Medicare Update Webinar: The Financial Impact of the CMS Final Fee Schedule Rule on Ophthalmic Practice
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Medicare Update Webinar: The Financial Impact of the CMS Final Fee Schedule Rule on Ophthalmic Practice David B. Glasser, MD, Secretary for Federal Affairs Michael X. Repka, MD, MBA, Medical Director for Governmental Affairs Kayla L. Amodeo, PhD, Director, Health Policy Moderator: Sue Vicchrilli, Director, Coding & Reimbursement

Topics
• Medicare Physician Fee Schedule Impact Overview and Advocacy
o Coding Changes for CY 2021
▪ Revised Codes
▪ Revalued Codes
▪ New Codes
• Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical
Center (ASC) payment rule CY 2021 Update
• Medicare Value-Based Payment Overview and CY 2021 Update
• Most Favored Nations Interim Final Rule
2
CY 2021 Medicare Physician Fee
Schedule Impact Overview and
Advocacy
3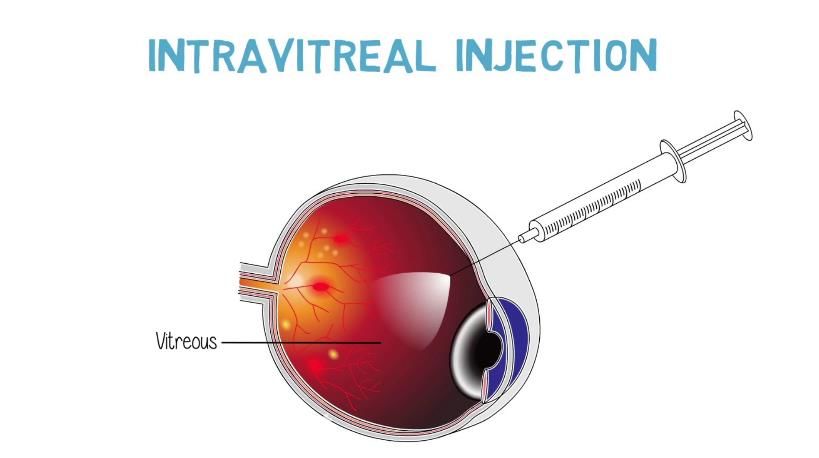
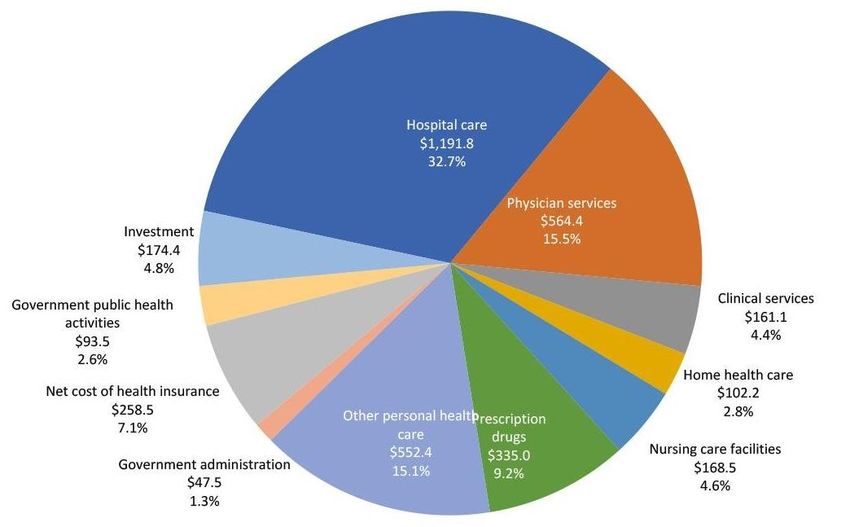
Annual US Healthcare Spending
All Spending: $3,649 Billion Medicare Spending: $842 Billion
4
Inflation-Adjusted Medicare Payment Updates
10%
5%
0%
Physician
-5%
Hospital Inpatient
-10% Hospital Outpatient
-15% SNF
-20%
-25%
-30%
01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19
5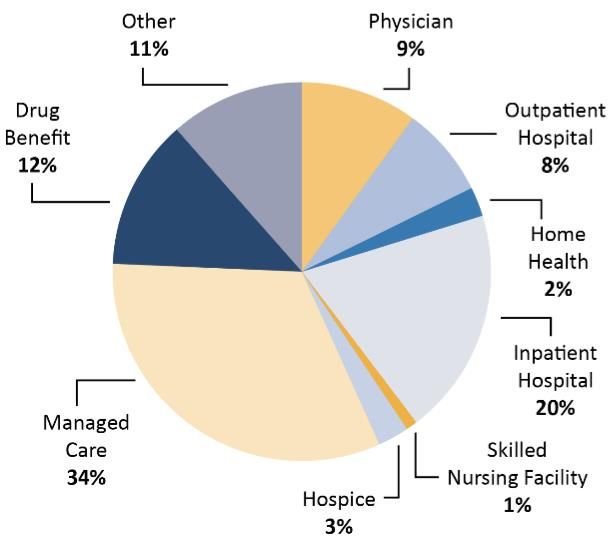
Medicare Physician Fee Schedule
• “Unconscionable” payment cuts must not be implemented. “Physicians
are already experiencing substantial economic hardships due to COVID-19,
so these pay cuts could not come at a worse time,” Dr. Bailey said.
610.2% reduction in the Medicare CF - Why?
• Budget neutrality: decreases payments for all services by reducing CF
o Triggered by anticipated expenditure increases greater than $20 million
• $10.2 billion increase in spending targeting primary care
o $5.6 billion: RUC-recommended increased payments for E/M services
o $3.3 billion: New CMS-created add-on complexity code for E/M services
o $1.3 billion: Other CMS-approved increases
Winners Losers
Endocrinology +17% Radiology -11%
Rheumatology +16% Thoracic Surgery -8%
Heme/Onc +14% Vascular Surgery -7%
Family Practice +13% Ophthalmology -6%
7Common Theme: Give More $ To Primary Care
ASSUMPTIONS
• There are too few PCPs, too many proceduralists
o Healthcare workforce predictions since 1910 share one characteristic: all have been
wrong
• PCP management is the answer to out-of-control spending
o Has not been demonstrated outside of capitated or salaried systems
• More PCPs will improve access to care
o Lack of insurance, high deductibles/copays are primary barriers to access
8Common Theme: Give More $ To Primary Care
• Zero sum game: payment being shifted from specialty/surgical care
o Last 10 years: primary care increases 14-18%, specialty decreases 1-20% (81%
IDTF)
• Politically driven, based on multiple flawed assumptions
• Increased payments for “cognitive” care will attract more PCPs
o PCP payments have already increased
9The Details – Surgery
CPT Code 2021 Facility 2021 Change
15823 $519 -8%
65222 (office) $64 -7%
65855 (office) $233 -8%
65756 $1,096 -9%
65780 $627 -8%
66170 $1,023 -8%
66172 $1,118 -8%
66761 (office) $286 -7%
66982 $696 -9%
66984 $508 -9%
67028 (office) $106 +3% (PE)
67028 (facility) $86 -15%
67036 $837 -9%
67108 $1,109 -9%
67110 (office) $841 -7%
67113 $1,240 -9%
67228 (office) $319 -9%
68761 (office) $142 -6%
68815 $208 -8%
10The Details – Office Visits, Tests
CPT Code 2021 Allowable 2021 Change
92002 $81 -5%
92004 $142 -7%
92012 $85 -6%
92014 $120 -7%
92083 $60 -6%
92132 $30 -6%
92133 $35 -8%
92134 $39 -7%
92235 $112 +6% (PE)
92240 $196 -5%
92250 $37 -19%
92285 $22 -2%
99202 $69 -10%
99203 $107 -3%
99204 $160 -4%
99205 $212 0%
99212 $54 +18%
99213 $87 +14%
99214 $123 +12%
99215 $173 +17%
11Academy is Fighting the Reimbursement Cuts
• Through the Surgical Care Coalition with American College of Surgeons
o AAO, 11 surgical specialties raised $2 million, launched PR campaign in June
• Through a broad coalition including non-surgical provider groups
o Radiology, Emergency Physicians, Occupational and Physical Therapists,
Anesthesiology, and Gastroenterology
• We continue to support the RUC process and recommended increases to
E/M values – these can benefit ophthalmologists as well as primary care
This is not the time to make cuts to health care and Medicare while the
U.S. healthcare system is under tremendous strain and financial stress,
and patients need high-quality care now more than ever.
12Solutions Congress is Considering
• Pressure CMS to revise 2021 fee schedule (did not move CMS)
• Waive budget neutrality for 1 year – Rep. Burgess
• Delay cut 6 months until new administration in place
• Surgical Care Coalition position:
o Apply E/M increases to post-op visits in global period (4.6% gain)
o Eliminate or delay complexity add-on code until RUC can review/value (2.4% gain)
o Hold codes harmless that would lose value from E/M increase:
HR 8702 (Bera/Bucshon)
Holding Providers Harmless from Medicare Cuts During COVID-19 Act of 2020
Delays cut 2 years giving the Administration and Congress time to revise the policy
13Coding Changes CY 2021
14Payment Based on Relative Value Since 1992
• RUC votes on values, makes recommendations to CMS
• Physician work: WRVUs
o Based on time and intensity of work on date of service and postop visits
o Survey-derived data compared relative to other procedures
• Practice expense: PERVUs
o Based on clinical staff time, equipment costs and time used, supplies
• Professional liability insurance cost: PLIRVUs
o Based on national trends for malpractice premiums
• Total Value = (WRVU + PERVU + PLIRVU) x CF (2021 = $32.4085)
15Steep Drop in Physician Payment in 2021
• Relative value units (RVUs) are
multiplied by a conversion factor
set by CMS to convert the RVUs
into payment rates
• The finalized 2021 conversion
factor is $32.41, a decrease of
$3.68 (-$10.2%) from the 2020
rate of $36.09
• Lowest since 1993
16Evaluation and Management Code Changes
• Scheduled to go into effect January 2021
• Eliminates the level 1 new patient code (99201)
• Introduces prolonged service and complexity add-on codes
• Substantial increases in payment for level 2-5 office visits
• E&M increases not applied to value of
o Postop visits: $115 million increase in Medicare payments to ophthalmology
o Eye codes (92002-92014): $267 million increase in Medicare payments
17New Patient E&M Work Values (2021)
Current Office
CPT Code New Office Pay Percent Change
Pay
99201 $46.56 Deleted N/A
99202 $77.23 $69.03 -10.6%
99203 $109.35 $106.30 -2.8%
99204 $167.09 $159.77 -4.4%
99205 $211.12 $210.98 -0.1%
18Established Patient E&M Work Values
(2021)
Current Office
CPT Code New Office Pay Percent Change
Pay
99211 $23.46 $22.04 -6.1%
99212 $46.19 $54.12 17.2%
99213 $76.15 $86.85 14.1%
99214 $110.43 $123.48 11.8%
99215 $148.33 $172.74 16.5%
19Coding Changes CY 2021
Revised for 2021 Revalued for 2021 New codes
• Trabeculostomy Ab Interno • Ophthalmic ultrasound • Remote Retinal OCT
(0621T, 0622T) anterior segment (76513) (0604T-0606T)
• Ophthalmic ultrasound • Remote retinal imaging • Iris Prosthesis Procedures
anterior segment (76513) (92227 and 92228) (0616T-0618T)
• Remote retinal imaging • Intravitreal injection (67028) • Imaging of retina using AI
(92227, 92228, 92229) (92229)
• Visit complexity inherent to
certain E/M (G2211)
• Prolonged services (G2212)
• PPE supplies during
COVID-19 (99072)
20Revised Codes
21Cat III Trabeculostomy Ab Interno
• 0622T was established to report use of ophthalmic endoscope when used
with trabeculostomy described in 05XXT
• Addition of an exclusionary parenthetical note following 06XXT
⚫0621T Trabeculostomy ab interno by laser;
⚫0622T with use of ophthalmic endoscope
► (Do not report 05XXT, 06XXT in conjunction with 92020)◄
22Ophthalmic US Anterior Segment (76513)
• 76513 was revised to reflect unilateral or bilateral service
76510 Ophthalmic ultrasound, diagnostic; B-scan and quantitative A-
scan performed during the same patient encounter
▲76513 anterior segment ultrasound, immersion (water bath) B-
scan or high resolution biomicroscopy, unilateral or
bilateral
(For scanning computerized ophthalmic diagnostic imaging of the
anterior and posterior segments using technology other than
ultrasound, see 92132, 92133, 92134)
23Remote retinal imaging (92227, 92228, 92229)
• 92227 was revised to become a parent to 92228
• 92227 and 92228 were revised to include imaging of retina for detection or
monitoring
• 92227 was revised to specify use by remote clinical staff and 92228 to specify
use by remote physicians/QHP
• 92229 (9225x in proposed rule) was added for retinal imaging with automated
point-of-care
24Remote retinal imaging (continued)
▲ 92227 Imaging of retina for detection or monitoring of disease; with remote
clinical staff review and report, unilateral or bilateral)
►(Do not report 92227 in conjunction with 92133, 92134, 92228, 92229, 92250)◄
▲ 92228 with remote physician or qualified health professional review and
report, unilateral or bilateral
►(Do not report 92228 in conjunction with 92133, 92134, 92227, 92229, 92250)◄
#⚫ 92229 point-of-care automated analysis and report, unilateral or
bilateral
►(Do not report 92229 in conjunction with 92133, 92134, 92227, 92228, 92250)◄
25Revalued Codes
26Ophthalmic US Anterior Segment (76513)
Revaluation
• 76513 was revalued due to high volume growth attributed to improved
equipment
• The RUC agreed with AAO’s recommendation of 0.60 RVU
• CMS in their proposed rule proposed a work RVU of 0.53 based on a
crosswalk to CPT code 74230 with identical intra-service and total times
• AAO was successful in advocating for the RUC-recommended value of 0.60
in the final rule
27Remote retinal imaging (92227-9) revaluation
• The RUC disagreed with AAO’s original recommendation of maintaining the
2020 work RVU of 0.37 for 92228 and approved a work RVU of 0.32
• CMS accepted the RUC-recommended value of 0.32 for 92228
• There are two practice sites for 92227 and 92228: the acquiring site (e.g. a
PCP practice) and the reading site (e.g. an ophthalmology practice)
• For both 92227 and 92228, direct PE pays for the clinical staff at both sites
and CMS accepted the RUC-recommended direct PE inputs for these codes
• 92227 and 92229 are PE only codes
28Imaging of retina using AI (92229)
• CPT 92229 Imaging of retina for detection or monitoring of
disease; with point-of-care automated analysis with
diagnostic report; unilateral or bilateral
• Can be used at a primary care practice site and the
artificial intelligence technology interprets the test instead
of a remotely located ophthalmologist
• CMS acknowledges AI applications are not well
accounted for in their PE methodology, but still eliminated
the $25.00 RUC-recommended analysis fee
• CMS finalized payment based on contractor pricing,
where each individual MAC sets their own pricing for each
locality
o The Academy will work with the MACs to advocate for the RUC-
recommended values, just as we did for ECP codes in 2020
29Intravitreal Injection (67028) Revaluation
• 67028 was identified by the RUC’s Relativity
Assessment Workgroup (RAW) as a code
where the original valuation was based on a
crosswalk code that had since been revalued
• CMS accepted the RUC-recommended work
value of 1.44, but refined the direct PE inputs
o CA024 “Clean room/equipment by clinical
staff” (CA024) was reduced from the RUC-
recommended 5 minutes to 3 minutes
o Equipment times were refined to match the
change in clinical labor time
30Work RVU Comparison
CPT Code Current 2020 Work RUC Rec. Work Final 2021 CMS
RVU RVU RVU
67028 1.44 1.44 1.44
76513 0.66 0.60 0.60
92227 0.00 0.00 (PE only) 0.00
92228 0.37 0.32 0.32
92229 NEW 0.00 (PE only) 0.00 Carrier priced
31Revaluation in Dollars
CPT Code 2020 Pay 2021 Pay Change in % Change in
Pay 2020- Pay 2020-
2021 2021
67028 (office) $ 103.22 $ 106.95 $ 3.73 3.62%
67028 (facility) $ 100.69 $ 85.23 -$15.46 -15.35%
76513 $ 101.41 $ 74.54 -$26.87 -26.50%
92227 $ 13.71 $ 15.56 $ 1.84 13.43%
92228 $ 34.65 $ 28.84 -$ 5.80 -16.75%
These are predicted averages for Medicare FFS across the US, actual values will vary slightly.
32New Codes
33Remote Retinal Optical Coherence
Tomography (0604T-0606T)
0604T Optical coherence tomography (OCT) of retina, remote,
patient-initiated image capture and transmission to a remote
surveillance center, unilateral or bilateral; initial device
provision, set-up and patient education on use of equipment
0605T remote surveillance center technical support, data
analyses and reports, with a minimum of 8 daily
recordings, each 30 days
34Remote Retinal Optical Coherence
Tomography (0604T-0606T)
0606T review, interpretation and report by the prescribing
physician or other qualified health care professional of
remote surveillance center data analyses, each 30 days
►(Do not report 0604T, 0605T, 0606T in conjunction with 99457,
99458)◄
35Iris Prosthesis Procedures (0616T-0618T)
0616T Insertion of iris prosthesis, including suture fixation and repair
or removal of iris, when performed; without removal of
crystalline lens or intraocular lens, without insertion of
intraocular lens
0617T with removal of crystalline lens and insertion of
intraocular lens
►(Do not report 0617T in conjunction with 66982, 66983,
66984)◄
36Iris Prosthesis Procedures (0616T-0618T)
0618T with secondary intraocular lens placement or
intraocular lens exchange
►(Do not report 0618T in conjunction with 66985, 66986)◄
►(Do not report 0616T, 0617T, 0618T in conjunction with
66600, 66680, 66682)◄
37G-codes: G2211 and G2212
G2211
• Visit complexity inherent to evaluation and management associated with medical care services
• (Add-on code, list separately in addition to office/outpatient evaluation and management visit, new or
established)
• Was GPC1X in proposed rule
• CMS is not establishing any policies that prohibit reporting the add-on code by any specialties, so
ophthalmologists can use it
• CMS does not expect G2211 to be used when E/M service is reported with a modifier (explicit
prohibition TBD)
• Can be reported for both new and established patients
G2212
• Describes prolonged office/outpatient E/M visits to be used in place of CPT code 99417
• (List separately in addition to CPT codes 99205, 99215 for office or other outpatient evaluation and
management services)
• Was 99XXX in proposed rule
38PPE supplies during COVID-19 (99072)
• Additional supplies, materials, and clinical staff time over and above those
usually included in an office visit or other non-facility service(s), when
performed during a Public Health Emergency, as defined by law, due to
respiratory-transmitted infectious disease
• Finalized as a bundled service on an interim basis
39Telehealth Provisions
• CMS finalized making certain telemedicine services permanent after the
public health emergency ends with a focus on improving rural telehealth
access
• The Academy requested that any services permanently added to the list of
Medicare covered telehealth services should be paid fairly relative to other
covered services
• Telehealth services covered now under the federally declared PHE, and
those made permanent, will only apply to rural areas after the PHE, barring
congressional action
40The Outpatient Prospective Payment
System (OPPS) and Ambulatory
Surgical Center (ASC) payment rule
CY 2021
41CMS Finalizes ASC Changes for CY 2021
• Takes effect January 1, 2021
• Payments increased by 2.4% for ASCs
• Expanding the list of services requiring prior authorization (PA) when
performed in HOPDs, which already includes blepharoplasty and botulinum
toxin
• The elimination of the inpatient-only list over a three-year transitional period
with the list completely phased out by calendar year 2024.
42CMS Finalizes ASC Changes for CY 2021
• CMS approved the application for device pass-through payment for the
Customflex Artificial Iris starting in 2021.
• CMS is not planning to extend the pass-through status for products due to
the public health emergency.
o Will consider an extension in future rulemaking
43IDxDR – Artificial Intelligence evaluation
of diabetic retinopathy (92229)
• CMS changed the assigned APC for CPT code 92229 to APC 5733 (Level 3
Minor Procedures) rather than APC 5732 (Level 2 Minor Procedures).
• CMS is also finalizing a change to the status indicator, assigning CPT code
92229 to APC 5733 with status indicator “S.” The Academy has urged CMS
to assign the code to a more appropriate APC, this reassignment will ensure
Medicare payment for this innovative service accurately reflects the cost of
providing this technological advance to patients.
44Insertion of drug-eluting implant (0356T)
• CMS did not change the assigned APC or status indicator for CPT code
0356T, insertion of drug-eluting implant (including punctal dilation and implant
removal when performed) into lacrimal canaliculus, each).
o CMS finalized their proposed policy without modification to assign CPT code 0356T to
APC 5692 (Level 2 Drug Administration) with OPPS status indicator “Q1” in the CY 2021
OPPS. Based on those assignments, CMS also finalized an ASC payment indicator for
CPT code 0356T of “N1” under the CY 2021 ASC payment system.
• The drug itself, Dexamethasone ophthalmic insert 0.1 mg (HCPCS code
J1096) is currently on pass-through status (assigned to APC 9308) and does
receive separate payment.
45Omidria and Non-Opioid Pain Management
• CMS will continue to apply separate payment for non-opioid pain
management drugs that function as surgical supplies when furnished in the
ASC setting for CY 2021.
• CMS agreed that Omidria meets this definition and does qualify as a non-
opioid pain management drug that functions as a surgical supply. CMS is
excluding Omidria from bundling under the ASC payment system beginning
Oct. 1, 2020 and in 2021.
46ASC Quality Reporting Changes for CY 2021
• CMS finalized continuing its policy of voluntary reporting for measure ASC-
11: Cataracts — Improvement in Patient’s Visual Function within 90 Days
Following Cataract Surgery.
• CMS finalized continuing the delay of implementation for measure ASC-15a-
e Consumer Assessment of Healthcare Providers and Systems Outpatient
and Ambulatory Surgery (OAS CAHPS) Survey.
• CMS finalized its proposal to give ASCs the opportunity to review and correct
data on measures submitted to CMS via a CMS online tool. The review and
corrections period will run concurrently with the data submission period.
47Medicare Value-Based Payment CY 2021 Update
2021 MIPS Eligibility
• Three Exclusions
1. New Medicare Provider: Enrolled in Medicare for the first-time during Performance
Year
2. Low-Volume Threshold:
▪ Clinician bills Medicare Part B no more than $90,000 OR
▪ Clinician sees 200 or fewer Medicare Part B patients
▪ Clinician provides 200 or fewer covered professional services to Part B patients.
3. APM Participation: Clinician is a qualified participant in an Advanced APM
If none of these exclusions apply, the MD/DO/OD is Eligible to Participate
in MIPS!
49MIPS Is Getting Harder
2020 & 2021 MIPS Proposed Scoring
2022
Threshold 2020 2021
(Proposed)
Threshold to Avoid a Penalty 45 points 60 points 74.01 points
Exceptional Performance
85 points 85 points 85 points
Threshold
50MIPS Proposed Performance Category Weights
MIPS Category Score Score Score Score Score Score
Weight Weight Weight Weight Weight Weight
2017 2018 2019 2020 2021 2022+
(propose
d)
Quality 60% 50% 45% 45% 40% 30%
Promoting Interoperability 25% 25% 25% 25% 25% 25%
(PI)
Improvement Activities (IA) 15% 15% 15% 15% 15% 15%
Cost 0% 10% 15% 15% 20% 30%
51MIPS 2021: What’s in Store?
MIPS APMs MIPS Eligibility
• MIPS APMs can report through • Unchanged
MIPS or a new APM
Performance Pathway (APP) Quality
• The APP includes a fixed set of • CMS Web Interface collection
measures for each performance type extended until 2022
category
52MIPS 2021: What’s in Store?
Cost Small Practices
• Scoring weight change by 5% • PI Hardship Maintained
Promoting Interoperability • 6-Point Small Practice Bonus in
Quality Category Maintained
• Minor scoring changes for 2021
• Double Credit for Each IA
Improvement Activities Maintained
• Unchanged
53MIPS and the IRIS® Registry
Benefits of IRIS® Registry participation include:
▪ Helps meet quality reporting requirements;
▪ Provides at least one outcome or high priority measure for most participants to report;
▪ Supports credit for improvement activities;
▪ Facilitates promoting interoperability reporting and counts towards the clinical data registry
reporting measure for integrated practices.
Bonus quality points via IRIS Registry participation
▪ For reporting multiple outcomes measures
▪ For electronic reporting through IRIS Registry-integrated EHR
54MIPS Extreme Circumstances Hardship
• Physicians who experience an extreme and uncontrollable
circumstance that is outside of their control can apply for an
extreme and uncontrollable circumstances hardship exception for
each individual category of the Merit-Based Incentive Payment
System
• Extreme and uncontrollable circumstances hardship exceptions
require you to apply for a hardship exception by Feb. 1, 2021 at 8
p.m. ET.
o CMS has not yet declared and automatic extreme and uncontrollable
circumstance exceptions
55Upcoming Practice Management Webinars
• Go to aao.org/meetings.
• Click on “Practice Management.”
• Register for these live Zoom webinars:
o Dec. 15: Reporting MIPS for 2021 (Free member benefit)
o Jan. 12: 2021 Coding Update
56Most Favored Nations Interim Final
Rule
57Most Favored Nations (MFN) Overview
• The rule creates a new, mandatory, 7-year drug price payment demonstration
that changes how CMS pays providers for a set of 50 drugs reimbursed
under Medicare Part B, including three anti-VEGF drugs
• During the mandatory drug-price demonstration, which starts Jan. 1, CMS
will switch to a payment model based on the lowest international price
• Instead of reimbursing for the average sales price plus 6 percent, CMS will
pay providers the lowest price plus a flat fee that will be adjusted quarterly for
inflation
58Demonstration Key Details
• Effective date: Jan. 1, 2021, to Dec. 30, 2027
• New calculation: Lowest international price plus flat fee
o Countries used in calculation: Members of the Organisation for Economic Co-
operation and Development that have at least 60 percent of the U.S. gross domestic
product per capita (GDP)
o Flat fee: $148.73 for the first quarter of 2021
• Participation:
o Mandatory
• Drugs affected:
o Top 50 most costly drugs reimbursed by Medicare
o Ophthalmology drugs affected: Eylea and Lucentis
o Exceptions: Include compounded drugs, which should exclude Avastin for
ophthalmic use
59Academy Response to MFN
• Press release
• Coalition sign-on letter
• Letter to HHS
• Grassroots
• Additional physician group
sign-on letters
• Public Comment
60Academy Member Resources
Visit:
o www.aao.org/medicare to find member resources
o www.aao.org/eye-on-advocacy-article/health-policy for 2021 Reimbursement
Articles, News, and Summaries
Email:
• Health Policy: HealthPolicy@aao.org
• MIPS Help: mips@aao.org
• IRIS Registry Help: irisregistry@aao.org
61Questions?
62You can also read