surveyor's temperature; however, failed to assess the
Surveyor for COVID‐19 exposure and/or symptoms as indicated per
facility's policy.‐ cited in 2 facilities
• During meal pass on the floors CNA failed to wash and sanitize hands
between tasks for different residents which involved the entry and exit
to different resident rooms, including passing trays & repositioning
residents for meal.
• Residents in hall with masks under nose/chin & staff did not provide
redirection. Hskpr cleaned 2 rooms without changing gloves.
Source: https://www.cms.gov/Medicare/Provider‐Enrollment‐and‐Certification/CertificationandComplianc/FSQRS
05/27/2021
FY 2021 F880 KY CITATIONS –
Complaint or FIC
• Staff entered room of resident on contact & airborne precautions wearing
only goggles & mask, with no gown or gloves on. Staff exited the room with
rolled up gown in hands & walked down hall to dispose gown.
• Staff entered room of resident in droplet precautions without donning
gown. Gloves & Facemasks found lying on ground in parking lot, lawn, & in
courtyard.
• Plastic barrier separating COVID unit from rest of building was not securely
intact in upper corner & was detached from wall, leaving an opening 12‐18
inches where plastic was hanging down. Curtain not pulled between 2
residents in room that were in TBP for 14 day observation period
Source: https://www.cms.gov/Medicare/Provider‐Enrollment‐and‐Certification/CertificationandComplianc/FSQRS
05/27/2021
www.proactivemedicalreview.com 35Mastering the Infection Control Focused Survey June 2021
FY 2021 F880 KY CITATIONS –
Complaint or FIC
• Housekeeper placed dirty linens from COVID unit in an uncovered bin
in the Administrative conference room
• Failed to complete daily COVID symptom monitoring at least every 12
hours per facility protocol – cited in 2 facilities
• COVID‐19 unit had been set up in A Station, which was located just off
the front entrance to the facility. The front entrance door was not
locked and allowed entry to anyone, and there was no signage stating
A Station was a COVID Unit, which required transmission‐based
precautions to be in effect.
• Linens transported from rooms of residents in TBP in bags without
placing in closed container for transport
Source: https://www.cms.gov/Medicare/Provider‐Enrollment‐and‐Certification/CertificationandComplianc/FSQRS
05/27/2021
FY 2021 F880 KY CITATIONS –
Complaint or FIC
• CNAs failed to perform hand hygiene after disposing soiled linen from room
on COVID unit before entering another room to provide care and pushed
linen down in barrel and didn’t perform hand hygiene
• SRNA not using eye protection as required, SRNA removed isolation gown in
hallway, dietary staff prepping food with face mask pulled under chin, 3
rooms without signage to alert staff of droplet precautions
• 2 staff entered COVID + room without wearing N95 mask
• Extended use of disposable isolation gowns used for caring for residents in
orange (symptomatic, pending confirmation of COVID status) & yellow
(unknown status) zones , without changing between residents and reusing
same gown for 7 day period.
• Staff entered facility and went to nurses desk (in patient care area) to be
screened, without being screened at entrance
Source: https://www.cms.gov/Medicare/Provider‐Enrollment‐and‐Certification/CertificationandComplianc/FSQRS
05/27/2021
www.proactivemedicalreview.com 36Mastering the Infection Control Focused Survey June 2021
FY 2021 F880 KY CITATIONS –
Complaint or FIC
• Failed to place resident who went out 3x week for dialysis on TBP d/t
risk of contracting COVID when out of facility
• No PPE/signage on doors of residents on 14 day TBP following
admission
Source: https://www.cms.gov/Medicare/Provider‐Enrollment‐and‐Certification/CertificationandComplianc/FSQRS
05/27/2021
PREPARING FOR INFECTION CONTROL
FOCUSED SURVEYS
www.proactivemedicalreview.com 37Mastering the Infection Control Focused Survey June 2021
CDC Infection Prevention & Control
Assessment Tool (ICAR)
Assessment Tool
DOCUMENTATION TO SUPPORT COVID‐19
PREVENTION/RESPONSE EFFORTS
• Time line of actions • Additions to Facility Assessment
• ‐ Efforts to obtain PPE • Updates to staffing plans
• QSO Documents with • Policy and Procedure updates
documentation of when and
• Education provided
what you implemented
• Tools implemented
• State Department of Health
guidance • QAPI
• CDC and other lead agency • Screening & testing logs
guidance • Surveillance data
• Contact Tracing
www.proactivemedicalreview.com 38Mastering the Infection Control Focused Survey June 2021
COVID‐SPECIFIC POLICIES & PROCEDURES
• Activities • Optimizing Supply of PPE
• Admission/Re‐admissions • Quarantine/Isolation Units
• Cohorting • COVID‐19 Testing
• Communal Dining • Resident Screening
• Communication/Reporting • Return to Work
• Use of Skilled MCR Waivers • Training
• Donning/Doffing PPE • Transfer/Discharges
• Emergency Staffing • Transmission‐Based Precautions
• Environmental Cleaning • Visitor Restrictions
TRAINING & COMPETENCY ASSESSMENTS
• Respiratory hygiene/cough • Donning/Doffing PPE
etiquette • Processes/protocols for
• Environmental cleaning & transmission‐based
disinfection precautions
• Reprocessing of reusable • COVID‐19 symptoms
medical equipment • How COVID‐19 transmitted
• Hand hygiene • Screening criteria and work
• PPE use exclusions
www.proactivemedicalreview.com 39Mastering the Infection Control Focused Survey June 2021
2021 Annual Survey Citations in KY
Oct 2020 Citations (Recertification Surveys)
• F550
• Catheter bag hanging on bed frame, not in dignity bag & visible from hallway
• F577
• Survey results binder not easily accessible to residents & residents did not know where
results were kept for them to view
• F578
• Failed to provide signed portable DNR order and/or advance directives for 4 residents
• F580
• IJ r/t failing to immediately notify MD of blood glucose levels less than 60 per facility
protocol
• F585
• Failed to ensure personal property safe from loss for 1 resident with missing clothing
• F600
• IJ r/t failing to protect 3 residents from abuse r/t resident who could not consent to sexual
activity who wandered to another unit found engaging in sexual activity with a resident on
restroom floor & a resident reported being afraid of another resident who has behavioral
outbursts during resident smoke breaks
www.proactivemedicalreview.com 40Mastering the Infection Control Focused Survey June 2021
Oct 2020 Citations (Recertification Surveys)
• F602
• Failed to ensure narcotics were not misappropriated
• F610
• IJ r/t failing to conduct thorough investigation of allegation of sexual abuse involving
2 residents
• F622
• Failed to provide notice of discharge to resident who was discharged while an
inpatient in an acute care facility who they could no longer meet needs of
• F641
• Inaccurate MDS r/t admission MDS assessed as severe hearing impairment with
hearing aide & quarterlies for resident assessed as no hearing impairment or hearing
aides; MDS did not include assessment for prosthetics; behaviors not documented
on MDS
Oct 2020 Citations (Recertification Surveys)
• F656
• Failed to ensure 3 residents had a person‐centered comprehensive care plan developed and implemented
to address the monitoring of hydration status
• Failed to implement person‐centered comprehensive care plan for 14 residents – fall interventions not on
CP, no CP r/t catheter dignity bag or restorative care, CP not implemented r/t: completing weekly skin
assessments, non‐pharamacological interventions to decrease target behaviors, to monitor meal intake
(Cited as actual harm)
• IJ r/t not addressing specific sexual comments made by resident & how staff should respond to sexually
suggestive comments; CP not developed r/t advance directives, prosthetic devices; CP r/t fall prevention,
nail care, placement of meal tray, & off‐loading boots not implemented.
• IJ r/t failing to follow care plan r/t blood glucose monitoring & notifying MD of low blood glucose levels
• Wandergaurd not on resident per CP. Resident not transferred to w/c to watch TV per CP
• F657
• No evidence that care plans were reviewed & revised timely, after residents were identified with severe
weight loss, to include measurable objectives & individualized interventions to meet nutrition/hydration
needs or to meet needs for fall interventions implemented after resident falls (cited as actual harm)
• Failed to revise care plan r/t behaviors for 5 residents (actual harm)
• Failed to revise care plans after falls to reflect new interventions
• Care plan did not address use of heel protectors & didn’t revise CP to include behavior of throwing
cups/pitchers of fluids on floor & staff not leaving fluids at bedside
www.proactivemedicalreview.com 41Mastering the Infection Control Focused Survey June 2021
Oct 2020 Citations (Recertification Surveys)
• F660
• Resident left the facility for a medical appointment with family. The resident did not return to
the facility. The resident attempted to return to the facility later that evening but then left
again. The facility did not complete AMA documentation, or complete documentation on the
resident's medical record of the incident and the discharge. In addition, the facility did not
initiate referrals for home care for continued medical services for the safety of the resident
• F677
• Staff left meal tray in middle of room & didn’t reposition resident to eat when tray delivered.
Resident waited over 40 minutes for staff to respond to call light to be able to eat & a
Resident had long fingernails with black/brown substance underneath.
• Resident remained in bed during times ordered by MD to be out of bed
• F679
• Resident’s admission assessment noted that it was very important to the resident to go
outside for fresh air when the weather was nice; however, observations and interviews
revealed that the resident was not given the opportunity to spend time outside
• Resident with signage in room stating she enjoyed music observed in room with silence
Oct 2020 Citations (Recertification Surveys)
• F684
• IJ r/t failing to follow facility protocol/standards of practice r/t low blood
glucose levels
• F686
• Failed to apply heel protectors as recommended after heels noted to be
reddened & boggy & failed to identify & monitor St. 1 to palm r/t
contracture
• Staff didn’t place heel protectors on resident, failed to order bed cradle per
wound clinic request, & didn’t maintain & provide up to date wound clinic
orders (Actual Harm)
• Heel protectors not implemented per orders
• F688
• Failed to ensure 7 residents who entered the facility without limited range of
motion (ROM) did not experience a reduction in
www.proactivemedicalreview.com 42Mastering the Infection Control Focused Survey June 2021
Oct 2020 Citations (Recertification Surveys)
• F689
• Resident who was assessed by the facility to need nectar thicken liquids and was noted to have access
to thin liquids
• Resident with 3 falls from bed in 11 hour timeframe did not have timely interventions implemented &
CP not revised timely with intervention status
• Failed to provide adequate supervision to prevent fall with injury & privacy curtain pulled to obstruct
visual supervision for resident with history of falls
• Failed to put interventions in place after falls to prevent falls
• Failed to supervise & ensure placement of wandergaurd for resident at risk for elopement
• F692
• Failed to ensure 5 residents maintained sufficient fluid intake to maintain proper hydration & health
• 5 residents went 45‐57 days without being weighed & had weight losses of 6‐13% (Actual harm)
• Failed to monitor fluid intake to ensure residents were meeting their fluid needs
• F694
• Nurse did not change stabilization device or needless endcap when performing Central Line dressing
change
Oct 2020 Citations (Recertification Surveys)
• F695
• Resident observed to receive O2 at 2L had order to receive at 3L.
• Did not have an AMBU at resident with trach bedside per policy
• F700
• Failed to ensure bed rails were removed per prior POC for 1 resident
• F725
• Failed to provide sufficient staff to provide scheduled showers, failed to provide hydration & ice to residents during shift, didn’t
complete unit staffing assignments, delays in answering call lights, & unable to meet 1:1 needs on memory care unit
• F726
• IJ r/t failing to ensure competence r/t providing care for residents requiring blood glucose monitoring & implementing facility
protocol for managing low blood sugar
• Failed to follow standards practice when suctioning/providing trach care‐ reached over sterile field several times, provided care
with back toward resident, didn’t clean stoma, didn’t oxygenate between suctions or monitor oxygen level
• F732
• Observation of the posted Nurse Staffing Information revealed the total number & the actual hours worked by licensed &
unlicensed nursing staff directly responsible for resident care was not posted for each shift
• F740
• Resident displayed various unwanted behaviors and stated he/she was in a prison; however, the facility did not provide the
resident with behavioral health services.
www.proactivemedicalreview.com 43Mastering the Infection Control Focused Survey June 2021
Oct 2020 Citations (Recertification Surveys)
• F741
• Failed to provide staff with the competencies and skill set to provide care to residents with mental and psychosocial
disorders r/t resident found in sexual act with other resident
• F744
• Staff pulled & privacy curtain of dementia resident in a manner which blocked the visual observation of the resident
and activity from the hallway. The resident remained in bed in a room without audible stimulation. The resident
yelled out for help and screamed with staff in the area, without response. (Actual Harm)
• F758
• No evidence non‐pharmacological interventions were used prior to administering PRN psychotropic med & failed to
ensure PRN orders for psychotropics were limited to 14 days
• F760
• Medication not started until 13 days after ordered
• F761
• 5 vials of medication opened, but with no open date on the label; 4 expired bottles of eye drops; and, 1 expired
inhaler available for staff to administer to residents
• 15 expired individually wrapped capsules in med cart
• Medication refrigerators in med rooms didn’t have locks on outside to secure mediations
• F765
• Failed to ensure controlled drugs were stored in a permanently affixed compartment as required in med room
refrigerator
Oct 2020 Citations (Recertification Surveys)
• F803
• Failed to provide alternate meals when requested
• F812
• No temp log on unit & resident refrigerators
• Ice buildup on containers in walk‐in‐freezer
• On 9/29, temp log was completed for entirety of month through 9/30
• F835
• Failed to have system in place to ensure audits were completed per the Acceptable Plan of Correction for
prior survey & failed to identify concerns with ROM & put interventions in place to prevent avoidable
declines (Actual Harm)
• IJ r/t failing to protect resident from abuse & repeat citations on 3 recertification surveys
• F837
• Failed to ensure the Governing Body, or designated persons functioning as a Governing Body, was
responsible & accountable for the QAPI program, related to the facility’s prior Acceptable POC (Actual
Harm)
• F838
• failed to conduct and document a facility‐wide assessment to determine what resources were necessary
to care for its residents competently during both day‐to‐day operations and emergencies; and review
and update that assessment, as necessary. Observation of the dry storage revealed there was not a 3 day
food storage for emergencies.
www.proactivemedicalreview.com 44Mastering the Infection Control Focused Survey June 2021
Oct 2020 Citations (Recertification Surveys)
• F842
• Narcotics that were signed out on narc sheet were not documented as administered on MAR
• F865
• Failed to maintain a QAPI Program that developed & implemented effective plans of action to
correct quality deficiencies. This was evidenced by the repeat deficiency from the
Abbreviated/Partial Extended Survey (Actual Harm)
• F867
• QAPI committee failed to identify quality deficiencies, take actions aimed at performance
improvement, track performance to ensure that improvements were realized and sustained
related to citations of F‐689, F‐692, F‐700, F‐758, and F‐865. This resulted in harm to 5
residents related to the facility's failure to have an effective plan to self‐identify quality of care
concerns, and implement a plan, to prevent the worsening significant/severe weight loss for
these residents. (Actual Harm)
• Failed to ensure to follow QAPI policy for conducting QAPI activities r/t repeat deficiencies
Oct 2020 Citations (Recertification Surveys)
• F880
• Failing to don appropriate PPE before entering room, staff who was not able to obtain temp
with infra‐red thermometer proceeded to clinical hallway, screener touched surveyors head
with thermometer & failed to clean between each person, staff smoking without social
distancing, social distancing & masks not maintained between residents while visiting on patio,
staff with mask worn under nose, laundry staff not wearing mask in laundry room while
handling linens
• Failed to utilize proper PPE & hand hygiene during meal tray delivery. Dirty trash bag on floor
in hallway
• Failing to don gown when entering room to talk to resident and deliver tray for resident on
droplet precautions.
• Staff did not wash hands after contact with residents, and failed to sanitize the equipment
used to obtain vital signs, and the pulse oximeter.
• F883
• Did not administer flu vaccine or document informed consent/declination of vaccine for 2
residents
www.proactivemedicalreview.com 45You can also read