Oncologic Reliability of Nipple-sparing Mastectomy for Selected Patients with Breast Cancer
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

in vivo 27: 387-394 (2013)
Oncologic Reliability of Nipple-sparing Mastectomy
for Selected Patients with Breast Cancer
ANTONIO RULLI1,3, DANIELA CARACAPPA1, FRANCESCO BARBERINI1, CARLO BOSELLI1,
ROBERTO CIROCCHI2, ELISA CASTELLANI1, GIUSEPPE NOYA1 and PIERO COVARELLI1
1General and Oncologic Surgery Unit, Department of Surgical, Radiological and
Odontostomatological Sciences, University of Perugia, Perugia, Italy;
2General Surgery Unit, University of Perugia, St. Maria Hospital, Terni, Italy
3Breast Unit, Department of Surgical, Radiological and Odontostomatological Sciences,
University of Perugia, Perugia, Italy
Abstract. Background: Nipple sparing mastectomy (NSM) oncologically safe technique that, in the respect of inclusion
is the current surgical alternative to conventional techniques, criteria may be performed in any patient with indication to
when mastectomy is required. This less invasive procedure mastectomy. A careful selection of patients by a
safeguards the integrity of the nipple areola complex (NAC), multidisciplinary team according to strict criteria is the key in
whose removal is recognized as a factor that exacerbates the determining feasibility as well as oncological safety and
patient’s feeling of mutilation, however ensuring oncological should lead the general acceptance and widespread use of
radicality for women with breast cancer. Patients and Methods: such surgical technique.
From January 2003 to January 2011, 77 patients underwent
Nipple Sparing Mastectomy (NSM). Patients were carefully Many patients undergoing mastectomy for breast cancer are
selected according to specific criteria. When requested, documented and informed about possible resective and
postoperative radiotherapy on the residual glandular tissue was reconstructive surgical strategies. Most of them at the
performed within 6 months of surgery. Patients were on close preoperative interview consciously discuss with the surgeon
clinical and instrumental follow-up every 4 months for 2 years about risks and benefits of the different types of
and every 6 months for the remaining 3 years. Results: Of the interventions. When mastectomy is required, patients
77 patients who underwent NSM, 10 suffering from bilateral willingly accept nipple-sparing mastectomy (NSM) which
cancer were subjected to bilateral procedure, for a total of 87 represents a radical procedure and together safeguards the
performed procedures. Furthermore, in the same group, 13 integrity of the nipple areola complex (NAC), thus reducing
NSMs were carried out for preventive purposes. The average the sense of mutilation linked to surgery (1). The loss of the
diameter of resected tumors was 13.5 mm, with a range of 2 to NAC is only fully perceived by a patient some weeks after
25 mm. During the follow-up (range 23-115 months, mean surgery, once the primary condition, breast cancer, has been
50.33 months) 2 locoregional recurrences in the NAC were surgically corrected (2-5).
observed, identified through instrumental check, and Data on the oncological reliability and feasibility of NSM
surgically treated by NAC removal after 33 and 37 months have been analyzed in many studies (6-11), several authors
respectively. Conclusion: According to the litterature data and have assessed the risk of subareolar recurrence after this
confirmed by our experience, we consider NSM as an surgical technique in relation to tumor size, its distance from
the nipple, nodal status and effectiveness of radiotherapy (3,
12-14). These studies revealed that such technique can be
This article is freely accessible online. adopted in carefully selected patients with stage I/II tumors at
a suitable distance from the NAC. When the subareolar
Correspondence to: Professor Antonio Rulli, General and Oncologic glandular tissue is spared, in order to ensure the viability of the
Surgery Unit, Department of Surgical, Radiological and NAC, the use of tangential breast irradiation or intraoperative
Odontostomatological Sciences, University of Perugia, S. Maria della
radiotherapy (IORT), exclusively targeted to the NAC, has been
Misericordia Hospital, S. Andrea delle Fratte, 06121, Perugia, Italy.
Tel: +39 0755783537, Fax: +39 0755783258, e-mail: rulli@unipg.it
proven to reduce relapse risk (15). Our aim was on the one
hand to assess the local recurrence rate in patients submitted to
Key Words: Breast cancer, nipple-sparing mastectomy, reconstructive curative NSM, and on the other to analyze the possible
surgery. complications of this less invasive procedure.
0258-851X/2013 $2.00+.40 387
in vivo 27: 387-394 (2013)
Table I. Inclusion and Exclusion criteria. Table II. Patient and tumor characteristics.
Inclusion criteria No. %
- Informed consent Patients 77
- Age between 18 and 75 years
- Diagnosis of ductal in situ carcinoma or infiltrating ductal carcinoma Age (years)
with a tumor diameter ≤2.5 cm Mean 50
- Distance of the tumor from the nipple ≥2.5 cm Range 32-74
- Cancer or microcalcifications not localized in the central field ≥50 Years 32 42%
- No blood secretions or other NAC disturbances ≤50 Years 45 58%
- Absence of skin involvement Histotype
- Indication to mastectomy for multifocal or diffuse microcalcifications IDC 47 63.51%
- Negative intraoperative assessment of NAC-bottom DCIS 24 32.43%
TC 1 1.35%
Exclusion criteria MC 1 1.35%
Other 1 1.35%
- Tumor or microcalcifications localized in the central quadrant or in T (Size: average 13.29 mm, range 2-25 mm)
the retroareolar region T1a 13 17.6%
- Blood secretions or other NAC alterations T1b 23 31%
- Positive intraoperative assesment of NAC-bottom T1c 24 32.4%
- Inflammatory carcinoma T2 14 19%
- Paget’s disease of the nipple Nodal status
- T ≥ 2.5 cm 0 59 79.8%
- Distance of the tumor from the nipple 3 7 9.4%
Grading
G1 8 16.7%
G2 34 70.8%
G3 6 12.5%
Estrogen receptor (ER)
The removal of the nipple, which is recognized as an Positive 66 89.2%
attribute of femininity and identity of the breast (15), is Negative 8 10.8%
experienced by patients as mutilation (16), thus stimulating Progestin receptor (PR)
surgeons to perform less invasive operations, such as NSM, Positive 62 83.8%
Negative 12 16.2%
with the purpose of preserving physical and psychological
Ki67
integrity and ensuring oncological radicality for women with 20 33 44.6%
ERBB2
Patients and Methods Overespressed 59 79.7%
Not overespressed 15 20.3%
From 1 January 2003 to 1 January 2011, at the Breast Unit of S.
IDC: Invasive carcinoma; DCIS: in situ carcinoma; TC: infiltrating
Maria della Misericordia Hospital Perugia, 87 patients underwent tubular carcinoma; MC: mucinous carcinoma.
standard NSM, which achieves, irrespective of the type of incision,
subcutaneous mastectomy with preservation of the NAC and
immediate reconstruction with tissue expander (Figure 1). Patients
were selected as a result of a multidisciplinary meeting attended by
oncological surgeons, plastic surgeons, radiotherapists, medical Patients underwent close clinical and instrumental follow-up
oncologists and pathologists, according to the parameters shown in every four months for two years and every six months for the
Table I. subsequent three years.
All patients underwent a follow-up mammogram 30 days after The median age was 50 years (range 32 to 74 years), 58% of the
surgery and were not submitted to radiotherapy after confirmation of patients were younger than 50 years. The average diameter of
complete removal of retroareolar glandula tissue, while patients in tumors was 13.5 mm, with a range of 2 to 25 mm (Table II). We
whom subareolar tissue was preserved in order to ensure NAC performed a total of 77 NSMs on 87 patients, since 10 were
viability (however, no more than 5 mm thick) underwent assessment suffering from bilateral cancer; 13 out of 87 procedures had
for radiotherapy. Postoperative radiotherapy of the residual prophylactic purpose in patients with contralateral cancer treated
glandular tissue was performed within six months of surgery. The with other surgical procedures. Thus the final number of
breast radiation technique involved the use of restricted tangential therapeutic NSMs was 74 (Table III - Figure 2). Considering the
fields and of traditional target simulation centering. The dose was 74 procedures with curative intent, the technique was performed in
divided into 2 Gy per fraction in five fractions per week, up to a 47 cases (63.51%) due to invasive carcinoma (IDC), in 24 cases
total dose of 50 Gy within five weeks. (32.43%) to in situ carcinoma (DCIS), and in one case each to
388
Rulli et al: Oncologic Reliability of Nipple-sparing Mastectomy in Patients with BC
Table III. Surgical and radiotherapic treatment of patients. Table V. Nipple Areola Complex disturbances.
No. % RT+ RT– Total
NSMs 87 No complications 7 (70%) 47 (94%) 54
Prophylactic NSMs 13 14.94% Local relapse ( NAC ) 1 (10%) 1 (2%) 2
Curative NSMs 74 85.06% Vascular alterations 2 (20%) 2 (4%) 4
Skin incision
Lateral 26 29.9% Total 10 50 60
Periareolar 61 70.1%
Radiotherapy 10/60 16.6% RT+: radiotherapy; RT–: no radiotherapy.
No radiotherapy 50/60 83.4%
NSM: Nipple Sparing Mastectomy.
Results
Table IV. Nipple Areola Complex bottom involvement. The NAC was resected in 14 (18.9%) out of the 74 patients
initially indicated for curative NSM: in 11 (78.6%)
No. Positive Negative immediately, due to intraoperative detection of involved NAC
histology histology
bottom, and in three (21.4%) at a later time due to a false-
Intraoperative assessment negative result on intraoperative frozen sections.
of NAC bottom 74 11 (14.9%) 63 (85.1%) Among the 11 cases out of 74 curative NSMs with
intraoperative detection of involved NAC bottom, only five
Definitive assessment of NACs (45.5%) cases were confirmed on the final pathology. Among
removed for positive intraoperative
assessment of NAC bottom 11 5 (45.4%) 6 (54.6%)
the 63 patients whose intraoperative NAC bottom sampling
was negative, final histology was positive in three cases
Definitive assessment (4.8%) and subsequent NAC excision confirmed the presence
of NAC bottom 63 3 (4.8%) 60 (95.2%) of tumor in only one of them (33.3%) (Table IV, Figure 2).
(between negative Amongst the remaining 60 curative NSMs with effective
intraoperative assessments)
NAC preservation, in the 50 cases (83.3%) with complete
NACs removed for 3 1 (33.3%) 2 (66.7%) removal of subareolar glandular tissue by inverting the
positive definitive assessment nipple like a finger in a glove (Figures 5 and 6),
(after negative radiotherapy was not performed in agreement with
intraopearive assessment) radiotherapists. This group presented one disease recurrence
Total number of removed NACs 14 (18.9%)
(2%) and two transient vascular disturbances of the NAC
(4%). In ten cases (16.7%), when glandular tissue (no more
than 5 mm) was preserved below the NAC, radiotherapy
with restricted tangential fields was performed. This group
infiltrating tubular carcinoma (TC), mucinous carcinoma (MC) and also had one recurrence (10%) and two transient vascular
undefined histotype (1.35% each) (Table II). Intraoperative random NAC disturbances (20%) (Figure 7, Table V).
sections of the NAC bottom were sent for histological assessment Among the 60 patients with effective preservation of the
on frozen specimen. NAC, at a mean follow-up of 50.33 months (range=23-115
Thirteen (14.94%) other NSMs were carried out in the same months), three developed recurrences (5%), of which two were
period for preventive purposes in patients with unilateral cancer
locoregional (3.3%) and one was of the axillary extension
and at high risk of controlateral recurrence. These patients, of
whose nine (69.2%) suffered from IDC and four (30.8%) from
(1.7%), all identified through instrumental follow-up. Of the
DCIS, simultaneously underwent therapeutic Modified Radical two retroareolar recurrences, one of 10 mm emerged after 33
Mastectomy (MRM) and contralateral preventive NSM. Final months in a patient with prior IDC G3 size 13 mm with
histology identified one case (7.7%) of colloid neoplasm (size 4 negative sentinel node biopsy (SNB) with radiotherapy of the
mm) widely distanced from the NAC among these 13 preventive nipple, and the other of 8 mm after 37 months in a patient
NSMs. with prior IDC G2 size 15 mm and negative SNB not
In summary, considering 74 curative and 13 prophylactic NSMs,
submitted to adjuvant radiotherapy. Both patients underwent
we performed a total of 87 procedures (Figure 2).
NSM was performed by means of lateral incision in 26 cases
excision of the NAC. The latter, with a prior G2 IDC of 8 mm
(29.9%) and through periareolar incision with lateral splits in 61 and negative SNB, exhibited a recurrence in the breast axillary
cases (70.1%), providing for all 87 patients an immediate extension after 39 months, although this was surgically
reconstruction with tissue expander (Table III, Figures 3 and 4). removed (Table VI). These patients are currently disease free.
389
in vivo 27: 387-394 (2013)
Figure 1. Immediate reconstruction with tissue expander. Figure 3. Periareolar incision allows an excellent exposure of
subareolar tissue.
Figure 4. Final outcome of lateral incision.
With regard to complications, in the early postoperative
period a hematoma was observed and resolved with surgical
evacuation; most patients reported lack of sensitivity of the
nipple skin, whereas complications due to radiotherapy of
the NAC were negligible in all cases.
In regard to the relationship between radiotherapy and
Figure 2. Intraoperative and final histology of the NAC. NSM: Nipple vascular disturbances of the NAC, obviously excluding the 14
sparing mastectomy; NAC: Nipple areola complex. Number of resected patients with nipple excision, four transient NAC ischemic
NAC is highlighted in red. alterations occurred: two (20%) in the group receiving
radiotherapy and two (4%) amongst the patients with
complete removal of retroareolar tissue (Table V).
Considering the 73 executed NSMs (60 therapeutic and 13
Three patients manifested distant metastasis during preventive), alterations due to transient insufficiency of blood
follow-up: one pulmonary, one supraclavicular and one supply only occurred in the group with periareolar incision
hepatic after 14, 24 and 30 and months respectively (Table with lateral extension, which however, resolved
VII). Two patients died of other diseases not related to spontaneously after about two weeks in all cases. No vascular
cancer. disturbances occurred in the 26 NSMs with lateral incision.
390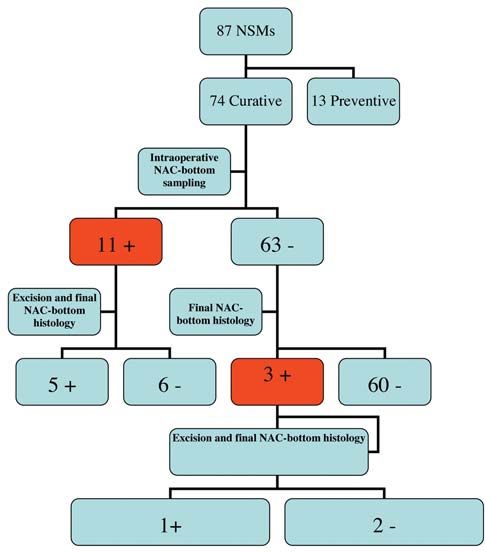
Rulli et al: Oncologic Reliability of Nipple-sparing Mastectomy in Patients with BC
Figure 5. Subareolar tissue completely removed like a finger in a glove.
Figure 7. Patients undergone to radiotherapy.
Discussion
The desire to ensure both oncologically result comparable to
that of classical MRM and psychological and physical
integrity of the patients was a major determining factor in
conducting this study over the eight years of our experience.
Figure 6. Subareolar tissue completely removed like a finger in a glove Our previous personal experience had already demonstrated
(inside view). technical feasibility and promising results in 10 patients (3).
391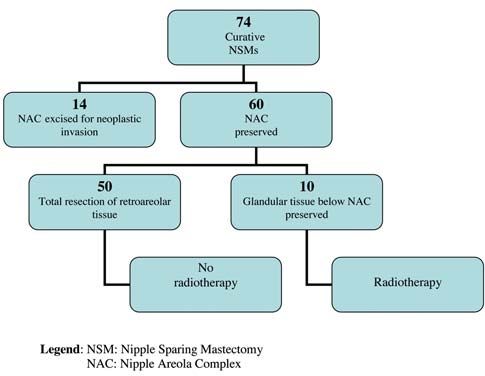
in vivo 27: 387-394 (2013)
Table VI. Locoregional relapse.
Follow-up (23-115 months) Location Patient history
33 Months Retroareolar IDC, G3, size 13 mm, negative SN, RT performed; treated with NAC excision.
37 Months Retroareolar IDC, G2, size 15 mm, negative SN, RT not performed; treated with NAC excision.
39 Months Axillary extension IDC, G2, size 8 mm, negative SN; treated with local excision
IDC: invasive carcinoma; SN: sentinel node; RT: radiotherapy; NAC: nipple areola complex.
The locoregional control of disease in the NAC was achieved Table VII. Metastatic disease.
by implementing a proper subareolar surgical procedure; in
Follow-up (23-115 months) Location
literature, the debate regarding the correct surgical technique
is still open. In fact, the decision to remove the retroareolar 30 Months Liver
glandular tissue is closely related on the one hand to the risk 24 Months Supraclavicular nodes
of local recurrence, and on the other to the vitality of the 14 Months Lung
NAC (17-19).
In our present series, only considering the 60 curative
NSMs, in 10 patients (16.6%) a small amount of subareolar
tissue was preserved with subsequent performance of
restricted tangential field radiotherapy (RT+ group) and in preserved) and in two (4%) of the RT- group (in which the
50 cases (83.3%) it was completely removed (RT- group). removal of retroareolar glandular tissue was considered
Retroareolar recurrences occurred in 20% of patients in the complete), however, these were transient and reversible
RT+ group vs. 4% of patients in the RT- group. Although (Table V).
such data relate to a small sample and require confirmation Although we have shown that total removal of retroareolar
of a wider series, they would seem to suggest a direct tissue is not detrimental to vascularization and increases
relationship between retroareolar recurrence and the amount oncological radicality, this procedure does lead to a
of retroareolar tissue preserved. worsening of the final esthetic result because a small portion
Data reported in literature show that the site of regional of the gland is critical to mantain the profile and the correct
recurrence is directly related to the tumor size (3,20), to its protrusion of the nipple. Most patients treated with radical
biological characteristics and proximity to the NAC (9, 21- excision of the retrareolar glandular tissue exhibited a
23). Petit and Veronesi argued in a prospective study on 579 reduction of the normal NAC protrusion.
cases that the recurrence rate after NSM and subsequent Some authors have focused on the comparison between
radiotherapy is not higher than that observed after MRM. the two different incisional options: radial on the upper-
Moreover, in the same series 56 patients with final outer quadrant , which offers easy access to the axilla and
histology positive for NAC infiltration, who refused adequate blood supply to the NAC, and periareolar, which
excision, did not exhibit any recurrence at a follow-up of may reduce the blood supply to the NAC, but favors a
20 months (14). Since one criticism of NSM is precisely excellent exposure of the subareolar tissue (27). Literature
the risk of subareolar recurrence, these data seem very data suggest that post-surgical alterations of the NAC are
significant. mostly attributable to the type of incision, and that radial
Some studies have similarly questioned the utility of incision on the upper-outer quadrant seems to respect more
radiotherapy, claiming that NSM is oncologically safe even the vascular integrity (28, 29). In a series of 54 procedures,
when not followed by radiation therapy (24). Other authors Crowe et al. reported 45 NSMs performed with lateral
corroborated such observation, defining the skin of the nipple incision without postoperative alterations of the NAC and
and areola as a physiological border of the mammary gland also claimed that medial incisions may actually compromise
(25, 26). blood flow (21). Within our series, the most practiced
In our personal experience, we attempted to obtain radical incision was periareolar, performed in 70.1% of cases and
removal of subareolar tissue and, through the improvement preferred since it provides immediate access to the
of the surgical technique, we succeeded in doing so without subareolar tissue, resulting in reduced time for the
increasing the risk of NAC necrosis. In fact, vascular intraoperative examination and faster and easier dissection
disturbances were observed in two (20%) patients of the RT+ of the gland, although it increases the risk of reduced blood
group (in which an amount of retroareolar tissue had been supply to the NAC.
392
Rulli et al: Oncologic Reliability of Nipple-sparing Mastectomy in Patients with BC
Given that in any study design there are several variables 8 Gajdos C, Tartter PI and Bleiweiss IJ: Subareolar breast cancers.
that influence the relapse rate, a careful selection of patients Am J Surg 180(3): 167-170, 2000.
by a multidisciplinary team according to strict criteria can 9 Vyas JJ, Chinoy RF andVaidya JS: Prediction of nipple and
areola involvement in breast cancer. Eur J Surg Oncol 24(1): 15-
help in determining feasibility, as well as oncological safety,
16, 1998.
and should lead to the general acceptance and widespread 10 Laronga C, Kemp B, Johnston D, Robb GL and Singletary SE:
use of such surgical technique. The incidence of occult nipple-areola complex involvement in
breast cancer patients receiving a skin-sparing mastectomy. Ann
Conclusion Surg Oncol 6(6): 609-613, 1999.
11 Gerber B, Krause A, Reimer T, Müller H, Küchenmeister I,
Eight years of experience have led us to the conclusion that Makovitzky J, Kundt G and Friese K: Skin-sparing mastectomy
NSM is an oncologically safe and valid technique that can with conservation of the nipple-areola complex and autologous
be used in any indication of mastectomy, as long as intra- reconstruction is an oncologically safe procedure. Ann Surg
and postoperative assessments exclude neoplastic 238(1): 120-127, 2003.
12 Petit JY, Veronesi U, Orecchia R, Rey P, Didier F, Giraldo A,
involvement of the NAC and always considering that
Luini A, De Lorenzi F, Rietjens M, Garusi C, Intra M, Yamaguchi
complete removal of retroareolar tissue may expose the S and Martella S: The nipple-sparing mastectomy: Early results
nipple to rare ischemic complications. of a feasibility study of a new application of perioperative
The achievement of our objective depends on a delicate radiotherapy (ELIOT) in the treatment of breast cancer when
balance between the maximum removal of glandular tissue mastectomy is indicated. Tumori 89(3): 288-291, 2003.
and the preservation of NAC viability. 13 Rusby JE, Brachtel EF, Taghian A, Michaelson JS, Koerner FC
and Smith BL: George Peters Award. Microscopic anatomy
Competing Interests within the nipple: Implications for nipple-sparing mastectomy.
Am J Surg 194(4): 433-437, 2007.
The Authors state that none of the authors involved in the 14 Petit JY, Veronesi U, Rey P, Rotmensz N, Botteri E, Rietjens M,
manuscript preparation has any conflicts of interest towards the Garusi C, De Lorenzi F, Martella S, Bosco R, Manconi A, Luini
manuscript itself, neither financial nor moral conflicts. Moreover, A, Galimberti V, Veronesi P, Ivaldi GB and Orecchia R: Nipple-
none of the Authors received support in the form of grants, sparing mastectomy: Risk of nipple-areolar recurrences in a
equipment, or pharmaceutical items. series of 579 cases. Breast Cancer Res Treat 114(1): 97-101,
2009.
References 15 Petit JY, Veronesi U, Orecchia R, Luini A, Rey P, Intra M, Didier
F, Martella S, Rietjens M, Garusi C, De Lorenzi F, Gatti G, Leon
1 Wang J, Xiao X, Wang J, Iqbal N, Baxter L, Skinner KA, Hicks ME and Casadio C: Nipple-sparing mastectomy in association
DG, Hajdu SI and Tang P: Predictors of nipple-areolar complex with intra operative radiotherapy (ELIOT): A new type of
involvement by breast carcinoma: Histopathologic analysis of mastectomy for breast cancer treatment. Breast Cancer Res Treat
787 consecutive therapeutic mastectomy specimens. Ann Surg 96(1): 47-51, 2006.
Oncol 19(4): 1174-1180, 2011. 16 Rowland JH, Desmond KA, Meyerowitz BE, Belin TR, Wyatt
2 Petit JY, Veronesi U, Luini A, Orecchia R, Rey PC, Martella S, GE and Ganz PA: Role of breast reconstructive surgery in
Didier F, De Lorenzi F, Rietjens M, Garusi C, Sonzogni A, physical and emotional outcomes among breast cancer survivors.
Galimberti V, Leida E, Lazzari R and Giraldo A: When J Natl Cancer Inst 92(17): 1422-1429, 2000.
mastectomy becomes inevitable: the nipple-sparing approach. 17 Stolier AJ and Grube BJ: Areola-sparing mastectomy: Defining
Breast 14(6): 527-531, 2005. the risks. J Am Coll Surg 201(1): 118-124, 2005.
3 Bistoni G, Rulli A, Izzo L, Noya G, Alfano C and Barberini F: 18 Komorowski AL, Zanini V, Regolo L, Carolei A, Wysocki WM
Nipple-sparing mastectomy. Preliminary results. J Exp Clin and Costa A: Necrotic complications after nipple- and areola-
Cancer Res 25(4): 495-497, 2006. sparing mastectomy. World J Surg 30(8): 1410-1413, 2006.
4 Didier F, Radice D, Gandini S, Bedolis R, Rotmensz N, Maldifassi 19 Stolier AJ, Sullivan SK and Dellacroce FJ: Technical
A, Santillo B, Luini A, Galimberti V, Scaffidi E, Lupo F, Martella S considerations in nipple-sparing mastectomy: 82 consecutive
and Petit JY: Does nipple preservation in mastectomy improve cases without necrosis. Ann Surg Oncol 15(5): 1341-1347, 2008.
satisfaction with cosmetic results, psychological adjustment, body 20 Brachtel EF, Rusby JE, Michaelson JS, Chen LL, Muzikansky
image and sexuality? Breast Cancer Res Treat 118(3): 623-633, A, Smith BL and Koerner FC: Occult nipple involvement in
2009. breast cancer: Clinicopathologic findings in 316 consecutive
5 Wellish DK, Schain WS, Barett Noone R and Little JW: The mastectomy specimens. J Clin Oncol 27(30): 4948-4954, 2009.
psychological contribution of nipple addition in breast 21 Crowe JP Jr, Kim JA, Yetman R, Banbury J, Patrick RJ and
reconstruction. Plast Reconstr Surg 80(5): 699-704, 1987. Baynes D: Nipple-sparing mastectomy: Technique and results of
6 Cense HA, Rutgers EJ, Lopes Cardozo M and Van Lanschot JJ: 54 procedures. Arch Surg 139(2): 148-150, 2004.
Nipple-sparing mastectomy in breast cancer: A viable option? 22 Kissin MW and Kark AE: Nipple preservation during
Eur J Surg Oncol 27(6): 521-526, 2001. mastectomy. Br J Surg 74: 58-61, 1987.
7 Lambert PA, Kolm P and Perry RR: Parameters that predict 23 Singletary SE: Skin-sparing mastectomy with immediate breast
nipple involvement in breast cancer. J Am Coll Surg 191(4): reconstruction: The M.D. Anderson Cancer Center experience.
354-359, 2000. Ann Surg Oncol 3: 411-416, 1996.
393in vivo 27: 387-394 (2013) 24 Sakurai T, Zhang N, Suzuma T, Umemura T, Yoshimura G, 28 Crowe JP, Patrick RJ, Yetman RJ and Djohan R: Nipple-sparing Sakurai T and Yang Q: Long-term follow-up of nipple-sparing mastectomy update: One hundred forty-nine procedures and mastectomy without radiotherapy: A single-center study at a clinical outcomes. Arch Surg 143(11): 1106-1110; discussion Japanese institution. Med Oncol 30(1): 481, 2013. 1110, 2008. 25 Paepke S, Schmid R, Fleckner S, Paepke D, Niemeyer M, 29 Regolo L, Ballardini B, Gallarotti E, Scoccia E and Zanini V: Schmalfeldt B, Jacobs VR and Kiechle M: Subcutaneous Nipple sparing mastectomy: An innovative skin incision for an mastectomy with conservation of the nipple-areola skin: alternative approach. Breast 17(1): 8-11, 2008. Broadening the indications. Ann Surg 250(2): 288-292, 2009. 26 Margulies AG, Hochberg J, Kepple J, Henry-Tillman RS, Westbrook K and Klimberg VS: Total skin-sparing mastectomy without preservation of the nipple-areola complex. Am J Surg 190(6): 907-912, 2005. 27 Babiera G and Simmons R: Nipple-areolar complex-sparing Received March 12, 2013 mastectomy: Feasibility, patient selection, and technique. Ann Revised March 29, 2013 Surg Oncol. 17 (Suppl 3): 245-248, 2010. Accepted April 1, 2013 394
You can also read