Medication for Anxiety and Depression - PJ Cowen Department of Psychiatry, University of Oxford
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Medication for Anxiety and
Depression
PJ Cowen
Department of Psychiatry, University
of Oxford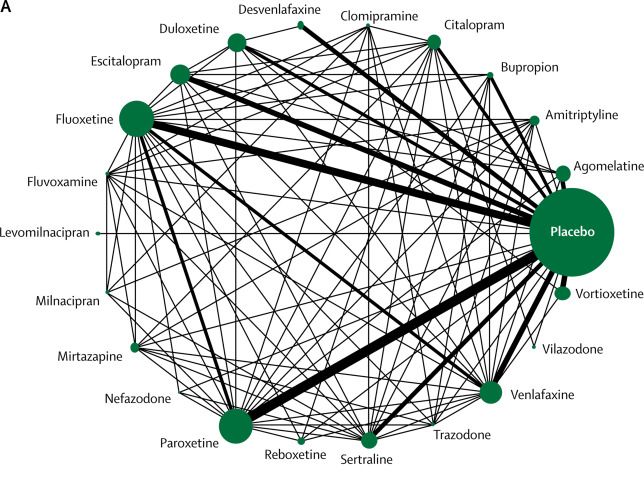
Topics • Medication for anxiety disorders • Medication for first line depression treatment • Medication for resistant depression • Recent studies with ketamine

Clinical Approach to Diagnosis
Baldwin et al, 2014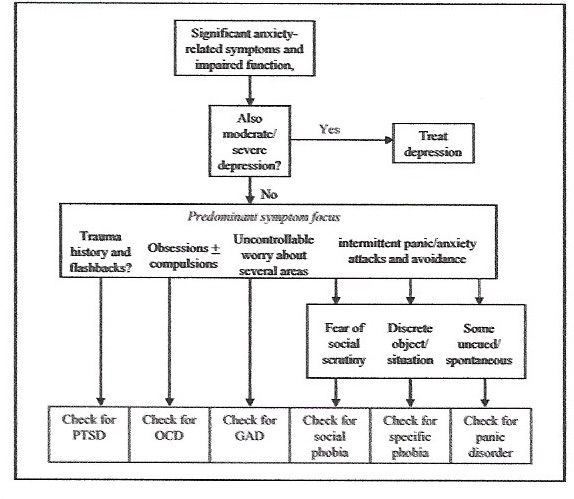
EU Community Studies of Anxiety
Disorders
Diagnosis 12 month Pharmacological
prevalence (%) Treatment
Specific phobia 6.4 N/A
PTSD 2.9 SSRI
Panic (± 1.8 SSRI
agoraphobia)
Agoraphobia (- 2.0 SSRI
panic)
Social Phobia 2.3 SSRI
GAD 2.5 SSRI
OCD 0.7 SSRI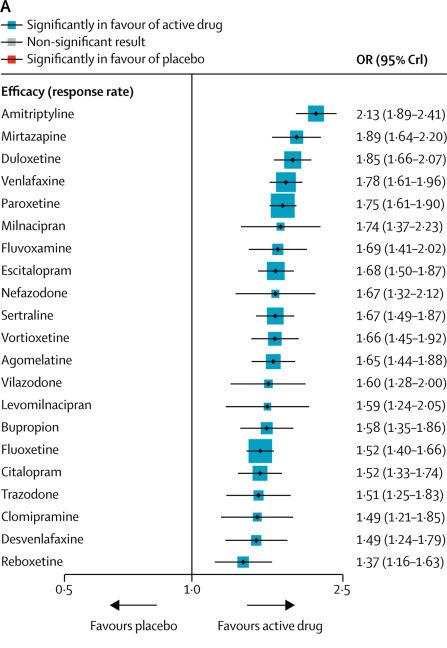
SSRIs and SNRIs in Anxiety
Disorders
SSRI Licensed Indications (additional to major
depression)
Paroxetine GAD, Panic, SAD, OCD, PTSD
Fluoxetine OCD
Sertraline Panic, SAD, OCD, PTSD
Citalopram Panic
Escitalopram GAD, Panic, SAD, OCD
Venlafaxine GAD, Panic, SAD
Duloxetine GAD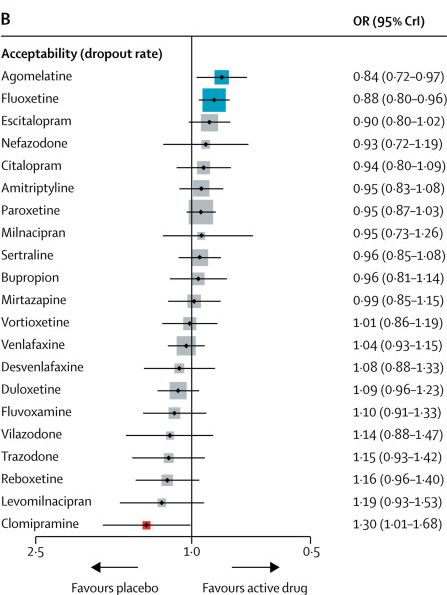
Pregabalin in GAD • Mode of action uncertain. Probably via blockade of a subunit of calcium channels • Side effects profile different to SSRI. Somnolence dizziness, increased appetite. Loss of visual acuity reported rarely. Withdrawal symptoms can occur (insomnia, anxiety) • Daily dose 150-600mg (2 or 3 x daily). No clear dose response • Misuse potential • Can be combined with antidepressants
NICE Guidelines for Anxiety • Stepped Care Approach • Psychological treatments preferred • Generally recommend SSRIs if drug therapy needed. SNRI second line. Pregabalin third line (GAD). • Benzodiazepines- maximum 2-4 weeks • Continuation treatment generally indicated
Depression-threshold for
prescribing (NICE)
• Antidepressants not recommended for mild
depression (PHQ 9 < 15)- unless chronic symptoms or
previous history of more severe depression
• PHQ9 15-19 Antidepressants or psychotherapy
• PHQ9 > 19 Antidepressants and psychotherapy
• ‘Normally choose an SSRI in generic form’ (but not, if
patient taking: triptans, NSAIDs, warfarin, heparin,
aspirin)- Consider mirtazapine or use SSRI with
gastroprotective medicine (except triptan).Network Meta-Analysis of Antidepressant
Efficacy in Major Depression
Cipriani et al, 2018Efficacy and Tolerability of Antidepressants
in Major Depression
Cipriani et al, 2018Early Pharmacological Approaches to
TRD (NICE)
1. Consider raising dose (allows time for natural
recovery to start and to carry out further
assessments)
2. Switch (initially another SSRI, or a better tolerated
new generation antidepressant)
3. An antidepressant of a different pharmacological
class that may be less well tolerated (eg a TCA (but
not dosulepin),venlafaxine, or an MAOI)Different Class vs SSRIs Switch in SSRI-
Resistant patients
Papakostos et al 2007Further Management (NICE
Guidelines)
1. Antidepressant combination (eg mirtazapine with
SSRI or SNRI; in US bupropion plus SSRI popular)
2. Lithium augmentation
3. Atypical antipsychotic augmentationMirtazapine Addition to Ineffective
SSRI/SNRI Treatment
• 480 depressed patients on SSRI/SNRI at least
six weeks
• Randomised to mirtazapine addition (up to
30mg) or placebo.
• Primary outcome BDI at 12 weeks
• Adjusted difference in scores -1.83 (-3.92-
0.27; p= 0.087)
• Conclusion- No convincing evidence of clinical
benefitMeta-analysis of atypical antipsychotic
augmentation of SSRI treatment
Agent and study Treatment, Control, Odds ratio (fixed) Odds ratio (fixed)
n n (95% CI) (95% CI)
Olanzapine studies
Shelton et al 6 / 10 2 / 10 6.00 (0.81, 44.35)
Shelton et al 25 / 146 18 / 142 1.42 (0.74, 2.74)
Corya et al 69 / 230 10 / 56 1.97 (0.94, 4.13)
Thase et al I 24 / 102 18 / 104 1.47 (0.74, 2.91)
Thase et al II 30 / 98 16 / 102 2.37 (1.20, 4.70)
Subtotal 586 414 1.83 (1.30, 2.56)
Risperidone studies
Mahmoud et al 26 / 137 12 / 131 2.32 (1.12, 4.83)
Keitner et al 32 / 62 8 / 33 3.33 (1.30, 8.53)
Reeves et al 4 / 12 2 / 11 2.25 (0.32, 15.76)
Subtotal 211 175 2.63 (1.51, 4.57)
Quetiapine studies
Khullar et al 3/8 0/7 9.55 (0.40, 225.19)
Mattingly et al 11 / 24 2 / 13 4.65 (0.84, 25.66)
McIntyre et al 9 / 29 5 / 29 2.16 (0.62, 7.49)
Earley et al 110 / 327 38 / 160 1.63 (1.06, 2.50)
El-Khalili et al 112 / 289 35 / 143 1.95 (1.25, 3.06)
Subtotal 677 352 1.89 (1.41, 2.54)
Aripiprazole studies
Berman et al 47 / 181 27 / 172 1.88 (1.11, 3.19)
Berman et al 64 / 174 32 / 169 2.49 (1.52, 4.08)
Marcus et al 47 / 185 28 / 184 1.90 (1.13, 3.19)
Subtotal 540 525 2.09 (1.55, 2.81)
Total 2014 1466 2.00 (1.69, 2.37)
0.1 0.2 0.5 1 2 5 10
Favours control Favours treatment
SSRI, selective serotonin reuptake inhibitor;
CI, confidence interval Nelson JC, Papakostas GI. Am J Psychiatry 2009;166:980-91Meta-Analysis of Atypical Antipsychotic
augmentation of SSRI Treatment (ii)
• Response rate 44.2% vs 29.9%
• Remission rate 30.7% vs 17.2%
• For Response NNT= 9
• For Remission NNT= 9
• Discontinuation (adverse effects) NNH= 17
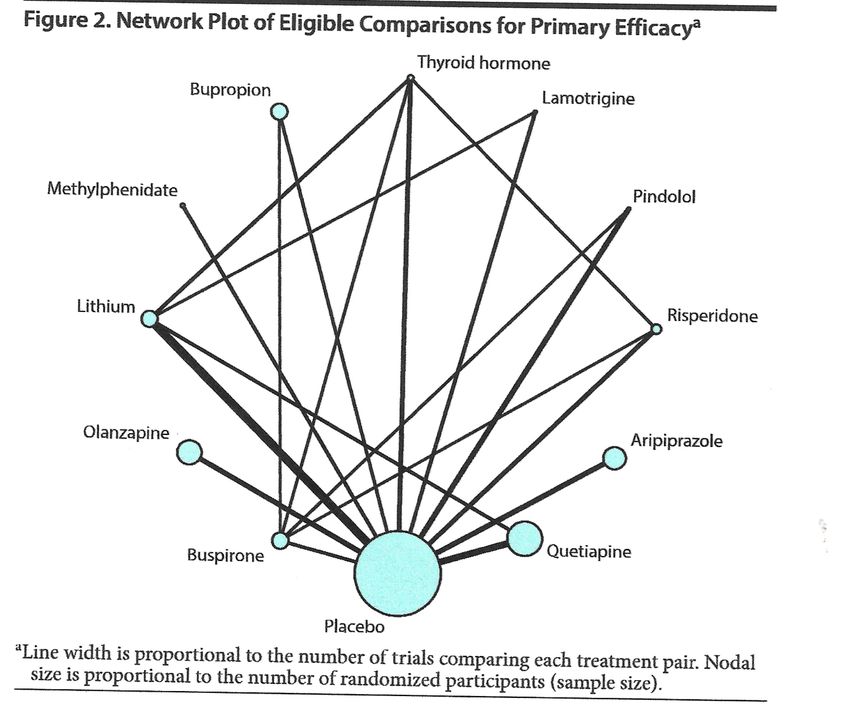
(Papakostas and Nelson, 2009)Network Meta-analysis of Augmentation
Treatments for Resistant Depression (n= 6,700)
*
*
*
*
Zhou et al,
2015LQD Study • Funded by NIHR • Multi-centre-pragmatic study of lithium versus quetiapine as add-on therapy in patients with TRD (persisting depression despite having tried two or more antidepressants in current episode). • 276 patients randomised openly to 12 months treatment • Referral: Oxfordhealth.trdclinic@nhs.net
Ketamine as an Antidepressant • Ketamine is an antagonist at glutamate NMDA receptors • Used as general anaesthetic • At sub-anaesthetic doses, intravenous ketamine can provide some temporary relief from depression in resistant depression (bipolar and unipolar)
Ketamine produces a rapid alleviation of depression in TRD
Zarate et al 2006Meta-analysis of Ketamine
Remission in TRD
McGirr et al, 2015Subsequent Experience with Ketamine • Transient antidepressant effect (1-7 days) confirmed in numerous controlled studies (NNT for response 3-5). • Response not generally maintained with available glutamatergic agents (memantine, riluzole). • Other NMDA and glutamate receptor antagonists developed by Industry not consistently effective in trials • Intranasal s-ketamine may be effective and more useful for longer-term maintenance. • Worries about longer-term adverse effects remain
Conclusions • For anxiety, psychological treatment preferred. SSRIs first line if drug treatment needed. • SSRIs continue to be first line medication for the treatment of depression. Escitalopram (now generic) offers the best balance of acceptability and risk. Mirtazapine is non-SSRI alternative. • Switching within or between class is a reasonable option if a patient with depression is insufficiently helped by an initial SSRI • Augmentation with low dose atypical antipsychotic drugs is probably effective but the adverse effect burden is troublesome. Utility vs lithium needs exploring • Ketamine might provide symptomatic relief for patients who have persistent depressive symptoms despite multiple trials of psychological and pharmacological treatment
You can also read