Meeting of the General Assembly - October 2nd, 2021, 9:00 am ASMA conference room / Zoom 4107 Laurel Street Anchorage, 99508 - Alaska State ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Meeting of the General Assembly
October 2nd, 2021, 9:00 am
ASMA conference room / Zoom
4107 Laurel Street
Anchorage, 99508
Meeting Book - ASMA General Assembly Meeting October 2, 2021
Agenda
Board of Trustees
President's Statement
Speaker's Statement
Approval of Minutes May meeting
Budget
Website Update
Cassie Jeanes
FAMLI Leadership Training Program
Pam Ventgen
Legislative Report
Kevin Jardell
Attorney's Report
Roger Holmes
Committee Reports
Drs. Powell, Foland, Merkouris
WWAMI Update
Barb Doty, M.D.
10:00 am POLST - Physician Orders for Life Sustaining Treatment
Ursula McVeigh, M.D.
10:30 am COVID-19 and Health in Alaska
Anne Zink, M.D.
Next meeting and adjourn
A laska State Medical Association
414107 Laurel Street Anchorage, Alaska 99508 (907) 562-0304
ASMA Board of Trustees 2021-2022
President Janice Sheufelt, M.D.
Past President Steve Sivils, D.O.
President Elect Jessica Panko, M.D.
Speaker Mary Ann Foland, M.D.
AMA Delegate Alex Malter, M.D.
AMA Alternate Delegate Rhene Merkouris, M.D.
Trustee 1st District Joe Roth, M.D.
Trustee 2nd & 4th Districts Clay Triplehorn, M.D.
Trustee 3rd District Sarah Roberts, M.D.
Secretary/Treasurer Steve Compton, M.D.
Secretary/Treasurer Elect Kristin Mitchell, M.D.
PA Representative Christi Froiland, PA-C
ALPAC/Legislative Committee Chair Eli Powell, M.D.
Physician Health Committee Chair Mary Ann Foland, M.D.
Public Health Committee Chair Rhene Merkouris, M.D.
Roger Holmes, Esq Attorney
Kevin Jardell Lobbyist
Pam Ventgen Executive Director
Cassie Jeanes Office Manager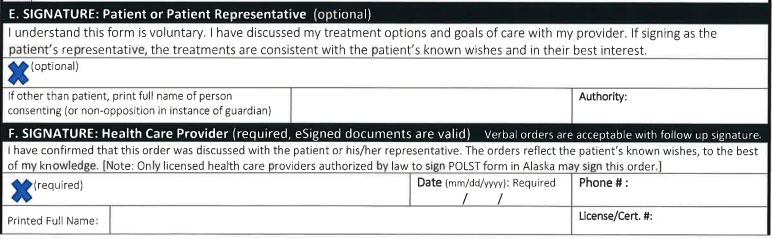
Alaska State Medical Association
House of Delegates/General Assembly Meeting
May 8th, 2021 – Zoom Meeting
Minutes
1. The meeting was called to order at 9:02 am by Speaker Rathkopf.
2. Introduction of Delegates. The following delegates were present: Drs. Demain, Grimberg, Benjamin,
Miknich, Young, Panko, Merkouris, Buchholz, and Bonar.
Board of Trustees present: Drs. Sivils, Powell, Mitchell, Foland, Roth, Malter, Rathkopf, Sheufelt, and
Compton. Members present: Drs. Roberts, Klix, Nelson, Finley, Al Gross, Monica Gross, Helen Adams, Doty,
Marks, O’Malley, Kerstin Miller, Arom Evans, Tim Olsen, DeKeyser, Manion, Colescott, Stoltz.
PAs present: Froiland, Hall.
Guests: Dr. Zink, Dr. Buckley, Terri Folk (AMA).
Staff: Jeanes, Ventgen, Holmes, Jardell.
3. President’s Statement & Membership update: Dr. Sivils expressed his appreciation to the members and staff
for work done this year. Membership is up a bit from last year. It has been a challenging year for all and he
was grateful for the opportunity to serve.
4. Speaker of the House Statement: Dr. Rathkopf has served on the board for 10 years and thanked Drs. Foland
and Malter in particular for their mentorship.
5. Upon a motion by Foland, seconded by Malter, the minutes of the October 3rd, 2020 HOD were approved.
6. Election of Officers: Dr. Rathkopf presented the following proposed slate of officers.
a. President: Janice Sheufelt MD
b. President-Elect: Jessica Panko MD
c. Speaker: Mary Ann Foland MD
d. AMA Delegate: Alex Malter MD
e. AMA Alternate Delegate: Rhene Merkouris MD
f. Trustee 1st District: Joe Roth MD
g. Trustee 2nd & 4th District: Clay Triplehorn MD
h. Trustee 3rd District: Sarah Roberts MD
i. Secretary/Treasurer: Steve Compton MD
j. Secretary/Treasurer Elect: Kristin Mitchell MD
Upon a motion by Demain, seconded by Merkouris, the slate of officers was unanimously approved.
7. Bylaws Revisions were introduced and briefly explained by Roger Holmes. The previous Bylaws went back
about 40 years and were outdated. Many House of Delegates positions were vacant. The committees listed
in the Bylaws were nonfunctioning and the functioning committees were not listed. There was some
discussion of having committee chairs have a seat on the Board of Trustees. Upon a motion by Demain,
seconded by Powell, an amendment was suggested that committee chairs be appointed by the president and
approved by the membership. After approval the committee chair would have a voting seat on the Board of
Trustees. This amendment passed. Then upon a motion by Mitchell, seconded by Demain, the Bylaws were
unanimously adopted.
8. Legislative Update was given by Kevin Jardell. He began by stating that 328 bills had been introduced this
year, 5 have passed the legislative process. Mr. Jardell then briefly reviewed the bills of most interest to
ASMA and their current status. He will continue to follow these issues for ASMA.
9. State of the State’s Health (10:00 am). Dr. Anne Zink joined the meeting and gave a brief update on health
matters in the state. A lively discussion followed about various matters. It was agreed that the COVID hotline
would be transitioned to other state resources and Dr. Zink thanked the physicians who had staffed the
hotline.
10. AMA Representative Comments (10:30 am). Following a brief break Dr. Brooke Buckley spoke about the
services and training provided by the AMA’s political action committee. It is a nonpartisan committee that
offers training to physicians and their spouses interested in running for office and supports physician
members of congress.
11. Interstate Medical Licensure Compact was reviewed by Ms. Ventgen. It is one option to cut down on delays
in the current medical licensing process though the compact has some weaknesses. Several members
expressed concern about keeping Alaska’s licensing standards high. Upon a motion by Malter, seconded by
Sheufelt, it was agreed that ASMA will continue to work on improving licensing methods and provide an
update at the October General Assembly meeting.
12. ARP DRG system was going into effect July 1, 2021. Dr. Benjamin explained what the ARP DRG system was
and that the implementation date has been postponed.
13. Committee Reports:
a. AMA – Dr. Malter gave a brief review of the AMA’s virtual meeting.
b. PHC – Dr. Foland stated that the PHC had a handful of graduates, still a lot of participants with a
few more in the wings.
c. Legislative/ALPAC – Dr. Powell explained the workings of the committee and that it was
nonpartisan and built relationships with legislators who supported issues of interest to ASMA.
d. Public Health – Dr. Merkouris agreed to chair this new committee and work with the Department
of Health and Social Services on matters of statewide interest.
14. FAMLI Leadership program – Ms. Ventgen explained that we had grant funding to run the program one more
year and that applications will be solicited in the fall.
15. New Business – There was no new business introduced.
16. Set next meeting date: October 2nd, 2021
17. Upon a motion by Malter, seconded by Sivils, the meeting adjourned at 11:55 am.2021 Current
2020 Actual 2022 Budget
YTD
INCOME Total Total Total
Dues $215,660.00 $188,280.00 $190,000.00
Advertising $44,405.00 $5,575.00 $5,000.00
Sales $13,724.00 $2,461.00 $1,000.00
PHC $62,515.00 $40,684.00 $45,000.00
Perdiem (MIEC) $11,200.00 $0.00
MIEC $33,766.00 $27,459.00 $59,000.00
WWAMI $3,920.00 $3,600.00 $3,500.00
Rental Income $0.00 $0.00 $0.00
Interest $112.57 $33.02 $30.00
FBKS Donation $9,300.00 $0.00
KP Donation $6,212.00 $0.00
Grants $115,000.00 $0.00
postage $900.00
Total Income: $516,714.57 $268,092.02 $303,530.00
EXPENSES
Payroll/Health Insurance$292,536.00 $115,000.00 $210,000.00
Employee Fringe $14,400.00 $11,901.00 $12,000.00
Accounting $7,307.00 $3,875.00 $3,000.00
Website $20,022.00 $14,755.00 $5,000.00
Computer/IT $8,117.00 $11,444.00 $13,000.00
Lobbyist $40,000.00 $40,000.00 $40,000.00
Legal $11,000.00 $13,000.00 $12,000.00
Phone/internet $7,650.00 $2,754.00 $4,000.00
Utilities $6,400.00 $3,331.00 $6,000.00
Admin $8,807.00 $276.00 $500.00
Property Maintenance $12,767.00 $5,996.00 $12,000.00
Office Supplies $2,976.00 $2,276.00 $2,000.00
Minor Equip $952.00 $1,819.00 $1,550.00
Real Estate Tax #REF! $8,000.00
Fed Inc Tax #REF! $5,472.00 $3,000.00
Insurance $2,783.00 $1,739.00 $1,800.00
Publications $18,600.00 $3,845.00 $7,000.00
PHC #REF! $1,146.00 $2,000.00
Postage $4,111.00 $523.00 $1,000.00
Bank Charges & CC Fees $8,101.00 $3,561.00 $3,000.00
NET Travel #REF! $23.00 $0.00
Affiliate Programs $600.00 $790.00 $1,500.00
Member Mailings $4,875.00 $2,411.00 $1,200.00
Total Expense #REF! $245,937.00 $349,550.00
-$516,714.00 $268,092.00 -$303,530.00
$11,892.00 $26,565.00 $46,020.00What is the Future Alaska Medical
Leaders Program?
Alaska State
Today's dynamic health care system
requires a set of leadership skills
which are not typically taught medical
Medical Association
school. This program unpacks the
nuances of leading with emotional
intelligence, managing change,
building critical thinking skills, and
resiliency in an effort to create
2022
efficacious leaders.
2022 Program Dates:
The Future Alaska
January 7, 14 & 21 2022
February 4, 11 & 25, 2022
March 4, 18, 2022
Medical
April 1, 8, & 29, 2022
May 6, 2022 Leaders
Program
What can I expect to learn in this
program?
The program will expand your sphere
Interested in participating
of meaningful influence to include
or have questions? IN PARTNERSHIP WITH
patients, organizational leaders, and
other healthcare professionals.
Participants will be able to apply their Contact Pam at the Alaska The Physician
learning to patient advocacy/care, State Medical Association:
organizational outcomes, and Foundation
community relations.
pventgen@asmadocs.org
Physician leadership manifests in
many different ways. From direct (907) 244-7266
patient interactions to community
engagement, a physician needs to
have the skills to advocate for, impact,
and advance care.Core Modules
Leading with Emotional Intelligence & Relationship
Management
Effective Transition & Change Management
Who is FutureSYNC International?
While FutureSYNC Intl. works with Team Engagement Strategies & Five Behaviors of a
organizations of all types, over 80% of
our business is within the house of Cohesive Team
medicine. We have a keen
understanding of the challenges facing
today’s medical professionals.
The Accountability Balance Beam: Personal
Accountability & Holding People Accountable
In 2013 FutureSYNC Intl. partnered with
the Montana Medical Association to
create their first Physician Leadership Advanced Critical Thinking Skills: The Leadership
Effectiveness Program. With the goal
of engaging and uniting participants,
Perspective
the program enhances the leadership
skills for physicians by preparing them Thinking Strategically
to fill emerging leadership roles and
influence healthcare policy. 175
physicians have walked away from our The Influence of Outcomes
programs with practical and action-
oriented leadership skills to become
catalysts for effective change in their Building Resiliency & Managing Burnout
organizations and communities.
Conversations of ConsequenceAlaska State Medical Association
Future Alaska Medical Leaders, Inc
(FAMLI)
Leadership Program Application
The Future Alaska Medical Leaders Inc (FAMLI) program is a leadership development program that
takes place over five months. Designed to build and enhance leadership skills of physicians, this
program prepares participants to gain skills in emerging leadership roles and influencing healthcare
policy.
Applicant Information
Full Name:
Date:
Last First M.I.
Mailing
Address:
Street Address Apartment/Unit #
City State ZIP Code
Cell Phone: Personal
Email
Work phone:
What is your medical
specialty?
Are you a member of the Alaska State YES NO
Medical Association?
Specialty Society? YES NO If yes, please
list
How did you learn about this program?
1Check one of the following categories which best Private practice physician
describes your current employment situation.
Group practice
Tribal/Military
Employed by hospital/clinic/organization
Name of employing organization:
References
Please list three professional references.
Full Name: Relationship:
Company: Phone:
Address:
Full Name: Relationship:
Company: Phone:
Address:
Full Name: Relationship:
Company: Phone:
Address:
Activities and Perspectives
Please list up to four hospital, specialty, and/or ASMA activities (e.g., committee member, component society member),
or leadership positions (e.g., committee chair, AMA delegate, officer) in which you currently participate or have
previously participated.
Please list up to four other organizations of which you are or have been a member (e.g., Chamber of Commerce, Rotary
Club, etc.).
Please state briefly any contributions, achievements, or recognitions which you consider significant, including how you
exhibited a leadership role.
We are interested in your personal reflection on leadership. There is no right or wrong answer.
What is leadership:
2Please tell us what specific skills/knowledge you hope to gain from your Physician Leadership program experience; and
in return what contribution/gifts/talents you feel you could bring to the program.
Statewide Perspective
One of the goals of the FAMLI program is to build a substantial network of physician leaders who can
enhance their problem-solving and other leadership abilities through shared perspectives and
working together.
Describe the most notable opportunity facing healthcare in Alaska today:
Please describe the most significant threat facing healthcare in Alaska today.
Signature
I certify that my answers are true and complete to the best of my knowledge.
Please attach a copy of your current CV.
Signature: Date:
APPLICATIONS MUST BE RECEIVED NO LATER THAN November 1, 2021.
Participants are selected by the FAMLI leadership program application committee based on the merits of
the information provided on this application. The Committee seeks representation from a cross-section
of the community including rural, urban, business, non-profit, government, gender, and ethnic and
minority groups. Information on this application is used to add diversity and balance to the class. It is
not available for any other purpose.
CONFIRMATION WILL BE SENT BY EMAIL UPON RECEIPT OF APPLICATION
Successful applicants will be notified by November 15, 2021.
3Medical Record #:
Alaska POLST (Physician Orders for Life Sustaining Treatment) Form
Health care providers should complete this form only after a conversation with their patient or the patient’s representative.
The POLST decision-making process is for patients who are at risk for a life-threatening clinical event because they have a
serious life-limiting medical condition, which may include advanced frailty.
Patient Information. Having a POLST form is always voluntary.
Patient First Name: ___________________________________________________________
This is a medical order, Middle Name/Initial: _______________________ Preferred name: ______________________
not an Advance Directive. Last Name: ________________________________________ Suffix (Jr, Sr, etc): ______________
DOB (mm/dd/yyyy): ______/_______/_________ State where form was completed:___________________
Gender: M F X Social Security Number’s last 4 digits (optional): xxx-xx-___ ___ ___ ___
A. Cardiopulmonary Resuscitation Orders. Follow these orders if patient has no pulse and is not breathing.
YES CPR: Attempt Resuscitation, including mechanical ventilation, NO CPR: Do Not Attempt Resuscitation.
Pick 1
defibrillation and cardioversion. (Requires choosing Full Treatments (May choose any option in Section B)
in Section B)
B. Initial Treatment Orders. Follow these orders if patient has a pulse and/or is breathing.
Reassess and discuss interventions with patient or patient representative regularly to ensure treatments are meeting patient’s care goals.
Consider a time-trial of interventions based on goals and specific outcomes.
Full Treatments (required if choose CPR in Section A). Goal: Attempt to sustain life by all medically effective means. Provide
appropriate medical and surgical treatments as indicated to attempt to prolong life, including intensive care.
Selective Treatments. Goal: Attempt to restore function while avoiding intensive care and resuscitation efforts (ventilator,
defibrillation and cardioversion). May use non-invasive positive airway pressure, antibiotics and IV fluids as indicated. Avoid intensive
Pick 1
care. Transfer to hospital if treatment needs cannot be met in current location, unless another treatment preference is documented in
Section C of this form.
Comfort-focused Treatments. Goal: Maximize comfort through symptom management; allow natural death. Use oxygen, suction
and manual treatment of airway obstruction as needed for comfort. Avoid treatments listed in full or select treatments unless consistent
with comfort goal. Transfer to hospital only if comfort cannot be achieved in current setting.
C. Additional Orders or Instructions. These orders are in addition to those above (e.g., blood products, dialysis).
[EMS protocols may limit emergency responder ability to act on orders in this section.]
D. Medically Assisted Nutrition (Offer food by mouth if desired by patient, safe and tolerated)
Pick 1
Provide feeding through new or existing surgically-placed tubes No artificial means of nutrition desired
Trial period for artificial nutrition but no surgically-placed tubes Discussed but no decision made (standard of care provided)
E. SIGNATURE: Patient or Patient Representative (optional)
I understand this form is voluntary. I have discussed my treatment options and goals of care with my provider. If signing as the
patient’s representative, the treatments are consistent with the patient’s known wishes and in their best interest.
(optional)
If other than patient, print full name of person Authority:
consenting (or non-opposition in instance of guardian)
F. SIGNATURE: Health Care Provider (required, eSigned documents are valid) Verbal orders are acceptable with follow up signature.
I have confirmed that this order was discussed with the patient or his/her representative. The orders reflect the patient’s known wishes, to the best
of my knowledge. [Note: Only licensed health care providers authorized by law to sign POLST form in Alaska may sign this order.]
(required) Date (mm/dd/yyyy): Required Phone # :
/ /
Printed Full Name: License/Cert. #:
A copied, faxed or electronic version of this form is a legal and valid medical order. This form does not expire. Version 1, June 3, 2020.Alaska POLST Form – Page 2 *****ATTACH TO PAGE 1*******
Patient Full Name:
Form Completion Information (required)
Reviewed patient’s advance directive to confirm Yes; date of the document reviewed:___________________
no conflict with POLST orders: Conflict exists, notified patient (if patient lacks capacity, noted in chart)
(A POLST form does not replace an advance Advance directive not available
directive or living will) No advance directive exists
Check everyone who Patient with decision-making capacity Court Appointed Guardian Parent of Minor
participated in discussion: Legal Surrogate / Health Care Agent Other: ____________________________________
Professional Assisting Health Care Provider w/ Form Completion (if applicable): Date (mm/dd/yyyy): Phone #:
Full Name: / / ( )
This individual is the patient’s: Physician’s Assistant Social Worker Nurse Clergy Other:
Contact Information (optional)
Patient’s Emergency Contact. (Note: Listing a person here does not grant them authority to be a legal representative. Only an
advance directive or state law can grant that authority.)
Full Name: Phone #:
Legal Representative
Day: ( )
Other emergency contact Night: ( )
Primary Care Provider Name: Phone:
( )
Name of Agency:
Patient is enrolled in hospice
Agency Phone: ( )
Form Information & Instructions
Completing a POLST form:
- Provider should document basis for this form in the patient’s medical record notes.
- Patient representative is determined by Alaska Statute, and in accordance with state law, may be able execute or void this POLST
form only if the patient lacks decision-making capacity.
- Only licensed health care providers authorized to sign POLST forms in Alaska (M.D./D.O.) can sign this form.
- Original (if available) is given to patient; provider keeps a copy in medical record.
- Last 4 digits of SSN are optional but can help identify / match a patient to their form.
- If a translated POLST form is used during conversation, attach the translation to the signed English form.
- The most recently completed valid POLST form supersedes all previously completed POLST forms.
Using a POLST form:
- Any incomplete section of POLST creates no presumption about patient’s preferences for treatment. Provide standard of care.
- No defibrillator (including automated external defibrillators) or chest compressions should be used if “No CPR” is chosen.
- For all options, use medication by any appropriate route, positioning, wound care and other measures to relieve pain and suffering.
Reviewing a POLST form: This form does not expire but should be reviewed whenever the patient:
(1) is transferred from one care setting or level to another;
(2) has a substantial change in health status;
(3) changes primary provider; or
(4) changes his/her treatment preferences or goals of care.
Modifying a POLST form: This form cannot be modified. If changes are needed, void form and complete a new POLST form.
Voiding a POLST form:
- If a patient or patient representative (for patients lacking capacity) wants to void the form: destroy paper form and contact patient’s
health care provider to void orders in patient’s medical record (and POLST registry, if applicable).
- For health care providers: destroy patient copy (if possible), note in patient record form is voided and notify registries (if applicable).
This form may be added to a secure electronic registry so health care providers can find it.
For Barcodes / ID Sticker
Copied, faxed or electronic versions of this form are legal and valid. Version 1, 10.2019Alaska POLST
Patient Guide to the POLST Form
POLST forms are medical orders that your provider uses to tell another provider what
treatments you want when you cannot speak for yourself. Since the POLST form is how your
provider tells another provider what you want, the words and phrases on the form use medical
terminology. The POLST form was not created for patients to fill out and complete: your
provider should be the person filling it out after talking with you.
This guide was created to help patients and caregivers learn more about the POLST form.
Table of Contents
The POLST Form: 3 Decisions …………………………………………………………………………………………… 2
Decision 1: Yes CPR or No CPR………………………………………………………………………………. 3
Decision 2: Goals of Care and Medical Treatments………………………………………………… 4
Decision 3: Medically Assisted Nutrition (Tube Feeding)……………………………………….. 5
Other POLST Form Sections………………………………………………………………………………………………. 5
Patient information……………………………………………………………………………………………….. 5
Additional Orders…………………………………………………………………………………………………… 5
Signatures……………………………………………………………………………………………………………... 6
Other Important information…………………………………………………………………………………. 6
For More information……………………………………………………………………………………………………….. 7
1
v. 1The POLST Form: 3 Decisions
In talking with your provider about POLST you will be talking about:
• Your current medical condition (diagnosis);
• What is likely to happen as your condition progresses (prognosis)
• Your goals of care, what you want to do, what you enjoy doing; and
• Treatment options, along with how each option effects what you want to be doing.
The goal or purpose of talking with your provider about these things is to decide:
• Are you okay going to the hospital? Or would you want to stay where you are?
• Are you okay going to the intensive care unit and possibly being on a breathing
machine?
• Are you okay having surgery?
Your answers to these questions give your provider information about how to complete your
POLST form. In Section B, the form lists 3 Goals by 3 options. What fits you best?
• Full Treatments: your treatment goal is to have everything done that is medically
appropriate and possible to attempt to save your life. You would be okay going to the
hospital and being in the intensive care unit on a breathing machine.
• Selective Treatments: Your treatment goal is to treat medical problems that can be
reversed. You would be okay going to the hospital but just to get medicine that would
treat an infection you caught. You would not want surgery, to be in the intensive care
unit or on a breathing machine.
• Comfort-focused Treatments: Your treatment goal is to make you as comfortable as
possible and allow death to happen naturally. You would not want to go to the hospital,
be on a breathing machine or have surgery.
As you talk, you will be working with your provider to make three decisions about what
treatments you want. If you don’t want to , that’s okay: you will receive the “standard of care”
for that section. That means that whatever is usually provided to anyone in a situation like
yours, will be provided to you. During a medical emergency, it means doing everything
medically reasonable and possible to attempt to save your life. This can mean providing
cardiopulmonary resuscitation (CPR) to attempt to bring you back to life, transporting you to
the hospital, and possibly putting you in the intensive care unit (ICU) on a breathing machine.
Your provider will complete the following sections of the POLST form based on your talk.
2
v. 1Decision 1: Yes CPR or No CPR
In a medical emergency, the first thing a provider will do is see if you have a pulse or are
breathing. If you do not have a pulse and are not breathing, the provider wants to know if you
want cardiopulmonary resuscitation or CPR. This first order box on the POLST form I where it
will say “Yes CPR” meaning that you want to have CPR attempted or “No CPR” meaning that
you do not want CPR attempted. Having a POLST form that says “No CPR” is Section A means it
is a do-not-resuscitate, or DNR, order.
• Cardiopulmonary Resuscitation (CPR). CPR can be attempted when you stop breathing
and you no longer have a heartbeat: the form uses the word “attempted” because CPR
does not always work. Getting CPR means someone is pushing hard on your chest to
restart your heart. They may use an electrical shock, called defibrillation. They may use a
breathing tube which is a tube put down your through to help you breathe, called
intubation. If needed, you may be put on a machine called a ventilator that pumps air in
and out of your lungs through a breathing tube.
• Do Not Attempt Resuscitation: This “No CPR” option is also called Do Not Resuscitate
(DNR) or Allow Natural Death. It means you do not want CPR attempted because either
you do not want it or because it won’t help you.
If you do not want to make a decision about CPR, that is okay. In an emergency, the standard of
care will be provided which is almost always attempting CPR.
If you choose “Yes CPR” that means you must choose “Full Treatments” in Section B. This is
because, for emergency providers to attempt CPR, they must be able to put a plastic tube down
your throat (called “intubation”) if needed and only “Full Treatments” allows this option.
Additionally, if CPR is successful, you will need to go to the hospital and probably be in the
intensive care unit (ICU) on a breathing machine. Again, these treatments are only provided
under “Full Treatments” below.
3
v. 1Decision 2: Goals of Care and Medical Treatments
If you have a pulse or are breathing, the next most important question is do you want to go to
the hospital and, if yes, what treatments do you want there. Section B on the POLST form
provides this information. Most of your conversation with your provider is likely about this
section because this is where you talk about what different treatment options mean for you,
given your current medical condition and goals of care. For example, going to the intensive care
unit (ICU) doesn’t mean the same thing to everyone. People have different treatments there,
spend different amounts of time in the ICU and have different results.
• Full Treatments. Your provider must choose this option if you wanted CPR but if this is
still a choice if you chose No CPR. This choice means you want everything medically
appropriate done to help you live. If necessary, you are okay going to the intensive care
unit, having a breathing tube, and being on a ventilator.
• Selective Treatments. This choice is if you are okay going to the hospital, but you do
not want a breathing tube or to be on a ventilator. You are okay with getting antibiotics
and other drugs through an IV/ tube placed in a vein. Usually getting drugs or fluids
through an IV are for a short period of time to help you get through a specific illness. If
you have further instructions you can write that in section C of this form, for example, if
you do or do not want to receive blood products, antibiotics, or dialysis.
• Comfort-Focused Treatments. These treatments are always provided no matter what
you choose in this section. This choice means you want to stay where you are and be
made comfortable. You only want to go to the hospital if you cannot be made
comfortable where you are now.
The language at the top of this part of the form tells the providers treating you that they need
to check in with you or your surrogate (the person making treatment decisions for you if you
cannot speak or communicate) to make sure that the treatments you are being provided still
meet your goals. This may mean that certain treatments are provided for a limited amount of
time to see if they help you improve
4
v. 1Decision 3: Medically Assisted Nutrition
Although it isn’t critical for emergency care, it is very helpful for health care providers to know
your wishes about feeding tubes, called medically assisted nutrition. Some feeding tubes
require a surgery to place them. Please watch the video www.polst.org/form to learn more
about tube feeding options.
Other POLST Form Sections
There are other sections of the POLST form, but most are instructions to help make sure your
provider uses the POLST form properly. Below is information on some of the other sections.
Patient information
This section is important for the following reasons:
1. It reminds everyone that having a POLST form is your choice and that you should not
be forced to have one.
2. It reminds everyone that a POLST form is a medical order. And that it is not an
advance directive. See www.polst.org for more information.
3. It asks for information about you. This is to help make sure it is your POLST form. The
more information a provider has the more confident they are that this is your form and your
wishes.
5
v. 1Additional Orders
Signatures
Though optional, it is recommended that you or your surrogate be asked to sign this form.
When you are signing, you are agreeing that:
• You understand you do not need to have a POLST form. It is your choice to have one.
• You have had a conversation with your provider and talked about what is important to
you given your current medical condition.
If you are the patient’s surrogate, you are signing the form saying that what you talked about
with the patient’s provider, and the decisions you made, were likely what the patient would
have chosen if he/she were able to talk.
To be an active, portable, medical order your POLST must be signed by a physician. If the health
care professional assisting you with the form is not a physician, they will write their name on
the back of the form and make arrangements for a physician to review and sign your form.
Other Important information
Most of the form instructions on the back side of the form are for your provider, but there are
two things it is important for patients to know:
1. If you want to change, or modify, your POLST form you need to make an appointment
with your provider. You cannot change your POLST form yourself. It is a medical order
signed by your provider: just as you cannot change a prescription written by your
provider, you cannot change the POLST form. Instead, your provider must void or cancel
your current POLST form and fill out a new one.
6
v. 12. If you want to void or cancel your POLST form you can. You should write “VOID” in large
letters across it or destroy the document. You also need to tell your provider you have
done this so that they remove it from your medical record. If your provider does not
know you have voided your POLST form, they may see it in your medical record and
think it is still what you want and provide those treatments if you cannot speak for
yourself and need care.
For More information
• Talk with your provider
• Look at our videos on www.polst.org/form
• Review advance care planning, advance directives and POLST form information, starting
at www.akpolst.org
Adapted, with gratitude, from National POLST: Patient Guide to the POLST Form. v. 1
7
v. 1STATE OF ALASKA
DEPARTMENT OF HEALTH
AND SOCIAL SERVICES
Physician Orders for Life
Sustaining Treatment
(POLST) ProgramTable of Contents ALASKA POLST PROGRAM: AN INTRODUCTION 3 REQUIREMENT TO HONOR POLST FORMS 3 WHO SHOULD CONSIDER HAVING A POLST FORM? 3 DETERMINE IF THE PATIENT HAS A CONDITION THAT WARRANTS POLST FORM COMPLETION 3 POLST USE FOR PATIENTS WITH SIGNIFICANT PHYSICAL DISABILITIES, DEVELOPMENTAL DISABILITIES AND/OR SIGNIFICANT MENTAL HEALTH CONDITION WHO ARE NEAR THE END OF LIFE 4 USE OF POLST FOR INDIVIDUALS WITH GUARDIANS 4 ADVANCE DIRECTIVES AND POLST: WORKING TOGETHER IN ADVANCE CARE PLANNING 4 WHO CAN FILL OUT A POLST FORM? 5 WHAT IF THE PATIENT DOES NOT HAVE AN ADVANCE DIRECTIVE? 5 DETERMINING APPROPRIATE SURROGATE/HEALTH CARE DECISION-MAKER FOR THOSE WHO HAVE NOT COMPLETED AN ADVANCE DIRECTIVE 6 COMPLETING THE POLST FORM 7 PATIENT INFORMATION—REQUIRED 7 SECTION A: CARDIOPULMONARY RESUSCITATION ORDERS 7 SECTION B: INITIAL TREATMENT ORDERS 8 FULL TREATMENTS 8 SELECTIVE TREATMENTS 8 COMFORT-FOCUSED TREATMENTS 8 SECTION C: ADDITIONAL ORDERS OR INSTRUCTIONS 8 SECTION D: MEDICALLY ASSISTED NUTRITION 9 SECTION E: SIGNATURE/PATIENT OR PATIENT REPRESENTATIVE (OPTIONAL) 9 SECTION F: SIGNATURE/HEALTH CARE PROVIDER 10 FORM VALIDITY AND EXPIRATION 10 FORM COMPLETION INFORMATION (REQUIRED) 10 CONTACT INFORMATION (OPTIONAL) 10 USING POLST WITH AN INTERPRETER 11 June 3, 2020. 7AAC 16.010 Do-Not-Resuscitate Protocol Reference Document 1 of 12
MODIFYING THE POLST FORM 11 VOIDING THE POLST FORM 11 TRANSFERRING A PATIENT WITH A POLST FORM 11 SHOULD YOU TRANSFER PATIENTS WITH COMFORT-FOCUSED TREATMENT ORDERS? 11 ADDRESSING DISPUTES REGARDING A POLST FORM 11 June 3, 2020. 7AAC 16.010 Do-Not-Resuscitate Protocol Reference Document 2 of 12
Alaska POLST Program: An Introduction
POLST is an acronym that stands for Physician Orders for Life-Sustaining Treatment. POLST
helps give seriously-ill patients more control over the medical treatment they receive. The
POLST form guides discussions between patients, their families, their physician, and their
healthcare team about treatment wishes in instances of serious illness. POLST transforms those
wishes into physician orders, which are actionable and to be respected across the continuum of
healthcare settings. POLST helps to ensure that patients receive the treatments that they want,
and do not receive treatments that they do not want.
The POLST form complements an Advance Directive and does not replace that document. An
Advance Directive is still necessary to appoint a legal healthcare decision maker, and is
recommended for all adults, regardless of their health status. Use of the POLST form is designed
for persons with advanced chronic, progressive and/or end-stage illness.
Completing a POLST form is completely voluntary. It is intended for patients with advanced
illness or frailty and records choices for medical treatment in the patient’s current state of
health. Once initial medical treatment is begun and the risks and benefits of further therapy are
clear, the patient’s treatment wishes may change, in which case POLST orders can and should
be changed to reflect new preferences and treatment choices. If a POLST form is completed,
Alaska law requires that the healthcare professional honor the completed POLST form and is
provided immunity from civil or criminal liability when complying in good faith with a patient’s
POLST requests.
Requirement to Honor POLST Forms
The State of Alaska has defined that all individuals, including EMT’s, First Responders, and
health care providers shall comply with life-sustaining treatment orders executed by a physician
(M.D./D.O.) according to Alaska Statute AS 13.52.60.
Who Should Consider Having a POLST Form?
The POLST form is intended for patients with advanced illness or frailty where accurate
predictions cannot be made but death is likely in the foreseeable future.
Determine If The Patient Has A Condition That Warrants POLST Form Completion
The health care professional (M.D./D.O.) may use several questions to determine if a POLST
form is warranted. If the answer is “Yes” to any of these questions, the patient may have a
condition that warrants the completion of a POLST form. A POLST form may be completed on
the basis of a deteriorating irreversible health condition.
Does the patient have a disease process that is in an advanced stage;
Is the patient experiencing a significant decline in health (such as frequent aspiration
pneumonias);
Is the patient in a palliative care, hospice program, or skilled nursing facility ; and/or
June 3, 2020. 7AAC 16.010 Do-Not-Resuscitate Protocol Reference Document 3 of 12 Has this patient’s level of functioning become more severely impaired as a result of a
deteriorating health condition when intervention will not significantly impact the
process of decline?
POLST Use for Patients With Significant Physical Disabilities, Developmental
Disabilities and/or Significant Mental Health Condition Who Are Near the End of Life
Special consideration is required when completing a POLST form for a patient with significant
physical disabilities, developmental disabilities and/or a significant mental health condition.
Patients in these groups have the right to both the highest quality of care for their chronic
disability and for equally high quality care at the end of their life.
Patients with disabilities are at risk of bias resulting in under-treatment and/or have their
chronic health conditions mistaken for illnesses or conditions nearing the end of life. The
challenge to the health care professional is to discern when the patient is transitioning from a
stable chronic disability to a more advanced phase of their illness.
Use of POLST for Individuals with Guardians
A guardian is the legal representative of the patient and should participate in a POLST
discussion. Physicians may sign a POLST that includes limitations of treatment when the
patient’s guardian offers a non-opposition to their recommendations for withholding life-saving
or life-sustaining treatment.
Advance Directives and POLST: Working Together in Advance Care
Planning
The voluntary use of the POLST form and the Advance Directive form are complementary to
advance care planning to ensure patient wishes are followed. The purpose of advanced care
planning is to document patient treatment preferences, provide a venue for reviewing and
regularly updating these preferences, and communicate these preferences clearly to first
responders and health care providers. While the Advance Directive and POLST forms differ,
they both play important roles in end-of-life planning.
The POLST form is designed to direct medical treatment in acute situations through specific
medical orders addressing defined medical interventions. Since these orders are followed in
emergent conditions, the POLST should reflect what the patient would want now in their
current state of health.
The focus of the Advance Directive is to document future health care instructions for patients
who no longer can speak for themselves.
Patients with medical decision-making capacity should be assisted by their health care
professional (M.D./D.O.) in voiding their current POLST form and creating a new POLST form to
reflect changing circumstances and wishes. If, however, the patient becomes incapacitated, the
health care instructions and surrogate/health care decision-maker appointed in an Advance
June 3, 2020. 7AAC 16.010 Do-Not-Resuscitate Protocol Reference Document 4 of 12Directive play an important role in implementing goals for care consistent with the patient
wishes in their new state of health. The surrogate/health care decision-maker would participate
in updating POLST orders (if needed) to be consistent with a patient’s preferences as the
patient’s health status changes.
Note that the POLST form is a medical order and not intended to replace an Advance Directive.
The Advance Directive is the appropriate legal document to appoint a surrogate/health care
decision-maker.
Advanced Directive POLST
A Voluntary Legal Document A Voluntary Medical Order
For all adults regardless of health status. For those with advanced illness, or frailty, or
a limited prognosis at any age, depending on
health status.
1. Appoints a legal decision-maker A patient or surrogate/health care decision-
2. Memorizes values and preferences maker participates in the shared decision
3. Is signed by the patient and witnessed making of the POLST form. When the form is
and/or notarized signed by a physician, it becomes a medical
order.
Provides for theoretical situations in which a Provides for likely events that can be
person may not have capacity for decision foreseen. Specific medical orders addressing
making. Guidelines for imagined future defined medical interventions for situations
situations which may arise and for which a that are likely to arise given the patient’s
person may have preferences for a particular health status and prognosis.
kind of care plan.
Who Can Fill Out A POLST Form?
The POLST form is intended for the patient to complete in consultation with his/her health care
provider. If the patient is not fully capable of making decisions, the surrogate/health care
decision-maker as appointed in the Advance Directive is the legally recognized surrogate and
discussions should occur with this person. It is prudent for the signer to review the Advance
Directive and verify its validity. The surrogate/health care decision-maker has the legal right to
accept or refuse medical treatments for the patient as defined by Alaska Statute.
What If The Patient Does Not Have An Advance Directive?
If the patient does not have an Advance Directive, AS 13.52.030 identifies the appropriate
surrogate decision makers that may be invited to speak on the incapacitated patient’s behalf or
provide input into treatment options. Facility ethics committees or institutional policy may
provide additional guidance for those who do not have a surrogate/health care decision-maker.
June 3, 2020. 7AAC 16.010 Do-Not-Resuscitate Protocol Reference Document 5 of 12Determining Appropriate Surrogate/Health Care Decision-Maker for Those Who Have Not Completed an Advance Directive An adult may designate an individual to act as a surrogate/health care decision-maker. In the absence of a designation, or if the designee is not reasonably available, Alaska law defines the classes of patient family who may act as surrogate in AS 13.52.030 (c). If none of the persons identified in the statute is available, then life-sustaining procedures may be withheld or withdrawn upon the direction and under the supervision of the attending physician (some health systems have additional procedures for decision making in the care of those without a surrogate/health care decision-maker). June 3, 2020. 7AAC 16.010 Do-Not-Resuscitate Protocol Reference Document 6 of 12
Completing the POLST Form
The next section of this guidance provides a section-by-section review and instructions for
completing the POLST form. Note that the provider should document the patient’s goals of care
and details of the discussion upon which the orders are based in the patient’s medical record.
References to the “patient’s representative” indicate the surrogate/health care decision-maker
who is permitted to complete or void this form by Alaska Statute.
Any incomplete portion of this form defaults to the presumption that full treatment should be
provided for that section.
Patient Information—Required
The following information is required in the Patient Information section of the POLST form:
Patient First Name
Last Name
DOB
The following information is optional, but is helpful for providing further identification of the
patient:
Middle Name/Initial
Preferred Name
Suffix
Gender
Social Security Number’s last 4 digits
State where form was completed
Section A: Cardiopulmonary Resuscitation Orders
These orders apply only when the patient has no pulse and is not breathing. If the patient
wants CPR and CPR is ordered, then the “YES CPR” box is checked. Full CPR measures should be
carried out and 9-1-1 should be called. If a patient has indicated that they do not want CPR in
the event of no pulse and no breathing, then the “NO CPR” box is checked. CPR should not be
performed.
Section A also includes reference to “mechanical ventilation, defibrillation and cardioversion.”
This information is intended to support the provider in providing clarity to the patient regarding
what “YES CPR” means.
Note: If the patient chooses “YES CPR” in Section A, then the “Full Treatments” box must be
checked in Section B.
June 3, 2020. 7AAC 16.010 Do-Not-Resuscitate Protocol Reference Document 7 of 12Section B: Initial Treatment Orders This section begins with a reminder to reassess and discuss interventions with the patient or patient representative regularly. This is an important element to ensure that the POLST form represents the patient’s most current care goals. These orders in Section B apply to the patient who has a pulse and is breathing. Full Treatments “Goal: Attempt to sustain life by all medically effective means. Provide appropriate medical and surgical treatments as indicated to attempt to prolong life, including intensive care.” This area should be chosen if all life-sustaining treatments are desired. This includes use of intubation, advanced airway intervention, mechanical ventilation, cardioversion, transfer to hospital and use of intensive care as indicated with no limitation of treatment. Full treatments must be chosen if YES CPR is chosen in Section A of this form. Additional clarifying orders may be included in Section C, Additional Orders or Instructions. Selective Treatments “Goal: Attempt to restore function while avoiding intensive care and resuscitation efforts (ventilator, defibrillation and cardioversion). May use non-invasive positive airway pressure, antibiotics and IV fluids as indicated. Avoid intensive care. Transfer to hospital if treatment needs cannot be met in current location, unless another treatment preference is documented in Section C of this form.” This area should be chosen if the patient’s care goals include hospitalization if needed, but the patient wishes to avoid mechanical ventilation and the intensive care unit (ICU). Some patients may want hospitalization and treatments for reversible conditions or exacerbations of their underlying illness with the goal of restoring them to their current state of health (e.g., hospitalization for dehydration, pneumonia). Additional clarifying orders or other specific wishes to limit treatments may be included in Section C, Additional Orders or Instructions. Comfort-focused Treatments “Goal: Maximize comfort through symptom management; allow natural death. Use oxygen, suction and manual treatment of airway obstruction as needed for comfort. Avoid treatments listed in full or select treatments unless consistent with comfort goal. Transfer to hospital only if comfort cannot be achieved in current setting.” This area should be chosen for those patients wishing to avoid hospitalization. Additional clarifying orders may be included in Section C, Additional Orders or Instructions. Section C: Additional Orders or Instructions The purpose of this section is to put context around anything ordered in Section B and any other specific treatment wishes. Information written in this section comprises medical orders June 3, 2020. 7AAC 16.010 Do-Not-Resuscitate Protocol Reference Document 8 of 12
that are in addition to those listed in Section B. These orders may include, but are not limited to: dialysis, blood products, limited time interventions, hydration, cardiac or breathing support, antiarrhythmic drugs, medications, antibiotic treatments, hyperalimentation, electrolyte or acid/base corrective measures, hospice evaluation, chemotherapy or radiation preferences, and diagnostic testing preferences (labs, imaging, or X-ray diagnostic testing restrictions). This section also includes the note “EMS protocols may limit emergency responder ability to act on orders in this section.” EMS regulations, Scope of Practice, and agency protocols dictate the treatments they can provide, and they may not be able to honor what is ordered in this section. Section D: Medically Assisted Nutrition The intent of this area of the POLST form is to indicate high-level decision making about the patient’s desire for surgical (long-term) or non-surgical (short term) treatment to support nutrition needs. Choices in this section include: Provide feeding through new or existing surgically-placed tubes Trial period for artificial nutrition but no surgically–placed tubes No artificial means of nutrition desired Discussed but no decision made (standard of care provided) The purpose of including the choice “Discussed but no decision made (standard of care provided)” is to indicate to other providers that this issue has been previously addressed with the patient. The reference to “standard of care” is included as a reminder to all parties that the absence of a decision defaults to providing the standard of care in this area. Section E: Signature/Patient or Patient Representative (optional) The first statement in this area reinforces that this form is voluntary, and indicates that the patient has discussed treatment options and goals of care with their provider. The patient signature is not required, however, it is highly encouraged that the patient sign this form to confirm that the document accurately reflects the patient’s preferences. It is understood that most states require a patient signature on this form, and the form may not be honored in other states without the patient’s signature included. It is the responsibility of the signer in Section F to know if the patient is capable of making decisions and signing the POLST form. If the patient is not capable of making decisions, the signer in Section F must ensure that the information included on this form was discussed with the appropriate patient representative appointed in the Advance Directive. If there is no Advance Directive, or there is no patient representative identified in the Advance Directive, then refer to the section of this document entitled Determining Appropriate Surrogate For Those Who Have Not Completed An Advance Directive for additional guidance. June 3, 2020. 7AAC 16.010 Do-Not-Resuscitate Protocol Reference Document 9 of 12
Section F: Signature/Health Care Provider POLST is a medical order and, to be valid, must be signed by an authorized provider. In Alaska, only a M.D. or D.O. is authorized to sign in Section F. By signing this form, the provider confirms that the orders were discussed with the patient and they reflect the patient’s wishes. A verbal order is also acceptable, with a follow-up signature, in accordance with the facility’s verbal orders policy. Note: forms may be completed electronically and signed using an electronic signature. If the POLST form has been prepared by someone other than the signer, this attestation confirms that the signing professional personally knows that the information is correct. It is the legal responsibility of the signer, not the preparer, to confirm that POLST orders reflect the patient’s wishes in their current state of health and to assure that a copy of the form is submitted to the POLST Registry. Form Validity and Expiration The bottom of Page 1 of the POLST form indicates that a “copied, faxed or electronic version of this form is a legal and valid medical order.” It is understood that the original copy of the POLST form may not be available, and this statement affirms that other presentations of the form are valid. The final statement on Page 1 indicates “This form does not expire.” While this form and the orders therein do not expire, it is vital that the provider or his/her designee reviews this firm regularly with the patient or patient’s representative. This is recommended to occur at the following intervals: When the patient is transferred from one care setting or level to another; Has a substantial change in health status; Changes primary provider; or Changes his/her treatment preferences or goals of care. Form Completion Information (required) All individuals present for the POLST discussion must be documented in this section. This includes individuals who are not legal decision-makers (friends, family members, etc.). If a health care provider assists in form completion, other than the M.D./D.O. who signed the orders, then this individual’s name must be legibly written in the designated area, along with the date and phone number. Additionally, the provider type must be indicated by checking the correct box or completing the “Other” category. Contact Information (optional) Contact information is provided in this section for convenience and is not required. Note that designating an individual as the Patient’s Emergency Contact in this section does not grant them authority to act as a legal representative for the patient. This is explicitly stated on the form. June 3, 2020. 7AAC 16.010 Do-Not-Resuscitate Protocol Reference Document 10 of 12
You can also read