OCCUPATIONAL health SOUTHERN AFRICA - the Mine ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
OCCUPATIONALhealth
SOUTHERN AFRICA
Vol. 26 No. 2 MARCH/APRIL 2020
Official Journal of SASOM, SAIOH, SASOHN and MMPA
• The South African Society of Occupational Medicine
• Southern African Institute for Occupational Hygiene
• South African Society of Occupational Health Nursing Practitioners
• Mine Medical Professionals Association
An accredited journal of the Department of Higher Education and Training (RSA)
Occupational Health Southern Africa www.occhealth.co.za Vol 26 No 2 March/February 2020 1
2 Vol 26 No 2 March/April 2020 Occupational Health Southern Africa www.occhealth.co.za

Vol. 26 No. 2 March/April 2020 Cover photo: Springkell TB Sanatorium was
OCCUPATIONALhealth
opened by the Chamber of Mines in 1911
source: https://heritage-estate.co.za
SOUTHERN AFRICA
EDITOR-IN-CHIEF
Gill Nelson, PhD (Occupational Health): University of the Witwatersrand, SA. Affiliations: University of the Witwatersrand, SA;
MMPA Life Member
e-mail: gill.nelson@wits.ac.za
ASSISTANT EDITOR
Ntombizodwa Ndlovu, PhD (Occupational Health): University of the Witwatersrand, SA. Affiliation: University of the
Witwatersrand, SA
e-mail: zodwa.ndlovu@wits.ac.za
The South African Society of
Occupational Medicine (SASOM)
EDITORIAL BOARD
Jaco Botha
Cas Badenhorst, PhD (Occupational Hygiene): North-West University, SA. Affiliations: Anglo American, SA; North-West University, SA;
Tel: +27 (0)12 803 7418
SAIOH Member
Fax: +27 (0)11 507 5085
e-mail: info@sasom.org Kevin Beaumont, MA (English): University of Natal, SA. Affiliation: MettaMedia, Publisher’s Representative
website: www.sasom.org Michelle Bester, M Tech Nursing Science: Tshwane University of Technology, SA. Affiliations: Tshwane University of Technology, SA;
SASOHN Member
Natalie Copeling, B Tech (Occupational Health Nursing): Stellenbosch University, SA. Affiliations: Cape Peninsula University of
Technology, SA; SASOHN Member
Johan du Plessis, PhD (Occupational Hygiene): North-West University, SA. Affiliations: North-West University, SA; SAIOH Member
Spo Kgalamono, FCPHM (Occ Med): CMSA, SA. Affiliations: National Institute for Occupational Health, SA; University of the Witwatersrand,
SA; SASOM Member
Daan Kocks, MD: Medical University of Southern Africa, SA-FCPHM (Occ Med): CMSA, SA. Affiliations: Sefako Makgatho Health
Sciences University, SA; SASOM President
Dipalesa Mokoboto, MBCHB: University of KwaZulu-Natal, SA; MPhil (Medical Law and Ethics): University of Pretoria, SA. Affiliations:
Department of Mineral Resources and Energy, SA; University of Pretoria, SA; MMPA Deputy President
Southern African Institute for Vusumuzi Nhlapho, DOccMed: RCP, London, UK. Affiliations: South African Medical Association; MMPA Member
Occupational Hygiene (SAIOH)
Kate Smart
EDITORIAL ADVISORY PANEL
Tel: +27 (0)71 672 4916 Tom Fuller, ScD (Industrial Hygiene/Work Environment): University of Massachusetts Lowell, USA; MSPH (Radiological Hygiene): The
Fax: +27 (0)86 631 6117 University of North Carolina, USA; MBA (Finance): Suffolk University, USA. Affiliations: Occupational Hygiene Training Association,
e-mail: info@saioh.co.za Board member; IOHA, President-elect
website: www.saioh.co.za
Jim Phillips, PhD: Leeds University, UK. Affiliation: University of Johannesburg, SA
André Rose, MBBCH, MMed (Community Health), FCPHM, PhD: University of the Free State, SA. Affiliation: National Institutes of
Health, USA
Mary Ross, MBBCH: University of the Witwatersrand, SA; Fellowships in Occupational Medicine (SA and UK), Public Health (UK), Travel
Medicine (UK), Tropical Medicine (Australasia). Affiliations: University of the Witwatersrand, SA; Faculty of Occupational Medicine, UK;
Journal of the Society for Occupational Medicine, UK; International Commission for Occupational Health; World Health Organization;
SASOM Honorary Life Member; MMPA Honorary Life Member
PRODUCTION BY TECHNEWS PUBLISHING PUBLISHER
Michelle Perry Kevin Beaumont, Cell: +27 (0)82 774 2210
South African Society of
Tel: +27 (0)31 764 0593 PO Box 210, Tulbagh, 6820
Occupational Health Nursing e-mail: michelle@dbn.technews.co.za e-mail: kevin@mettamedia.co.za
Practitioners (SASOHN)
Lettie Grantham ADVERTISING SUBSCRIPTION SERVICES
Tel: +27 (0)861 SASOHN (727646) Tracy Wolter, Cell: +27 (0)82 331 2440 Kevin Beaumont, Cell: +27 (0)82 774 2210
Fax: +27 (0)86 263 8757 e-mail: tracy@technews.co.za e-mail: kevin@mettamedia.co.za
e-mail: office@sasohn.co.za
website: www.sasohn.co.za
© Copyright Material appearing in this issue may not be reproduced without the permission of the editors or publishers in any form whatsoever.
Disclaimer: The publishers, editors, SASOHN, SASOM, SAIOH and MMPA are not liable for any damages or loss incurred as a result of any statement
contained in this journal. Whilst every effort is made to ensure accuracy in this publication, neither the publishers, editors, SASOHN, SASOM, SAIOH
nor MMPA accept any responsibility for errors or omissions in the content and reserve the right to edit all contributions. The views expressed in this
publication are not necessarily those of the publishers, editors, SASOHN, SASOM, SAIOH or MMPA, neither do these societies, publishers or editors
endorse, or guarantee the products or services advertised, or claims made by the manufacturers. It is the author’s responsibility to obtain the neces-
sary permissions to publish articles.
This Journal is on the Department of Higher Education and Training’s list of Approved South African Journals; authors of peer-reviewed
papers thus qualify for subsidies for their affiliated tertiary institutions. It is also listed in African Index Medicus; and is on the International
Committee of Medical Journal Editors (ICMJE) website list of Journals Following the ICMJE Recommendations for the Conduct, Reporting,
Editing and Publication of Scholarly Work in Medical Journals.
Mine Medical Professionals Also published online at www.occhealth.co.za
Association (MMPA) Use your personal login details to access past issues. Should you have any queries, e-mail kevin@mettamedia.co.za.
Mbalenhle Buthelezi
How to subscribe
Tel: +27 (0)11 568 2054
e-mail: mbalenhleb@mpas.org.za
website: www.mmpa.org.za
Join SASOHN, SAIOH, SASOM or MMPA and receive a premier subscription to Occupational Health Southern
Africa as a benefit of Society membership.
PUBLISHED BY Alternatively, subscribe directly to the Journal via our website: www.occhealth.co.za.
MettaMedia Click on the ‘Subscribe’ button and follow four simple steps to activate your annual subscription.
Occupational Health Southern Africa www.occhealth.co.za Vol 26 No 2 March/February 2020 3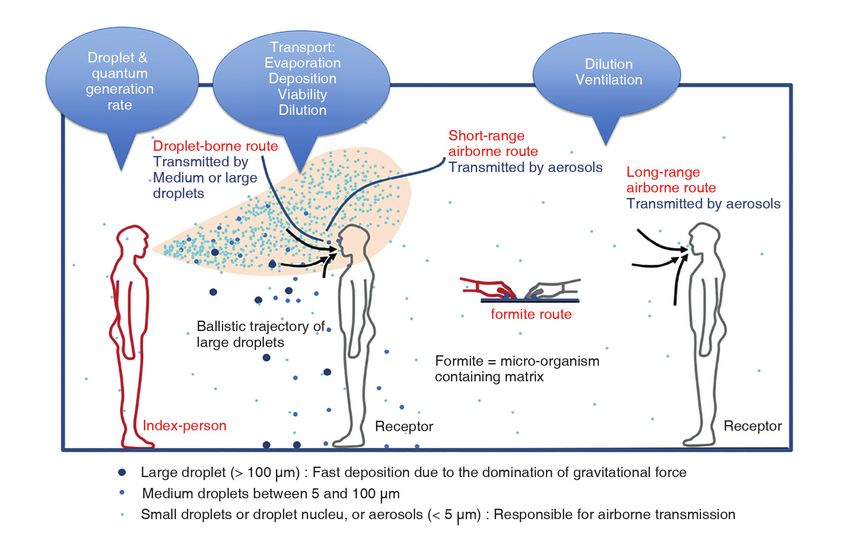
From the Guest Editor . . .
Rajen Naidoo – Associate Professor; Head: Occupational and Environmental Health; College of Health Sciences, University of KwaZulu-Natal
e-mail: naidoon@ukzn.ac.za
This issue of Occupational Health to protect our workers. These manuscripts provide the first steps.
Southern Africa is published at a COVID-19 is historic in its own right but, within this issue of the
pivotal moment in the history of the Journal, the epidemic and the history of occupational health have a
planet. Outside wars, no person has poignant meeting. The original focus of this special issue was to have
faced such a direct threat to their been solely on the history of occupational health. It was supposed to
health and wellbeing in over 100 coincide with the International Commission on Occupational Health’s
years. While the World Wars had a dev- (ICOH’s) 7th International Conference of the History of Prevention
astating impact and, more recently, of Occupational and Environmental Diseases Scientific Committee,
especially in South Africa, the HIV/ scheduled for Durban in May 2020, now a minor casualty of the epi-
AIDS epidemic threatened our infant demic. The Conference has been postponed to 2022. Further details
democracy, control was possible. can be found in the announcement on the last page of this issue, and
COVID-19’s ubiquitous presence and on the Journal website.
rapid spread, its severe impact, its vari- Despite the rapid turn of events, manuscripts already accepted
ous unknowns, and the absence of therapeutic interventions at this for this issue reflect the original theme of ‘history’. The contents pro-
stage, force us to develop new ways of working and engaging socially. vide us pause in the context of COVID-19 – the histories of the four
This is a life-changing moment in history, indeed. organisations primarily responsible for shaping occupational health
COVID-19 has dramatic occupational health consequences. Health in our country are traced, and prominent practitioners who led the
workers are the single most affected working population, globally. way are featured. Interestingly, all of these histories in South African
While most countries are not actively collecting data on the number occupational health can trace their routes to the first major epidemic
of infections and deaths among health workers, it is estimated that to arrive on our shores. The discovery of precious metals set South
10–20% of all infected cases are health workers.1,2 The numbers Africa on a new course of development. In order to exploit mineral
emerging from countries such as Italy (4 800),3 Spain (12 200)4 and wealth effectively, workers were imported from the coal mines of
the United Kingdom (65 deaths)5 are all likely to be underestimates Wales and Cornwall, and from other parts of Europe. They brought
– but provide a clear picture that these are the workers that require with them tuberculosis and, faced with the high levels of silica in our
our earnest attention. mines, they succumbed, in their hundreds, to miners’ phthisis. This,
As we emerge into a new phase of the epidemic and the ‘unlock- at the time, was unusual, leading the Chamber of Mines, in 1902, to
ing’ of the economy, workers in essential industries and other key make a call to the international community to undertake research
sectors will bear the brunt of the infection. It becomes necessary to and propose interventions.6 From these early days, grew structures
ensure that we have the appropriate protocols in place to protect such as the Pneumoconiosis Research Unit and our early legislation
these returning workers as best we can. There are several challenges in miners’ health. The professional bodies that arose subsequently,
emerging for occupational health professionals in this new phase. and the pioneers in early occupational health, were largely driven to
Our best estimates, that 10–15% of South African workplaces have address this new epidemic. Today, we recognise their rich history in
some sort of occupational health cover, implies that there are more protecting workers in this country, and find ways to apply the lessons of
unprotected workers who will enter into the ‘unlocked’ economy. Even 100 years ago to the new crisis facing workers today. History, in the
if strict criteria for ‘unlocking’ are put into place, all economic sectors are shape of deadly infections affecting thousands of workers, repeats itself.
dependent on a supply chain of small and medium enterprises, casual
workers and informal workers – most of whom lack the occupational REFERENCES
health safety net of the larger enterprises they support. Within the sup- 1. Burrer SL, De Perio MA, Hughes MM, Kuhar DT, Luckhaupt SA, McDaniel CJ,
et al. Characteristics of health care personnel with COVID-19 - United States,
port network is also public transport – a closed, high-risk environment. February 12-April 9, 2020. MMWR Morb Mortal Wkly Rep. 2020; 69:477-481. DOI:
It is clear that, if we wish to ‘unlock’ our economy and simultaneously http://dx.doi.org/10.15585/mmwr.mm6915e6.
not overwhelm our health services and place our health workers’ lives 2. Editorial. COVID-19: protecting health-care workers. Lancet. 2020;
395(10228):922. doi:10.1016/S0140-6736(20)30644-9.
at risk, we have to begin a new way of practising our discipline; the 3. Mastrangelo A. Coronavirus: 4,824 Italian healthcare workers are infected.
private sector has to take responsibility for the protection of the health Bretibart.com Mar 23, 2020. Available from: https://www.breitbart.com/
of ALL workers within its supply chain. europe/2020/03/23/coronavirus-4824-italian-healthcare-workers-are-infected/
(accessed 19 Apr 2020).
In this edition of the Journal, three manuscripts provide us with 4. Reuters. World News. Nearly 12,300 Spanish health workers have coronavirus.
approaches to protecting the health of workers (Singh et al., Bouwer Mar 30, 2020. Available from: https://www.reuters.com/article/us-health-coro-
et al. and Fuller). Protecting the health of our health workers, essential navirus-spain-workers-idUSKBN21H1HR (accessed 19 Apr 2020).
5. Doctors, nurses, porters, volunteers: the UK health workers who have died
sector workers, and those tasked with saving our economy, in both from Covid-19. theguardian.com Apr 19, 2020. Available from: https://www.
the formal and informal sectors, becomes the responsibility of every theguardian.com/world/2020/apr/16/doctors-nurses-porters-volunteers-the-
reader of this Journal. Our strategies will evolve as our understanding uk-health-workers-who-have-died-from-covid-19 (accessed Apr 19, 2020).
6. The prevention of miners’ phthisis (notice). Br Med J. 1902; 2:1276. Available
improves but, armed with the basic principles of our respective disci- from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2401978/ (accessed 20
plines in occupational health, we need to bring our collective strength Apr 2020).
41 Vol 26 No 2 March/April 2020 Occupational Health Southern Africa www.occhealth.co.za
Occupational Health Southern Africa www.occhealth.co.za Vol 26 No 2 March/February 2020 5
ISSUES IN OCCUPATIONAL HEALTH NON-PEER REVIEWED
COVID-19 pandemic: workplace readiness to control
and contain the spread of coronavirus
TS Singh1,2, DO Matuka1,2, M Muvhali1, T Duba1
1. National Institute for Occupational Health (NIOH), National Health ABSTRACT
Laboratory Service (NHLS), Johannesburg, South Africa The coronavirus outbreak has been declared a pandemic by the
2. Department of Clinical Microbiology and Infectious Diseases, World Health Organization. It is a huge concern to both public and
School of Pathology, University of the Witwatersrand,
occupational health and is the biggest current threat to the global
Johannesburg, South Africa
economy and financial markets. The aim of this paper is to highlight
the key occupational health challenges based on available literature
Correspondence: Dr Tanusha Singh, National Institute for
and to provide some guidance on preventive measures. A literature
Occupational Health, PO Box 4788, Johannesburg, 2000,
South Africa. e-mail: tanushas@nioh.ac.za search was conducted on PubMed and Google for studies published
from January to March 2020. Google translate was used for articles
Keywords: coronavirus, work-related, occupational infectious disease, in foreign languages. The literature showed that healthcare workers
infection prevention and control, transmission, biorisk assessment are a high-risk group, although any worker is at potential risk. The key
challenges identified relate to labour rights and sick leave, compensa-
How to cite this paper: Singh TS, Matuka DO, Muvhali M, Duba T. tion, impact of quarantine on business continuity, and whether trans-
COVID-19 pandemic: workplace readiness to control and contain the mission is purely through droplets or if airborne transmission plays a
spread of coronavirus. Occup Health Southern Afr. 2020; 26(2):42-45. role. The evidence, although limited, provides guidance for slowing
down and reducing the risk of spread of the virus.
INTRODUCTION be determined.2,7-9 The main route of transmission is person-to-person
The new coronavirus disease (COVID-19) outbreak that has spread through respiratory droplets (coughing, sneezing, talking) and close
across several countries1 and continents has been declared a pandemic contact (proximity of ≤ 1 metre) to an infected person.2,3,10-13 The
by the World Health Organization (WHO). The outbreak has become a expelled infectious droplets may land on objects in the workplace,
global public and occupational health threat, raising several challenges such as tables, desks or equipment. Workers might touch these con-
for managing exposure and work-related disease.2,3 The President of taminated surfaces and then touch their eyes, noses or mouths, which
South Africa, the Honourable Cyril Ramaphosa, declared COVID-19 a are entry points for the virus.7 The reproductive number for the coro-
national disaster and announced strict measures to deal with it, includ- navirus is 2.5 indicating that, on average, an infected individual infects
ing a 21-day lockdown4 which was extended by a further two weeks.5 at least two to three additional people. The risk of transmission from
The purpose of this paper is to raise awareness of COVID-19 readi- asymptomatic individuals, although low, has also been reported.13-15
ness in the workplace and to highlight minimum preventive measures
to control and contain the spread of the virus. Gilbert and colleagues SYMPTOMS ASSOCIATED WITH EXPOSURE TO
determined the capacity of countries to detect and respond to cases SARS-CoV-2
and showed that South Africa, while having a high importation risk, The average incubation period is 5.2 days, ranging from two to 14 days
also had a moderate-to-high capacity to respond to outbreaks.6 Given from exposure to onset of symptoms.9 The early clinical manifestation
the risk, capacity-building training efforts of occupational health of COVID-19 is mild flu-like symptoms which can be followed by severe
professionals must be implemented and cascaded through the labour respiratory distress and pneumonia.12,16 The typical symptoms include
and health systems for readiness at a national level.7 Also needed are fever (> 38 °C), headache, dry cough, shortness of breath, malaise and
strong partnerships across the following six streams: 1) surveillance; sore throat.8,12,16 Approximately 80% of persons present with mild
2) laboratory diagnosis; 3) quarantine, infection prevention and control; to moderate disease (similar to the common flu or cold) and recover.
4) contact tracing and clinical case management; 5) risk assessment Fifteen per cent of cases require hospital admission, and 5% of cases may
and communication; and 6) supply chain management and stockpiles.6 become critically ill and require intensive care unit (ICU) admission; 3%
This literature review was informed by scientific articles published might succumb to the infection.17
from January to March 2020, and publicly available information as of
24 April 2020. Due to the fact that the outbreak is still evolving, there EPIDEMIOLOGY
is limited literature available in the scientific domain. From the onset of the outbreak in December 2019, until 24 April 2020,
there have been 2 833 047 confirmed positive cases and 197 353 deaths
SOURCES AND ROUTE OF TRANSMISSION across 210 countries around the world and two international convey-
Coronaviruses belong to a family of enveloped ribonucleic acid (RNA) ances (the Diamond Princess and MS Zaandam cruise ships). The infection
viruses. The species responsible for COVID-19 is severe acute respira- is increasing daily due to the rapid spread of the virus and strained health
tory syndrome coronavirus 2 (SARS-CoV-2). It is thought that the systems, including lack of diagnostic capacity in many countries. Whilst
transmission chain started from bats to humans. Although it has been the United States of America (USA) has the highest number of reported
suggested that the intermediate host is the pangolin, this remains to cases currently, Spain has been most affected by the outbreak. Spain
42 Vol 26 No 2 March/April 2020 Occupational Health Southern Africa www.occhealth.co.za
ISSUES IN OCCUPATIONAL HEALTH NON-PEER REVIEWED
has more cases and deaths per one million population, exceeding that acquired COVID-10 case has disease arising out of or contracted in the
of China, the epicentre of the disease outbreak.18 In the first two weeks course of work by an employee. The lack of a robust occupational health
of March 2020, the number of cases outside China increased 13-fold, surveillance system impacts on access to accurate data on risk sectors to
causing concern about the spread.7 However, the situation in China enable the implementation of adequate preventive strategies.
improved significantly and the lockdown in Wuhan was lifted in April.
The latter is indicative of the reversal of the exponential increase in OCCUPATIONAL RISK GROUPS
the number of cases through lockdown measures. In South Africa, the Although every person is potentially at risk of exposure to COVID-
infection rate of 49% dropped to 4% by the 4th week of the lockdown.5 19, the risk is higher for workers interacting with persons (within a
Table 1 shows the number of confirmed cases and deaths by country 1–2 m zone) who are potentially infected due to the operations in which
or conveyance, as of 24 April 2020. they work. Examples are:
A notable number of cases reported in China and Singapore have • Healthcare (e.g. paramedics, nurses, doctors, porters, other health
been due to occupational exposure.2,11 At the time of writing this paper, professionals)
there were 4 220 cases and 79 deaths of COVID-19 reported in South • Airline operations (e.g. airline cabin crew, aircraft cleaners, mechanics)
Africa across all provinces, with Gauteng having the highest number. The • Border control (e.g. security officials, and other border officials)
initial cases were imported; however, community transmission is more • Laboratories (e.g. medical technologists, scientists, laboratory assis-
widespread now. Locally, a number of workers have been infected. An tants and researchers)
occupational link has been confirmed in three of 25 cases submitted • Pathology and funeral services (e.g. mortuary attendants, autopsy
to the Compensation Commissioner to date.These include healthcare technicians and funeral directors)
workers, South African Police Service workers, correctional service offi- • Solid waste and wastewater management (e.g. waste pickers, water
cials, South African National Defence Force workers, and mining and treatment plant workers)
energy sector workers. As defined in the Compensation for Occupational The first documented occupational risk group was seafood and wet
Injuries and Diseases (COID) Act (Act No. 130 of 1993), an occupationally market animal workers at a wholesale market in China.12 Initially, in an
Table 1. Number of confirmed SARS-CoV-2 cases and deaths by countries with the highest number of cases,
conveyances and the SADC countries, as at 24 April 20207,18
Total cases/ Total deaths/ Total tests/
Country Total cases New cases* Total deaths Active cases
1M pop┼ 1M pop┼ 1M pop┼
World countries
USA 925 758 38 958 52 217 763 109 2 797 158 15 219
Spain 219 764 6 740 22 524 104 885 4 700 482 19 896
Italy 192 994 3 021 25 969 106 527 3 192 430 27 164
France 159 828 1 645 22 245 94 090 2 449 341 7 103
Germany 154 999 1 870 5 760 39 439 1 850 69 24 738
UK 143 464 5 386 19 506 123 614 2 113 287 9 016
Turkey 104 912 3 122 2 600 80 575 1 244 31 9 844
Iran 88 194 1 168 5 574 16 021 1 050 66 4 761
China 82 816 126 4 632 838 58 3 -
Russia 68 622 5 849 615 62 439 470 4 17 474
Diamond Princess╪ 712 - 13 54 - - -
MS Zaandam╪ 9 - 2 7 - -
Southern African Development Community (SADC) countries
South Africa 4 220 267 79 2 668 71 1 2 569
Angola 25 - 2 17 0.8 0.06 -
Botswana 22 - 1 21 9 0.4 2 136
DRC§ 394 17 25 321 4 0.3 -
eSwatini 36 5 1 25 31 0.9 615
Lesotho - - - - - - -
Madagascar 122 1 - 61 4 - 85
Malawi 33 - 3 26 2 0.2 30
Mauritius 331 - 9 37 260 7 10 516
Mozambique 65 19 - 53 2 - 46
Namibia 16 - - 9 6 - 232
Seychelles 11 - - 5 112 - -
Tanzania 299 15 10 241 5 0.2 -
Zambia 84 8 3 44 5 0.2 141
Zimbabwe 29 1 4 23 2 0.3 367
*no. new cases: 23 April 2020; † total no. cases per 1 million population; ‡ conveyance; § Democratic Republic of Congo
Occupational Health Southern Africa www.occhealth.co.za Vol 26 No 2 March/April 2020 43
ISSUES IN OCCUPATIONAL HEALTH NON-PEER REVIEWED
analysis of the first 425 cases in Wuhan, healthcare workers (HCWs) were hygiene practices2 and practising social distancing, and should not
recognised as the second-highest risk group, after workers at the wet rely only on personal protective equipment (PPE).11 Employers should
market, after 14 HCWs were infected by a patient in a Wuhan hospital therefore make provisions for wash basins, hand sanitisers and PPE (as
cluster.2,12 In addition, HCWs (and their families and friends) experi- informed by the risk assessment), all of which should be readily avail-
ence social stigmatisation from a fearful public as they are accused of able to all employees, visitors and contractors, as determined by policy.
spreading the virus.2 Of those infected, 77.5% worked in general wards, Sick employees presenting with symptoms related to COVID-19 should
17.5% in the emergency department, and 5% in ICUs.2 Hospital-related be encouraged to stay at home. However, should they present at work,
transmission among HCWs could be up to 29%.19 In Singapore, 68% of they should be separated from healthy workers. Ideally, a dedicated area
probable occupationally-acquired COVID-19 cases included workers in should be identified by the employer for temporary isolation of sus-
the tourism, retail and hospitality, transport and security, and construc- pected cases. If an employee is confirmed to have COVID-19, employers
tion industries (Table 2). Other workers at risk are cruise ship crew, e.g. should inform fellow employees of possible workplace exposure, while
waiters and cleaners,16 and workers with co-morbidities (diabetes, renal maintaining confidentiality.21
disease, cardiac disease or chronic lung diseases).8,20 It is recommended that a tiered approach be followed to address
primary, secondary and tertiary prevention measures. Naturally, the risks
RECOMMENDED CONTROL AND CONTAINMENT will be similar for some occupations, hence public and private employers
MEASURES FOR COVID-19 IN WORKPLACES and employees, trade unions and government should collaborate on
Since the onset of the COVID-19 outbreak, prevention and control have preventive strategies for all concerned. The recommended approach is
been major factors in curbing the rapidly-spreading virus. Therefore, cur- illustrated in Figure 1.
rent and credible information on the coronavirus and detailed protocols
on planning and preparedness in the workplace for early detection, CHALLENGES
prompt isolation of contacts and suspected cases, and active surveillance, There are a number of challenges that hamper the containment and
are essential.2,3,7,11,21 Employers should provide a safe and healthy work- control of the COVID-19. Some of these are listed below:
place for employees, contractors and visitors, guided by the company’s • There is a delay between disease development and progression,
occupational health and safety policy. The COVID-19 outbreak presents diagnosis and quarantine.12
new risks to organisations and, thus, employers need to review their • Healthcare systems are strained, surveillance is inadequate, labora-
biorisk assessment strategies and compile risk management matrices for tory capacity is limited, public health human resources are scarce,
both health and safety, and business risks. Information and understand- and there are limited financial means to address these factors.
ing of the likelihood and consequences of COVID-19 are needed to help • Multiple health challenges face the African continent, such as
refine risk assessments which will inform mitigation strategies within rapid population growth, increased movement of people, existing
the work environment. This should include business continuity plans to endemic diseases (eg. human immunodeficiency virus (HIV), tuber-
cushion any economic or job losses. The implementation of necessary culosis, malaria), emerging and re-emerging diseases, and increasing
control measures should be tailor-made for various sectors, and risks incidence of non-communicable diseases.6
should be communicated to all employees.8 Restrictions on employee • The main symptoms (fever, cough and shortness at breath) may
travel (e.g. essential or emergency work) and monitoring thereof should not all be discernible at early stages of the disease, therefore a high
be part of the mitigation plan. Occupational settings should consider level of clinical suspicion should be maintained to prevent disease
having dedicated response teams that should remain in consultation transmission.16
with public health authorities for the early recognition and reporting • There is no treatment, vaccine or pre-existing immunity to the virus.
of suspected COVID-19 cases. • Screening efforts may miss asymptomatic individuals who could
All employees should be educated and alerted about the risk of transmit the virus.
COVID-19. Workers can be protected by good hand and respiratory • A possible airborne mode of transmission is likely; however, insuf-
ficient scientific evidence is available.
• Shortages of outbreak-related resources (e.g. PPE supply and/or uni-
Table 2. Job types of 17 of the 25 probable
versal masking) pose a challenge to workplaces globally, particularly
occupationally-related COVID-19 cases in Singapore
(4–11 February 2020)2 in healthcare. Thus, interim measures for protecting workers must
be put in place based on priority, i.e. imminent risk in the workplace,
Job type No. cases and available financial resources.
Retail staff selling complimentary health products 4 • Lack of awareness leads to individuals presenting to ear, nose and
Domestic worker of one of the retail staff cases above 1 throat (ENT) departments, thus overloading and increasing risk expo-
Tour guide who led tour group 1 sure to HCWs.
Jewellery store worker 1 • Contact tracing may miss certain individuals as the person under
Multinational company staff attending international business 3 investigation (PUI) may not recall all contacts, or fear reporting them.
meeting • The biological agent classification for SARS-CoV-2 definition in the
Taxi driver 1 current regulation does not match the actual disease presentation.
Private hire car driver 1 • Immune susceptibility varies among workers and, therefore, the
Sentosa Resort employee 1
risk profiles are different. In addition, workers do not disclose their
underlying conditions, thus making it difficult to prioritise them.
Security officer who served quarantine order to two persons 1
• Compliance to lockdown measures is problematic in some
Casino worker 1
areas and occupational sectors (e.g. public transport and
Workers at construction site 2
informal trade).
44 Vol 26 No 2 March/April 2020 Occupational Health Southern Africa www.occhealth.co.za
ISSUES IN OCCUPATIONAL HEALTH NON-PEER REVIEWED
Figure 1. Recommended business approach to workplace readiness for COVID-19
CONCLUSION message-by-president-cyril-ramaphosa-on-covid-19-pandemic-thursday-9-april-2020/
COVID-19 is now considered a global pandemic and the virus is spreading (accessed 10 Apr 2020).
6. Nkengasong JN, Mankoula W. Looming threat of COVID-19 infection in Africa: act col-
at an unprecedented rate. Given the challenges highlighted in this paper, lectively, and fast. Lancet. 2020; 395(10227):841-842.
it is crucial that scarce resources be appropriately allocated to prepare 7. World Health Organization. Coronavirus situation reports; 2020. Available from: https://
and respond effectively in a unified and co-ordinated manner across www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed
12 Apr 2020).
workplaces, countries and continents. Technical operations and testing 8. O’Keefe LC. Middle East Respiratory Syndrome coronavirus. Workplace Health Saf. 2016;
must be impeccable and quality-assured, and collaboration and com- 64(5):184-186.
munication needs to be strengthened. The actions needed in the occupa- 9. Sun P, Lu X, Xu C, Sun W, Pan B. Understanding of COVID-19 based on current evidence. J
Med Virol. 2020; 1-4. doi: 10.1002/jmv.25722.
tional health arena are fundamental and will contribute to the prevention 10. Kapata N, Ihekweazu C, Ntoumi F, Raji T, Chanda-Kapata P, Mukonka V, et al. Is Africa
of a social, health and economic tragedy. It is the responsibility of the prepared for tackling the COVID-19 (SARS-CoV-2) epidemic? Lessons from past outbreaks,
employer to implement a preparedness plan for containing and control- ongoing pan-African public health efforts, and implications for the future. Int J Infect Dis.
2020; 93:233-236.
ling potential exposures, as well as to review its business continuity plans, 11. Peng PW, Ho PL, Hota SS. Outbreak of a new coronavirus: what anaesthetists should know.
in order to maintain a healthy, safe and sustainable workplace. Br J Anaesth. 2020; doi: 10.1016/j.bja.2020.02.008.
12. Ralph R, Lew J, Zeng T, Francis M, Xue B, Roux M, et al. 2019-nCoV (Wuhan virus), a novel
Coronavirus: human-to-human transmission, travel-related cases, and vaccine readiness. J
DECLARATION Infect Dev Ctries. 2020; 14(1):3-17.
The authors declare that this is their own work; all the sources used in 13. Rocklöv J, Sjödin H, Wilder-Smith A. COVID-19 outbreak on the Diamond Princess cruise
this paper have been duly acknowledged and there are no conflicts of ship: estimating the epidemic potential and effectiveness of public health counter measures
J Travel Med; 28 Feb 2020. Available from: https://doi.org/10.1093/jtm/taaa030 (accessed
interest. 12 Apr 2020).
14. Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, et al. Transmission
AUTHOR CONTRIBUTIONS of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med. 2020;
382(10):970-971.
Conception and design of the paper: TSS, DOM 15. Zhang S, Diao M, Yu W, Pei L, Lin Z, Chen D. Estimation of the reproductive number of
Drafting of the paper: all authors novel coronavirus (COVID-19) and the probable outbreak size on the Diamond Princess cruise
Critical revision of the paper: TSS ship: a data-driven analysis. Int J Infect Dis. 2020; 93:201-204.
16. Arashiro T, Furukawa K, Nakamura A. COVID-19 in 2 persons with mild upper respiratory
symptoms on a cruise ship, Japan. Emerg Infect Dis. 2020; 26(6), doi: 10.3201/eid2606.200452.
REFERENCES 17. National Institute for Comminicable Diseases. How to manage the threat of COVID in
1. Joob B, Wiwanitkit V. COVID-19 in medical personnel: observation from Thailand. J Hosp your workplace or institution. National Institute for Communicable Diseases. Johannesburg:
Infect. 2020; 27 Feb. doi: 10.1016/j.jhin.2020.02.016. NICD; 2020. Available from: https://www.nicd.ac.za/how-to-minimize-risk-of-covid-19-in-the-
2. Koh D. Occupational risks for COVID-19. Occup Med (Lond). 2020; 70(1):3-5. workplace/ (accessed 12 Apr 2020).
3. Spina S, Marrazzo F, Migliari M, Stucchi R, Sforza A, Fumagalli R. The response of 18. Worldometer. Coronoavirus. Available from: https://www.worldometers.info/coronavirus/
Milan’s Emergency Medical System to the COVID-19 outbreak in Italy. Lancet. 2020; (accessed 12 Apr 2020).
395(10227):E49-E50. 19. Chen X, Tian J, Li G, Li G. Initiation of a new infection control system for the COVID-19
4. News24. Ramaphosa declares national disaster, announces strict measures to deal outbreak. Lancet Infect Dis. 2020; 20(4):397-398.
with Covid-19 crisis. https://www.news24.com/SouthAfrica/News/state-of-war- 20. Sohrabi C, Alsafi Z, O’Neill N, Khan M, Kerwan A, Al-Jabir A, et al. World Health Organization
ramaphosa-takes-command-of-covid-19-response-as-national-disaster-is- declares Global Emergency: a review of the 2019 Novel Coronavirus (COVID-19). Int J Surg.
declared-20200316 (accessed 12 Apr 2020). 2020; 76:71-76.
5. Republic of South Africa. Department of Health. Message by President Cyril 21. Cheng VC, Wong SC, To KK, Ho PL, Yuen KY. Preparedness and proactive infection control
Ramaphosa on COVID-19 pandemic Thursday, 9 April 2020. Issued by the Presidency measures against the emerging Wuhan coronavirus pneumonia in China. J Hosp Infect.
of the Republic of South Africa. Available from: https://sacoronavirus.co.za/2020/04/09/ 2020; 104(3):245-255.
Occupational Health Southern Africa www.occhealth.co.za Vol 26 No 2 March/April 2020 45
ISSUES IN OCCUPATIONAL HEALTH NON-PEER REVIEWED
South Africa’s industry preparedness to control
COVID-19 transmission
D Brouwer1, V Govender1, M Hermanus2
1. School of Public Health, Faculty of Health Sciences, University of the ABSTRACT
Witwatersrand, Johannesburg, South Africa South African industry needs to prepare for a long-term battle to control
2. Wits Mining Institute, University of the Witwatersrand, Johannesburg, transmission of the 2019 novel coronavirus disease (COVID-19), guided
South Africa by occupational health risk assessment and management. Knowledge
of the exposure pathways is key to developing sustainable and effec-
Correspondence: Prof. Derk Brouwer, School of Public Health, Wits
tive control strategies. A starting point is the identification of exposure
Education Campus, Parktown, 2193. e-mail: derk.brouwer@wits.ac.za
scenarios with enhanced transmission risk and high-risk persons who are
predisposed to greater severity of COVID-19 illness. Workplace control
Keywords: exposure pathway, risk management, workplace controls,
occupational health options, according to the well-known hierarchy of controls, should
be implemented. This will require that employers, together with their
How to cite this paper: Brouwer D, Govender V, Hermanus M. South multidisciplinary teams and stakeholders, be decisive, weigh up the risks
Africa’s industry preparedness to control COVID-19 transmission. Occup in context, and act in a manner commensurate with the magnitude of
Health Southern Afr. 2020; 26(2):46-50. this threat.
INTRODUCTION of the measures; however, there are still many unknowns. Anticipating
On 18 March 2020, regulations in terms of the Disaster Management a post-lockdown situation in South Africa, industry should prepare for
Act were pronounced; subsequently, on 26 March 2020, South Africa continuation of preventive measures for ‘flattening the curve’ of the
went into a nationwide lockdown to prevent a total collapse of the expected follow-up infection waves, when operations are restarted
healthcare system.1 On 17 March 2020, the Department of Employment or upscaled. In this paper, we discuss the transmission pathways
and Labour (DEL) published a COVID-19 planning guidance for in occupational settings in more general terms and explore the
employers2 and, on 26 March 2020, the Department of Mineral preparedness of South African industry to comply with the general
Resources and Energy (DMRE) issued guiding principles on prevention recommendations regarding transmission control.
and management of COVID-19 in the South African mining industry.3
On 20 March 2020, the DEL was also quick to respond with a notice THE TRANSMISSION PATHWAYS
on the compensation for occupationally-acquired novel coronavirus The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (the
disease (COVID-19), which covers occupationally-acquired COVID-19 virus that causes COVID-19) is, like other enveloped viruses, a protein
cases resulting from single or multiple exposures to confirmed cases of molecule (ribonucleic acid (RNA)) covered by a protective layer of lipids
COVID-19 in the workplace, or after official trips to high-risk countries.4 (fat), which, when absorbed by the cells of the ocular, nasal or buccal
The legislation governing non-mining industry workplaces in relation mucosa, changes their genetic code (mutation) and converts them
to COVID-19 is the Occupational Health and Safety (OHS) Act (Act No. into aggressor and multiplier cells.9 Virus particles in the air and on
85 of 1993), as amended, read with the Hazardous Biological Agents fomites (surfaces and substrates that are likely to carry infection) are
Regulations, Section 8 (1) of the (OHS) Act.5 Specifically, Section 8 (2)(b) exposed to a range of environmental conditions that influence their
requires steps such as may be reasonably practicable to eliminate or persistence. Relative humidity, fomite material and air temperature
mitigate any hazard or potential hazard before resorting to personal can greatly impact enveloped virus inactivation rates.
protective equipment (PPE). However, in the case of COVID-19, a In the publicly available information, e.g. the World Health
combination of controls is required, although the main principle is Organization (WHO) scientific brief,10 the transmission pathways are,
to follow the hierarchy of controls.2 The guidance is focused on the in general, well described, as well as standard precautionary measures
broader group – healthcare workers/health professionals. to reduce the probability of transmission. However, there are still many
The health and safety of miners is governed by the Mine Health unknowns, especially regarding COVID-19 virus viability, both in air and
and Safety Act (Act No. 29 of 1996)6 and the mining industry has on surfaces under different environmental conditions.
well-organised and well-functioning occupational health and medical The pathway resulting in intake by inhalation by a receptor-
facilities. Guided by the Minerals Industry Risk Management Process7 person is subdivided into the so-called direct and indirect routes9-13
and adopting the Minerals Council’s COVID-19 Ten Point Plan of (Figure 1).
Action,8 it is well positioned to develop customised COVID-19 prevention The direct route is determined by the ability to inhale droplets emitted
strategies for its workforce, extending to the peri-mining communities. into the air by the infected (index) person. The droplets consist of a
In addition to the healthcare sector, the energy (including relevant protein nucleus surrounded by liquid (mainly water). Both speech by
mining activities) and food sectors have been designated as essential the index person and, for example, coughing/sneezing, will generate
services, thus putting pressure on these sectors to comply with high droplets. However, the droplets differ, regarding size, composition and
standards of hygiene, social distancing and use of effective PPE. the number of infectious quanta per droplet. Expiration characteristics
The global spread of the COVID-19 and measures to control the of speech and sneezing/coughing also affect the number of droplets
pandemic are developing rapidly, as is our knowledge on the effectiveness generated, as well as their exhalation speed and the frequency and
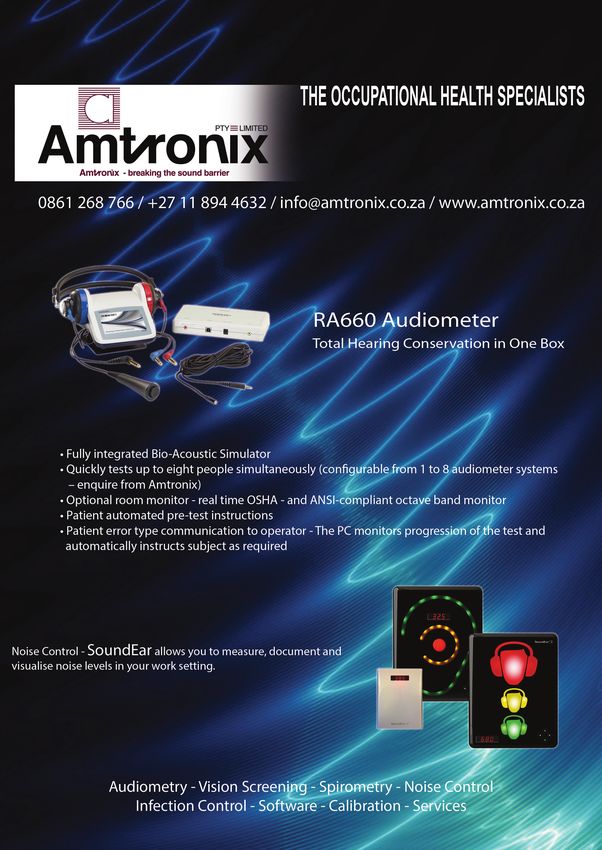
46 Vol 26 No 2 March/April 2020 Occupational Health Southern Africa www.occhealth.co.zaISSUES IN OCCUPATIONAL HEALTH NON-PEER REVIEWED Figure 1. Illustration of different transmission pathways. Small droplets (< 5 μm), sometimes called aerosols, are responsible for the short-range airborne route, long-range airborne route, and indirect contact route; large droplets are responsible for the direct spray route and indirect contact route. The balloons illustrate the determinants of the processes. Figure adapted and modified from Wei and Li, 201611 duration of the droplet generation. Normal breathing generates The indirect route is the fomite route. Droplets may have deposited droplets < 1 µm in size, whereas coughing can release droplets up to on surfaces and substrates where the virus may survive for a while. 100 µm. As a rule of thumb, at very close distances (up to 150–200 cm), Hand-contact with these surfaces (fomites), followed by hand-mouth/ even larger droplets (called aerosols) may reach the breathing zone nose mucous contact, is considered an important transmission route. of a receptor. Within this zone (between index and receptor persons), Specific information for the COVID-19 virus is presently scarce16 but droplets are greatly affected by environmental conditions such as rela- is expected to be quite similar to other coronaviruses.18 Survival time tive humidity and temperature which determine, in combination with shows huge variation, from a few hours on porous surfaces, e.g. card- the initial droplet size, their time of residence in the air. Smaller droplets board, to three days on smooth, non-porous surfaces, e.g. stainless of up to 5–10 µm, however, remain airborne for a longer period. With steel and plastic.16,18 However, the viability of the virus, indicated by increasing index-receptor distance, the fate of the droplets (especially the virus titre, rapidly declines, as shown by the reported half-lives their time of residence in air) is affected by relative humidity and of 5.6 hours on stainless steel and 6.8 hours on plastic.16 Usually, the temperature. In general, low relative humidity and high temperature survival time on the skin is much shorter compared to that on non- will enhance the evaporation of the water part of the aerosol, and the animate surfaces. The transfer efficacy of pathogens from surface to size of the aerosol will decrease rapidly to approximately 30% of its hand, and from hand to the perioral area or the nose, is highly variable original size. These aerosols will be captured by air movement, may but could be up to 30% or more.17-19 Observations from other studies remain airborne for a long period, and may be inhaled by receptor- show that the frequency of hand-to-face contact is eight times per person(s) much further away from the index-person. Especially for hour, on average.22,23 indoor environments, this ‘long-range airborne transport’ might be (or become) an important pathway. Recent experimental studies OCCUPATIONAL EXPOSURE SCENARIOS provide evidence that the aerosols containing COVID-19 virus have There is consensus that high exposure risks are experienced by caring a half-life of approximately 1.2 hours, and can be detected for up to and protective service workers, e.g. healthcare workers, healthcare or three hours,16 indicating that this route of transmission cannot be laboratory personnel, medical transport workers, and morgue workers excluded.13-15 However, currently, the WHO states that, only in specific (broadly, those who may have contact with patients, patients’ tissues, clinical circumstances and settings in which procedures that generate etc., including faecal shedding).2,15,24,25 Beyond these workers, there aerosols are performed, may airborne transmission be possible, and is a wide range of service economy workers who have frequent and that the detection of COVID-19 RNA in environmental samples, based close interaction with many people over the course of a shift, and who on polymerase chain reaction (PCR)-based assays, is not indicative of may therefore be at risk of respiratory infections like COVID-19. Shop viable viruses that could be transmissible. Thus, the current focus is workers in high-volume retail settings, taxi and bus drivers, cleaners, very much on the ‘droplet’ route. teachers, bank workers, hospitality and penitentiary workers, etc. Occupational Health Southern Africa www.occhealth.co.za Vol 26 No 2 March/April 2020 47
ISSUES IN OCCUPATIONAL HEALTH NON-PEER REVIEWED
are among the many service-sector employees who are at risk. Many be governed by a workplace COVID-19 policy, and should include
of these workers will have either physical contact with the public or body temperature screening at points of entry as well as measures to
indirect contact through exchange of goods and money.26 In addi- reduce the emission of exhaled droplets, i.e. behavioural practices such
tion, all high-population-density work environments, such as labour as ‘controlled-sneezing’,33 and wearing of face masks.30-32 The latter
centres, consulting rooms, points of entry for personnel, etc. can be has been proven to be effective in healthcare settings where infected
considered as potential ‘hot spots’ for transmission. It is unknown, patients wore masks. However, it is plausible that even home-made
however, if specific workplace conditions, such as dust exposure, high cloth face masks will reduce the emission of droplets into the air to
air velocities, and hot and humid environments, may modify COVID-19 a certain extent. Definitely, the larger droplets will be captured, and
transmission. For example, similar to nanoparticles, the smaller droplets the swelling of the cotton fibres when moisturised may prevent even
might be scavenged by, or adhere to, dust particles and be transported smaller droplets escaping.
through the air over long distances.27 However, it is also likely that Regarding the droplet transmission pathway, structural measures
adherence to dust will decrease the survival time of the virus. such as simple (face) screens and barriers used in some customer-facing
Several sectors have been designated as ‘essential services’ during roles, including those of taxi/bus drivers and banking staff, might offer
the lockdown, including medical care services, supply chains (e.g. energy some degree of protection from COVID-19, compared to the more open
and food), retail workers and public transport.28 Thus, these sectors interactive style of work that teachers or general shop staff adopt. More
should remain in full operation; however, in many instances it will be a drastic measures would be, for example, the transition to self-scanning
challenge to comply with the precautionary measures recommended of purchased goods, and replacement of traditional door handles with
to the general public, such as keeping a ‘social or physical distancing’ of elbow-operating systems or automatic doors. Adequate room ventila-
1.5 to 2 metres, and appropriate sanitation. Clearly, the currently allowed tion in combination with reduced occupancy of rooms are key factors to
loading capacity of 70% for minibus taxis,29 and the transfer of money, reduce the long-range transport of aerosols and shorten the associated
increase the potential to violate these general rules.26 Specifically, for the transmission pathway, as demonstrated in tuberculosis transmission
energy-supply chain, the innate nature of mining operations lends itself research.20,37 Furthermore, engineering controls to reduce the emis-
to dense occupancy in living quarters, while commuting to workplaces, sion of dust should be extended as it is hypothesised that concurrent
in change- and lamp-rooms, and in travelling to the stopes, whether it exposure to dust may affect exposure to COVID-19.
be in a vehicle or cage, or on foot. In addition, specific mining processes Adequate personal hygiene, including handwashing, will require that
require teams whose members work in close proximity to each other, workers are well instructed and facilitated, and should be paired with
providing additional COVID-19 transmission points. However, surface cleaning procedures to provide frequent and adequate cleaning of sur-
mining operations and mechanised mining provide ample opportunities faces, especially those that are frequently touched by different persons.38
to enforce safe hygiene practices. Personal protective equipment which includes gloves, goggles, face
Food production involves one or more of the following processes: shields, face masks, aprons, overalls, hair and shoe covers, and respira-
continuous or semi-continuous production, batch production, or craft tory protection, will only be effective if workers are adequately trained
or hand finishing. During production and transport to market, many to use protective clothing and equipment, which includes instructions
people come into contact with each other and the food product, e.g. on how to correctly don, use/wear and doff it.
during harvesting, sorting and packing.30 Although the Department The effectiveness of the facemask type of respirator, or the so-
of Health (DoH) COVID-19 hygiene protocol, which emphasises hand- called disposable filtering facepiece (FFP), is very much determined
washing and hygiene measures, would also apply to the food supply by the ‘fit’, i.e. the presence or absence of facial leakages, rather than
sector, circumstances encountered in the sector are not regulated. For the filtration efficacy.39 In addition, it is quite often forgotten that
this reason, lessons can be learned from the United Kingdom where the ‘disposable’ implies replacement and not reuse. It will be interest-
COVID-19 epidemic is ahead of South Africa. Here, the trade unions in ing to determine whether adherence of viruses to dust particles will
the food sector are not convinced that the Food Standards Authority- result in a Trojan horse effect if the particle size is close to the so-called
issued guidelines to food manufacturers, aimed at keeping workers most-penetrating particle sizes, which are in the range of 40 to 300 nm,
safe and preventing person-to-person transmission, are adequate, and depending on the filter material.40 As research indicates, appropri-
have called for a ‘mandatory imposition’ by government of a 2 m social ate donning practices very much determine the fit of respirators,41
distancing rule.31 and inappropriate doffing of respirators and gloves enhances cross-
contamination.15,42 Thus, the use of masks, i.e. non-medical masks for
WORKPLACE EXPOSURE CONTROL OPTIONS non-healthcare workers and the general public, must be accompanied
With COVID-19, it may not be possible to eliminate the hazard. The most by mask hygiene, and awareness and education.
effective exposure control measures are associated with prevention of
transmission from infected persons and asymptomatic carriers; thus, the OCCUPATIONAL HEALTH PREVENTION AND
exposure pathways and the hierarchy of controls for COVID-19 are vital, SURVEILLANCE
i.e. engineering controls, administrative controls, safe work practices, The general principles that play a major role in keeping workers healthy
behaviour risk management (a type of administrative control), and PPE. and safe, i.e. IDENTIFY, PREVENT, TRACE, TEST, TREAT, through early diag-
Thus, measures, at the source, to detect early infected and/or potentially nosis, early treatment, and rehabilitation will also apply to the control
infected persons, are key. of COVID-19, whilst maintaining workers’ dignity.
According to the National Institute for Communicable Diseases
(NICD) case definition, persons under investigation (PUI) who should Persons under investigation
be tested for COVID-19 are those presenting with acute respiratory COVID-19 symptom and fever screening at work and at home, to identify
illness or a cough, sore throat, shortness of breath, fever ≥ 38 °C, or a suspected cases and contacts early, should be given priority. Contacts
history of fever.32 Initiatives to detect PUIs in workplace settings should should be actively and promptly traced, tested and treated. Infected
48 Vol 26 No 2 March/April 2020 Occupational Health Southern Africa www.occhealth.co.zaISSUES IN OCCUPATIONAL HEALTH NON-PEER REVIEWED
workers should be placed in isolation immediately. Contacts and work- lockdown, post COVID-19 illness or post COVID-19 quarantine must
ers with flu-like symptoms should remain self-quarantined at home or be developed and communicated to the workforce to educate and reas-
in specific quarantine accommodation. It may become necessary for sure workers. Medical incapacity policies should be reviewed and judi-
employers to engage with local authorities to access specific COVID-19 ciously applied in suspected, infected and recovering COVID-19 cases.
quarantine facilities for their employees who are unable to self-isolate
in their usual accommodations. Risk communications
The information must target specific behaviour modifications that
Identification of persons with high-risk profiles prevent COVID-19. Existing peer-educator platforms, and health
As part of the risk management process, high-risk COVID-19 categories and safety committees, should be used effectively to educate and
amongst the workforce should be actively identified and appropriately raise awareness on prevention of contracting and prevention of
managed as they are predisposed to experiencing greater severity of transmission of COVID-19. General health promotion materials,
COVID-19 illness. According to the Centres for Disease Control (CDC), illustrating good cough hygiene, hand washing, respiratory etiquette,
older adults and people of any age who have serious underlying medical COVID-19 symptoms, quarantine/isolation methods, and informa-
conditions might be at higher risk for severe illness from COVID-19.43 tion on available healthcare facilities, must be freely available, using
Thus, employees with the following conditions should be identified multiple communication channels.
and actively monitored:
• pre-existing lung diseases such as asthma, obstructive airways Other support mechanisms
diseases, active/chronic/past tuberculosis, and pneumoconiosis, e.g. Employers would do well to engage with the service providers of
silicosis in mine workers; their employee assistance programmes to provide advice, stress man-
• comorbid risk factors and pre-existing diseases such as cardiorespi- agement and psychosocial support to their workers. A COVID-19 hotline,
ratory disease, diabetes, hypertension, auto-immune disorders and managed by the company’s occupational health staff, could assist with
cancers; triaging workers. This would take a substantial burden off the public
• human immunodeficiency virus (HIV)-infected employees with low health systems and hotlines managed by the NICD and other agencies.
cluster of differentiation 4 (CD4) cell counts or poorly managed HIV;
and, CONCLUSION
• smokers, who are at higher risk for more severe COVID-19. There is no doubt that the South African workforce is vulnerable to
The South African population has high tuberculosis and HIV rates. COVID-19. In the 1990s, when the mining sector was most impacted
According to the WHO, tuberculosis patients who have lung damage by HIV and tuberculosis, without life-saving antiretroviral drugs, it had
from past episodes of tuberculosis or chronic obstructive pulmonary to respond in a most decisive and unprecedented manner by applying
disease may suffer from more severe illness if they are infected with multipronged, multidisciplinary and novel approaches to tackle the
COVID-19.44 There is thus a strong case for concurrent testing for both extraordinary burden of disease. Other sectors should take cognisance
conditions in these individuals as the COVID-19 clinical picture could of the lessons learned and not reinvent the wheel. Leading practices
easily mimic that of tuberculosis. The WHO also emphasises that, while that worked to contain the HIV and tuberculosis epidemics should be
untreated HIV is an important risk factor for progression to tuberculosis adopted and enhanced to contain and mitigate the impact of COVID-19
or for poor outcomes in tuberculosis patients, the influence of HIV on on the South African economy. For the various exposure scenarios, it is
the prognosis of COVID-19 patients remains unclear. This means that necessary to determine the most effective measure to limit COVID-19
employers should take “additional precautions for all people with transmission. Exposure science and occupational hygiene are impor-
advanced HIV or poorly controlled HIV”.44 With regard to smoking and tant fields of expertise to assist in exposure-control decision making.
COVID-19, a systematic review noted that, despite the limited available There is no time for complacency. Employers, together with their
data, evidence that smoking is associated with adverse outcomes of multidisciplinary teams and stakeholders, need to be decisive, weigh
COVID-19 is increasing.45 up the risks in context, and act in a manner commensurate with
These high-risk workers and those at higher risk for severe illness the magnitude of this threat. The COVID-19 workplace policies should
should be fast-tracked to receive prophylaxis for the seasonal influenza not only be aligned to the prompt governmental response and progres-
(‘flu vaccine), pneumococcal pneumonia (pneumococcal vaccine) and sive legislative frameworks, but, as outlined in this paper, go beyond
tuberculosis (isoniazid preventive therapy), as advised by their doctors. this and be reflective of a relentless and tenacious fight against the
impact of COVID-19.
Customised COVID-19 workplace policies and procedures
COVID-19 policies must be integrated into strategic risk management DECLARATION
frameworks and core business practices and be endorsed by top The authors declare that this is their own work; all the sources used in
leadership and employees alike. In addition, employers should be acutely this paper have been duly acknowledged and there are no conflicts
aware of the local community COVID-19 epidemiological patterns, and of interest.
plan for community outbreak intervention strategies to provide support
to communities. AUTHOR CONTRIBUTIONS
Workplace policies must be clear about who is entitled to sick Conception and design of the paper: DB
leave or quarantine sick leave, and explicit about how this should be Drafting of the paper: all authors
implemented. Multidisciplinary teams, comprising human resources Critical revision of the paper: all authors
practitioners, labour representatives and occupational medicine
practitioners, should prepare for determining how PUIs will be Note: this paper is based on information that was available as
reintegrated into the workplace. Policies and procedures for post of 10 April 2020.
Occupational Health Southern Africa www.occhealth.co.za Vol 26 No 2 March/April 2020 49You can also read