MYCOTOXIN CONTROL IN LOW- AND MIDDLE-INCOME COUNTRIES - IARC WORKING GROUP REPORT NO. 9
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

MYCOTOXIN CONTROL
IN LOW- AND MIDDLE-
INCOME COUNTRIES
EDITED BY CHRISTOPHER P. WILD,
J. DAVID MILLER, AND JOHN D. GROOPMAN
IARC WORKING GROUP
REPORT NO. 9
MYCOTOXIN CONTROL
IN LOW- AND MIDDLE-
INCOME COUNTRIES
EDITED BY CHRISTOPHER P. WILD,
J. DAVID MILLER, AND JOHN D. GROOPMAN
IARC WORKING GROUP
REPORT NO. 9
Published by the International Agency for Research on Cancer,
150 cours Albert Thomas, 69372 Lyon Cedex 08, France
©International Agency for Research on Cancer, 2015
Distributed by
WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland
(tel: +41 22 791 3264; fax: +41 22 791 4857; email: bookorders@who.int).
Publications of the World Health Organization enjoy copyright protection in accordance with the provisions of
Protocol 2 of the Universal Copyright Convention. All rights reserved.
The designations employed and the presentation of the material in this publication do not imply the expression of any
opinion whatsoever on the part of the Secretariat of the World Health Organization concerning the legal status of any
country, territory, city, or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.
The boundaries and names shown and the designations used on the maps do not imply the expression of any
opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory,
city, or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines
on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or
recommended by the World Health Organization in preference to others of a similar nature that are not mentioned.
Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
The authors alone are responsible for the views expressed in this publication.
The International Agency for Research on Cancer welcomes requests for permission to reproduce or translate its
publications, in part or in full. Requests for permission to reproduce or translate IARC publications – whether for sale or
for non-commercial distribution – should be addressed to the IARC Communications Group, at: publications@iarc.fr.
Cover image: Spreading groundnuts for sun-drying prior to storage in Guinea (Credit: C.P. Wild/IARC).
This book is also available in electronic format from
http://www.iarc.fr/en/publications/pdfs-online/wrk/wrk9/index.php.
IARC Library Cataloguing in Publication Data
Mycotoxin control in low- and middle-income countries / edited by Christopher P. Wild, J. David Miller, John D.
Groopman
(IARC Working Group Reports; 9)
1. Mycotoxins 2. Aflatoxins – adverse effects 3. Fumonisins – adverse effects 4. Developing Countries 5. Food
Contamination – prevention and control 6. Growth Disorders – epidemiology 7. Liver Neoplasms – prevention and
control
I. IARC Working Group Reports II. Series
ISBN 978-92-832-2510-2 (NLM Classification: W1)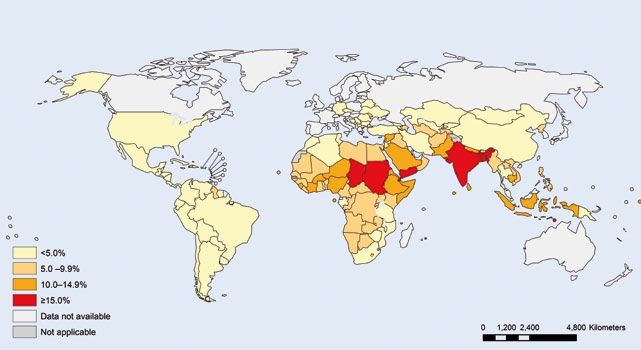
Table of contents Working Group members....................................................................................................................................................v Acknowledgements...........................................................................................................................................................viii Executive summary.............................................................................................................................................................ix Chapter 1...............................................................................................................................................................................1 Human exposure to aflatoxins and fumonisins Chapter 2..............................................................................................................................................................................7 Child stunting in developing countries Chapter 3............................................................................................................................................................................13 Effects of aflatoxins on aflatoxicosis and liver cancer Chapter 4............................................................................................................................................................................17 Effects of aflatoxins and fumonisins on child growth Chapter 5............................................................................................................................................................................23 Fetal and neonatal toxicities of aflatoxins and fumonisins Chapter 6............................................................................................................................................................................27 Effects of aflatoxins and fumonisins on the immune system and gut function Chapter 7............................................................................................................................................................................31 Intervention strategies to reduce human exposure to aflatoxins and fumonisins References........................................................................................................................................................................43 Disclosures of interests....................................................................................................................................................54

Working Group members
Participants Dr Robert Black Dr Wentzel Gelderblom
Director, Institute of Institute of Biomedical
Dr Chidozie Amuzie International Programs and Microbial Biotechnology
MPI Research and Michigan State Johns Hopkins Bloomberg School of Cape Peninsula University
University Public Health of Technology
Mattawan, MI, USA Baltimore, MD, USA Cape Town, South Africa
chidozie.amuzie@mpiresearch.com rblack@jhsph.edu gelderblomw@cput.ac.za
Dr Ranajit Bandyopadhyay Dr Hester Burger Dr Yun Yun Gong
International Institute of Tropical Institute of Biomedical and Microbial School of Biological Sciences
Agriculture (IITA) Biotechnology Queen’s University Belfast
Ibadan, Oyo State, Nigeria Cape Peninsula University of Belfast, United Kingdom
r.bandyopadhyay@cgiar.org Technology y.gong@qub.ac.uk
Cape Town, South Africa
Dr Ramesh V. Bhat (unable to burgerh@cput.ac.za Dr John D. Groopman
attend) Department of Environmental Health
International food safety Dr Kitty F. Cardwell Sciences
specialist (retired) National Institute Johns Hopkins Bloomberg School of
Hyderabad, India of Food and Agriculture Public Health
rameshbhatv@gmail.com Washington, DC, USA Baltimore, MD, USA
kcardwell@nifa.usda.gov jgroopm1@jhu.edu
Working Group members v
Dr Martin Kimanya Dr Gordon S. Shephard Representatives
School of Life Sciences and Institute of Biomedical and Microbial
Bioengineering Biotechnology Dr Amare Ayalew (unable to
Nelson Mandela African Cape Peninsula University of attend)
Institution of Science and Technology Partnership for Aflatoxin Control in
Technology Cape Town, South Africa Africa (PACA)
Arusha, United Republic of Tanzania gshephard@mweb.co.za African Union Commission
martin.kimanya@nm-aist.ac.tz Addis Ababa, Ethiopia
Dr Rebecca Stoltzfus amarea@africa-union.org
Dr J. David Miller (Chair of the Director, Program in International
Meeting) Nutrition Dr Vittorio Fattori
Department of Chemistry Division of Nutritional Sciences Food Safety and Codex Unit
College of Natural Sciences Cornell University Food and Agriculture Organization
Carleton University Ithaca, NY, USA of the United Nations (FAO)
Ottawa, Ontario, Canada rjs62@cornell.edu Rome, Italy
david_miller@carleton.ca vittorio.fattori@fao.org
Dr Yoshiko Sugita-Konishi
Dr Isabelle Oswald Department of Food Hygiene Dr Sindura Ganapathi
Toxalim Research Centre The Graduate School of Life and Program Officer, Global Health
in Food Toxicology Environmental Sciences Bill & Melinda Gates Foundation
French National Institute Azabu University Seattle, WA, USA
for Agricultural Research (INRA) Sagamihara, Kanagawa Prefecture, sindura.ganapathi@gatesfoundation.org
Toulouse, France Japan
isabelle.oswald@toulouse.inra.fr y-konishi@azabu-u.ac.jp Dr Jef Leroy
International Food Policy
Dr Michelangelo Pascale Dr Paul C. Turner Research Institute
Institute of Sciences of Food Maryland Institute for Applied Washington, DC, USA
Production Environmental Health j.leroy@cgiar.org
National Research Council of Italy College Park, MD, USA
Bari, Italy pturner3@umd.edu Dr Adelheid Onyango
michelangelo.pascale@ispa.cnr.it Department of Nutrition for Health
Dr Gerald N. Wogan and Development
Dr Gary A. Payne Department of Biological World Health Organization
Department of Plant Pathology Engineering Geneva, Switzerland
North Carolina State University Massachusetts Institute of onyangoa@who.int
Raleigh, NC, USA Technology
gary_payne@ncsu.edu Cambridge, MA, USA Dr Shelly Sundberg
wogan@mit.edu Senior Program Officer, Global Health
Dr Timothy D. Phillips Bill & Melinda Gates Foundation
College of Veterinary Medicine Dr Felicia Wu (joined by Seattle, WA, USA
and Biomedical Sciences teleconference) shelly.sundberg@gatesfoundation.org
Texas A&M University Department of Agricultural, Food,
College Station, TX, USA and Resource Economics Dr Angelika Tritscher
tphillips@cvm.tamu.edu Michigan State University Department of Food Safety and
East Lansing, MI, USA Zoonoses
Dr Ronald Riley fwu@anr.msu.edu World Health Organization
Toxicology and Mycotoxin Research Geneva, Switzerland
Unit tritschera@who.int
United States Department of
Agriculture
Athens, GA, USA
ron.riley@ars.usda.gov
vi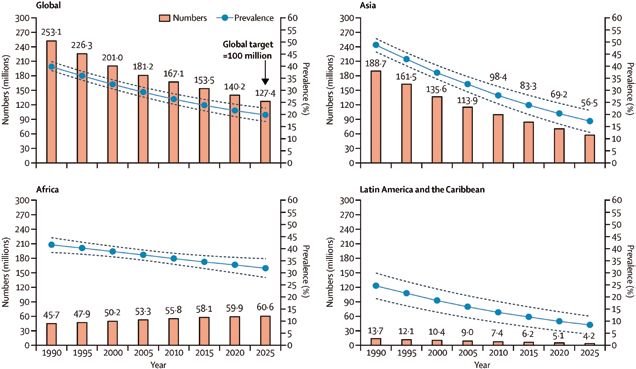
IARC Secretariat Administrative Assistance Production Team
Dr Rosita Accardi-Gheit Ms Susan Haver-Legros Jennifer Brandt
Infections and Cancer Biology Administrative Assistant Technical Editor
Group Office of the Director
Section of Infections International Agency for Research Karen Müller
International Agency for Research on Cancer English Editor
on Cancer Lyon, France
Lyon, France havers@iarc.fr Sylvia Lesage
accardir@iarc.fr Publishing Assistant
Ms Laurence Marnat
Dr Reetta Holmila Secretary
Epigenetics Group Office of the Director
Section of Mechanisms of International Agency for Research
Carcinogenesis on Cancer
International Agency for Research Lyon, France
on Cancer marnatl@iarc.fr
Lyon, France
holmilar@iarc.fr
Dr Christopher P. Wild
Director
International Agency for Research
on Cancer
Lyon, France
director@iarc.fr
Working Group members viiAcknowledgements The production of this IARC Working Group Report was partially funded by a grant from the Bill & Melinda Gates Foundation to IARC. Thanks go to Reetta Holmila, Rosita Accardi-Gheit, Susan Haver-Legros, and Laurence Marnat for their sup- port at the Working Group meeting and during the preparation of this Report. The meeting was the occasion to present the IARC Medal of Honour (2010) to Professor Gerald Wogan in person, to recognize his lifetime contribution to understanding the role of aflatoxins in human liver cancer. viii Acknowledgements
Executive summary
An estimated 500 million of the The International Agency for ies needed to yield further evidence
poorest people in sub-Saharan Af- Research on Cancer (IARC) of of the merit of specific intervention
rica, Latin America, and Asia are the World Health Organization approaches.
exposed to mycotoxins at levels that convened a Working Group Meet- The Working Group addressed
substantially increase mortality and ing in Lyon from 30 June to 3 July current scientific knowledge in four
morbidity (Pitt et al., 2012). The prob- 2014. This IARC Working Group key areas: the extent of exposures
lem is not newly recognized. Shortly Report provides a systematic, in- to aflatoxin and fumonisin; the ef-
after the discovery of aflatoxins, the dependent review of the scien- fects on prenatal, infant, and child
impact on child health was brought tific evidence base on the adverse health; relevant mechanistic infor-
into immediate focus. After the re- health effects from aflatoxin and mation; and effective intervention
porting of several deaths in children fumonisin exposure through con- strategies in low-income settings.
in Africa due to consumption of afla- sumption of contaminated maize In the past, the focus has largely
toxin-contaminated meal, a decision and groundnuts. An evaluation is been on the impact of aflatoxin
was made in 1966 by the FAO/WHO/ provided of interventions, available on cancer risk. Considering sev-
UNICEF Protein Advisory Group to on an individual and a community eral recent studies, mainly in Af-
set a limit of 30 ppb aflatoxin in pro- level, to reduce human exposure rica, this Report also considers
tein supplements made from ground- and disease. Therefore, this Re- the potentially far greater burden
nuts (Anonymous, 1966). In con- port provides an authoritative basis of growth faltering after weaning
trast to the situation today, in 1966 for action at an international level, (child stunting).
throughout most of Africa the propor- enabling decision-makers to invest Stunting in children results from
tion of calories from maize was mod- with confidence in effective strate- chronic undernutrition, leading to
est, with a greater proportion coming gies to save lives. It also provides adverse effects on survival, health,
from sorghum, millet, and cassava. guidance on additional critical stud- and development, entailing a large
Executive summary. Mycotoxin control in low- and middle-income countries ixglobal population burden; in 2012, an is inexpensive and user-friendly and Four of the interventions were
estimated 162 million children young- has a wide dynamic range should judged to be ready for implemen-
er than 5 years worldwide were stunt- be developed. This could support a tation. The intervention for which
ed. Poor-quality diets and high rates rapid alert system that informs re- the strongest evidence of improve-
of infection, both in pregnancy and sponses and appropriate actions for ment of health exists, but which is
in the first years of life, result in poor food safety. also the most difficult to achieve,
child growth, but the relative contri- Aflatoxins are a cause of human was to increase dietary diversity.
butions to stunting are unknown. At liver cancer and, in high doses, have Other strategies deemed ready for
the same time, provision of all of the caused deaths from aflatoxicosis. implementation were sorting of the
established nutrition-specific inter- More recently, significant negative ef- crop; a package of post-harvest
ventions in the most affected regions fects of aflatoxin on child growth have measures, including improved
would reduce the prevalence of been reported, as well as immune storage; and, in Latin America for
stunting by only about 20% (Bhutta et modulation. These observations are maize, optimized nixtamalization.
al., 2013), illustrating the large knowl- consistent with impaired fetal devel- Several interventions were consid-
edge gap in how to prevent stunting, opment and immune system and ered that might be used in emer-
including the potential impact of ex- gut function in animal models. Taken gency situations of extremely high
posure to mycotoxins. together, the few well-documented contamination (e.g. chemoprotec-
This Report concludes that surveil- population-based studies and the tants, agents that can be put into
lance data on exposure to aflatoxins mechanistic data in relevant animal the diet to ameliorate the effects of
are generally lacking outside the de- models suggest that mycotoxin ex- aflatoxin once ingested).
veloped countries. However, avail- posure contributes to stunting, inde- As currently envisaged, the rec-
able data from measurements of con- pendent of and with other risk factors. ommendations would be relevant
taminated crops and through the use Further longitudinal studies of my- for investment of public, nongov-
of exposure biomarkers in exposed cotoxin exposure and child stunting, ernmental organization, and pri-
populations demonstrate that myco- including studies of the underlying vate funds at the scale of the sub-
toxin exposures can be high through- mechanisms, merit investment. sistence farmer, the smallholder,
out Africa, as well as in Latin America The Working Group assessed the and through to a more advanced
and parts of Asia. More recently, question of effective interventions value chain.
among maize-consuming populations in low-income countries using stud-
in these regions, the high concurrent ies where there was reliable direct References
exposure to aflatoxins and fumonisins or indirect evidence of improvement
Anonymous (1966). Alarm about mycotoxins.
has been documented. of health, including reduced myco- Nature. 212:1512.
Notwithstanding the challenges, toxin biomarker levels. Using widely
future mycotoxin monitoring pro- accepted criteria for evaluating evi- Bhutta ZA, Das JK, Rizvi A, Gaffey MF, Walk-
er N, Horton S, et al.; Lancet Nutrition Inter-
grammes should be prioritized. As- dence about public health interven- ventions Review Group; Maternal and Child
sessment of possible implementation tions, some 15 interventions were Nutrition Study Group (2013). Evidence-based
within existing surveillance systems placed into one of four categories: (1) interventions for improvement of maternal
and child nutrition: what can be done and at
should be considered. In the short sufficient evidence for implementa- what cost? Lancet. 382(9890):452–77. http://
term, data from individual studies of tion, (2) needs more field evaluation, dx.doi.org/10.1016/S0140-6736(13)60996-4
sufficient quality should be added (3) needs formative research, and (4) PMID:23746776
to the Global Environment Monitor- no evidence or ineffective. Recom- Pitt JI, Wild CP, Baan RA, Gelderblom WCA,
ing System (GEMS)/Food Contami- mendations on how to approach the Miller JD, Riley RT, et al., editors (2012).
nation Database. Finally, a rapid necessary further investigation and Improving public health through mycotoxin
control. Lyon, France: International Agency for
screening approach aimed at the potential scale-up were also consid- Research on Cancer (IARC Scientific Publica-
field/subsistence-farming level that ered. tions Series, No. 158).
xChapter 1
chapter 1.
Human exposure to
aflatoxins and fumonisins
Data on the prevalence of myco- clear picture of the extent to which their role in disease development,
toxins in staple foods are essential mycotoxins compromise food safety and determine the efficacy of in-
for all applied research into their and health, at either an individual or tervention strategies. The recent
impact on health and on effective a population level. However, this is development of multitoxin analytical
mitigation. Country- or region- generally not achieved in develop- methods, whether applied to food or
specific knowledge enables the ing countries, primarily due to a lack to biological samples as biomark-
identification of susceptible edible of country-specific data, resources, ers, has raised awareness of the
crops that are responsible for toxin and analytical capacity. concurrent exposure to aflatoxin
exposure in specific populations. Exposure biomarkers, such as and fumonisin as well as sometimes
Prevalence data can indicate how serum aflatoxin–albumin adducts to other, unanticipated mycotoxins.
effective maximum levels have been (AF–alb) or urinary fumonisin B1
in influencing food safety, while (UFB1), offer a more integrated es- Exposure to aflatoxins
acknowledging that their enforce- timate of exposure from all sources
ment could have food security im- for either aflatoxin or fumonisin, and Aflatoxins are mycotoxins found
plications. Monitoring of prevalence offer potentially more reliable expo- in four main forms: aflatoxin B1
also provides information on how sure estimates. Measurement of ex- (AFB1), B2 (AFB2), G1 (AFG1), and
various implemented strategies to posure, either by measures of food G2 (AFG2). Aflatoxins occur on a
reduce contamination or exposure consumption combined with con- wide range of crops, including the
levels directly affect toxin levels. tamination levels or by using bio- major staple cereals (e.g. maize),
Ideally, exposure assessment, as markers of exposure, can be used edible nuts and legumes, and their
one component of risk assessment, to identify the main dietary contribu- products. In general, AFB1 occurs
integrates mycotoxin levels with tors to exposure, detect areas with at the highest levels and is the most
food consumption patterns and thus unacceptable exposures, assess toxic. The main fungal producers
provides, via risk characterization, a health impacts of mycotoxins and of aflatoxins are Aspergillus flavus,
Chapter 1. Human exposure to aflatoxins and fumonisins 1which produces AFB1 and AFB2, This compound can be detected in income regions. However, it is im- and Aspergillus parasiticus, which the urine and milk of exposed ani- portant to note that these estimates produces all four forms. Contamina- mals, including humans. Data on are based on very limited data- tion can occur before or after harvest the carryover of AFM1 to breast milk sets, particularly in those regions at or both. are limited, but the carryover has greatest risk of high exposures. Aflatoxin contamination levels been estimated at 0.1–0.4% (Zarba can vary widely, from products that et al., 1992), and exposure of in- Exposure to fumonisins meet the strict maximum levels fants to AFM1 from human breast set by the European Commission milk has been reported in devel- Fumonisins, which are produced (2 µg/kg for AFB1; 4 µg/kg for total oping countries (Shephard, 2004; mainly by Fusarium verticillioides aflatoxins [sum of AFB1, AFB2, Turner, 2013; Magoha et al., 2014). (Sacc.) Nirenberg and F. proliferatum AFG1, and AFG2] for cereals and In addition, AFM1 from milk of live- (Matsush.) Nirenberg, are common nuts for direct human consumption) stock consuming AFB1-contami- contaminants of maize and maize- (European Commission, 2010) nated feed is a further source of based products. Fumonisin B1 (FB1) to products with levels that can exposure. The 56th meeting of the is the most abundant (generally pose a risk of acute aflatoxicosis. Joint FAO/WHO Expert Committee ~70% of the total fumonisin contam- For example, determination of on Food Additives (JECFA) com- ination), and it normally co-occurs total aflatoxins in a rural market piled data on AFM1 levels found with lesser amounts of fumonisin B2 survey in four districts during an in commercial raw and processed (FB2) and B3 (FB3). Occurrence on acute outbreak in Kenya, in 2004, dairy milk (Henry et al., 2001). sorghum has also been reported showed a range of total aflatoxins of However, few data were available (Bulder et al., 2012). 1–46 400 µg/kg, with 7% of samples from Africa, and those reported are Fumonisins were evaluated by above 1000 µg/kg (Lewis et al., unlikely to reflect typical village- or JECFA in 2001 and 2012 (Bolger 2005). In 2003, data available from subsistence farm-level exposures. et al., 2001; Bulder et al., 2012). As African countries were summarized Further study is needed to better exposure is a product of both con- by Shephard (2003). More recent understand the consequences of tamination level and consumption, data, including summaries of global AFM1 ingestion from breast milk certain rural communities in de- occurrence in samples submitted and/or from the milk of livestock in veloping countries can exceed the for analysis, have been presented Africa. provisional maximum tolerable dai- by Rodrigues et al. (2011) and Global intake estimates for af- ly intake (PMTDI) of 2 μg/kg bw/day Schatzmayr and Streit (2013). latoxin (ng/kg body weight [bw]/ of fumonisin if their diet contains Recent African data have also been day) have been reported based high amounts of maize (Burger et provided by Gnonlonfin et al. (2013). on estimates of typical maize al., 2010). Examples from this literature include and nut consumption, con- Fumonisin intake estimates (µg/ groundnut cake from Nigeria (range, tamination levels, and body kg bw/day) in several regions of 20–455 μg/kg); raw groundnut weight (Liu and Wu, 2010). For Africa were recently reviewed (Wild from Kenya (non-detectable to Africa, estimates were made for and Gong, 2010), including Burki- 7525 μg/kg) and Botswana (12– the Democratic Republic of the na Faso (0–2); Bizana (1–19), Cen- 329 μg/kg); and maize from Benin Congo (range, 0–27), Ethiopia (1– tane (2–36), Transkei (4), and Kwa (2–2500 μg/kg), Ghana (20–355 μg/ 36), The Gambia (4–115), Kenya Zulu-Natal (0), South Africa; and kg), and Zambia (1–109 μg/kg). (4–133), Mozambique (39–180), Bomet, Kenya (< 0.1). Intakes of Other aflatoxin-contaminated food Nigeria (139–227), South Africa 0.2–26 µg/kg bw/day in Tanzanian sources reported in various African (0–17), the United Republic of Tan- children were reported (Kimanya countries include cassava, tiger zania (0–50), and Zimbabwe (18– et al., 2014). nuts, cowpeas, sorghum, okra, 43). Similarly high intakes were In Latin America, estimates of and hot peppers, although due to reported for China and countries fumonisin intake in Guatemala were consumption patterns, maize and in South-East Asia, compared with reported to be 3.5 µg/kg bw/day groundnuts dominate in terms of western Europe and North Amer- (urban) and 15.5 µg/kg bw/day (rural) level of exposure. ica at 0–1 ng/kg bw/day (Turner (Wild and Gong, 2010), and more Aflatoxin M1 (AFM1) is a toxic et al., 2012; Schleicher et al., recently a range of 0.20–23 µg/ metabolite of AFB1 and a possible 2013). These data indicate a much kg bw/day was reported (Torres et human carcinogen (IARC, 2012). higher burden of exposure in low- al., 2014). 2
Chapter 1
Biomarkers for aflatoxins Health and Nutrition Examination cally significant correlation was ob-
and fumonisins Survey (NHANES) were almost all served between the concentrations
(99%) below the limit of detection of these biomarkers (r = 0.375,
Food contamination and food intake (LOD), and the geometric mean of P < 0.001) (Shirima et al., 2013).
can vary greatly within rural subsis- the positives was only 0.8 pg/mg Urinary aflatoxin and fumonisins
tence farm settings and between vil- (Schleicher et al., 2013). were observed less frequently in
lages and individuals. Assessments AF–alb has also been used in samples from two major cities,
of both of these parameters present various studies to assess associa- Yaoundé and Bamenda, in Cam-
analytical and measurement diffi- tions between aflatoxin exposure eroon (Abia et al., 2013) and from
culties. In addition, there is interin- and infant and early childhood rural regions of Nigeria (Ezekiel et
dividual variation in toxicokinetics growth faltering (Turner, 2013). al., 2014), although co-exposures
and toxicodynamics related to toxin Typically there is greater confi- did occur. Differences in the sen-
ingestion. For these reasons, con- dence in the long-term markers sitivities of the analytical methods
siderable effort has been given to of aflatoxin exposure to assess between these studies limit direct
developing biomarkers for aflatoxins health outcomes, as they provide comparison. A separate study from
and fumonisins (Turner et al., 2012). an integrated measure over several Cameroon, looking at urinary my-
For AFB1, the peripheral blood months. Several putative biomark- cotoxin markers in young children,
AF–alb biomarker has been validat- ers for fumonisin exposure have also reported aflatoxin and fumoni-
ed for moderate- to long-term expo- been investigated. These include sin exposure (Njumbe Ediage et al.,
sure (several months), whereas the sphingoid bases in plasma and 2013). These data were comple-
urinary biomarkers, aflatoxin–N7- urine and FB1 in hair, nails, serum, mented by a survey across multiple
guanine and AFM1, reflect shorter urine, and faeces (Shephard et al., agro-ecological zones in Camer-
exposures. The application of these 2007); however, none of these have oon, in which maize, groundnuts,
biomarkers has helped establish been validated in human studies. and cassava were found to be con-
the link between aflatoxin exposure UFB1 has been measured in hu- taminated with multiple mycotoxins
and the development of liver cancer man samples in regions with known (fumonisins were found in 74% of
(Kensler et al., 2011; IARC, 2012) high exposure to dietary fumonisins the maize samples and aflatoxins
and has allowed the efficacy of in- (Gong et al., 2008a; Xu et al., 2010; in 22% of the maize, 29% of the
tervention studies to be demonstrat- van der Westhuizen et al., 2011; Ri- groundnuts, and 25% of the cas-
ed (Turner et al., 2005). ley et al., 2012; Torres et al., 2014). sava samples) (Ediage et al., 2014).
Validated aflatoxin biomarker In general, statistically significant In a study by Probst et al. (2014), a
data from sub-Saharan Africa show relationships between UFB1 and ei- total of 339 maize samples from 18
that the ranges of exposures are ther estimated or measured FB1 in- countries in Africa were assessed
likely to vary greatly in many re- takes were reported; however, the for aflatoxin and fumonisin contam-
gions and within and across closely data indicate that the urinary mea- ination. Aflatoxins were detected
located villages and agro-ecolog- sure was only moderately reflective (LOD, 1 µg/kg) in 47% of the sam-
ical zones, as well as seasonally of the level of intake. ples, with 7% exceeding 20 µg/kg
and annually (Turner et al., 2012; and 6% exceeding 100 µg/kg (the
Turner, 2013). The biomarker data Co-occurrence of aflatoxins maximum level was 1409 µg/kg).
further highlight the early-life bur- and fumonisins Fumonisins were detected (LOD,
den of exposure, including in utero 500 µg/kg) in 81% of the samples,
and during early infancy. Exposures The co-occurrence of aflatoxins and with 7% exceeding 5000 µg/kg and
in West African studies involve both fumonisins has been widely docu- 3% exceeding 100 000 µg/kg. Afla-
maize and groundnuts as the pri- mented by both biomarker studies toxin and fumonisin co-contamina-
mary sources of intake of aflatox- and food analyses. In the United tion occurred in 35% of the samples.
ins. Typical biomarker levels in chil- Republic of Tanzania, AF–alb and Concentrations of co-contaminants
dren younger than 5 years in Benin, UFB1 were assessed in young varied by region, but for the Coast
The Gambia, and Togo range up children (Shirima et al., 2013). The Province in Kenya, for example,
to 1000 pg aflatoxin–lysine/mg al- prevalence of detection of both of 50% of samples contained high
bumin (Turner, 2013). By compari- the mycotoxins was high, and 82% levels of both aflatoxins (mean,
son, levels of AF–alb reported from of the children were positive for 97 µg/kg) and fumonisins (mean,
the recent United States National both. Also, a modest but statisti- 32 000 µg/kg) (Probst et al., 2014).
Chapter 1. Human exposure to aflatoxins and fumonisins 3In Latin America, co-exposures Key scientific gaps mycotoxin detection in food com-
to aflatoxins and fumonisins have modities is a complex task, there is
also been documented. Maize from The problem of mycotoxin exposure a tool available to support countries
22 districts in Guatemala was ana- is most acute in developing coun- in this regard: the Food and Agri-
lysed; 36% of 572 samples tested tries, which lack resources and ana- culture Organization of the United
positive for aflatoxins (mean, 63 µg/ lytical capacity for analyses. Conse- Nations (FAO) Mycotoxin Sam-
kg; range of positives, 5–2655 µg/ quently, few data are reported from pling Tool (http://www.fstools.org/
kg), and 99% of 640 samples test- developing countries and those mycotoxins/). Further, there is a
ed positive for fumonisins (mean, available are usually based on only World Health Organization (WHO)
1800 µg/kg; range of positives, 10– a limited number of samples of un- programme (Global Environment
17 000 µg/kg) (Torres et al., 2015). certain quality. As a result, there is Monitoring System – Food Contam-
a widening gap between the qual- ination Monitoring and Assessment
Analytical limitations ity and quantity of prevalence data Programme [GEMS/Food]) that
generated by laboratories in devel- collects global food contamination
One limitation with urinary biomark- oped countries compared with de- data and reports food consumption
er approaches is the volumes of veloping countries. There is thus a data. Average per capita food con-
urine required. Even though techno- need in the developing countries to sumption data are reported based
logical development of highly sen- have sampling and analytical tools on the FAO Food Balance Sheet
sitive liquid chromatography-mass available that are fit for specific pur- data. It is important to note that the
spectrometry (LC-MS) techniques poses, such as: database provides average con-
will help support biomonitoring, the • A rapid screening method aimed sumption levels but will not capture
approach itself may be limited by at the field/subsistence farm lev- the food consumption pattern at the
instrumentation costs, restricting el that is inexpensive and user- subsistence farm level. Another da-
analysis to specialist laboratories. friendly and has a wide dynamic tabase within GEMS/Food collects
With the development of multitoxin analytical range. This could addi- occurrence data for contamina-
analytical techniques based on tionally help support a rapid alert tion levels, including aflatoxins and
LC-MS/MS, multibiomarker meth- system that informs responses and fumonisins in food products and
ods have been developed for urinary appropriate actions for food safety. crops. It would be useful to highlight
biomeasures for toxins, including • A comprehensive regional or coun- the opportunity for researchers to
FB1 and AFM1 (Solfrizzo et al., 2011; try-wide monitoring programme, add their studies to this database.
Warth et al., 2012), as extensions involving the establishment of However, acquiring data on con-
of multimycotoxin methods for food a reference laboratory within a sumption and contamination levels
analysis. These methods have been country/region. The monitoring in subsistence farmers will remain a
applied in Africa to evaluate expo- programme should be developed significant hurdle.
sure (Abia et al., 2013; Shephard within existing surveillance sys- Among monitoring options, an
et al., 2013; Ezekiel et al., 2014). To tems and be expanded over time. approach that might be implement-
date, there have been limited efforts For example, many regions have ed is sampling at community maize
to compare multimycotoxin methods national health and nutrition pro- milling facilities. For example, in
from different laboratories. Thus, grammes where archived biospec- some parts of East Africa farmers
currently there is greater confidence imens could be requested. Future could bring maize to a local milling
in the data from single measures, national surveys of this nature may operation, where subsampling and
and for increased utility these inter- be asked to collect larger volumes aflatoxin and fumonisin analyses
laboratory comparison studies are of biospecimens (e.g. to support could be carried out using rapid
urgently needed. An additional con- urinary xenobiotic surveillance). test kits for field application. Rela-
cern is that some of the multimyco- De novo monitoring activities could tively large data collection activities
toxin methods, especially for foods, include both food measures and may be possible in such settings,
may be measuring contaminants of biomarkers. providing an improved surveillance,
limited relevance to human health. For a successful food monitoring although this will capture only some
This could result in additional costs programme, it is essential to have of the prevalence data in some re-
(e.g. of measuring > 60 metabolites) effective sampling plans in place. gions and none in others. This also
while potentially leading to inaccu- While it is recognized that design- may, however, provide a target site
rate measurements. ing effective sampling plans for for intervention.
4Chapter 1
Measures of individual exposures sure is known to be high. The lack predictive of the level of intake com-
are important for epidemiological in- of reagents such as aflatoxin– pared with relationships reported for
vestigations of disease causation lysine and mono-adducted AF–alb aflatoxin biomarkers. For general
and for demonstration of efficacy is a major constraint and needs to be biomonitoring this is not a major is-
of intervention. The development of addressed. Enzyme-linked immuno- sue; however, this is a concern when
a reliable source of certified stan- sorbent assay (ELISA) approaches making assessments in relation to
dards, especially for aflatoxin bio- are typically less expensive, but an putative health effects and assess-
markers, would allow a substantial additional issue is a lack of commer- ing the efficacy of interventions. For
increase in biomarker-directed epi- cially available kits or antibodies. the use of FB1 and AFM1, it was noted
demiology research. While LC-MS provides robust data, that neither of these predicts longer-
Therefore, the problem of insuf- the analytical costs are prohibitive term exposures, and while serum
ficient data could also be addressed for most laboratories. Exposure of AF–alb is used for this purpose in af-
by the use of individual biomark- in
fants in developing countries to latoxin biomonitoring and epidemiol-
ers of exposure. Aflatoxin biomark- AFM1 also needs to be monitored as ogy, there remains a need to develop
ers are well understood, but the these countries are prone to higher a long-term exposure biomarker for
most useful for long-term exposure AFB1 exposures. fumonisin. An additional challenge
studies, AF–alb, is currently mea- UFB1 has been measured by is the need for higher-throughput
sured in only a limited number of LC-MS in several world regions, and analytical tools, which would benefit
laboratories. It would be advanta- again a current concern is the cost of from a cooperative activity between
geous if this analysis were more the analysis. While dose–response experts in exposure assessment and
generally available, especially in relationships were reported, the uri- researchers with subject matter ex-
countries where aflatoxin expo- nary measure was not as strongly pertise in mycotoxins.
Chapter 1. Human exposure to aflatoxins and fumonisins 5chapter 2.
Chapter 2
Child stunting in
developing countries
Stunting and wasting in children the most effective intervention is the there are others such as head cir-
are measures reflecting states of supply of foods with adequate nutri- cumference and mid-upper arm
chronic and acute undernutrition tional quality to complement breast- circumference that are commonly
that have important adverse effects feeding in the first 2 years of life. used in surveillance for severe
on survival, health, and develop- The physical growth of children acute malnutrition.
ment. In impoverished settings, within a normative range has im- Length (recumbent, for age
poor-quality diets and high rates of portant implications both within < 2 years) or height (standing, for
infection, both in pregnancy and in that age span and into adulthood age 2–4 years) or weight is com-
the first 2 years of life, lead to fe- (Bhutta et al., 2013). Insufficient pared to an international growth
tal growth restriction (FGR) and gains in length/height and weight standard (WHO Multicentre Growth
poor child growth. This results in from birth to age 5 years, resulting Reference Study Group, 2006),
an estimated 26% of the world’s from childhood undernutrition, put and the result is most commonly
children younger than 5 years hav- the child at increased risk of mor- expressed as a Z-score (standard
ing stunted stature, and 8% be- bidity and mortality from infectious deviation score). The Z-score is the
ing much too thin for their height diseases as well as impaired mental observed value for length/height or
(i.e. wasted) (UNICEF-WHO-The development, reduced learning ca- weight minus the median value of
World Bank, 2012). Proven inter- pacity in school, and lower earning the growth standard, with this result
ventions to prevent the FGR that potential as an adult, among other divided by the standard deviation of
contributes to stunting include mul- effects (Victora et al., 2008; Adair the growth standard. If the Z-score
tiple vitamin and mineral supple- et al., 2013; Bhutta et al., 2013). for length/height-for-age is below
ments and provision of balanced As noted, childhood undernutri- −2, the child is considered to have
energy/protein supplements to tion is usually defined by physical inadequate linear growth or to be
pregnant women, as well as control size. Measures of length/height and stunted. If the Z-score for weight-
of maternal infections. After birth, weight are most common, although for-age is below −2, the child is said
Chapter 2. Child stunting in developing countries 7to be underweight. The weight and 1990, with an average annual rate to infectious agents and toxins. The
length/height measures can be used of reduction of 2.1%. The preva- global prevalence of moderate or
together to create an indicator of lence of stunting varies substan- severe wasting was estimated to be
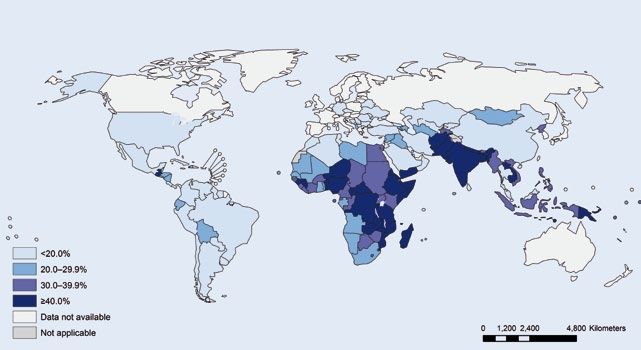
wasting: a child whose Z-score for tially by world region (Fig. 2.1), with 8.0% (95% CI, 6.8–9.3%) for 2011.
weight-for-length/height is below −2 the highest prevalence in Africa and Again, there is regional variation in
is considered to be wasted. South-Central Asia (which includes the prevalence (Fig. 2.3), with the
India). The decline in the preva- highest prevalence in South-Central
Prevalence of child lence of stunting has been greater Asia (14.8%; 95% CI, 11.1–19.4%),
malnutrition for Asia and Latin America than South-East Asia (9.7%; 95% CI,
for Africa, which is the only region 7.5–12.6%), and Africa (8.5%; 95%
The latest UNICEF-WHO-The World that has had an increasing number CI, 7.4–9.6%). The numbers of chil-
Bank joint child malnutrition esti- of stunted children, due to the slow dren with wasting and severe wast-
mates provide global and regional declines in the prevalence and the ing were estimated to be 52 million
prevalences for stunting and wast- high fertility rate (Fig. 2.2) (UNI- and 19 million, respectively, for
ing based primarily on population- CEF-WHO-The World Bank, 2012; 2011. Recent estimates indicate that
based, nationally representative Bhutta et al., 2013). nearly 2 million deaths in children
surveys, with modelling to make In countries with an overall preva- worldwide can be attributed to FGR
regional estimates (UNICEF-WHO- lence of stunting greater than 10%, and stunting, or a third of all child
The World Bank, 2012). The global there is a gap – in some cases very deaths (UNICEF-WHO-The World
prevalence of stunting in children wide – between the high prevalence Bank, 2012; Bhutta et al., 2013).
younger than 5 years was estimated in the poorest 20% and the low prev-
to be 26% (95% confidence interval alence in the least poor 20% of the Risk factors for child
[CI], 24–28%) for 2011, the most re- population. This illustrates the rela- malnutrition
cent data. The number of stunted tionship of stunting and other forms
children in that year was estimated of undernutrition with poverty and Preventable causes of FGR in utero
to be 165 million. The prevalence of the associated problems of food in- and reduced growth of the child dur-
stunting has declined from 40% in security and environmental exposure ing the first 2 years of life include low
Fig. 2.1. Latest country prevalence estimates for stunting among children younger than 5 years. Source: Reprinted
from UNICEF-WHO-The World Bank (2012), p. 9, © 2012, with the permission of the publisher.
8Fig. 2.2. Trends in prevalence and numbers of children with stunted growth (height-for-age Z-score < −2), by
selected United Nations regions and globally, 1990–2010, and projected to 2025 on the basis of United Nations
prevalence estimates. Source: Reprinted from Black et al. (2013), © 2013, with permission from Elsevier. Data from
UNICEF-WHO-The World Bank (2012).
Chapter 2
Fig. 2.3. Latest country prevalence estimates for wasting among children younger than 5 years. Source: Reprinted
from UNICEF-WHO-The World Bank (2012), p. 10, © 2012, with the permission of the publisher.
Chapter 2. Child stunting in developing countries 9body mass index, small weight gain High rates of diarrhoea and other and quality of diets and provision
and micronutrient deficiencies dur- infectious diseases also affect this of safe food supplements contain-
ing pregnancy, and maternal infec- age group, even with continued ing adequate micronutrients have
tions (Bhutta et al., 2013; Christian et breastfeeding as complementary been shown to improve growth and
al., 2013). It has been estimated that foods are introduced. In a pooled reduce the prevalence of stunting.
27% of all births in low- and middle- analysis of nine community-based Full (90% coverage) implementa-
income countries have FGR, with the studies in low-income countries, the tion of these interventions would re-
highest prevalence in Asia, especial- odds of stunting at age 24 months duce stunting by at least 20% in the
ly South Asia (Bhutta et al., 2013; Lee increased multiplicatively with each 34 countries that include 90% of the
et al., 2013). Nutritional status at birth episode of diarrhoea or day of di- world’s stunted children (Fig. 2.4).
is related to the risk of being stunted arrhoea before that age. The pro- These interventions would also be
at age 2 years. Globally, it has been portion of stunting attributed to five useful to prevent wasting (Bhutta et
estimated that 20% of stunting can previous episodes of diarrhoea was al., 2013). In stable non-emergency
be attributed to FGR. In some coun- 25% (95% CI, 8–38%) (Checkley et situations, wasting usually coexists
tries the attributable fraction is even al., 2008). In addition to the clinical with stunting after age 6–9 months.
higher. In India, where nearly half of infections, frequent exposure to con- However, severe acute malnutrition
all births have FGR, the attributable taminated food and water and the (i.e. severe wasting) can occur more
fraction for stunting is more than a household environment results in abruptly even in a previously well-
third (Christian et al., 2013). ingestion of microbes, causing sub- nourished child due to food scarcity,
Most of the growth faltering lead- clinical infections that damage the such as in famine, natural disaster,
ing to stunting occurs between small intestine. It has been hypoth- or civil conflict. These are situations
ages 3 months and 18–24 months esized that environmental enteric where targeted food distribution pro-
(Victora et al., 2010), a period of vul- dysfunction (EED) or environmental grammes are needed.
nerability because often insufficient enteropathy, a condition character- There is limited evidence that
and poor-quality food is provided to ized by structural abnormalities of interventions in sectors other than
the child. Exclusive breastfeeding is the intestinal epithelium, altered bar- health and nutrition may have a
recommended for the first 6 months rier integrity, mucosal inflammation, beneficial impact on stunting. These
of life but is uncommonly practiced; and reduced nutrient absorption, areas include efforts to improve ag-
globally, only about 30% of infants may contribute to growth faltering ricultural productivity and improve-
aged 1–5 months are exclusively and stunting (Keusch et al., 2013). It ments in water, sanitation, and hy-
breastfed (Bhutta et al., 2013). The has also been hypothesized that zinc giene, because of their potential to
early introduction of fluids will re- deficiency may be involved in the reduce the rates of diarrhoea and
duce the production and ingestion pathogenesis of EED (Lindenmayer possibly the occurrence of EED
of breast milk and substitute foods et al., 2014). As noted by Lunn (Dangour et al., 2013; Spears, 2013).
of lesser nutritional quality that also (2000) and discussed later in this Food safety interventions would be
have a high risk of microbial con- Report, there is a potential role for expected to positively influence nu-
tamination. In most of the affected ingested mycotoxins to contribute trition and growth in young children
regions, more than 60% of children to EED or to other mechanisms that by eliminating infectious agents that
aged 6–23 months are breast- lead to stunting. cause diarrhoea through foodborne
fed (Bhutta et al., 2013). However, transmission and possibly through
the complementary foods that are Interventions against child avoidance of exposure to chemicals
introduced too often have inad- malnutrition and mycotoxins.
equate nutrient density, calories,
protein, essential fats, and micronu- Although breastfeeding, as recom- Key scientific gaps and
trients, and may contain infectious mended for the first 2 years of life, is research needs
bacteria and/or toxins. Deficiency important for the babies’ health and
of the micronutrient zinc has been dietary intake, the major interven- Recent publications indicate that
consistently associated with stunt- tions to prevent stunting are related FGR is a more important contribu-
ing, and increased linear growth in to the foods that are given in addition tor to neonatal and infant mortality
infants has been demonstrated with to breast milk from age 6–23 months (Katz et al., 2013) and to stunted
provision of daily zinc supplements (i.e. complementary diet). Educa- linear growth (Christian et al.,
(Bhutta et al., 2013). tion about age-appropriate quantity 2013) than previously recognized.
10Fig. 2.4. Countries with the highest burden of malnutrition. These 34 countries account for 90% of the global burden
of malnutrition. Source: Reprinted from Bhutta et al. (2013), © 2013, with permission from Elsevier.
Chapter 2
This makes it imperative to look with multiple micronutrients in preg- ments improves growth and reduces
more closely at the causes of FGR nancy, instead of only iron and the occurrence of stunting; however,
and possible interventions to re- folic acid, would provide added the effect size relative to the height
duce it or ameliorate its negative benefits at modest additional cost. deficit is small. Zinc supplements
effects. Maternal undernutrition and If multiple micronutrients are to be for children in the first 2 years of
infection, as well as other possible provided to pregnant women or to life also have a statistically signifi-
determinants of FGR, need addi- children, further product develop- cant, but small, benefit in reducing
tional study, especially to identify ment research, linked with stud- stunting. The Lancet nutrition series
feasible interventions to reduce its ies of the prevalence and extent of estimated that the nutrition-specific
occurrence. If programmes intend micronutrient deficiencies in various interventions together, if scaled up
to increase the provision of bal- low-income populations, is needed. to 90%, would reduce the preva-
anced energy/protein supplements This will ensure that the composi- lence of stunting by only about 20%
during pregnancy, there are ques- tion is optimized to meet nutritional (Bhutta et al., 2013), illustrating the
tions about the composition of sup- needs, reduce nutrient interactions, large gap in our knowledge of how
plements (preferably using locally avoid side-effects, enhance accept- to prevent stunting. Additional stud-
available and safe foods) and their ability, and reduce costs. ies of the determinants of stunted
timing in pregnancy, how best to Most stunting of linear growth growth need to include the possible
target the food supplements to vul- takes place in the first 2 years of role of subclinical infections and ex-
nerable populations and undernour- life. The relative contributions to posure to potentially harmful agents
ished or food-insecure women, how stunting of dietary insufficiency, such as mycotoxins.
to achieve sufficient consumption, infectious diseases or subclinical The first 2 years of life are a
and ultimately the cost–effective- infections, and inflammation are un- crucial period for both develop-
ness of alternative ways to deliver known and may vary, as does the ment and growth, which need to
this intervention. prevalence of stunting, by setting in be considered separately as well
In spite of the known benefits of low- and middle-income countries. as jointly. Young children in impov-
iron and folic acid supplementation There is good evidence that promo- erished households lack both the
in pregnancy, the current use of this tion of nutritious complementary stimulation needed for cognitive and
intervention is low. Supplementation foods or provision of food supple- psychosocial development and the
Chapter 2. Child stunting in developing countries 11food and environmental conditions serious consequences for survival, derstanding of the behavioural and needed to promote physical growth health, and development. Implemen- biological determinants of stunting and prevent illness. tation of proven interventions to pre- and wasting, including the possible In conclusion, stunting and wast- vent their occurrence and to provide role of mycotoxins, and the effec- ing are nutritional conditions that most treatment must be given greater pri- tiveness of other nutrition-specific commonly affect children in low- and ority. Parallel efforts should address interventions and nutrition-sensitive middle-income countries and have the evidence gaps through better un- approaches. 12
chapter 3.
Effects of aflatoxins on
aflatoxicosis and liver cancer
Chapter 3
While there has been a very ex- proliferation, a lesion often noted in outbreak. In a survey of 65 markets
tensive focus on the role of aflatoxin experimental animals after acute af- and 243 maize vendors, 350 maize
exposure in hepatocellular carci- latoxin exposure (Krishnamachari et products were collected from the
noma (HCC), over the years sev- al., 1975; Bhat and Krishnamachari, most affected districts. Of these
eral cases of acute aflatoxicosis in 1977). An outbreak of acute aflatox- maize products, 55% had aflatox-
humans have been reported in re- icosis in Kenya in 1981 was also as- in levels greater than the Kenyan
gions of some developing countries sociated with consumption of maize regulatory limit of 20 ppb, 35% had
(Shank et al., 1971). highly contaminated with aflatoxin levels greater than 100 ppb, and 7%
(Ngindu et al., 1982). There were had levels greater than 1000 ppb.
Acute aflatoxin poisoning 20 hospital admissions, with 60% Makueni, the district with the most
mortality. In a more recent report aflatoxicosis cases, had signifi-
The clinical manifestations of afla- (Lye et al., 1995), the consumption cantly higher aflatoxin levels in
toxicosis include vomiting, abdomi- of aflatoxin-contaminated noodles maize from markets than did Thika,
nal pain, pulmonary oedema, fatty resulted in acute hepatic encepha- the study district with the fewest
infiltration, and necrosis of the liver. lopathy in children in Malaysia. Up cases (geometric mean aflatoxin,
In the 1970s, there was an outbreak to 3 mg of aflatoxin was suspected 52.91 ppb vs 7.52 ppb; P = 0.0004).
of putative aflatoxin poisoning in to be present in a single serving of Maize obtained from local farms in
western India when heavily moulded contaminated noodles. the affected area was significantly
maize was consumed. There were In April 2004, one of the largest more likely to have aflatoxin levels
at least 97 fatalities, all of which oc- documented aflatoxicosis outbreaks greater than 20 ppb compared with
curred in households where the con- occurred in rural Kenya, resulting maize bought from other regions of
taminated maize was consumed. in 317 cases and 125 deaths. Af- Kenya or other countries (odds ratio
Histopathology of liver speci- latoxin-contaminated home-grown [OR], 2.71; 95% confidence interval
mens revealed extensive bile duct maize was the major source of the [CI], 1.12–6.59). In addition to the
Chapter 3. Effects of aflatoxins on aflatoxicosis and liver cancer 13You can also read