Objective - Overview of Difficult to Control Atopic Dermatitis - Association of Asthma Educators
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
3/4/21
Overview of Difficult to Control
Atopic Dermatitis
Gregory Metz, MD, AE-C
Oklahoma Allergy and Asthma Clinic
Clinical Associate Prof of Medicine, University of Oklahoma
AAE March 2021
Objective
Discuss diagnostic and appropriate treatment modalities, including biologic therapy,
and the challenges of clinical management in patients with atopic dermatitis
1
3/4/21
Disclosures
None
The AAE acknowledges that this program did not receive funding in support of this program. It is
understood that the program is planned for scientific/educational purposes and not for the purpose
of promoting any product. This program is not a repeat program or enduring version of a prior
program. Gregory Metz, today's speaker, has no relevant financial relationships with ineligible
companies and will disclose prior to presenting. In addition, none of the planners for this
educational activity have a relevant financial relationship(s) to disclose with ineligible companies
whose primary business is producing, marketing, selling, re-selling, or distributing healthcare
products used by or on patients.
Fishbein AB, Silverberg JI, Wilson EJ, et al. Update on Atopic Dermatitis: Diagnosis, Severity Assessment, and Treatment Selection. J Allergy Clin Immunol Pract. 2020 Jan;8(1):91-101
2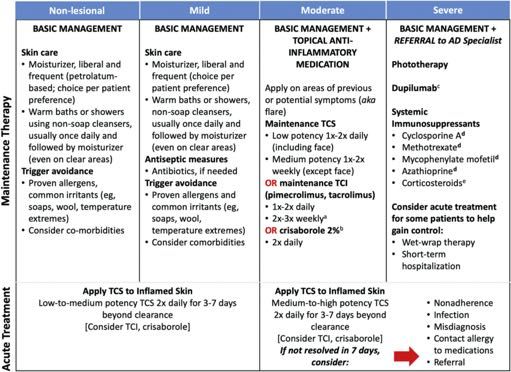
3/4/21
Atopic Dermatitis
• Prevalence of AD is ~13% of the population1,2
• Of those, ~20% moderate AD, ~2-3% severe AD
• If AD not responding to standard therapies, first start by re-evaluating the diagnosis
1 Arkwright PD, Motala C, Subramanian H, et al. Management of difficult-to-treat atopic dermatitis. J Allergy Clin Immunol Pract. 2013 Mar;1(2):142-51.
2 Boguniewicz M, Alexis AF, Beck LA, et al. Exp Persp on Management of Mod-to-Sev AD: A Multidisciplinary Consensus Addressing Current and Emerging Therapies. JACI in Prac 2017 Nov - Dec;5(6):1519-32.
Characteristic features of AD1
• Essential features:
• Itching
• Typical morphology (facial/neck/extensor in young; flexural any age)
• Chronic & relapsing course
• Important features:
• Early age of onset, atopic hx, dry skin, lichenification
• Associated features:
• Keratosis pilaris, hyperlinear palms, perifollicular accentuation
1 Boguniewicz M, Alexis AF, Beck LA, et al. Expert Persp on Mngmt of Mod-to-Sev AD: A Multidisciplinary Consensus Addressing Current and Emerging Therapies. J Allergy Clin Immunol Pract. 2017 Nov - Dec;5(6):1519-32.
3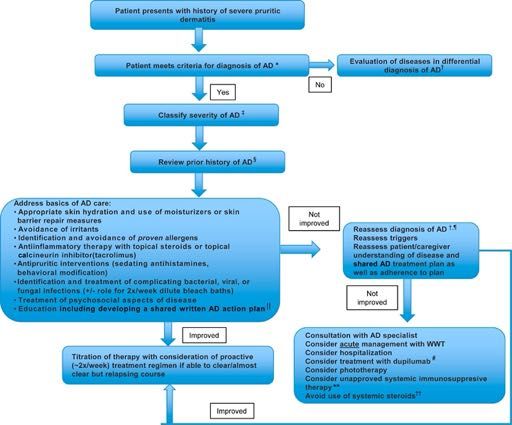
3/4/21
AD: Differential Diagnosis
• Other diseases that can be mistaken for AD:
• Other primary skin conditions (Netherton Syndrome, KP, Psoriasis, seb derm)
• PID (SCID, Wiskott-Aldrich, Hyper-IgE Syndromes)
• Graft vs. host disease
• Mineral/vitamin deficiencies
• Infections (impetigo, fungal, scabies)
• Drug reactions
• Contact dermatitis, allergic & irritant
• Malignancies (cutaneous T cell lymphoma, Letterer-Siwe disease)
Atopic Dermatitis
The majority of treatment failures are caused by not understanding or fully implementing
standard therapies1
• Poor understanding of disease etiology, course and treatment
• Inappropriate treatment expectations
• Unaware of correct treatment frequency / treatment regimen too complex
• Poor motivation
• Child in charge of treatment
• Lack of perceived benefit from therapies
• Concern for side effects (burning) or long term effects (steroid phobia)
• Cost
• Running out of medications too quickly
• Inability to refill medications
1Arkwright PD, Motala C, Subramanian H, et al. Management of difficult-to-treat atopic dermatitis. J Allergy Clin Immunol Pract. 2013 Mar;1(2):142-51.
4
3/4/21
Atopic Dermatitis & Allergic Comorbidities
• Food allergies
• Airborne allergies
• Hypersensitivity to contactants
• Hypersensitivity to treatments
AD and Food Allergy: It’s Complicated
Rarely is food allergy the primary cause of AD
• The rate of food-exacerbated AD varies with the severity1
• 1-3% of children with mild AD
• 5-10% of children with moderate AD
• 20-30% of children with severe AD
• Food-exacerbated AD is very rare adults.
• Food allergy should be considered with AD in 2 settings2:
• Immediate allergic symptoms with ingestion of a suspected food allergen
• Children
3/4/21
Environmental Allergies
• Exposure to environmental allergens may exacerbate underlying AD
• Common allergens include dust mite, animals and pollens (tree, weed, grass)1
• Diagnosis involves thorough history and selected allergy testing
1Werfel T, Heratizadeh A, Niebuhr M, et al. Exac. of AD on grass pollen exposure in an environmental challenge chamber. JACI. 2015 Jul;136(1):96-103.
When to Consider Allergic Contact Dermatitis (ACD)?
• Patient has erythematous papules, vesicles or eczematous rash especially when localized
• Patient presents with anogenital rash or “baboon syndrome”
• Severe hand eczema (especially in an industry worker)
• Widespread dermatitis prior to initiating systemic immunosuppression
• Patient’s dermatitis fails to respond to treatment
• If ACD is suspected, chemical allergy testing (patch testing) is recommended
63/4/21
Sources of Contact Allergens1
• Airborne exposure (plant/botanical sources)
• Ragweed/Compositae
• Direct application by personal care products, treatments
• Soap, shampoo, jewelry/metals/clothing, moisturizers that we ask patients to use
• Prescription ointments and creams prescribed (including topical steroids)
• Ectopic transfer of the allergen
• Nail glues, hair products
• Connubial contact dermatitis
• Systemic contact dermatitis
• Nickel, BOP, Gold, Mercury, Cobalt, Al, Chromium, Zinc
• Propylene glycol (cetirizine, acetaminophen, ibuprofen, glucosamine, clarithromycin, cellcept)
• Formaldehyde (aspartame used as a sugar substitute is metabolized in the body to formaldehyde)
• Ethylenediamine (midol, pamprin, hydroxyzine, cetirizine, levocetirizine, meclizine)
1Contact Dermatitis 2011. Jeanne Duus Johansen, Peter J. Frosch
Common Causative Contact Allergens by Site
Location Source Allergens
Face Cosmetics, plants, ectopic transfer Pollen (compositae), fragrance, BOP,
methacrylates, tosylamide/formaldehyde
Scalp/Neck Cosmetics, hair products, hair dye, jewelry Paraphenylenediamine, cocoamidopropyl
betaine, fragrance, BOP, formaldehyde/FR
Hands Lotion, cosmetics, gloves Formaldehyde/FR, fragrance, rubber
chemicals (thiurams, carbamates), topical
antibiotics
Anogenital Topical medications, topical analgesics, Topical steroids, fragrance, MI/MCI
cleaning/soothing wipes
Feet Shoes Carbamates, thiurams, chromates
Legs Lotions, medications Fragrance, BOP, topical antibiotics, topical
steroids, lanolin
73/4/21
AD and Infections
• Most patients with AD are colonized with Staph aureus
• Even without active infection, immune reactions to Staph can exacerbate AD
• Skin infections with Staph aureus can also occur
• Warning signs: painful skin, assymetric, oozing, crusting, failure to improve
• Increasing incidence of MRSA
• Secondary HSV infection (eczema herpeticum) is a dermatologic emergency
• Monomorphic vesicles, punched-out erosions, hemorrhagic crusts
• Immune reactions (both IgE and T cell mediated) to skin colonizers such as Malassezia
species can flare head and neck dermatitis
AD Standard Therapies
• Patient education
• Moisturizers
• Reduce itching/scratching
• Avoidance of allergic and irritant triggers
• Topical steroids
• Topical calcineurin Inhibitors
• Topical PDE4 inhibitors
• Treatment of infections if they occur
• Mixed recommendations on bathing frequency & bleach baths
• Attend to sleep disturbance & psychologic effects
83/4/21
Figure 1
Arkwright PD, Motala C, Subramanian H, et al. Management of difficult-to-treat atopic dermatitis. J Allergy Clin Immunol Pract. 2013 Mar;1(2):142-51
Therapies for refractory AD
• Wet wraps
• Biologic therapies
• Dupilumab
• mAb targeting alpha subunit of IL4/IL13 receptor (blocks inflammatory pathway in ADA)
• Systemic immunosuppressants/immunomodulators
• Phototherapy
93/4/21
AD Case
• 56 year old male with long history of allergies, asthma and eczema presents for
evaluation of worsening eczema and bilateral hand rash.
• Since his teens, he has experienced widespread dry skin, itching and red patches that
are all over, but worse behind knees and in the antecubital fossa
• His rash worsened over the past 6 months and now involves both hands leading to
fissuring and pain
Past Medical Hx
• Seasonal runny nose, congestion, worse in the spring and fall
• Symptomatic GERD, using ranitidine prn
• Asthma since childhood, no ER visits, no systemic steroids in past year. Using
fluticasone 110mcg 1 puff bid, albuterol about once per month
• Meds:
Cetirizine 10mg daily
Fluticasone nasal 2 squirts daily
Fluticasone 110mcg 1 puff bid
Albuterol 1-2 puffs every 4-6 hours only as needed
TMC 0.1% cream to affected skin bid prn
103/4/21
AD Case
• Allergies: no known medication or food allergies
• Family history: both parents have AR
• Social history:
• Works in a bank, in office, on computer, does not handle money, does not use foam or gel pad while typing
• On the weekends, he likes to play tennis, does not wear gloves to play
• No pets in the home
• Does not wear gloves for routine yardwork
AD Case
PE:
• AAOx4
• Sclera and conjunctiva are clear
• Nasal mucosa boggy
• Lungs clear without wheezing
• CV regular rate and rhythm
• MSK no joint swelling
• Widespread dry skin, scattered excoriations, lichenification involving popliteal and antecubital
fossa. Bilateral hands with erythema and fissuring. No crusting, oozing or streaking erythema.
113/4/21
www.uptodate.com
What questions do you have
for the patient?
123/4/21
AD Case
• When asked “why do you think you are having this rash?”, his explanation demonstrates good
understanding of AD and treatment but he’s not sure why hands are now affected
• He is avoiding all irritants, fabric softeners, dryer sheets
• He is not using hand sanitizer & completely drying hands after washing
• Using all hypoallergenic skin care products (brought own hand soap to work)
• Pat drying skin after bathing
• Using CeraVe cream BID
• Has TMC 0.1% used 1-2 x per day to rash (avoiding face and neck)
• Dilute bleach baths once per week
• These therapies historically adequately controlled his symptoms
• He does report the only new therapy is that when his hands fissure open and bleed, he puts on over the
counter topical antibiotic
• No recurrent infections or other symptoms suggestive of other systemic disease process
Poll Question: what should we do next?
Perform food allergy testing to evaluate for food trigger
Treat with antibiotic for secondary skin infection
Perform chemical allergy testing (patch testing)
Increase frequency of topical steroid use to 3-4 times per day
133/4/21
Figure 1
Arkwright PD, Motala C, Subramanian H, et al. Management of difficult-to-treat atopic dermatitis. J Allergy Clin Immunol Pract. 2013 Mar;1(2):142-51
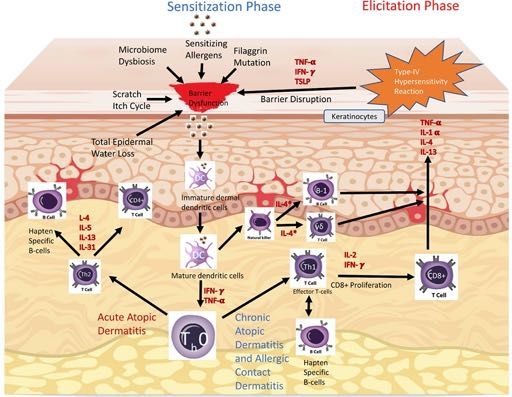
AD & Allergic Contact Dermatitis: Pathophysiology
Milam EC, Jacob SE, Cohen DE. Contact Dermatitis in the Patient with Atopic Dermatitis. J Allergy Clin Immunol Pract. 2019 Jan;7(1):18-26.
143/4/21
Milam EC, Jacob SE, Cohen DE. Contact Dermatitis in the Patient with Atopic Dermatitis. J Allergy Clin Immunol Pract. 2019 Jan;7(1):18-26.
Application of Patch Tests Removal of Patches at 48 Hours Final Read at 96 Hours
Adapted from Milam EC, Jacob SE, Cohen DE. Contact Dermatitis in the Patient with Atopic Dermatitis. J Allergy Clin Immunol Pract. 2019 Jan;7(1):18-26.
153/4/21
Patch Test Results
Positive tests (3+) to:
• Bacitracin (topical antibiotic)
• Balsum of Peru (BOP- fragrance)
• Methylisothiazolinone/Methylchloroisothiazolinone (MI/MCI- preservative)
Case
• Implemented complete avoidance of topical antibiotic ointment with significant
improvement
• He checked to make sure he was avoiding BOP and MI/MCI at home and work
• The following month, he called and said he identified another exposure to both
BOP and MCI/MI
• A couple of times per month, he visits and sometimes helps his brother who is restoring a vintage
car. If his hands got greasy, he uses cleaning wipes that his brother has in his garage.
163/4/21
On ingredient list, it has both BOP and MI
Patient’s hand dermatitis almost completely resolved with
allergen avoidance and his chronic AD was better controlled
with allergen/irritant avoidance, frequent moisturization and
as needed topical anti-inflammatory therapy
173/4/21
Summary
Brar KK, Nicol NH, Boguniewicz M. Strategies for Successful Management of Severe Atopic Dermatitis. JACI Prac. 2019 Jan;7(1):1-16.
The Journal of Allergy and Clinical Im m unology: In Practice 2020 891-101DOI: (10.1016/j.jaip.2019.06.044)
183/4/21
Questions?
19You can also read