Medical Cannabis and its Role in Chronic Pain Management - Gregory T Carter, MD, MS - Russo CME
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Medical Cannabis and its
Role in Chronic Pain
Management
Gregory T Carter, MD, MS
Spokane Pain Conference
November 10, 2018 2:30-3:30 PM
The Centennial Hotel
303 W North River Dr
Spokane, WA 99201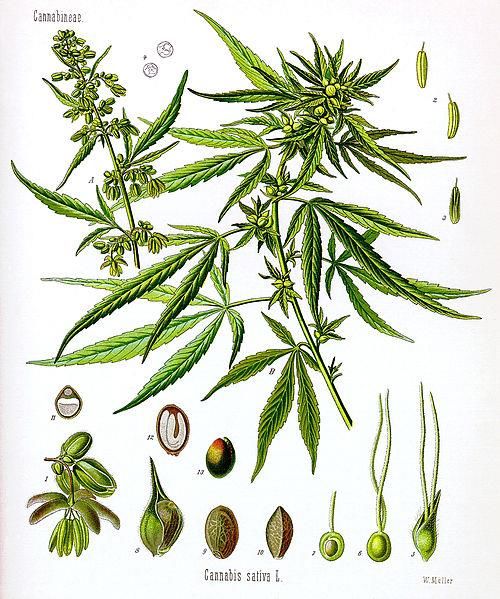
Disclosure: Educational Grant Support Cy Pres grant, #12-2-39485-7, awarded to the University of Washington Alcohol & Drug Abuse Institute; PI Dr. Bia Carlini; speaker is subPI Funding awarded to support research and education on the medicinal uses of cannabis in WA state Website for on-line physician training: http://adai.uw.edu/mcacp/ Speaker has no other disclosures
Learning Objectives I: At the conclusion of the presentation the attendee will be able to - Understand historical aspects of medicinal cannabis describe the major pharmacological effects of cannabinoids that are applicable to chronic pain Understand the current state of research and data base
Learning Objectives II: At the conclusion of the presentation the attendee will be able to - explain and describe the risks and benefits of cannabis use in this setting explain and describe the physiological changes occurring with activation of the endocannabinoid system through cannabis use Describe practical applications in a clinical setting
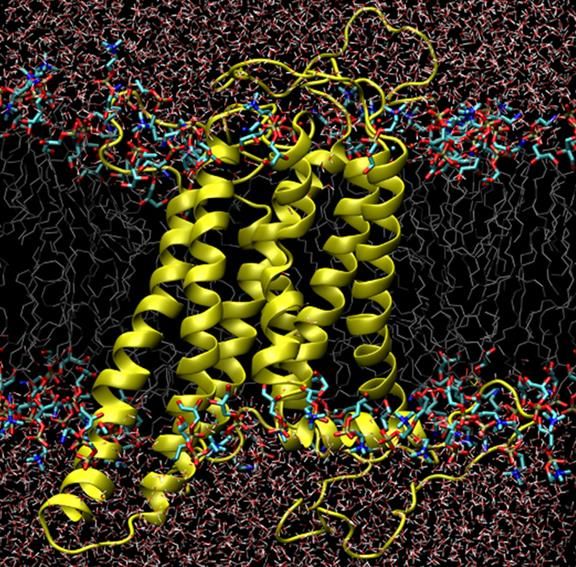
History The cannabis plant dates back approximately 35 million years. Cannabis sativa among the oldest agricultural crops in the world, cultivated for at least 10,000 years. It has been used as a food, a nutraceutical, herbal medicine, prescription medicine and spiritual/recreational intoxicant for all of recorded human history.
History
Pain is the most common symptom that drives
patients to see a health care provider.
Cannabis has long been used as an analgesic
Its analgesic properties are noted in most, if not all,
“materias medica” ever written. Ancient medical
texts, both far and middle east
Pen Ts'ao Ching -the earliest Chinese pharmacopoeia
The Pen Ts'ao Ching was passed on by oral traditions
established by 2700 BC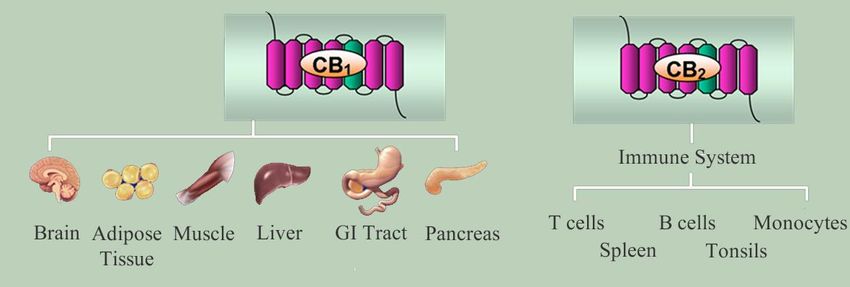
History in the USA Important crop: cultivated for fiber, rope, clothing, seeds for oil and fuel. Cannabis based medications were produced by Eli- Lilly, Parke Davis, and Sharp Dohme (now Merck Sharp Dohme). Prescribed by physicians in the United States 1890- 1937.

Historical Use in USA
Historical Use in USA Medicinal cannabis products were manufactured by such well known pharmaceutical firms as Eli Lilly, Squibb, Merck, Parke-Davis, Sharp and Dohme, and the Smith Brothers. In the early 20th century cannabis was a common constituent of both physician’s prescriptions and an ingredient in patent medicines. In the 1920s American physicians wrote three million cannabis-containing prescriptions per year.

Eradication History 1930 - Use of cannabis under increasing scrutiny by Federal Bureau of Narcotics (FBN). 1937 - The Marijuana Tax Act made possession or transfer of cannabis illegal throughout the United States under federal law. The American Medical Association (AMA) opposed the act 1942 - All use of cannabis was criminalized in the United States by 1942 and still remains as such under Federal law
Characterization History 1964 - THC (Tetrahydrocannabinol) first isolated as an aromatic terpenoid in Israel by Dr. Raphael Mechoulam By comparison morphine isolated in early 19th century, cocoa and cocaine in middle 19th century. Discovered earlier because called morphine and cocaine are alkaloids, which will precipitate out as a salt – very easy to prepare. THC is the main psychoactive substance in cannabis and thought to be the primary ingredient for years
Characterization History By mid 1970s Elisandro Carlini studied cannabidiol (CBD) – shows analgesic and anti-epilipetic effects in animal models CBD originally believed to be precursor to THC. Now known that CBD and THC are produced independently Other cannabinoids discovered in the following years CBN (Cannabinol), CBV (Cannabivarin), THCV (Tetrahydrocannabivarin), among many others
Turning Point: Discovery of Endocannabinoid System Intricately involved in normal human physiology. Cannabinoid receptors are found in the brain and peripheral tissues – nerves, gut, immune cells. Dense receptor concentration in the cerebellum, basal ganglia, and hippocampus. Few cannabinoid receptors in the respiratory areas in brainstem. The cannabinoid receptors CB1 and CB2, two G protein- coupled receptors that are located in the central and peripheral nervous systems, and ubiquitously throughout human physiological systems.
The Endocannabinoid System Endocannabinoids are both neuromodulators and immunomodulators. Controls pain, appetite, mood, sleep, gut motility, muscle coordination, short term memory. Inflammatory levels – endocannabinoids suppress inflammation. Activation of cannabinoid receptors leads to activation of GTPases in macrophages, neutrophils, and B/T cells. CB2 receptors regulate migration of B cells and maintain healthy IgM levels.
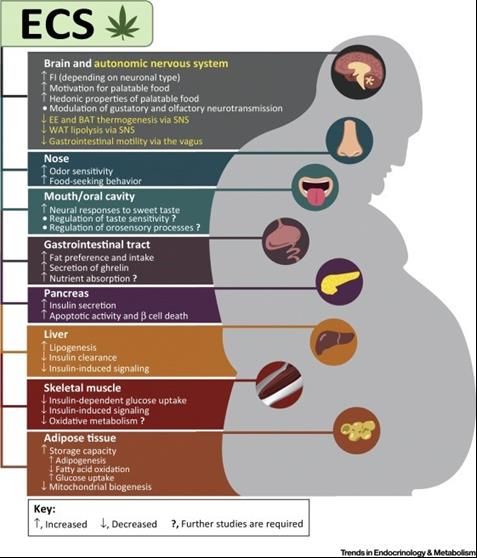
Physiological Effects of Endocannabinoids
Endocannabinoids are often produced as an adaptive
response to cellular stress, aimed at reestablishing cell
homeostatis. “Runner’s high”
Endocannabinoids affect a large number of physiological
processes including:
• Feeding behavior • Learning, memory emotions
• Energy balance, metabolism, GI • Immune and inflammatory
responses
function
• Cardiovascular function
• Pain perception
• Reproduction
• Motor control and posture
• Bone formationCannabinoid Receptors
G-protein-coupled receptors
CB1 receptors highly expressed in the brain
--CB1 receptors also found in adipose tissue, liver, muscle, the GI tract,
pancreas, and reproductive and cardiovascular tissue.
CB2 receptors are expressed primarily in immune cells
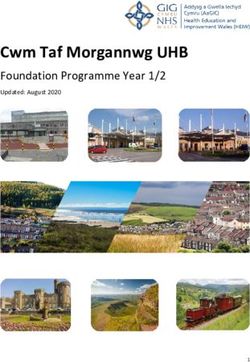
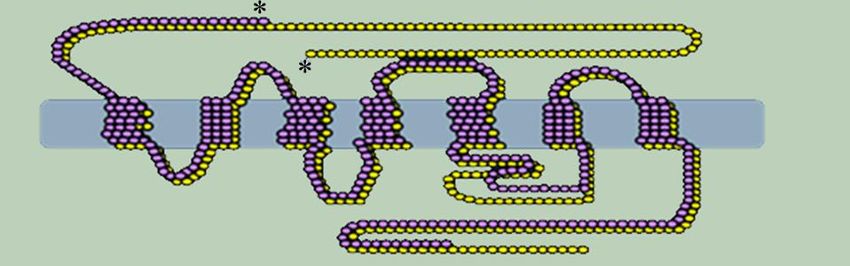
CB2 receptor expression in neurons is being studied.The CB1 Receptor
The CB1 receptor consists of 7 transmembrane helices.
Courtesy of Patricia Reggio, PhDKey ECS Elements
Cannabinoid receptors are G-protein-coupled receptors • Central nervous system
- Hippocampus
- Basal ganglia
- Cortex
- Cerebellum
- Hypothalamus
- Limbic structures
- Brainstem
• GI tract (myenteric neurons
and epithelial cells)
*360 *472
• Liver (hepatocytes)
CB1 receptor • Adipose tissue
Endocannabinoids
• Muscle
• Pancreas (α-cells)
2-Arachidonoyl-glycerol • Immune cells and tissues
Anandamide - T cells, B cells
- Macrophages
Endogenous, phospholipid-derived metabolites that bind - Dendritic cells
to and activate cannabinoid receptors. - Spleen, tonsils
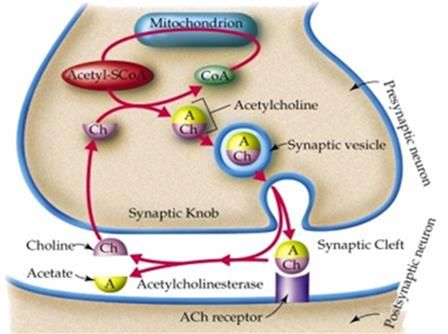
CB2 receptor - Adipose tissueDifference Between Classical & Retrograde Neurotransmission
Classical neurotransmitter Retrograde neurotransmitter
Presynaptic Presynaptic
Postsynaptic PostsynapticCannabis plant: cannabinoids, terpenoids and more Major Cannabinoids Tetrahydroncannabinol (THC) – mind altering properties Cannabidiol (CBD): analgesia; moderates effects of THC. Cannabinol (CBN): anticonvulsant. Tetrahydrocannabivarin (THCV): anti-inflammatory. Cannabichromene (CBC): mixed effects. Cannabicyclol (CBL)
Types of Cannabis Plants Type 1: High THC, Low or No CBD* Type 2: Equal amounts of THC and CBD** Type 3: Low THC, High CBD/CBN** *generally preferred for recreational use **generally preferred for medical use
Indica vs Sativa Indica: short dense plants, darker green; higher amounts of THC and lesser CBD/CBN or equal amounts THC/CBD produced (type 1&2 plants). Sativa: tall, thin plants, light green, reach heights of 20 feet. Sativa plants typically have lower overall THC content than Indica plants. May produce higher amounts of CBD. Type 3 plants. Hemp is a subspecies of Sativa plants
Research: what is the data base? PubMed search done one 9/2/2018 Opioid = 150,323 marijuana = 28,241 Opiate = 20,615 Cannabis = 18,506 Methadone = 15, 744 Cannabinoids = 15,566 Oxycodone = 3339 Hydrocodone = 1070
Research on Cannabis Due to restrictions on research the animal model/basic science data base is far more extensive than human studies Primarily done in rodent models Some work done in primates Variable delivery systems and outcome measures
Conducting clinical research using cannabis: Drug Enforcement Admin (DEA) - Schedule I DEA provides researchers with a special registration and has certain requirements at the site cannabis will be studied. Funding from National Institute on Drug Abuse (NIDA) within the National Institutes of Health NIDA provides cannabis from the University of Mississippi
Human Research - Evaluation of medicinal cannabis in
humans is still evolving – but remains significantly restricted
due to Federal laws in US
COMPARED TO PHARMA - Studies are small, imperfectly
controlled, use smoked cannabis, limited by regulations (NIDA
budgets of $500,000 versus millions in industry trials). trials are
small – typically single centered, short duration
Feds require using Mississippi cannabis -poor composition and
irregular bioavailability. Historically delivered as cigarettes -
delivery system suboptimal – smoking
The discovery of the endocannabinoid system has stirred
research interest from industry – still laws make research
difficult since cannabis is schedule 1. Won’t have
industry/pharma funding until that changes.Patient reports of efficacy and the Internet Internet = new source of patient reported data. Widely available to both clinicians and the public This has led to melding of peer-reviewed data and anecdotal reporting. This creates challenges in terms of improving the quality and safety of medical care. There is scientific evidence and “real-world evidence”—that is, evidence derived from data gathered from actual patient experiences, in all their diversity How we may adapt “real-world evidence” into scientific evidence is a daunting task
Cannabis and Evidence-based medicine (EBM) Historically recorded use of cannabis as medicine dates back thousands of years EBM is a relatively new concept, coming of age only in the last quarter century and partly driven by technological developments (modern computers and the internet) Today most nationally funded health care systems in the United States are basing practice guidelines on EBM. Goal is standardizing practice through EBM clinical practice guidelines (CPG).
Example of a well done EBM Class 1 Study on
smoked cannabis for neuropathic pain
Abrams DI, Rowbotham MC, Petersen KL, et al. Cannabis in painful HIV-
associated sensory neuropathy: a randomized placebo-controlled trial.
Neurology 2007; 68(7):515-21.Metanalysis of Human Data for pain Phillips TJ, Cherry CL, Cox S, Marshall SJ, Rice AS. Pharmacological treatment of painful HIV-associated sensory neuropathy: a systematic review and meta-analysis of randomised controlled trials. PLoS One 2010; 28;5(12):e14433. Martín-Sánchez E, Furukawa TA, Taylor J, Martin JL. Systematic review and meta-analysis of cannabis treatment for chronic pain. Pain Med 2009; 10(8):1353-68. Campbell FA, Tramèr MR, Carroll D, Reynolds DJ, Moore RA, McQuay HJ. Are cannabinoids an effective and safe treatment option in the management of pain? A qualitative systematic review. BMJ 2001; 323(7303):13-6. Machado Rocha FC, Stéfano SC, De Cássia Haiek R, Rosa Oliveira LM, Da Silveira DX. Therapeutic use of Cannabis sativa on chemotherapy-induced nausea and vomiting among cancer patients: systematic review and meta-analysis. Eur J Cancer Care 2008;17(5):431-43.
Lynch ME et al., 2011 review Lynch ME, Campbell F. Cannabinoids for Treatment of Chronic Non-Cancer Pain; a Systematic Review of Randomized Trials. Br J Clin Pharmacol 2011 2(5):735-44 PMID: 21426373 Systematic review of RCTs for cannabis treating chronic non-cancer pain: neuropathic pain, fibromyalgia, rheumatoid arthritis, and mixed chronic pain. Quality of trials = excellent. 15 of the 18 trials showed significant analgesic effect of cannabis. No serious adverse effects; only a few withdrawals from the studies. Overall evidence indicates that cannabinoids are safe and effective.
Lynch ME et al., 2015 f/u review
Lynch ME, Ware MA. Cannabinoids for the Treatment of Chronic Non-
Cancer Pain: An Updated Systematic Review of Randomized Controlled
Trials. J Neuroimmune Pharmacol. 2015; 10(2):293-301
Eleven new trials
Quality of trials excellent.
Seven trials showed significant analgesic effect.
Several trials also showed improvement in sleep, muscle stiffness and
spasticity
Adverse effects most frequently reported such as fatigue and dizziness were
mild to moderate in severity and generally well tolerated.
This review adds further support that currently
available cannabinoids are safe, moderately effective
analgesics that provide a reasonable therapeutic
option in the management of chronic non-cancer pain.Hill KP. Medical Marijuana for Treatment of Chronic Pain and Other
Medical and Psychiatric Problems: A Clinical Review. JAMA 2015; 23-
30;313(24):2474-83
Use of marijuana for chronic pain, neuropathic pain,
and spasticity due to multiple sclerosis is supported
by high-quality evidence.
Six trials that included 325 patients examined
chronic pain
6 trials that included 396 patients investigated
neuropathic pain
12 trials that included 1600 patients focused on
multiple sclerosis
“Several of these trials had positive results,
suggesting that marijuana or cannabinoids
may be efficacious for these indications”Cohen NL, Heinz AJ, Ilgen M, Bonn-Miller MO. Pain, Cannabis Species, and Cannabis Use Disorders. J Stud Alcohol Drugs. 2016 77(3):515-20. 163 medical cannabis users completed assessments of medical cannabis use motives, history, preferences (species type), and problems, as well as current pain level. Individuals who used cannabis to manage chronic pain experienced fewer cannabis use problems than those who did not use it for pain; among those who used it for pain, the average pain level in the past week was not associated with cannabis use problems. individuals who used cannabis for chronic pain were more likely to use indica over sativa.
Mücke M, Phillips T, Radbruch L, Petzke F, Häuser W. Cannabis-based
medicines for chronic neuropathic pain in adults. Cochrane Database Syst
Rev. 2018 2018 Mar 7;3:CD012182
included 16 studies, 1750 participants.
studies ranged from 2 to 26 weeks long
Study quality: low in 2 studies, moderate in 12
studies and high in 2 studies.
9 studies were at high risk of bias for study size.
Cannabis-based medicines increased
number of people achieving 50% or greater
pain relief compared with placebo (21%
versus 17%; - 95% confidence interval)Baron EP, et al Patterns of medicinal cannabis use, strain analysis, and substitution effect
among patients with migraine, headache, arthritis, and chronic pain in a medicinal cannabis
cohort. J Headache Pain. 2018 24;19(1):37
Chronic pain was the most common reason for cannabis
use, consistent with most registries. The majority of headache
patients treating with cannabis were positive for migraine.
Hybrid strains were preferred: high THC (Δ9-
tetrahydrocannabinol)/THCA (tetrahydrocannabinolic acid), low
CBD (cannabidiol)/CBDA (cannabidiolic acid), strain with
predominant terpenes β-caryophyllene and β-myrcene, most
preferred in the headache
May reflect the potent analgesic, anti-inflammatory, and anti-
emetic properties of THC, with anti-inflammatory and analgesic
properties of other cannabinoids and terpenoids
Prospective studies are needed, but results may provide early
insight into optimizing crossbred cannabis strainsSocietal Benefit overall reductions in Medicare spending when states implemented medical marijuana laws were estimated to be $165.2 million per year in 2013. Bradford AC, Bradford WD. Medical Marijuana Laws Reduce Prescription Medication Use In Medicare Part D. Health Aff (Millwood). 2016 1;35(7):1230-6. Medical cannabis laws are associated with significantly lower state-level opioid overdose mortality rates. Bachhuber MA, Saloner B, Cunningham CO, Barry CL.Medical cannabis laws and opioid analgesic overdose mortality in the United States, 1999-2010. JAMA Intern Med. 2014 ;174(10):1668-73.
Whiting PF, Wolff RF, Deshpande S, et al. Cannabinoids for Medical Use: A
Systematic Review and Meta-analysis. JAMA 2015; 23-30;313(24):2456-73.
79 trials (6462 participants) were included
Most trials showed improvement in
symptoms associated with use of
cannabinoids
nausea and vomiting
reduction in pain
reduction in spasticity
Common AEs included dizziness, dry mouth, nausea,
fatigue, somnolence, euphoria, vomiting,
disorientation, drowsiness, confusion, loss of
balance, and hallucinationUse discretion in reading literature Walitt B, Klose P, Fitzcharles MA, Phillips T, Häuser W. Cannabinoids for fibromyalgia. Cochrane Database Syst Rev. 2016 Jul 18;7:CD011694 This study actually only looks at nabilone. Nabilone is 100% THC, not the same thing as “cannabinoids” Authors found no convincing, unbiased, high quality evidence suggesting that nabilone is of value in treating people with fibromyalgia. The tolerability of nabilone was low in people with fibromyalgia.
Stockings E, et al Cannabis and cannabinoids for the treatment of people with
chronic non-cancer pain conditions: a systematic review and meta-analysis of
controlled and observational studies. Pain 2018 May 25.
no significant impacts upon physical or emotional
functioning
low-quality evidence of improved sleep and patient
global impression of change.
Evidence for effectiveness of cannabinoids in CNCP
is limited.
Effects suggest NNTB are high, and NNTH low, with
limited impact on other domains.
It appears unlikely that cannabinoids are highly
effective medicines for CNCP.
From NIDA; limited bibliography (40 references)Nielsen S, Sabioni P, Trigo JM, Ware MA et al. Opioid-Sparing Effect of
Cannabinoids: A Systematic Review and Meta-Analysis.
Neuropsychopharmacology 2017. 42(9):1752-1765
included pre-clinical and clinical studies
19 pre-clinical and 9 clinical studies met the search criteria.
17 of 19 pre-clinical studies provided evidence of synergistic
effects from opioid and cannabinoid co-administration.
pre-clinical studies indicate that the median effective dose
(ED50) of morphine administered in combination with delta-
9-tetrahydrocannabinol (delta-9-THC) is 3.6 times lower
(95% confidence interval (CI) 1.95, 6.76; n=6) than the ED50
of morphine alone. Thus pre-clinical studies provide robust
evidence of the opioid-sparing effect of cannabinoids,
Only 1 of 9 clinical studies identified provided very-
low-quality evidence of such an effect.
Prospective high-quality-controlled clinical trials
are required to determine the opioid-sparing effect
of cannabinoids.Abuhasira R, Schleider LB, Mechoulam R, Novack V. Epidemiological
characteristics, safety and efficacy of medical cannabis in the elderly. Eur J Intern
Med. 2018;49:44-50.
prospective study- included 2736 patients above 65 years of age who
received medical cannabis from January 2015 to October 2017 in clinic
Outcomes were pain intensity, quality of life and adverse events at six
months.
mean age was 74.5 ± 7.5 years.
The most common indications for cannabis treatment were pain (66.6%)
and cancer (60.8%).
After six months of treatment, 93.7% of the respondents reported
improvement in their condition and the reported pain level was reduced
from a median of 8 on a scale of 0-10 to a median of 4. Most common
adverse events were: dizziness (9.7%) and dry mouth (7.1%).
After six months, 18.1% stopped using opioid analgesics or reduced their
dose.
cannabis is safe and efficacious in the elderly population.
Cannabis use may decrease the use of other prescription medicines,
including opioids. Gathering more evidence-based data, including data
from double-blind randomized-controlled trials, in this special population
is imperative.Mari Carmen Torres-Moreno, Esther Papaseit, Marta Torrens, et al. Assessment of Efficacy
and Tolerability of Medicinal Cannabinoids in Patients With Multiple Sclerosis. A Systematic
Review and Meta-analysis. JAMA Network Open. 2018;1(6):e183485.
Cannabis safe for use in this population
Oral compounding only - results suggest a limited
efficacy of cannabinoids for the treatment of
spasticity, pain, and bladder dysfunction in patients
with MS.Using in clinical medicine Clinical Pharmacology Methods of use Dosing paradigms Side effects Patient instructions Risk/Benefits
CLINICAL PHARMACOLOGY OF CANNABIS
95-99% plasma protein bound -hydroxylation,
oxidation, and conjugation for rapidly clearance
from plasma
First-pass metabolism through liver (after PO
admin) to 11-OH-THC
Elimination is slow: days to weeks 20-35% found in
urine; 65-80% found in feces; stored in adipose;
Pregnancy Category C: in breast milk
Works through a known receptor based systemRoutes of delivery
• Smoking: fastest acting but irritates the bronchial tree.
• Vaporizing: 70% fewer irritants than smoking and preserves more cannabinoids
than smoking
• Water Pipe (Bong): Removes irritants and THC in equal proportions, cools
smoke but still smoking.
• Sublingual: Tincture applied under the tongue. Acts in about 15 minutes.
• Tea: Traditional form consumed for millennia in India. Can be made from leaves,
roots, or flowering tops. Usually made with milk or cream to absorb fat soluble
cannabinoids.
• Oral/Edibles: Take minimum of 45 to 75 minutes to act. l.
• Topical: Used for over a century by curanderos in Southern Mexico and Central
America to treat arthritis in hands and wrists.
• Prescription: Dronabinol (Marinol) (THC), Nabiximol (Sativex) (Canada, UK
and EU)
• Rectal: RSO suppositories.
• Juicing: The raw, newly picked plant (undried) has all its cannabinoids in the
acid form including THCa (the non-psychotropic precursor to THC,) CBDa, etc. There are
apparently no psychotropic effects from juicing the newly picked plant.
Methods of Use DO NOT SMOKE – Use vaporizer for fast effect. Oral or sublingual tincture ingestion for longer effect. Topical for local effect. Use low doses of cannabis that has high CBD/CBN and low THC. Do not need to be high to get pain relief.
Vaporization of Cannabis Safe alternative to smoking
How Do Vaporizers Work? When cannabinoids are heated to between 285 °F (140 °C) and 392 °F (200 °C) they boil and vaporize – “e-cigarette.” Studies show that vaporization is most effective at around 338 °F (170 °C). A vaporization temperature over 392 °F (200 °C) will burn the cannabis, creating unwanted smoke.
Dosing Paradigms
Self titration - START
LOW; GO SLOW.
Vapor: 2-3 inhalations,
stop, wait ten minutes.
Do not need to be high to
get pain relief.Side Effects Disinhibition, relaxation, drowsiness Feeling of well being, exhilaration, euphoria Sensory - perceptual changes Recent memory impairment Balance/stability impaired Decreased muscle strength, small tremor Poor on complex motor tasks (e.g., driving)
Effects on Behavior Can impair judgment. Slowed reaction time. Motor impairment. Disorganized thoughts, confusion. May get paranoia, agitation. Do Not Drive!
Clinical Effects no overdose, overall well tolerated if used as advised No constipation No respiratory suppression Relieves pain, improves sleep Improves appetite Works synergistically with opioids – potential to lower opioid dose -Decrease needs for opioids?
Advising the Patient Adverse effects: mainly seen in new users. Start low, go slow and easy. These are reversible, short lived effects (3-4 hours max). Serious adverse effects NOT seen in chronic users.
Authorizing a patient: Risk Evaluation and Mitigation Strategy Screen the patient – use standard the risk screening tools. Stratify treatment: If the patient is legit, try the standard non-opioid drugs first: AEDs, SSRIs, SNRIs, TCAs, etc. If the standard first line meds do not work then –consider CANNABIS before OPIOIDS. Start low go slow, Monitor for abberrant behavior and dependency If patient already on opioids, then use cannabis to lower their dose of opioids (and other meds).
Who may authorize in WA state? Physicians (MD/DO) Advanced Care Practitioners: Physician Assistants (PA-Cs) and Advanced Registered Nurse Practitioners (ARNP) Naturopathic Physicians (ND) Having authorization saves your patient money (less taxation) and allows them to possess more cannabis
For what conditions?
Cancer, human immunodeficiency virus (HIV), multiple
sclerosis, epilepsy or spasticity disorders.
Intractable pain (pain unrelieved by standard medical
treatments
Glaucoma
Crohn's disease
Hepatitis C with debilitating nausea or intractable pain
Diseases which result in nausea, vomiting, wasting,
appetite loss, cramping, seizures, muscle spasms, or
spasticity
chronic renal failure requiring hemodialysis.
Posttraumatic stress disorder.
Traumatic brain injury.
Mental health conditions don't qualifyDrug interactions
drug-drug interactions not well documented -
there is a need for more study
May decreases bioavailability of methadone
May enhance some anti-cholinergic side
effects: dry mouth, tachycardia
CBD may inhibit benzodiazepine
metabolism
Forms of cannabis with higher THC concentration
may enhance cognitive and psychomotor
effects of other medications and intoxicants –
this is particularly important when counseling the
patient regarding drivingOther effects Medical cannabis also has similar adverse effects as the FDA-approved cannabis-based medications mainly consisting of: CNS related adverse effects Cardiovascular –tachycardia, possible hypotension respiratory related adverse effects not common unless smoked. Cannabinoids are bronchodilators and may improve some forms of reactive airway disease
Final comments
Patient should use high quality cannabis to
improve efficacy: high CBD, CBN, lower
THC –
do not need to be high to get pain relief
use a delivery route that maximizes benefits and
minimizes side effects.
Cannabis is not for everyone - Some people cannot
tolerate it or it does not work for them.
There is a risk for psychological addiction.
Tolerance may develop in heavy, long term users -
may need higher doses.
Patient/family will have to purchase or grow it still
some social stigma.What About Marinol? 100% THC in pure form is a schedule 3 drug (Marinol). Natural cannabis at 3 - 15% THC is schedule I, dangerous, no medical use. Purification and concentration is NOT always a good thing. Effective medical cannabis = low THC, high in other cannabinoids. Marinol is a powerful sedative hypnotic, prescribe with caution
Newer Products – Sativex 1:1 combination from two clonal cannabis cultivars yielding a high THC extract and a high CBD extract THC and CBD comprise some 70% (w/w) of the total BDS Each 100 μL pump-action spray provides 2.7mg of THC and 2.5mg of CBD Intermediate onset: 15-40 minutes Allows dose titration; Reduces first pass metabolism Not avail in USA now
Epidiolex is a formulation of CBD. Like Sativex, it is derived from cannabis contains no THC Approved here for Lennox-Gastaut Syndrome (refractory seizures). No data on chronic pain
Thank you Questions/Discussion
You can also read