OREGON HEALTH AND SCIENCE UNIVERSITY OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE - OHSU
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
OHSU Health System
Office of Clinical Integration and Evidence-Based Practice
Evidence Brief
March 2019
OREGON HEALTH AND SCIENCE UNIVERSITY
OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE
Evidence-Based Practice Summary
Comparison between two 52mg levonorgestrel-releasing intrauterine systems: Liletta and Mirena
BACKGROUND AND RATIONALE
In the United States, 45% of pregnancies each year are unintended (Finer 2016). Females who use long-acting reversible contraception
(LARC) methods, specifically the copper intrauterine device, levonorgestrel intrauterine systems (LNG-IUS), or single-rod contraceptive
implants, have substantially lower rates of unintended pregnancies (CDC 2013 and Winner 2012). Currently, four different LNG-IUSs
have been approved by the Food and Drug Administration (FDA) and are available in the U.S.: two devices that contain 52mg of LNG
[Mirena (LNG-IUS 52 mg) and Liletta, Levosert in Europe (LNG 52 mg)], a device that contains 19.5 mg [Kyleena (LNG-IUS 19.5 mg)]
and a slightly smaller device that contains 13.5 mg [Skyla, Jaydess in Europe (LNG-IUS 13.5 mg)].
Mirena was initially developed in Finland and Sweden in the 1980s, receiving FDA approval in 2000 for the U.S. market (U.S. FDA).
Liletta was subsequently developed by Medicines360, a non-profit pharmaceutical company in the U.S., to address financial barriers for
low-income females obtaining LARCs. Liletta was approved by the FDA in 2015, and since then has been marketed as a lower cost
alternative for clinics eligible for 340B pricing through the Department of Health and Human Services (Curtis 2017). The two 52mg of
LNG devices are similar in device dimensions and duration of use, but vary slightly in LNG daily release and insertion tube diameter.
The purpose of this evidence brief is to explore the comparative effectiveness between the Liletta and Mirena, and to determine if
differences in features effect patient outcomes or satisfaction.
1Office of Clinical Integration and EBP GRADE Table
LNG-IUD comparison table from Grandi 2018 expert opinion article:
*Liletta was approved for 5 years in 2018.
ASK THE QUESTION
In women of reproductive age, what is the comparative effectiveness (unintended pregnancy rate, pain, bleeding, device malfunction,
satisfaction) of the Mirena levonorgestrel-releasing intrauterine system compared to Liletta?
SEARCH FOR EVIDENCE
Appendix C
CRITICALLY ANALYZE THE EVIDENCE
Over 200 clinical trials were found evaluating levonorgestrel-releasing intrauterine systems (LNG-IUS), with the majority studying the
LNG-IUS systems against other contraception methods, comparing difference doses of LNG, or studying its effect in sub-populations,
such as in women with endometriosis or breast cancer. Only one study was found directly studying Mirena or Liletta, investigating its
impact on bleeding patterns. Therefore, the results are compared from the Phase III clinical trials for both devices that were conducted
2Office of Clinical Integration and EBP GRADE Table
to determine each device’s efficacy. For Mirena, two clinical trials were found evaluating its efficacy and one pharmacokinetics study
evaluating average LNG serum concentration over three years. For Liletta, one clinical trial is currently underway evaluating its efficacy,
with four research articles published reporting the data and one pharmacokinetics study evaluating average LNG micrograms per day
release.
Mirena
Mirena has been studied for safety and efficacy in two clinical trials (Andersson 1994 and Luukkainen 1986) in Finland and Sweden.
1169 women 18 to 35 years of age at enrollment used Mirena for up to 5 years, for a total of 45,000 women months of exposure.
Subjects had previously been pregnant, had no history of ectopic pregnancy, had no history of pelvic inflammatory disease over the
preceding 12 months, were predominantly Caucasian, and over 70% of the participants had previously used IUDs (intrauterine
devices). The reported 12-month pregnancy rates were less than or equal to 0.2 per 100 women and the cumulative 5-year pregnancy
rate was approximately 0.7 per 100 women. However, due to limitations of the available data a precise estimate of the pregnancy rate
is not possible (U.S. FDA). 16.8% of women experienced amenorrhea within the first year. (FDA 2000; Andersson 1994; Luukkainen
1986)
Liletta
ACCESS IUS is a Phase III Clinical Trial (Teal 2019) that has been underway since 2009 and was designed to assess efficacy and
safety of a branded LNG 52-mg IUS (Liletta) in a diverse population of females. The trial is ongoing at 29 U.S. sites, including
reproductive health clinics, private officers, and university centers. The clinical trial included over 1,751 women, with 58% nulliparous
females. Over the course of the trial, nine pregnancies occurred in four nulliparous and five parous participants. The 5-year life-table
pregnancy rates in nulliparous and parous females were 0.83% (95% CI 0.28-2.50%) and 1.26% (95% CI 0.51-3.10%), respectively.
Six (67%) pregnancies were ectopic, resulting in an ectopic pregnancy rate through five years of 0.13 per 100 women-years.
Approximately 50% of participants experienced amenorrhea or spotting only during the last 90 days of the first year of use and 80%
experienced amenorrhea, spotting, or light bleeding only. By the third year, these rates reached over 70% and 90%, respectively, and
stayed approximately the same through the fifth year. Overall, 322 (18.8%) participants discontinued use as a result of an adverse
event. The most frequent event related to expulsion (n=65 [3.8%]), most (50 [80.6%]) during the first year of use. Only 39 2.2% IUS
users discontinued as a result of bleeding symptoms. Pelvic infection was diagnosed in 14 (0.8%) participants (FDA 2015; Teal 2019;
Eisenberg 2015).
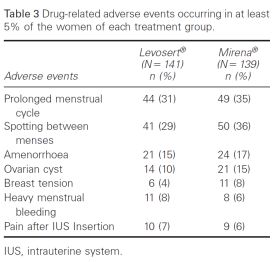
One RCT (Mawet 2014) was conducted directly comparing Levosert (European name for Liletta device) for the treatment of heavy
menstrual bleeding in comparison to Mirena. Study found that Levosert as well as Mirena users experienced a consequent and similar
(P > 0.1) reduction in menstrual blood loss (-142.3 and -146.4 mL, respectively. Adverse events were reported with similar frequency
3Office of Clinical Integration and EBP GRADE Table
between the two groups. Users complained of pain after insertion of the IUS with the same frequency in both Levosert (7.1%) and
Mirena (6.5%).
Two studies were found investigating the pharmacokinetics of the each device. The 5-year average release rate was 14.7 mcg/day in
the Liletta study (Creinin 2016). The average LNG serum concentration over 3 years of use for Mirena was 218 ng/L for LNG-IUS 20
mug/24 h (Apter 2014).
Overall, there is low to very low level of evidence regarding the efficacy of the Mirena vs. Liletta devices. Both Liletta and Mirena clinical
trials are considered to have “moderate risk of bias” due to study limitations and imprecision. One important difference to note is
between populations studied in both device’s trials. Mirena included only parous women, while Liletta included both parous and
nulliparous women.
Pregnancy Rates
Mirena Liletta
Pregnancy Rates – 12 month 0.2 – Parous1,11 0.15 – Parous and Nulliparous14
Pregnancy Rates – Cumulative 5-year 0.7 – Parous1,11 0.83 – Nulliparous14
1.26 – Parous14
Ectopic Pregnancies 0.02 – Parous1,11 0.13 – Parous and Nulliparous14
Bleeding Patterns
Mirena Liletta
Amenorrhea 16.8% - 1st year1,11 36.6% - 1styear14
43.4% - 2 year14
nd
51.0% - 3rd year14
Adverse Events
4Office of Clinical Integration and EBP GRADE Table
Mirena Liletta
Expulsion 5.8%1,11 3.8%14
Pain after IUS Insertion 7.1%12 6.5%12
GRADE Table Templates
BODY OF EVIDENCE APPRAISAL TABLE FOR:
Population: Nulliparous and parous women aged 16–45 years
Modality: Liletta
Outcome: Pregnancy Rates
Quality (certainty) of evidence for: (outcome)
High
Moderate
Low
Very Low
Risk of Bias across studies: Lower Quality Rating if: Other Considerations:
High Studies inconsistent (wide variation of treatment effect across Lower Quality Rating if:
Medium studies, population, interventions, or outcomes varied) - Unknown Publication Bias (e.g. pharmaceutical company sponsors study
Low on effectiveness of drug only small, positive studies found)
Studies are indirect (PICO question is quite different from the
available evidence in regard to population, intervention, comparison, Increase Quality Rating if:
or outcome) Large effect
Dose-response gradient
Studies are imprecise (when studies include few patients and few Plausible confounders or other biases increase certainty of
events, and thus have wide confidence intervals, and the results are effect
uncertain)
Endpoint Results / Outcome
Study Acronym; Author; Year
Aim of Study Patient Population Study Methods (Absolute Event Rates, P Design Limitations
Published; Location
values; OR or RR; & 95% CI)
Author: Teal, S.B., et al. To assess the 5-year Size: 1751 enrollees including Type: RCT Results: The 5-year life-table Study Limitations:
Year Published: 2019 contraceptive efficacy and 1,600 females aged 16-35 and pregnancy rate was 0.92% None
safety of a levonorgestrel 151 aged 36-45. Intervention: Women were (95% CI 0.46-1.82%) over RCTs
Location: University of Lack of blinding
(LNG) 52-mg intrauterine enrolled in a 4:1 ration to 59,399 cycles. Nine
Colorado Lack of allocation
system (IUS) from an ongoing Liletta and Mirena. After pregnancies occurred in four
Journal: Obstetrics & At time of data evaluation, 495 concealment
10-year phase 3 contraceptive enrolling 159 of the planned nulliparous and give parous
Gynecology participants finished 5 years Stopped early for benefit
trial 400 Mirena participants, it was participants. The 5-year life-
and 176 had entered the Incorrect analysis of ITT
determined that this table pregnancy rates in
seventh year of IUS use Selective reporting of
comparator group would no nulliparous and parous
longer needed for non-U.S. females was 0.83% (95% CI measures (e.g., no effect
0.28-2.50%) and 1.26% (95% outcome)
5Office of Clinical Integration and EBP GRADE Table
Inclusion Criteria: Healthy, filing, further enrollment was CI 0.51-3.10%), respectively. Large losses to F/U
sexually active (at least four limited to LNG20. Six pregnancies (67%) were Difference in important
times monthly), nulliparous and ectopic, resulting in an prognostic factors at baseline
parous females aged 16-45 Subjects completed screening ectopic pregnancy rate
years with regular menstrual and enrollment, follow-up through 5 years of 0.13 per
cycles (21-35 days when not during the first year including 100 women-years. No
using hormones). No visits at 1, 3, 6 and 12 months pregnancies occurred in LNG
restrictions on weight or body and a telephone contact at 52-mg IUS users aged 36-45
mass index. month 9. years of age at enrollment.
Exclusion Criteria: Women Participants completed a diary *Because Mirena cohort was
using contraception for cycle for the first 24 months for daily not large enough for
control, women recently using recording of other effectiveness calculations or
progestin injectable contraceptive use and the statistically meaningful
contraception within the greatest amount of bleeding comparisons, those data are
preceding 9 months or 6 that day as none, spotting, light not presented.
months. Women who flow, normal flow, or heavy
discontinued study due to flow based on their own
pregnancy. subjective impression. After 24
months, the diary included only
additional contraceptive use.
Participants were asked at
each visit or telephone contact
beginning with month 27 to
describe their bleeding pattern
over the preceding 3 months.
Author: Eisenberg, D.L., et al. To assess 3-year data on the Size: 1751 nulliparous and Type: Secondary analysis of Results: Six pregnancies Study Limitations:
Year Published: 2015 efficacy and safety of a new multiparous women, across 29 data from the ACCESS IUS occurred, four of which were None
52-mg levonorgestrel clinical sites in USA multicenter, Phase 3, open- ectopic. The Pearl Index for Non-Randomized Studies
Location: Medicines360, San LNG20 was 0.15 (95% CI Failure to develop and
Francisco, CA intrauterine contraceptive label clinical trial
(LNG20) designed for up to 7 0.02-0.55) through Year 1, apply appropriate eligibility
and Allergan, Irvine, CA Of the 1751 women enrolled, 0.26 (95% CI 0.10-0.57) criteria
years use 1714 (97.9%) had successful Intervention: Pregnancy rate
Journal: Contraception through Year 2, and 0.22 Flawed measurement of
placement: 14 (0.8%) of these was evaluated for women aged (95% CI 0.08-0.49) through both exposure and outcome
women discontinued prior to 16-35 using the Pearl Index. Year 3. The cumulative life- Failure to adequately
90 days for non-bleeding- Evaluated bleeding patterns for table pregnancy rate was 0.55 control confounding
related complaints leaving women using a daily diary (95% CI 0.24-1.23) through 3 Incomplete or
1700 women in the analysis. completed by participants for years. inadequately short follow-up
the first 2 years and by
Inclusion Criteria: Healthy, questionnaire every 3 months
non-pregnant, sexually active, thereafter. Assessed
nulliparous and parous amenorrhea rates over 3 years
women aged 16–45 years who and the proportion of subjects
desired a hormonal with infrequent, frequent,
6Office of Clinical Integration and EBP GRADE Table
IUS for contraception. prolonged and irregular
Participants had to report bleeding per 90-day reference
regular menstrual cycles every period over 2 years for the
21–35 days with a variation of entire study population as well
typical cycle length of no more as comparing nulliparous and
than 5 days. Women with parous women and obese and
successful IUS placement non-obese women
Exclusion Criteria: Women
using contraception for cycle
control Women recently using
progestin injectable
contraception within the
preceding 9 months or 6
months.
References:
1. Teal, S. B., et al. (2019). "Five-Year Contraceptive Efficacy and Safety of a Levonorgestrel 52-mg Intrauterine System." Obstetrics & Gynecology 133(1): 63-70.
2. Eisenberg, D. L., et al. (2015). "Three-year efficacy and safety of a new 52-mg levonorgestrel-releasing intrauterine system." Contraception 92(1): 10-16.
BODY OF EVIDENCE APPRAISAL TABLE FOR:
Population: Parous Women between 18 – 38 years old
Modality: Mirena
Outcome: Pregnancy Rates
Quality (certainty) of evidence for: (outcome)
High
Moderate
Low
Very Low
Risk of Bias across studies: Lower Quality Rating if: Other Considerations:
High Studies inconsistent (wide variation of treatment effect across Lower Quality Rating if:
Medium studies, population, interventions, or outcomes varied) Publication Bias (e.g. pharmaceutical company sponsors study
Low on effectiveness of drug only small, positive studies found)
Studies are indirect (PICO question is quite different from the
available evidence in regard to population, intervention, comparison, Increase Quality Rating if:
or outcome) Large effect
Dose-response gradient
Studies are imprecise (when studies include few patients and few Plausible confounders or other biases increase certainty of
events, and thus have wide confidence intervals, and the results are effect
uncertain)
Endpoint Results / Outcome
Study Acronym; Author; Year
Aim of Study Patient Population Study Methods (Absolute Event Rates, P Design Limitations
Published; Location
values; OR or RR; & 95% CI)
Author: Andersson, K., et al. To investigate more Size: 2758 women were Type: RCT Results: The 5-year Study Limitations:
Year Published: 1994 extensively a study between allocated, 937 had a Nova T cumulative gross pregnancy None
7Office of Clinical Integration and EBP GRADE Table
Location: Finland and Sweden LNG-IUD and Nova T during and 1821 had an LNG-IUD Intervention: Women were rate was 0.5% for the LNG- RCTs
Journal: Contraception five years of use inserted. randomized to treatment by IUD. During the 60-month Lack of blinding
Nova T or LNG-IUD. A observation period, 5 women Lack of allocation
Inclusion Criteria: Healthy standardized interview was in the LNG-IUD group concealment
women, 18-38 years old and at performed at admission and at became pregnant. Among the Stopped early for benefit
least one previous pregnancy. every follow-up visit, which pregnancies, 1 was ectopic. Incorrect analysis of ITT
was planned after 3 and 12 Selective reporting of
months and then yearly up to measures (e.g., no effect
Exclusion Criteria: Women five years. Furthermore, during outcome)
with a history of ectopic the first 12 months, all women Large losses to F/U
pregnancy, who were breast- were requested to note Difference in important
feeding, or had used injectable bleeding patterns continuously prognostic factors at baseline
hormones for contraception on a specially designed chart. – Baseline characteristics note
during the preceding 12 included
months were excluded.
Author: Luukkainen, T., et al. To study the levonorgestrel- Size: 10,600 women-months of Type: RCT Results: There was only one Study Limitations:
releasing IUD (LNG-IUD) to LNG-IUD use. pregnancy for both LNG-IUDs None
Year Published: 1986
reduce problems encountered together during the 10,605 RCTs
Location: Finland Intervention: Participants were
with conventional IUDS, such woman-months of use, with a Lack of blinding
Journal: Contraception randomized to receive three
as an increase in the amount Pearl-Index of 0.2 for both Lack of allocation
Inclusion Criteria: Healthy different IUDS, two LNG-IUDs,
and duration of bleeding and combined for 20 ug, and 0.11 concealment
women selecting fertility with 20 ug or 30 ug,
greater risk of infection. combined. Stopped early for benefit
control in clinics were asked to respectively. The control
Incorrect analysis of ITT
participate, if they had no device was the Nova T.
Selective reporting of
history of ectopic pregnancy. measures (e.g., no effect
outcome)
Exclusion Criteria: No Large losses to F/U
exclusions were made based Difference in important
on medical history. prognostic factors at baseline
References:
1. Andersson, K., et al. (1994). "Levonorgestrel-releasing and copper-releasing (Nova T) IUDs during five years of use: a randomized comparative trial." Contraception 49(1): 56-72.
2. Luukkainen, T., et al. (1986). "Five years' experience with levonorgestrel-releasing IUDs." Contraception 33(2): 139-148.
BODY OF EVIDENCE APPRAISAL TABLE FOR:
Population: Nulliparous and parous women aged 16–45 years
Modality: Liletta
Outcome: Bleeding patterns
Quality (certainty) of evidence for: (outcome)
High
Moderate
Low
Very Low
8Office of Clinical Integration and EBP GRADE Table
Risk of Bias across studies: Lower Quality Rating if: Other Considerations:
High Studies inconsistent (wide variation of treatment effect across Lower Quality Rating if:
Medium studies, population, interventions, or outcomes varied) Publication Bias (e.g. pharmaceutical company sponsors study
Low on effectiveness of drug only small, positive studies found)
Studies are indirect (PICO question is quite different from the
available evidence in regard to population, intervention, comparison, Increase Quality Rating if:
or outcome) Large effect
Dose-response gradient
Studies are imprecise (when studies include few patients and few Plausible confounders or other biases increase certainty of
events, and thus have wide confidence intervals, and the results are effect
uncertain)
Endpoint Results / Outcome
Study Acronym; Author; Year
Aim of Study Patient Population Study Methods (Absolute Event Rates, P Design Limitations
Published; Location
values; OR or RR; & 95% CI)
Author: Teal, S.B., et al. To assess the 5-year Size: 1751 enrollees including Type: RCT Results: Amenorrhea rates Study Limitations:
Year Published: 2019 contraceptive efficacy and 1,600 females aged 16-35 and increased over 5 years of None
safety of a levonorgestrel 151 aged 36-45. Intervention: Women were follow-up. Approximately 50% RCTs
Location: University of Lack of blinding
(LNG) 52-mg intrauterine enrolled in a 4:1 ration to of participants experienced
Colorado Lack of allocation
system (IUS) from an ongoing Liletta and Mirena. After amenorrhea or spotting only
Journal: Obstetrics & At time of data evaluation, 495 concealment
10-year phase 3 contraceptive enrolling 159 of the planned during the last 90 days of the
Gynecology participants finished 5 years Stopped early for benefit
trial 400 Mirena participants, it was first year of use and 80%
and 176 had entered the Incorrect analysis of ITT
determined that this experienced amenorrhea,
seventh year of IUS use Selective reporting of
comparator group would no spotting, or light bleeding
longer needed for non-U.S. only. By the third year, these measures (e.g., no effect
Inclusion Criteria: Healthy, filing, further enrollment was rates reached 70% and 90%, outcome)
sexually active (at least four limited to LNG20. respectively, and stayed Large losses to F/U
times monthly), nulliparous and approximately the same Difference in important
parous females aged 16-45 Subjects completed screening through the fifth year. prognostic factors at baseline
years with regular menstrual and enrollment, follow-up
cycles (21-35 days when not during the first year including
using hormones). No For participants who
visits at 1, 3, 6 and 12 months subjectively reported heavy
restrictions on weight or body and a telephone contact at
mass index. menstrual flow at baseline, 53
month 9. of 145 (36.6%), 52 of 122
(43.4%), and 52 of 102 (51%)
Exclusion Criteria: Women Participants completed a diary reported amenorrhea or
using contraception for cycle for the first 24 months for daily spotting only at 1, 2, and 3
control Women recently using recording of other years, respectively.
progestin injectable contraceptive use and the
contraception within the greatest amount of bleeding
preceding 9 months or 6 that day as none, spotting, light *Because Mirena cohort was
months. Women who flow, normal flow, or heavy not large enough for
discontinued study due to flow based on their own effectiveness calculations or
pregnancy. subjective impression. After 24 statistically meaningful
months, the diary included only comparisons, those data are not
additional contraceptive use. presented.
Participants were asked at
9Office of Clinical Integration and EBP GRADE Table
each visit or telephone contact
beginning with month 27 to
describe their bleeding pattern
over the preceding 3 months.
Author: Eisenberg, D.L., et al. To assess 3-year data on the Size: 1751 nulliparous and Type: Secondary analysis of Results: Amenorrhea rates at Study Limitations:
Year Published: 2015 efficacy and safety of a new multiparous women, across 29 data from the ACCESS IUS 1 and 3 years in None
52-mg levonorgestrel clinical sites in USA multicenter, Phase 3, open- levonorgestrel 52mg IUS Non-Randomized Studies
Location: Medicines360, San users were 19 and 37%, Failure to develop and
Francisco, CA intrauterine contraceptive label clinical trial
(LNG20) designed for up to 7 respectively. The infrequent apply appropriate eligibility
and Allergan, Irvine, CA Of the 1751 women enrolled, bleeding rate increased from criteria
years use 1714 (97.9%) had successful Intervention: Evaluated
Journal: Contraception 14% in the first 90 days to Flawed measurement of
placement: 14 (0.8%) of these bleeding patterns for women 30% at the end of Year 1, and both exposure and outcome
women discontinued prior to using a daily diary completed was maintained at the same Failure to adequately
90 days for non-bleeding- by participants for the first 2 rate through Year 2. Frequent, control confounding
related complaints leaving years and by questionnaire prolonged and irregular Incomplete or
1700 women in the analysis. every 3 months thereafter. bleeding declined to low inadequately short follow-up
Assessed amenorrhea rates levels by the end of the first
over 3 years and the year. Discontinuation for
Inclusion Criteria: Healthy, proportion of subjects with
non-pregnant, sexually active, bleeding related complaints
infrequent, frequent, occurred in 35 (2.1%, 95% CI
nulliparous and parous prolonged and irregular
women aged 16–45 years who 1.3–2.7%) women during the
bleeding per 90-day reference first 36 months; only one
desired a hormonal period over 2 years for the
IUS for contraception. subject discontinued for
entire study population as well amenorrhea (in Year 2).
Participants had to report as comparing nulliparous and
regular menstrual cycles every Outcomes did not vary for
parous women and obese and nulliparous versus parous or
21–35 days with a variation of non-obese women
typical cycle length of no more obese versus non-obese
than 5 days. Women with women.
successful IUS placement
Exclusion Criteria: Women
using contraception for cycle
control Women recently using
10Office of Clinical Integration and EBP GRADE Table
progestin injectable
contraception within the
preceding 9 months or 6
months.
Author: Darney, P.D., et al. To evaluate amenorrhea Size: 1714 nulliparous and Type: Secondary cohort Results: In the month before Study Limitations:
Year Published: 2018 patterns and predictors of multiparous women, across 29 analysis of data from the enrollment, 148 and 1566 None
amenorrhea during the first clinical sites in USA ACCESS IUS multicenter, women, respectively, had Non-Randomized Studies
Location: University of Phase 3, open-label clinical trial used and not used a Failure to develop and
year after levonorgestrel 52
California, San Francisco levonorgestrel IUS. Prior users apply appropriate eligibility
mg intrauterine system (IUS)
Journal: Contraception Inclusion Criteria: Healthy, averaged 50+/-19 months of criteria
placement Intervention: Subjects
non-pregnant, sexually active, use before IUS placement; Flawed measurement of
nulliparous and parous completed screening and
enrollment, follow-up during 38.4% of these women both exposure and outcome
women aged 16–45 years who reported amenorrhea at 12 Failure to adequately
desired a hormonal the first year including visits at
1, 3, 6 and 12 months and a months. Amenorrhea rates for control confounding
IUS for contraception. non-prior-users at 3, 6, 9 and Incomplete or
Participants had to report telephone contact at month 9.
12 months were 0.2%, 9.1%, inadequately short follow-up
regular menstrual cycles every 17.2% and 16.9%,
21–35 days with a variation of Subjects completed a daily
paper diary to indicate the respectively. During the first
typical cycle length of no more 12 months, 29 (1.7%) women
than 5 days. Women with greatest amount of bleeding
that day as none, spotting, light discontinued for bleeding
successful IUS placement irregularities; no women
flow, normal flow or heavy
flow. discontinued for amenorrhea.
Exclusion Criteria: Women The only significant predictor
using contraception for cycle of amenorrhea at 12 months
control Women recently using was self-reported baseline
progestin injectable duration of menstrual flow of
contraception within the fewer than 7 days vs. 7 or
preceding 9 months or 6 more days (18.2% vs. 5.2%,
months. adjusted odds ratio 3.70
[1.69, 8.07]). No relationships
were found between 12-
month amenorrhea rates and
age, parity, race, body mass
index, baseline flow intensity
or hormonal contraception
use immediately prior to IUS
placement.
Author: Schreiber, C.A., et al. To evaluate bleeding patterns Size: 1700 nulliparous and Type: Secondary cohort Results: Amenorrhea rates in Study Limitations:
for the Liletta((R)) multiparous women, across 29 analysis of data from the levonorgestrel 52mg IUS None
Year Published: 2018
levonorgestrel 52 mg clinical sites in USA ACCESS IUS multicenter, users increased over 3 years. Non-Randomized Studies
Location: Phase 3, open-label clinical trial Infrequent bleeding was Failure to develop and
intrauterine system (IUS) using
Journal: European Journal of the World Health Organization reported by 14% of apply appropriate eligibility
Contraception & Reproductive Inclusion Criteria: Healthy, levonorgestrel 52mg IUS criteria
Belsey definitions non-pregnant, sexually active, Intervention: Subjects
Health Care users in the first 90 days, Flawed measurement of
nulliparous and parous completed screening and
increased to 30% at the end both exposure and outcome
enrollment, follow-up during
11Office of Clinical Integration and EBP GRADE Table
women aged 16–45 years who the first year including visits at of Year 1, and was maintained Failure to adequately
desired a hormonal 1, 3, 6 and 12 months and a at the same rate through Year control confounding
IUS for contraception. telephone contact at month 9. 2. Frequent bleeding occurred Incomplete or
Participants had to report in 26% of levonorgestrel inadequately short follow-up
regular menstrual cycles every Subjects completed a daily 52mg IUS users in the first 90
21–35 days with a variation of paper diary to indicate the days and quickly declined to
typical cycle length of no more greatest amount of bleeding fewer than 10% in the second
than 5 days. Women with that day as none, spotting, light 90-day reference period.
successful IUS placement flow, normal flow or heavy Prolonged bleeding declined
flow. in a similar manner from 51%
Exclusion Criteria: Women in the first 90 days to 10% in
using contraception for cycle the second 90-day reference
control Women recently using period. Irregular bleeding was
progestin injectable reported by 38% of women in
contraception within the the first 90 days, declining to
preceding 9 months or 6 14% in the second 90 days
months. and 6% by the end of the first
year. Outcomes did not vary
for nulliparous versus parous
or obese versus non-obese
women.
References:
1. Darney, P. D., et al. (2018). "Amenorrhea rates and predictors during 1 year of levonorgestrel 52 mg intrauterine system use." Contraception 97(3): 210-21
2. Eisenberg, D. L., et al. (2015). "Three-year efficacy and safety of a new 52-mg levonorgestrel-releasing intrauterine system." Contraception 92(1): 10-16.
3. Schreiber, C. A., et al. (2018). "Bleeding patterns for the Liletta((R)) levonorgestrel 52 mg intrauterine system." European Journal of Contraception & Reproductive Health Care 23(2): 116-120.
4. Teal, S. B., et al. (2019). "Five-Year Contraceptive Efficacy and Safety of a Levonorgestrel 52-mg Intrauterine System." Obstetrics & Gynecology 133(1): 63-70.
BODY OF EVIDENCE APPRAISAL TABLE FOR:
Population: Parous Women between 18 – 38 years old
Modality: Mirena
Outcome: Bleeding patterns
Quality (certainty) of evidence for: (outcome)
High
Moderate
Low
Very Low
Risk of Bias across studies: Lower Quality Rating if: Other Considerations:
High Studies inconsistent (wide variation of treatment effect across Lower Quality Rating if:
Medium studies, population, interventions, or outcomes varied) Publication Bias (e.g. pharmaceutical company sponsors study
Low on effectiveness of drug only small, positive studies found)
Studies are indirect (PICO question is quite different from the
available evidence in regard to population, intervention, comparison, Increase Quality Rating if:
or outcome) Large effect
Dose-response gradient
12Office of Clinical Integration and EBP GRADE Table
Studies are imprecise (when studies include few patients and few Plausible confounders or other biases increase certainty of
events, and thus have wide confidence intervals, and the results are effect
uncertain)
Endpoint Results / Outcome
Study Acronym; Author; Year
Aim of Study Patient Population Study Methods (Absolute Event Rates, P Design Limitations
Published; Location
values; OR or RR; & 95% CI)
Author: Andersson, K., et al. To investigate more Size: 2758 women were Type: RCT Results: During the first year Study Limitations:
extensively a study between allocated, 937 had a Nova T after IUD insertion, 16.8% of None
Year Published: 1994
LNG-IUD and Nova T during and 1821 had an LNG-IUD the LNG-IUD users RCTs
Location: Finland and Sweden Intervention: Women were
five years of use inserted. experienced a period of at Lack of blinding
Journal: Contraception randomized to treatment by
least 90 days’ amenorrhea. Lack of allocation
Nova T or LNG-IUD. A
The cumulative net rate of concealment
Inclusion Criteria: Healthy standardized interview was
removal because of Stopped early for benefit
women, 18-38 years old and at performed at admission and at
amenorrhea was 4.3 for LNG- Incorrect analysis of ITT
least one previous pregnancy. every follow-up visit, which
IUD. Amenorrhea led to Selective reporting of
was planned after 3 and 12
higher termination rate in measures (e.g., no effect
months and then yearly up to
Exclusion Criteria: Women younger women compared to outcome)
five years. Furthermore, during
with a history of ectopic older. Large losses to F/U
the first 12 months, all women
pregnancy, who were breast- Difference in important
were requested to note
feeding, or had used injectable prognostic factors at baseline
bleeding patterns continuously
hormones for contraception – Baseline characteristics note
on a specially designed chart.
during the preceding 12 included
months were excluded.
Author: Luukkainen, T., et al. To study the levonorgestrel- Size: 10,600 women-months of Type: RCT Results: The amount and Study Limitations:
Year Published: 1986 releasing IUD (LNG-IUD) to LNG-IUD use. duration of menstrual None
reduce problems encountered Intervention: Participants were bleeding was greatly reduced, RCTs
Location: Finland leading to a high incidence of Lack of blinding
with conventional IUDS, such randomized to receive three
Journal: Contraception as an increase in the amount oligo- or amenorrhea. Lack of allocation
Inclusion Criteria: Healthy different IUDS, two LNG-IUDs,
and duration of bleeding and with 20 ug or 30 ug, concealment
greater risk of infection. women selecting fertility Removals for amenorrhea Stopped early for benefit
control in clinics were asked to respectively. The control
device was the Nova T. occurred during the first two Incorrect analysis of ITT
participate, if they had no years and were followed by Selective reporting of
history of ectopic pregnancy. normal menstrual cycles. measures (e.g., no effect
outcome)
Exclusion Criteria: No Large losses to F/U
exclusions were made based Difference in important
on medical history. prognostic factors at baseline
References:
1. Andersson, K., et al. (1994). "Levonorgestrel-releasing and copper-releasing (Nova T) IUDs during five years of use: a randomized comparative trial." Contraception 49(1): 56-72.
2. Luukkainen, T., et al. (1986). "Five years' experience with levonorgestrel-releasing IUDs." Contraception 33(2): 139-148.
13Office of Clinical Integration and EBP GRADE Table
BODY OF EVIDENCE APPRAISAL TABLE FOR:
Population: Nulliparous and parous women aged 16–45 years
Modality: Levosert (Liletta in US) vs. Mirena
Outcome: Bleeding patterns
Quality (certainty) of evidence for: (outcome)
High
Moderate
Low
Very Low
Risk of Bias across studies: Lower Quality Rating if: Other Considerations:
High Studies inconsistent (wide variation of treatment effect across Lower Quality Rating if:
Medium studies, population, interventions, or outcomes varied) - Unknown Publication Bias (e.g. pharmaceutical company sponsors study
Low on effectiveness of drug only small, positive studies found)
Studies are indirect (PICO question is quite different from the
available evidence in regard to population, intervention, comparison, Increase Quality Rating if:
or outcome) Large effect
Dose-response gradient
Studies are imprecise (when studies include few patients and few Plausible confounders or other biases increase certainty of
events, and thus have wide confidence intervals, and the results are effect
uncertain)
Endpoint Results / Outcome
Study Acronym; Author; Year
Aim of Study Patient Population Study Methods (Absolute Event Rates, P Design Limitations
Published; Location
values; OR or RR; & 95% CI)
Author: Mawet, M., et al. To evaluate a new Size: RCT Type: 280 women (141 Results: Levosert as well as Study Limitations:
levonorgestrel-releasing Levosert and 139 Mirena) Mirena users experienced a None
Year Published: 2014
intrauterine system (LNG-IUS) consequent and similar (P > RCTs
Location: Belgium Inclusion Criteria: Non- 0.1) reduction in MBL (-142.3 Lack of blinding
called Levosert((R)) for the menopausal women diagnosed Intervention: Participants were
Journal: European Journal of treatment of heavy menstrual and -146.4 mL, respectively, Lack of allocation
Contraception & Reproductive with functional heavy randomized to either Levosert in the ITT population; -150.9 concealment
bleeding (HMB) in comparison menstrual bleeding (defined as or Mirena in 1:1 ratio and
Health Care to the reference product and -151.2 mL, respectively, Stopped early for benefit
menstrual blood loss [MBL] followed for up to one year. in the PP population) after Incorrect analysis of ITT
Mirena((R)) >/= 80 mL) Menstrual bleeding loss was one year of use. Most of the Selective reporting of
evaluated using the modified decrease in MBL was reached measures (e.g., no effect
Wyatt pictogram scoring after three months (weeks 13 outcome)
Exclusion Criteria: Known or
system and recorded on a diary – 14) of treatment; it was Large losses to F/U
suspected pregnancy; a history
card. almost completely achieved Difference in important
of endometrial ablation or
curettage during the preceding after nine months (week 38) prognostic factors at baseline
three months; use of a Cu-IUD of treatment and remained
or LNG-IUS during the two stable thereafter.
months prior to screening;
current use of other hormonal
treatment (sex steroids);
endometrial polyps;
submucous myomas of any size
or intramural or subserous
14Office of Clinical Integration and EBP GRADE Table
myomas greater than 3 cm;
adenomyosis; atypical
hyperplasia or carcinoma of the
endometrium; an abnormal Pap
smear test or other evidence of
cervical malignancy; abnormal
uterine morphology; ovarian
cysts > 3 cm; a known or
suspected hormone-dependent
tumour; lower genital tract
infection; pelvic inflammatory
disease during the past three
months; abnormal liver
function; renal insufficiency;
uncontrolled hypertension;
valvular disease (including
corrections with prosthetic
valves); a body mass index
(BMI) > 30 kg/m 2 , and
hypersensitivity to device
material and/or LNG
References:
1. Mawet, M., et al. (2014). "Impact of a new levonorgestrel intrauterine system, Levosert((R)), on heavy menstrual bleeding: results of a one-year randomised controlled trial." European Journal of
Contraception & Reproductive Health Care 19(3): 169-179.
BODY OF EVIDENCE APPRAISAL TABLE FOR:
Population: Nulliparous and parous women aged 16–45 years
Modality: Liletta
Outcome: Adverse Events
Quality (certainty) of evidence for: (outcome)
High
Moderate
Low
Very Low
Risk of Bias across studies: Lower Quality Rating if: Other Considerations:
High Studies inconsistent (wide variation of treatment effect across Lower Quality Rating if:
Medium studies, population, interventions, or outcomes varied) Publication Bias (e.g. pharmaceutical company sponsors study
Low on effectiveness of drug only small, positive studies found)
Studies are indirect (PICO question is quite different from the
available evidence in regard to population, intervention, comparison, Increase Quality Rating if:
or outcome) Large effect
Dose-response gradient
Studies are imprecise (when studies include few patients and few Plausible confounders or other biases increase certainty of
events, and thus have wide confidence intervals, and the results are effect
uncertain)
15Office of Clinical Integration and EBP GRADE Table
Endpoint Results / Outcome
Study Acronym; Author; Year
Aim of Study Patient Population Study Methods (Absolute Event Rates, P Design Limitations
Published; Location
values; OR or RR; & 95% CI)
Author: Teal, S.B., et al. To assess the 5-year Size: 1751 enrollees including Type: RCT Results: Overall, 322 (18.8%) Study Limitations:
contraceptive efficacy and 1,600 females aged 16-35 and participants discontinued use None
Year Published: 2019
safety of a levonorgestrel 151 aged 36-45. as a result of an adverse RCTs
Location: University of Intervention: Women were
(LNG) 52-mg intrauterine event. The most frequent Lack of blinding
Colorado enrolled in a 4:1 ration to
system (IUS) from an ongoing event related to expulsion Lack of allocation
Journal: Obstetrics & At time of data evaluation, 495 Liletta and Mirena. After
10-year phase 3 contraceptive (n=65 [3.8%]). Only 39 2.2% concealment
Gynecology participants finished 5 years enrolling 159 of the planned
trial IUS users discontinued as a Stopped early for benefit
and 176 had entered the 400 Mirena participants, it was
result of bleeding symptoms. Incorrect analysis of ITT
seventh year of IUS use determined that this
Pelvic infection was Selective reporting of
comparator group would no
diagnosed in 14 (0.8%) measures (e.g., no effect
longer needed for non-U.S.
Inclusion Criteria: Healthy, participants. outcome)
filing, further enrollment was
sexually active (at least four Large losses to F/U
limited to LNG20.
times monthly), nulliparous and Difference in important
*Because Mirena cohort was prognostic factors at baseline
parous females aged 16-45 Subjects completed screening not large enough for
years with regular menstrual and enrollment, follow-up effectiveness calculations or
cycles (21-35 days when not during the first year including statistically meaningful
using hormones). No visits at 1, 3, 6 and 12 months comparisons, those data are
restrictions on weight or body and a telephone contact at not presented.
mass index. month 9.
Exclusion Criteria: Women Participants completed a diary
using contraception for cycle for the first 24 months for daily
control Women recently using recording of other
progestin injectable contraceptive use and the
contraception within the greatest amount of bleeding
preceding 9 months or 6 that day as none, spotting, light
months. Women who flow, normal flow, or heavy
discontinued study due to flow based on their own
pregnancy. subjective impression. After 24
months, the diary included only
additional contraceptive use.
Participants were asked at
each visit or telephone contact
beginning with month 27 to
describe their bleeding pattern
over the preceding 3 months.
16Office of Clinical Integration and EBP GRADE Table
Author: Eisenberg, D.L., et al. To assess 3-year data on the Size: 1751 nulliparous and Type: Secondary analysis of Results: Expulsion was Study Limitations:
Year Published: 2015 efficacy and safety of a new multiparous women, across 29 data from the ACCESS IUS reported in 62 (3.5%) None
52-mg levonorgestrel clinical sites in USA multicenter, Phase 3, open- participants, most (50 Non-Randomized Studies
Location: Medicines360, San [80.6%]) during the first year Failure to develop and
Francisco, CA intrauterine contraceptive label clinical trial
(LNG20) designed for up to 7 of use. Of women who apply appropriate eligibility
and Allergan, Irvine, CA Of the 1751 women enrolled, discontinued LNG20 and criteria
years use 1714 (97.9%) had successful Intervention: Evaluated
Journal: Contraception desired pregnancy, 86.8% Flawed measurement of
placement: 14 (0.8%) of these bleeding patterns for women conceived spontaneously both exposure and outcome
women discontinued prior to using a daily diary completed within 12 months. Pelvic Failure to adequately
90 days for non-bleeding- by participants for the first 2 infection was diagnosed in 10 control confounding
related complaints leaving years and by questionnaire (0.6%) women. Only 26 (1.5%) Incomplete or
1700 women in the analysis. every 3 months thereafter. LNG20 users discontinued inadequately short follow-up
Assessed amenorrhea rates due to bleeding complaints.
over 3 years and the
Inclusion Criteria: Healthy, proportion of subjects with
non-pregnant, sexually active, infrequent, frequent, prolonged
nulliparous and parous and irregular bleeding per 90-
women aged 16–45 years who day reference period over 2
desired a hormonal years for the entire study
IUS for contraception. population as well as
Participants had to report comparing nulliparous and
regular menstrual cycles every parous women and obese and
21–35 days with a variation of non-obese women
typical cycle length of no more
than 5 days. Women with
successful IUS placement
Exclusion Criteria: Women
using contraception for cycle
control Women recently using
progestin injectable
contraception within the
preceding 9 months or 6
months.
References:
1. Eisenberg, D. L., et al. (2015). "Three-year efficacy and safety of a new 52-mg levonorgestrel-releasing intrauterine system." Contraception 92(1): 10-16.
2. Teal, S. B., et al. (2019). "Five-Year Contraceptive Efficacy and Safety of a Levonorgestrel 52-mg Intrauterine System." Obstetrics & Gynecology 133(1): 63-70.
BODY OF EVIDENCE APPRAISAL TABLE FOR:
Population: Parous Women between 18 – 38 years old
Modality: Mirena
Outcome: Adverse Events
17Office of Clinical Integration and EBP GRADE Table
Quality (certainty) of evidence for: (outcome)
High
Moderate
Low
Very Low
Risk of Bias across studies: Lower Quality Rating if: Other Considerations:
High Studies inconsistent (wide variation of treatment effect across Lower Quality Rating if:
Medium studies, population, interventions, or outcomes varied) - Unknown Publication Bias (e.g. pharmaceutical company sponsors study
Low on effectiveness of drug only small, positive studies found)
Studies are indirect (PICO question is quite different from the
available evidence in regard to population, intervention, comparison, Increase Quality Rating if:
or outcome) Large effect
Dose-response gradient
Studies are imprecise (when studies include few patients and few Plausible confounders or other biases increase certainty of
events, and thus have wide confidence intervals, and the results are effect
uncertain)
Endpoint Results / Outcome
Study Acronym; Author; Year
Aim of Study Patient Population Study Methods (Absolute Event Rates, P Design Limitations
Published; Location
values; OR or RR; & 95% CI)
Author: Andersson, K., et al. To investigate more Size: 2758 women were Type: RCT Results: The 60-month Study Limitations:
Year Published: 1994 extensively a study between allocated, 937 had a Nova T cumulative gross expulsion None
LNG-IUD and Nova T during and 1821 had an LNG-IUD Intervention: Women were rate was 5.8 in the LNG-IUD RCTs
Location: Finland and Sweden Lack of blinding
five years of use inserted. randomized to treatment by group. Most expulsions were
Journal: Contraception noted during the first months Lack of allocation
Nova T or LNG-IUD. A
standardized interview was after insertion. concealment
Inclusion Criteria: Healthy Stopped early for benefit
women, 18-38 years old and at performed at admission and at
every follow-up visit, which Incorrect analysis of ITT
least one previous pregnancy. The 60-month gross removal Selective reporting of
was planned after 3 and 12 rates for pelvic inflammatory
months and then yearly up to measures (e.g., no effect
Exclusion Criteria: Women disease was 0.8. outcome)
five years. Furthermore, during
with a history of ectopic the first 12 months, all women Large losses to F/U
pregnancy, who were breast- were requested to note Difference in important
feeding, or had used injectable bleeding patterns continuously prognostic factors at baseline
hormones for contraception on a specially designed chart. – Baseline characteristics note
during the preceding 12 included
months were excluded.
References:
1. Andersson, K., et al. (1994). "Levonorgestrel-releasing and copper-releasing (Nova T) IUDs during five years of use: a randomized comparative trial." Contraception 49(1): 56-72.
BODY OF EVIDENCE APPRAISAL TABLE FOR:
Population: Nulliparous and parous women aged 16–45 years
Modality: Levosert (Liletta in US) vs. Mirena
Outcome: Adverse Events
18Office of Clinical Integration and EBP GRADE Table
Quality (certainty) of evidence for: (outcome)
High
Moderate
Low
Very Low
Risk of Bias across studies: Lower Quality Rating if: Other Considerations:
High Studies inconsistent (wide variation of treatment effect across Lower Quality Rating if:
Medium studies, population, interventions, or outcomes varied) Publication Bias (e.g. pharmaceutical company sponsors study
Low on effectiveness of drug only small, positive studies found)
Studies are indirect (PICO question is quite different from the
available evidence in regard to population, intervention, comparison, Increase Quality Rating if:
or outcome) Large effect
Dose-response gradient
Studies are imprecise (when studies include few patients and few Plausible confounders or other biases increase certainty of
events, and thus have wide confidence intervals, and the results are effect
uncertain)
Endpoint Results / Outcome
Study Acronym; Author; Year
Aim of Study Patient Population Study Methods (Absolute Event Rates, P Design Limitations
Published; Location
values; OR or RR; & 95% CI)
Author: Mawet, M., et al. To evaluate a new Size: RCT Type: 280 women (141 Results: Adverse events were Study Limitations:
Year Published: 2014 levonorgestrel-releasing Levosert and 139 Mirena) reported with similar None
intrauterine system (LNG-IUS) frequency between the two RCTs
Location: Belgium Inclusion Criteria: Non- groups. 15 subjects Lack of blinding
called Levosert((R)) for the
Journal: European Journal of menopausal women diagnosed Intervention: Participants were discontinued participation in Lack of allocation
treatment of heavy menstrual
Contraception & Reproductive with functional heavy randomized to either Levosert the study due to an adverse concealment
bleeding (HMB) in comparison
Health Care menstrual bleeding (defined as or Mirena in 1:1 ratio and event (AE). Six women in the Stopped early for benefit
to the reference product
menstrual blood loss [MBL] followed for up to one year. Levosert group and 5 in the Incorrect analysis of ITT
Mirena((R))
>/= 80 mL) Menstrual bleeding loss was Mirena group spontaneously Selective reporting of
evaluated using the modified expelled the device. 1 woman measures (e.g., no effect
Exclusion Criteria: Known or Wyatt pictogram scoring in the Levosert group left the outcome)
suspected pregnancy; a history system and recorded on a diary study because of amenorrhea Large losses to F/U
of endometrial ablation or card. and 3 in the Mirena group did Difference in important
curettage during the preceding so for arterial hypertension, prognostic factors at baseline
three months; use of a Cu-IUD ovarian cyst, and pelvic pain,
or LNG-IUS during the two respectively.
months prior to screening;
current use of other hormonal Users complained of pain
treatment (sex steroids); after insertion of the IUS with
endometrial polyps; the same frequency in both
submucous myomas of any size Levosert (7.1%) and Mirena
or intramural or subserous (6.5%).
myomas greater than 3 cm;
adenomyosis; atypical
hyperplasia or carcinoma of the
endometrium; an abnormal Pap
smear test or other evidence of
19Office of Clinical Integration and EBP GRADE Table
cervical malignancy; abnormal
uterine morphology; ovarian
cysts > 3 cm; a known or
suspected hormone-dependent
tumour; lower genital tract
infection; pelvic infl ammatory
disease during the past three
months; abnormal liver
function; renal insuffi ciency;
uncontrolled hypertension;
valvular disease (including
corrections with prosthetic
valves); a body mass index
(BMI) > 30 kg/m 2 , and
hypersensitivity to device
material and/or LNG
References:
1. Mawet, M., et al. (2014). "Impact of a new levonorgestrel intrauterine system, Levosert((R)), on heavy menstrual bleeding: results of a one-year randomised controlled trial." European Journal of
Contraception & Reproductive Health Care 19(3): 169-179.
BODY OF EVIDENCE APPRAISAL TABLE FOR:
Population: Nulliparous and parous women aged 16–45 years
Modality: Liletta
Outcome: Average micrograms (mcg) per day release
Quality (certainty) of evidence for: (outcome)
High
Moderate
Low
Very Low
Risk of Bias across studies: Lower Quality Rating if: Other Considerations:
High Studies inconsistent (wide variation of treatment effect across Lower Quality Rating if:
Medium studies, population, interventions, or outcomes varied) - Unknown Publication Bias (e.g. pharmaceutical company sponsors study
Low on effectiveness of drug only small, positive studies found)
Studies are indirect (PICO question is quite different from the
available evidence in regard to population, intervention, comparison, Increase Quality Rating if:
or outcome) Large effect
Dose-response gradient
Studies are imprecise (when studies include few patients and few Plausible confounders or other biases increase certainty of
events, and thus have wide confidence intervals, and the results are effect
uncertain)
Endpoint Results / Outcome
Study Acronym; Author; Year
Aim of Study Patient Population Study Methods (Absolute Event Rates, P Design Limitations
Published; Location
values; OR or RR; & 95% CI)
20Office of Clinical Integration and EBP GRADE Table
Author: Creinin, M.D., et al. To understand the potential Size: 100 samples including 64 Type: Secondary analysis of Results: An average initial Study Limitations:
Year Published: 2016 duration of action for Liletta(R), within 90-day intervals through data from the ACCESS IUS release rate of 19.5 mcg/day None
we conducted this study to 900 days and 36 samples multicenter, Phase 3, open- was calculated that decreased Non-Randomized Studies
Location: University of Failure to develop and
California, Davis estimate levonorgestrel (LNG) within 180-day intervals label clinical trial to 17.0, 14.8, 12.9, 11.3 and
release rates over 9.8 mcg/day after 1,2,3,4, and apply appropriate eligibility
Journal: Contraception approximately 5(1/2) years of 5 years, respectively The 5- criteria
Inclusion Criteria: Healthy, Flawed measurement of
product use non-pregnant, sexually active, year average release rate is
Intervention: Sponsor 14.7 mcg/day. both exposure and outcome
nulliparous and parous randomly selected samples Failure to adequately
women aged 16–45 years who within 90-day intervals through control confounding
desired a hormonal 900 days (approximately 2.5 Incomplete or
IUS for contraception. years) and 180-day intervals inadequately short follow-up
Participants had to report for the remaining duration
regular menstrual cycles every through 5.4 years (1980 days.
21–35 days with a variation of Sampling included the potential
typical cycle length of no more for different lots of product to
than 5 days. Women with be included, but all products
successful IUS placement met the same lot release
specifications and had similar
Exclusion Criteria: Women content in vitro release results.
using contraception for cycle Sponsor also performed an
control Women recently using initial levonogestrel content
progestin injectable analysis using 10 randomly
contraception within the selected samples from a single
preceding 9 months or 6 lot.
months. Women who
discontinued study due to Study used the levongestrel
pregnancy. content of all samples using
liquid chromatography to
estimate the average in vivo
drug release rate for the
duration of use of the
products. The drug content of
each sample was plotted and
analyzed during the duration of
exposure with an exponential
best-fit regression to calculate
the average rate of change of
system content over time
based on a monoexponential
decay content model.
References:
1. Creinin, M. D., et al. (2016). "Levonorgestrel release rates over 5 years with the Liletta(R) 52-mg intrauterine system." Contraception 94(4): 353-356.
21Office of Clinical Integration and EBP GRADE Table
BODY OF EVIDENCE APPRAISAL TABLE FOR:
Population: Nulliparous and parous women
Modality: Mirena
Outcome: Average LNG serum concentration over 3 years of use
Quality (certainty) of evidence for: (outcome)
High
Moderate
Low
Very Low
Risk of Bias across studies: Lower Quality Rating if: Other Considerations:
High Studies inconsistent (wide variation of treatment effect across Lower Quality Rating if:
Medium studies, population, interventions, or outcomes varied) Publication Bias (e.g. pharmaceutical company sponsors study
Low on effectiveness of drug only small, positive studies found)
Studies are indirect (PICO question is quite different from the
available evidence in regard to population, intervention, comparison, Increase Quality Rating if:
or outcome) Large effect
Dose-response gradient
Studies are imprecise (when studies include few patients and few Plausible confounders or other biases increase certainty of
events, and thus have wide confidence intervals, and the results are effect
uncertain)
Endpoint Results / Outcome
Study Acronym; Author; Year
Aim of Study Patient Population Study Methods (Absolute Event Rates, P Design Limitations
Published; Location
values; OR or RR; & 95% CI)
Author: Apter, D., et al. To assess the pharmacokinetics Size: 742 women Type: RCT Results: The average LNG Study Limitations:
and pharmacodynamics of serum concentration over 3 None
Year Published: 2014
levonorgestrel intrauterine years of use was 218 ng/L for RCTs
Location: Sweden Inclusion Criteria: Women in Intervention: Participants were
system (LNG-IUS) 13.5 mg and LNG-IUS 20 mug/24 h, Lack of blinding
Journal: Fertility & Sterility whom a placement was at least randomized to Levonorgestrel
LNG-IUS 19.5 mg (total Lack of allocation
attempted intrauterine system 13.5 mg,
content) concealment
LNG-IUS 19.5 mg, or LNG-IUS
Stopped early for benefit
20 mug/24 h (total content 52
Incorrect analysis of ITT
mg).
Selective reporting of
measures (e.g., no effect
A model developed in outcome)
NONMEM together with Large losses to F/U
software R was used to Difference in important
calculate the release rates of prognostic factors at baseline
LNG from LNG-IUS 13.5 mg – Baseline characteristics not
using ex vivo residual content included
data from the phase III study.
The dataset used for the model
development included 763
LNG-IUS 13.5 mg residual
content measurements
obtained at different time
points over 3 years form
22You can also read