Original Article The prevalence of gastro-esophageal reflux in asthmatic children
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Int J Clin Exp Med 2016;9(6):10394-10403
www.ijcem.com /ISSN:1940-5901/IJCEM0021366
Original Article
The prevalence of gastro-esophageal
reflux in asthmatic children
Eithar Karim El-Adham1, Khaled Hussein Taman2, Abdel-Aziz Mohamed El-Nekeidy3, Sahar El-Sayed
Abdel-Wahab4
1
Department of Radioisotopes, Nuclear Research Center, Atomic Energy Authority, Dokki 12311, Giza, Egypt;
2
Institute of Postgraduate Childhood Studies, Ain Shams University, Cairo, Egypt; 3Faculty of Medicine, Alexandria
University, Alexandria, Egypt; 4Anfushi Children Hospital, Ministry of Health, Alexandria, Egypt
Received December 7, 2015; Accepted March 19, 2016; Epub June 15, 2016; Published June 30, 2016
Abstract: Gastro-esophageal reflux disease (GERD) is the most common esophageal disorder in children. It causes
various pulmonary manifestations and bronchial asthma is one of them. The study aims to assess the prevalence
of GERD in a group of moderate persistent or severe persistent asthma and to evaluate the clinical response of
asthma to anti-reflux treatment. The study included 38 cases and found a significant difference in both symptoms
related to asthma and those related to GERD throughout the study. Also, there was a significant increase in forced
expiratory volume in one minute (FEV1) and a significant decrease in the frequency of use of rescue medication.
Furthermore, GERD has a role in worsening asthma symptoms and there will be potential benefit of anti-reflux
therapy on asthma. Patients with persistent asthma, should be screened for reflux, if no diagnostic method can be
performed for whatever reason, trial therapy with Proton pump Inhibitors (PPIS) is indicated. In conclusion, patients
with persistent asthma should be screened for reflux and receive treatment for better control of their asthma.
Keywords: Bronchial asthma, gastro esophageal reflux disease
Introduction The association of asthma with gastroesopha-
geal reflux disease has attracted particular
Asthma is a chronic inflammatory disorder of attention because about half of the patients
the airways. In susceptible individuals, this in- with asthma have GERD [4].
flammation causes recurrent wheezing, breath-
lessness, chest lightness and cough, particu- Proper management of GERD is important for
larly at night and/or in the early morning. These asthma control [5].
symptoms associated with widespread but va-
riable airflow it is at least particularly reversi- GERD is a common condition in the pediatric
ble either or with treatment. The inflammation population. It was clear that reflux plays a role
causes an increase in airway responsiveness in worsening of asthma symptoms and the
to a variety of stimuli [1]. potential effect of anti-reflux therapy on asthma
needs further investigations [6].
It is important to include GERD in the differen-
tial diagnosis with unexplained or refractory
Patients and methods
otolayngologic and respiratory complaints. Ma-
ny children with extra-esophageal don’t have
All studied children cases proved to have GERD
typical GERD symptoms making the diagnosis
and they received both prokinetic drug Dom-
difficult [2].
peridone (0.6 mg/1 g) and proton pump inhibi-
GERD can cause various pulmonary manifesta- tor, Omeprazole in a dose 0.7-3 mg/1 cg 1 day
tions as chronic cough, bronchial Asthma bron- for one and half month. This study was approv-
chitis, pneumonia and interstial fibrosis. Out of ed by the Ethical Committee of the Institute
these, bronchial asthma is one of the most of Postgraduate Childhood Studies, Ain Shams
common manifestations of GERD [3]. University. All participants were guaranteed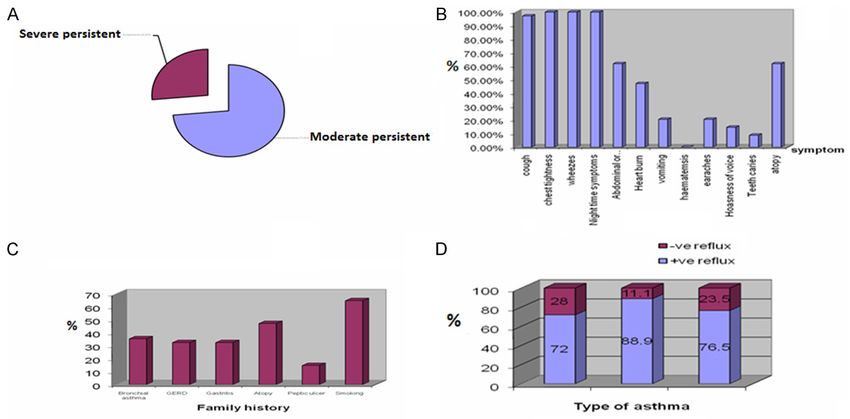
Gastroesophageal reflux in asthmatic children
Figure 1. Sex distribution of patients according to asthma severity.
confidentiality, and only the principal investiga- - Full clinical examination and calculation of
tor has full access to the data. body mass index (BMI).
The studied patients ware 16 males (42.1%) Investigations
and females (57.9%). Twenty eight (28) patients Laboratory investigations
(73.7%) had moderate persistent bronchial
asthma, while 10 patients (26.3%) had severe Serum gastrin (G-17) level was determined by
persistent bronchial asthma. radioimmunoassay using a commercial kit
(Diagnosis Products Corporation, Los Angeles),
All children were subjected to: with total coefficients of variation (CV) for two
controls ranged from 4 to 10% according to the
Full history including the following: previous literature [7].
- A) History of asthma: A - Pulmonary function test by means of spi-
rometry
- Asthma symptoms
B - Chest X-ray.
- History of use of anti-asthma therapy C - Barium swallow was done using barium
sulphate.
- B) GERD symptoms
D - Upper gastro-intestinal endoscopy using a
- C) History of other extra-esophageal symptoms flexible fiberoptic cndoscope (Olympus XPE
or signs of GERD such as recurrent ear infection type GIF).
hoarseness or dental caries.
All studied children proved to have GERD
received in addition to their anti-asthma thera-
- D) History of drug intake other than anti-
py; both prokinitic drug Dompevidone (0.6 mg
asthma therapy.
kg dose), and proton pump inhibitor (1*1*1)
Omeprazole in a dose of 0.7-3. co mg/kg/day
- E) Family History of asthma or other atopic
for one and half month.
diseases; in-addition to family history of peptic
ulcer and GERD. Follow up scheme: Follow up was done weekly
in order to assess the progress of illness,
- F) History of smoking either active or passive. patients and compliance with medication, and
the final assessment was done after 6 weeks
- The patients were classified according to the of treatment with anti-reflux medication. Pul-
GINA (asthma) guidance of asthma manage- monary function forced expiratory volume in
ment into moderate or severe persistent bron- one minute (FEV1) by spirometry was perform-
chial asthma. ed at 4 and 6 weeks.
10395 Int J Clin Exp Med 2016;9(6):10394-10403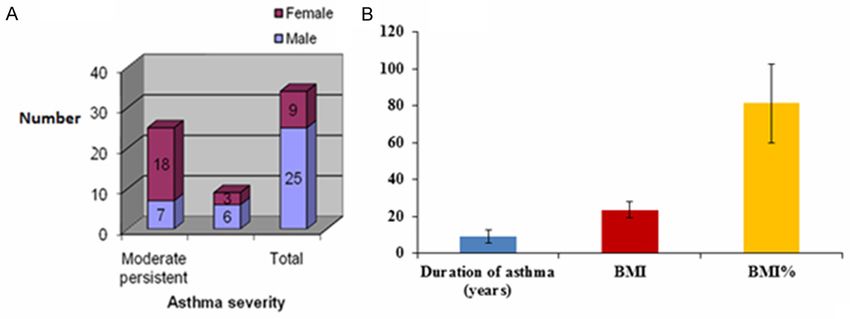
Gastroesophageal reflux in asthmatic children Figure 2. Chest score throughout the study (A), abdominal score throughout the study (B). 26 patients (76.5%) of the studied patients (34 patients) revealed GER duringthe barium study. 18 of them were patients with moderate persistent bronchial asthma while 8 patients were patients with severe persistent bronchial asthma. GER was docu- mented in 8 patients (23.5%) neither by barium study, nor by upper GI endoscopy (C) and (D). Figure 3. Change in FEV1 across time. Chi-Square =47.05*(P
Gastroesophageal reflux in asthmatic children
Table 1. Comparison between FEV1 throughout the to 3 (2-5 times/day) and reached 2 (1-3
study times/day) after 6 weeks of treatment
FEV1 2-FEV1 1 FEV1 3-FEV1 1 FEV1 3-FEV1 2 (Figure 4A and 4B).
Z -3.52 -4.80 -4.91
Asymp. Sig. 0.000* 0.000* 0.000*
A significant difference was found between
*Significance PGastroesophageal reflux in asthmatic children Figure 4. Change in need for rescue medication. Chi-square =61.79* at P
Gastroesophageal reflux in asthmatic children
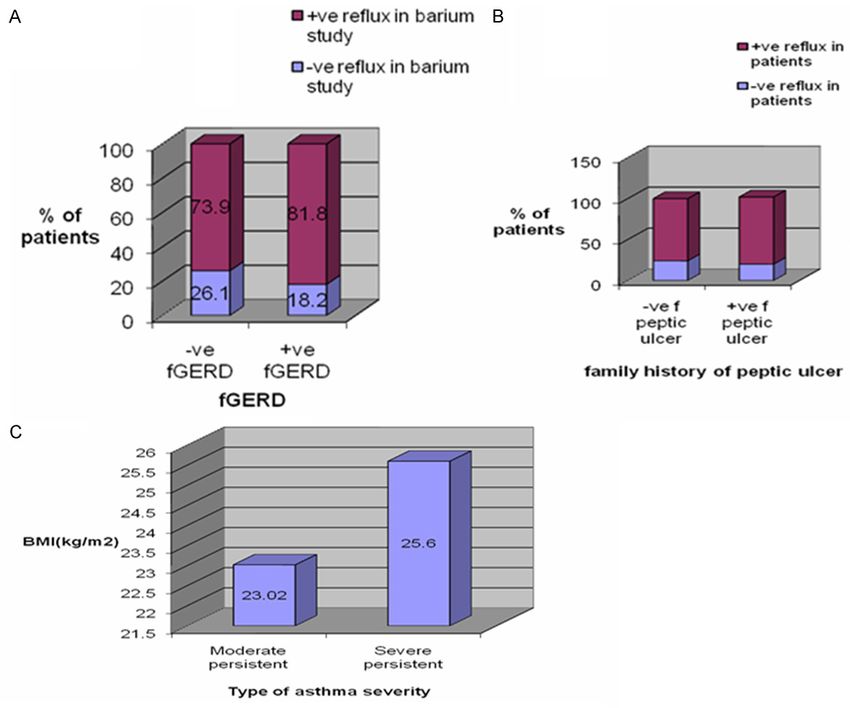
Figure 5. Patients with mod-
erate persistent bronchial
asthma and severe persis-
tent bronchial asthma; and
the prevalence of GER (A, B).
The prevalence of GER in the
studied patients and family
history of peptic ulcer (C).
from asthma with the prevalence increasing by cluding PH monitoring endoscopy and radiologi-
50% each decade [9]. In children, asthma is the cal manipulations [14].
most common childhood illness worldwide [10].
Other studies reported that GERD was diag-
In individuals with severe asthma, co-morbidi- nosed in 75% of children with chronic asthma
ties are common, and the most prevalent is who were refractory to medical treatment [15].
GERD [11].
Retrosternal pain was reported in 65.8% of the
According to a global definition, GERD can patients in our study, heart burn in 50%, 28.9%,
cause esophageal and extra-esophageal symp- had vomiting and none of them had dysphagia.
toms, which can co-exist or not in the same These results arc near to the results reported in
individual. Respiratory manifestations of GERD other studies and the older age of our cases
represent one of the most prevalent and chal- helped them to describe their symptoms.
lenging of these extra-esophageal symptoms
[12]. Epigastric discomfort, regurgitation and dys-
phagia were reported in 77%, 55% and 24% of
According to our results, GERD was present in adult patients with asthma, respectively, and
78.9% of the patients with moderate-severe these symptoms were significantly more fre-
persistent bronchial asthma. These rates are quent compared to healthy controls. Although
comparable with the upper limits reported in some children do not have GERD related symp-
the literature [13]. toms and this condition is likely to result from
that adults describe their symptoms better
Differences in reporting the incidence of GERD than children. So GERD symptoms may be less
result from differences in diagnostic tools in- prevalent in the childhood than in the adult-
10399 Int J Clin Exp Med 2016;9(6):10394-10403Gastroesophageal reflux in asthmatic children
Table 3. Comparing abdominal score throughout the recommend consideration of evaluation for
study GERD in patients who have poorly con-
Asymp. Sig.* trolled asthma. Especially with nighttime
Compared scores Z test symptoms, even in the absence of GERD
(2-tailed)
Abdominal score 1-abdominal score 2 0.000 1.000 symptoms or if GERD is present, irealment
Abdominal score 1-abdominal score 3 1.589 0.112 recommendations include using of a PPI
[19].
Abdominal score 1-abdominal score 4 4.115 0.000
Abdominal score 1-abdominal score 5 4.736 0.000 Our results showed that after treatment
Abdominal score 1-abdominal score 6 4.724 0.000 with Omeprazole and Domperidone there
Abdominal score 1-abdominal score 7 4.724 0.000 was a significant improvement of asthma
Abdominal score 2-abdominal score 3 1.930 0.054 regarding symptoms with a significant
Abdominal score 2-abdominal score 4 4.337 0.000 decrease in the occurrence of symptoms
Abdominal score 2-abdominal score 5 4.736 0.000 throughout the study, (for the whole stud-
Abdominal score 2-abdominal score 6 4.724 0.000 ied patients; PGastroesophageal reflux in asthmatic children
Table 4. Comparison of fasting and postprandial gastrin levels included well treated asthmatics
in moderate and severe persistent asthma with mild or moderate persis-
Fasting level Post prandial tent asthma and there was no
P value improvement in daily asthma
of gastrin level of gastrin
Moderate persistent asthma 67.56 ± 11.23 77.86 ± 9.73Gastroesophageal reflux in asthmatic children
od can be performed for whatever reason; trial [10] Gibson PG, Henry RL, Coughlan JL. fas-
therapy with PPIs is indicated, as the most troeophageal reflux treatment for asthma in
effective treatment with good tolerance. adults and children. Cochrane Database Syst
Rev 2003; CD001496.
Disclosure of conflict of interest [11] Gopal B, singhal P, Gaul SN. Gastroesophageal
reflux disease in bronchial asthma and the re-
None. sponse to omeprazole. Asian Pac J Allergy
Immunol 2005; 23: 29-34.
Address correspondence to: Eithar Karim El-Adham, [12] Hancox RJ, Milne BJ, Poulton R, Taylor DR,
Department of Radioisotopes, Nuclear Research Greene JM, Melachaln CR, Cowan JO, Flannery
Center, Atomic Energy Authority, Dokki 12311, Giza, EM, Herbison GP, Sears MR. Sex differences in
Egypt. Tel: +2 01222226329; Fax: +2 02 37493042; the relation between body mass index and
asthma and atopy in a birth cohort. Am J
E-mail: saso_d35@yahoo.com
Respire Crit Care Med 2005; 171: 440-5.
References [13] Kijander TO, Harding SM, Field SK, Stein MR,
Nelson H, Ekelund J. Effects of esomeprazole
[1] Aye M, Sivasli E, Bayraktarouglu Z, Ceylan H, 40 mg twice daily on asthma: a randomized
Coskun Y. Association of asthma with gas- placebo-controlled trial. Am J Respir Crit Care
troesohageal reflux disease in children. J Chin Med 2006; 173: 1091-7.
Med Assoc 2004; 67: 63-66. [14] Leggett JJ, Johnston Br, Mills M, Gamble J,
[2] Bateman ED, Boushey HA, Bousquet J, Busse Heaney GL. Prevalence of gastroesophageal
WW, Clark TJ, Pauwels RA, Pedersen SE; GOAL reflux in difficult asthma. Relationship to asth-
ma outcome. Chest 2005; 127: 1227-31.
Investigators Group. Can guide line-defined
[15] LIndstedet G, Olbe L, Kilander AF, Armbrecht U,
asthma control be achieved? The gaining
Runsteen JR, Lundberg PA. Analytical and clini-
Optimal be asthma control study. Am J Respir
cal evaluation of a radioimmunoassay for gas-
Crit Care Med 2008; 170: 836-44.
trin. Clin Chem 1985; 31: 76-82.
[3] Bisaccioni C, Aun Mv, Kalil J, Agondi Rc,
[16] Littner MR, Leang FM, Ballard ED, Huang B;
Giavina-Bianchi P. Co-morbidities in severe
Samra NK Lansoprazole Asthma Study Group.
ashma: frequency of rhinitis, masal polyposis,
Effect of 24 weeks of lansoprazole therapy on
gastroesophageal reflux disease, vocal cord
Asthma symptoms, exacerbations quality of
dysfunction and bronchiectasis. Clinics 2009;
life and pulmonary function in adult Asthmatic
64: 769-73.
patients with acid reflux syptoms. Chest 2005;
[4] Braman SS. The global burden of Asthma.
128: 1128-35.
Chest 2003; 130 Suppl: 45-125.
[17] Macie JK, Jalenta W. Serum gastrin concentra-
[5] Carloc C, Anna F, Alessandra A, Carlos Desiree tions in children with primary gastro esopha-
Z, Giulio DF. Asthma and gastroesophageal geal reflux and gastro esophageal reflux sec-
reflux disease. Effect of long term pantopra- ondary to cow’s milk allergy. Adv Med Sci
zole therapy. World J Gastroenterol 2005; 11: 2011; 56: 186-192.
7657-60. [18] Malaty HM, Fraley JK, Abudayyeh S, Fairly KW,
[6] Devault K. A balancing view: empiric proton Javed US, Aboul-Fotouh H, Mattek N, Gilger
pump inhibitor therapy remains the cheap but MA. Obesity and gastroesophageal reflux dis-
not by a knock out. Am J Gastroenterol 2006; ease and gastroesophageal reflux symptoms
101: 10-11. in children. Clin Exp Gastroenterol 2009; 2: 31-
[7] Fass R, Achem SR, harding S, Mital RK, Quigley. 36.
Review article: supra-esophageal manifesta- [19] Martinez FD, Wright A, Taussig LM, Holberg CJ,
tions of gastroesophageal reflux disease and Halonen M, Morgan WJ. Asthma and Wheezing
the role of night-time gasteroesophageal re- in the first six years of life. The Group Health
flux. Aliment pharmacol Ther 2004; 20: 26-38. Medical Associates. N Eng J Med 1995; 332:
[8] Field A. Statistical analysis for univariate analy- 133-138.
sis. In: Field A, editor. Discovering statistics us- [20] Mastronade JG, Anthonisen NR, Castro M,
ing spss. 2nd edition. London, California, New Holbrook JT, Lene FT, Teague WG, Wise RA. ef-
Delhi: sage publications l td; 2006. pp. 143- ficacy of esomeprazole for treatment of poorly
217. controlled asthma: a randomized controlled
[9] Galmiche JP, Zerbib F, Varannes SB. Review ar- trail. N Eng J Med 2009; 360: 1487-99.
ticle: respiratory manifestations of gastro- [21] Mathew JL, Singh M, Mittal SK. Gastro-
esophageal reflux disease. Coated form the oesophageal reflux and bron chial asthma: cur-
internet 2008; http//www.medscape.comvei- rent status and future directions. Postgrad
warticle/571744. Med J 2004; 80: 701-5.
10402 Int J Clin Exp Med 2016;9(6):10394-10403Gastroesophageal reflux in asthmatic children
[22] Orenstein S, Peters J, Khan S, Youssef N, [27] Stores G, Ellis AJ, Wiggs L. Sleep and psycho-
Hussain SZ. The esophagus. In: Behrman RE, logical distrbande in noeturnal asthma. Arch
Kliegman RM, Jenson HB, editors. Nelson text Dis Childhood 1998; 78: 413-9.
book of pediatries. 17th edition. Philadelphia: [28] Tessier DJ. Medical, surgical and Endosopic
W.B. Saunders Company; 2004. pp. 1217- management of gastroesophangeal reflux dis-
1227. ease. Permente J 2009; 13: 30-36.
[23] Scarupa MD, Mori N And Caning GJ. Gas- [29] Thakkar K, Boatright RO, Gilger MA, Elserag
troesophageal reflux disease in children with HB. Gastroesophageal reflux and asthma in
treatment implications. Pediatr Drugs 2005; 7: children: a systematic review. Pediatrics 2010;
177-86. 125: 25-30.
[24] Sopo SM, Radzik D, Calvani M. Does treatment [30] Tucci F, Resti M, Fontana R, Novembre E, Lanii
with proton pump inhibitors for gastroesopha- CA, Vicrucci A. Jastroesophageal reflux and
geal reflux disease (Gerd) improve asthma bronchial asthma: prevalence and effeut of
symptoms in chidren withashma and Gerd? cisapridetherapy, J Pediatr Gastmenlerol Nutr
A systematic review. J Investing Allergol Clin 1993; 17: 265-70.
Immunol 2009; 19: 1-5. [31] Vakil N, van Zanten SV, Kahrilas P, Dent J,
[25] Stirling RG, Chung KF. Severer asthma: defini- Jones R; Global Consensus Group. The Mon-
tion and mechanisms. Allergy 2001; 56: 825- treal Definition and classification of gastro-
40. esophageal reflux disease: a global evidence-
[26] Stordal K, Joha Nnesdottir GH, Bentsen BS, based consensus 2006; 101: 1900-20; quiz
Carlsen KC, Sandvikl L. Asthma and overweig- 1943.
ht are associated with symptoms of Gastro- [32] Vezi MF. Atypical manifestations of gastro-
oesophageal reflux. Acta Paediatr 2006; 95: esophageal reflux disease. Med Gen Med
1197-201. 2005; 7: 25-6.
10403 Int J Clin Exp Med 2016;9(6):10394-10403You can also read