Pathology pathologie - Digital Pathology - Revue canadienne de - Amazon S3
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Canadian Journal of Volume 10 | Issue/numéro 3
pathology
pathologie Revue canadienne de
Digital Pathology
Courtesy: Leica Biosystems
PM 43490512
www.cap-acp.org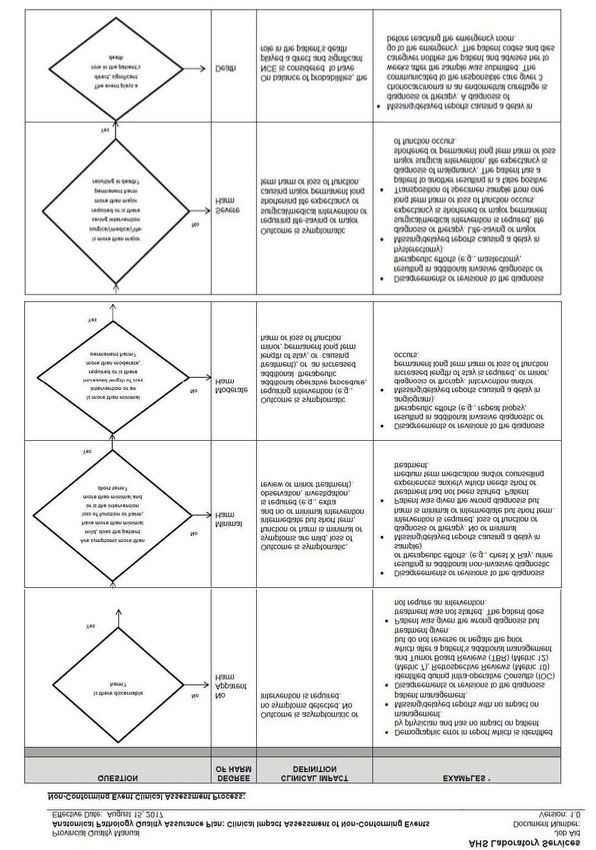
KEYTRUDA:
Pr ®
NOW FOR PATIENTS
WITH METASTATIC NSCLC
WITH NO PRIOR SYSTEMIC
CHEMOTHERAPY TREATMENT
FOR METASTATIC NSCLC1
NEW NSCLC INDICATION MELANOMA
KEYTRUDA® (pembrolizumab) as monotherapy is indicated KEYTRUDA® is indicated for the treatment
for the treatment of metastatic NSCLC in adults whose of patients with unresectable or metastatic
tumours have high PD-L1 expression [Tumour Proportion melanoma who have not received prior
Score (TPS) ≥50%] as determined by a validated test, with treatment with ipilimumab. Subjects with
no EGFR or ALK genomic tumour aberrations, and no prior BRAF V600 mutant melanoma may have
systemic chemotherapy treatment for metastatic NSCLC.1 received prior BRAF inhibitor therapy.1
Pembrolizumab is RECOMMENDED as
a FIRST-line treatment of metastatic NSCLC,
in patients with PD-L1+ expression ( TPS ≥50%)
and EGFR-, ALK- in the NCCN guidelines.2
Please see the NCCN guidelines for complete recommendations
Clinical use: • Other immune-mediated adverse events, • Has not been studied in patients with
Safety and efficacy of KEYTRUDA® in including uveitis, arthritis, myositis, bullous moderate or severe hepatic impairment
pediatric patients have not been established. pemphigoid, myasthenic syndrome, vasculitis, • Has not been studied in patients with
Guillain-Barré syndrome, hemolytic anemia, severe renal impairment
Relevant warnings and precautions:
pancreatitis, and partial seizures arising • Monitor liver and thyroid function tests
• Immune-mediated adverse reactions in a patient with inflammatory foci in and electrolytes during treatment
including: brain parenchyma
Pneumonitis For more information:
Solid organ transplant rejection Before prescribing KEYTRUDA®, please
Colitis Myocarditis
Hepatitis consult the product monograph available at
• Severe infusion-related reactions, including https://health-products.canada.ca/dpd-bdpp/
Nephritis and renal dysfunction hypersensitivity and anaphylaxis
Endocrinopathies including hypophysitis, • Embryofetal toxicity index-eng.jsp for important information
type 1 diabetes mellitus and thyroid relating to adverse reactions, drug interactions
• Not recommended in pregnant women and dosing information which have not been
disorders • In nursing women, a decision should be
Severe skin reactions, including discussed in this document.
made whether to discontinue breast-feeding
Stevens-Johnson syndrome and toxic or KEYTRUDA® taking into account the The product monograph is also available
epidermal necrolysis benefit of breast-feeding for the child by calling us at 1-800-567-2594 or by email
and the benefit of KEYTRUDA® therapy at medinfocanada@merck.com.
for the woman
ONCO-1226035-0000
ALK=anaplastic lymphoma kinase; EGFR=epidermal growth factor receptor; NCCN=National Comprehensive Cancer Network; NSCLC=non-small cell lung carcinoma;
PD-L1=programmed cell death ligand 1; TPS=tumour proportion score
References: 1. KEYTRUDA® Product Monograph. Merck Canada Inc. July 20, 2017. 2. National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology.
Non-small cell lung cancer. Version 5.2017. March 16, 2017.
®
Merck Sharp & Dohme Corp. Used under license.
© 2017 Merck Canada Inc. All rights reserved.
Canadian Journal of
Volume 10 | issue 3
pathology
Official Publication of the Canadian Association of Pathologists
EDitoR-iN-ChiEF table of Contents
4
George M Yousef MD, PhD, FRCPC
EDitoR EMERitUS Letter from the Editor-in-Chief: Publicly available data: a game
J. Godfrey Heathcote MA, MB, BChir, PhD, FRCPC changer in modern research?
9
FoUNDiNg EDitoR
Molecular Pathology Corner: Molecular testing in gastrointestinal
Jagdish Butany MBBS, MS, FRCPC
stromal tumours – we’ve got the GIST of it, now let’s go forward.
aSSoCiatE EDitoR Authors: Caroline S Allen and Catherine J Streutker MD, MSc, FRCPC.
17
Martin J. Trotter MD, PhD, FRCPC
Pathologists’ Assistants Corner: Case of the month -
PUbliShiNg EDitoR
Deborah McNamara
eye melanoma
Author: Martin Grealish MLT, MTM, PA(CCCPA).
aRt DiRECtoR
disCussion
21
Sherri Keenan
traNSlatioN Uncertain about uncertainty in pathology reports
Jocelyne Demers Owoka
Author: Jerusha Selvanayagam and Martin Hyrcza MD, PhD.
Éliane Fréchette
Magali Cloutier Provencher
guidelines
28
PUbliShiNg agENCy
Clockwork Communications inc. Measuring workload in nephropathology: a Canadian experience.
PO Box 33145, Halifax, NS, B3L 4T6 Authors: Kevin Yi Mi Ren MD, et al.
902.442.3882 / info@ClockworkCanada.com
ReseaRCh aRtiCle
40
Canadian Journal of Pathology is a peer-reviewed
journal published four times per year, by Clockwork
Communications Inc., on behalf of the Canadian Clinical impact reporting and assessment of non-conforming
Association of Pathologists. events in anatomical pathology.
Authors: Lisa M. DiFrancesco MD, FRCPC, Denise LaPerle MLT,
We cannot assume responsibility or commitment for
Tamara Trotter MLT, Máire A. Duggan MD, FRCPC.
unsolicited material. Any editorial material, including
photographs, that are accepted from an unsolicited
pathology infoRmatiCs
51
contributor, will become the property of the
Canadian Association of Pathologists.
Machine learning in pathology: A primer on techniques and
Copyright Canadian Association of Pathologists applications.
(CAP-ACP). All rights reserved. Reprinting in part Authors: Adrian B. Levine MD, Jasleen K. Grewal BSc, Steven J. M. Jones
or in whole forbidden without express written
PhD, FRSC, FCAHS, Stephen Yip MD, PhD, FRCPC.
consent from CAP-ACP.
Case RepoRt & ReViews
60
We welcome editorial submissions to
www.CanadianJournalOf Pathology.ca
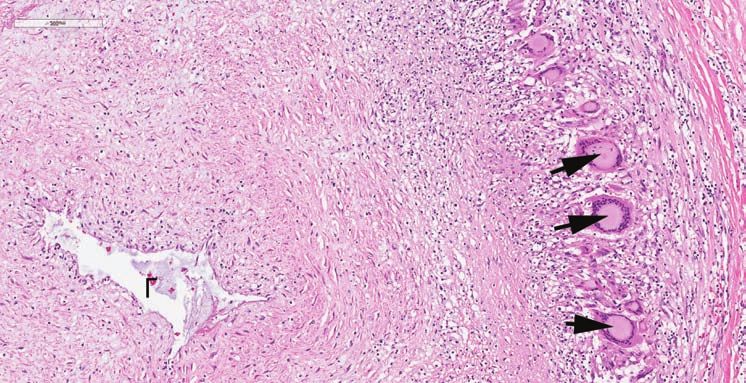
Divergent presentations of pulse granulomas: A sequela of colonic
Publications Mail Agreement No. 43490512 injury that is important to recognize
ISSN 1918-915X (print) Authors: Jordan Sim MD, Fawaz Halwani MD, Goo Lee MD, PhD.
65
ISSN 1918-9168 (online)
Return undeliverable Canadian addresses to:
Clockwork Communications inc Case report: Unsuspected giant cell coronary arteritis - a reminder
PO Box 33145 to clinicians and pathologists to advocate for autopsies.
Halifax, NS B3L 1K3 Authors: Guy Fradet MD, FRCSC, Dwayne Wenzel MD, William A.
Stinson BSc.
www.cap-acp.org Revue canadienne de pathologie | volume 10, numéro 3 | www.cap-acp.org 3
LETTER FROM THE
EDITOR-IN-CHIEF
PUBLICLY AVAILABLE DATA:
A GAME CHANGER IN MODERN RESEARCH?
P
ublicly available databases have been revolutionizing A recent Canadian initiative – the Tannenbaum Open
the world of research in recent years. Several examples Science Institute – transformed the Montreal Neurological
of highly curated open-access datasets include: The Institute into the first fully open science institute in the
Cancer Genome Atlas (TCGA), the International Cancer world. Its guiding principles include open access (of data,
Genome Consortium (ICGC), Gene Expression Omnibus protocols, and reagents), open research partnerships, open
(GEO), SNP databases, and many others. Databases of this 21st century bio/data banking, and open intellectual
scale are ordinarily made freely available to the scientific property. Moreover, publically available data are not
research community. These databases, that are often a result restricted to scientific results and spans numerous sectors.
of large scale international collaboration, rely on high
quality data and a solid study design. As a result these Open access is not limited to research results but can also
databases usually involve a large number of cases obtained include analytical tools and programs that can be of great
from multiple institutions across the world and equate to a help to researchers. Several programs are available for large
multimillion dollar investment. scale genomics and proteomics analysis like Cytoscape, gene
MANIA, and many more. Moreover, several of these
Data-sharing can have many advantages in the world of analytical tools are directly linked to and integrated with
research and it has the potential to lead us to the precipice high quality public databases which make it easier for
of a new era in the scientific community. Data sharing researchers to navigate through them and to perform simple
provides, for example, a unique and cost-effective analysis without the need for IT expert.
opportunity for many individual or small research groups
to utilize data for free. It provides access to high-quality Caution should, however, be taken when analyzing public
information that can be used for initial screening of research databases as there are a number of factors that can affect
hypothesis in small labs. Additionally, it can also be utilized the quality of open access data and analytics. These include
as an independent validation set for experimental results. contamination, suboptimal experimental protocols,
There are several examples in recent literature when public suboptimal statistical analysis, and technical experimental
data sets were used to enhance the quality and credibility of differences resulting in variation of results.
research findings. 1,2 Another point to consider is that
making data publically available increases transparency and Moving forward, an important obstacle that needs to be
collaboration within the research community and gives overcome is the lack of standardization between platforms
others the opportunity to independently verify the data. that use different technologies/experimental protocols that
Data-sharing can also maximize the potential of
interdisciplinary research and open the doors to a holistic
approach in research. continued on page 6
4 Canadian Journal of Pathology | Volume 10, Issue 3 | www.cap-acp.org
LETTRE DU RÉDACTEUR
EN CHEF
LES DONNÉES ACCESSIBLES AU PUBLIC :
UN ÉLÉMENT QUI CHANGE LA DONNE DANS LA
RECHERCHE MODERNE?
A
u cours des dernières années, les bases de données autres l’occasion de vérifier de manière indépendante les
accessibles au public ont révolutionné le monde de la données. Le partage de données peut aussi optimiser le
recherche. Parmi les nombreux exemples d’ensembles potentiel de la recherche interdisciplinaire et ouvrir les
de données en libre accès très bien organisés, notons : The portes à une approche holistique dans le domaine de la
Cancer Genome Atlas (TCGA), the International Cancer recherche.
Genome Consortium (ICGC), Gene Expression Omnibus
(GEO), les bases de données SNP et plusieurs autres. Les bases Une initiative canadienne récente — le Tannenbaum Open
de données de cette envergure sont habituellement accessibles Science Institute — a permis à l’Institut neurologique de
gratuitement pour la communauté de recherche scientifique. Montréal de devenir le premier institut scientifique au monde
Ces dernières, qui sont souvent le résultat d’une collaboration dont les données sont entièrement accessibles. Ses principes
internationale de grande envergure, dépendent de données de directeurs incluent l’accès libre (aux données, protocoles et
grande qualité et d’une solide méthodologie. Par conséquent, réactifs), les partenariats de recherche ouverts, les banques de
ces bases de données comportent habituellement un grand données/biologiques du XXIe siècle ouvertes et la propriété
nombre de cas qui ont été obtenus de différents établissements intellectuelle ouverte. En outre, les données accessibles au
à travers le monde et équivalent à un investissement de public ne sont pas restreintes aux conclusions scientifiques et
plusieurs millions de dollars. couvrent de nombreux secteurs.
Le partage de données peut présenter de nombreux L’accès libre ne se limite pas aux conclusions de recherche,
avantages dans le monde de la recherche en plus d’avoir le mais peut aussi inclure des outils et des programmes de
potentiel de nous amener au seuil d’une nouvelle ère au sein recherche qui peuvent s’avérer d’une grande aide pour les
de la communauté scientifique. Le partage des données chercheurs. De nombreux programmes sont disponibles pour
offre, par exemple, une occasion unique et économique pour les analyses génomiques et protéomiques de grande envergure,
plusieurs personnes ou de petits groupes de recherche comme Cytoscape, gene MANIA, et plusieurs autres. De plus,
d’utiliser gratuitement des données. Il permet d’avoir accès plusieurs de ces outils analytiques sont directement liés et
à de l’information de grande qualité qui peut être utilisée intégrés à des bases de données publiques de grande qualité
pour l’analyse initiale d’une hypothèse de recherche en petits permettant ainsi aux chercheurs de les consulter facilement et
laboratoires. De plus, le partage de données peut également d’effectuer de simples analyses sans avoir recours à un expert
être utilisé comme ensemble de validation indépendante en TI.
pour les résultats expérimentaux. Il existe dans la littérature
récente plusieurs exemples où les ensembles de données La prudence est cependant de mise lorsqu’on analyse des
publiques ont été utilisés pour rehausser la qualité et la bases de données publiques, car un certain nombre de
crédibilité des conclusions de recherche.1,2 Un autre élément facteurs peuvent influencer la qualité des données en libre
à prendre en considération est que le fait de donner libre accès et l’analytique. Parmi ces facteurs, notons : la
accès aux données accroît la transparence et la collaboration contamination, les protocoles expérimentaux sous-
au sein de la communauté de recherche tout en donnant aux optimaux, les analyses statistiques sous-optimales et les
Revue canadienne de pathologie | volume 10, numéro 3 | www.cap-acp.org 5
lEttRE DU RéDaCtEUR EN ChEF (suite)
différences expérimentales techniques entraînant une technologie qui oblige les chercheurs à développer un plan
variation des résultats. pour rendre publics les résultats de recherches financées par
l’État dans l’année suivant leur publication.
À l’avenir, un obstacle important que l’on doit surmonter est
le manque de normalisation entre les plateformes qui utilisent L’accès libre aux résultats de recherche constitue une
différentes technologies/protocoles expérimentaux et qui peut révolution prometteuse et substantielle dans nos normes de
parfois empêcher de comparer les résultats. Néanmoins, les recherche. Cette méthode possède des avantages considérables
outils informatiques ainsi que la normalisation de la qui l'emportent sur ses limites potentielles. La communauté
présentation des ensembles de données pourraient faire en scientifique devrait travailler main dans la main pour orienter
sorte que l’information devienne comparable et échangeable, la recherche en pathologie vers une nouvelle ère informatique.
pavant ainsi la voie à une plus grande collaboration et
davantage d’innovations dans le monde de la recherche. Plus George M. Yousef, M. D., Ph. D., FRCPC
de transparence et de détails techniques sont nécessaires pour Rédacteur en chef, Revue canadienne de pathologie
rendre les résultats comparables (type d’échantillons, sous-
types histologiques, procédure exacte pour l’extraction et le
traitement des molécules, etc.) et ils devraient tous être liés aux Références :
données.
1. Butz H., Szabo P.M., Nofech-Mozes R., Rotondo F.,
On devrait encourager et renforcer encore davantage cette Kovacs K., Mirham L. et coll., Integrative bioinformatics
attitude collaborative. Les organismes gouvernementaux analysis reveals new prognostic biomarkers of clear cell
devraient s’assurer que tout laboratoire de recherche financé renal cell carcinoma, Clin chem., 2014;60(10):1314-26.
par l’État rend public son travail. La générosité associée au
partage des données devrait toutefois aussi être reconnue à 2. Yousef G.M., Polymeris M.E., Yacoub G.M., Scorilas A.,
l’échelle universitaire. Certains pays ont d’ailleurs entrepris Soosaipillai A., Popalis C. et coll., Parallel overexpression
des démarches en ce sens. Par exemple, en 2013, les États- of seven kallikrein genes in ovarian cancer, Cancer res.,
Unis ont élaboré une politique relative à la science et à la 2003;63(9):2223-7.
lEttER FRoM thE EDitoR-iN-ChiEF (cont.)
can sometimes make the results incomparable. Nonetheless, Open access to research results is a promising and substantial
informatics tools, along with standardizing the format of revolution to our standards of research. It has significant
data sets, could make information comparable and advantages that outweigh its potential limitations. The
exchangeable thus paving the road for further collaboration scientific community should work together to bring pathology
and innovation in the world of research. More transparency research into a new era of informatics.
and technical details are needed to make results comparable
(sample type, histological subtype, exact procedure used for George M. Yousef MD, PhD, FRCPC
molecular extraction and processing, etc.) and should be all Editor-in-Chief, Canadian Journal of Pathology
linked to the data.
References:
This collaborative attitude should be encouraged and further
enforced. Government agencies should ensure that any 1. Butz H, Szabo PM, Nofech-Mozes R, Rotondo F, Kovacs
publicly-funded research labs make their work publicly K, Mirham L, et al. Integrative bioinformatics analysis
available. The generosity of data-sharing should, however, reveals new prognostic biomarkers of clear cell renal cell
also be academically recognized. Some countries have begun carcinoma. Clin Chem. 2014;60(10):1314-26.
taking steps in this. As an example, the US established a
Science and Technology policy, in 2013, that requires 2. Yousef GM, Polymeris ME, Yacoub GM, Scorilas A,
researchers to develop a plan to make the results of federally- Soosaipillai A, Popalis C, et al. Parallel overexpression of
funded research publicly available within one year of seven kallikrein genes in ovarian cancer. Cancer Res.
publication. 2003;63(9):2223-7.
6 Canadian Journal of Pathology | Volume 10, Issue 3 | www.cap-acp.org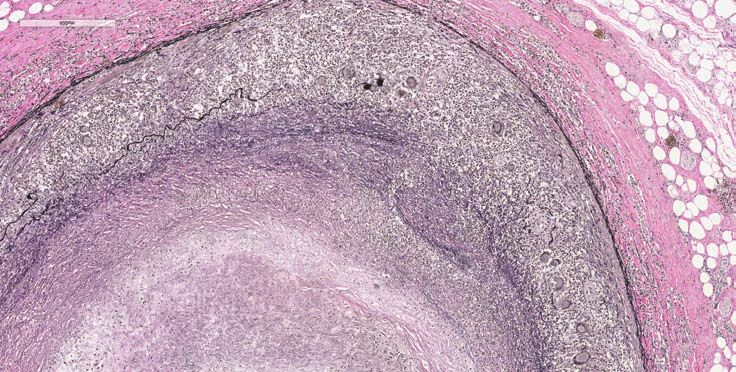
Striving to outsmart cancer. Together. AbbVie and pathologists are collaborating on common objectives: discovering and developing medicines that drive transformational improvements in cancer treatment. abbvieoncology.com @abbviecanada
EDitoRial boaRD
EDitoRial boaRD Irvaym B. Barsoum MD, MSc, PhD; Michael Carter MD, PhD; Hala Faragalla MD, FRCPC; Louis Gaboury
M.D., Ph.D., F.R.C.P.(C), F.C.A.P.; John Gartner MD CM, FRCPC; Laurette Geldenhuys MBBCH, FFPATH,
MMed, FRCPC, MAEd, FIAC; Zeina Ghorab MD, MSc; Nadia Ismiil MBChB, FRCPC; Jason Karamchandani
MD; Adriana Krizova MD, MSc, FRCPC; David Munoz MD, MSc, FRCPC; Christopher Naugler MD, FRCPC;
Tony Ng MD, PhD FRCPC; Sharon Nofech-Mozes MD; Maria Pasic PhD, FCACB; Aaron Pollett MD, MSc,
FRCPC; Rola Saleeb MD; Harman Sekhon MD, PhD, FCAP; Monalisa Sur MBBS, FCPath, MMed., MRCPath,
FRCPC; Aducio Thiesen MD, PhD, MSc, FRCPC; Stephen Yip MD, PhD, FRCPC.
iNtERNatioNal EDitoRial boaRD
Emma H. Allott PhD, University of North Carolina, USA; Fredrik Bosman MD, PhD, University of Lausanne,
Switzerland; Daniel Chan PhD, DABCC, FACB, Johns Hopkins University School of Medicine, USA; Runjan
Chetty MB BCh, FRCPA, FFPath, FRCPath, FRCPC, FCAP, Dphil, University of Toronto, Canada; Kumarasen
Cooper MBChB, Dphil, FRC path, University of Pennsylvania, USA; Brett Delahunt BSc Hons BMedSc MB
ChB MD FRCPA FFSc FRCPath, University of Otago, New Zealand; Sunil R Lakhani BSc (Hon), MBBS,
MRCPath, MD, FRCPath, FRCPA, The University of Queensland, Australia; Virginia A. LiVolsi MD, MASCP,
University of Pennsylvania, USA; Ricardo Lloyd MD, PhD, University of Wisconsin, USA; Jesse Mckenney MD,
Cleveland Clinic, USA; Chris Meijer MD, PhD, VU University, The Netherlands; George Netto MD, PhD, Johns
Hopkins University School of Medicine, USA; Isobel Scarisbrick PhD, Mayo Clinic, USA; Manfred Schmitt Dr.
rer. nat., Dr. med. habil. (Ph. D., M.D. sci.), Dipl.-Biologist, Technical University, Munich, Germany; Iris Schrijver
MD, Stanford University, USA; Andreas Scorilas PhD, University of Athens, Greece; Ming Tsao FRCPC, MD,
University of Toronto, Canada; Mark Wick MD, University of Virginia, USA.
CoMité DE RéDaCtioN
CoMité DE RéDaCtioN
Irvaym B. Barsoum, M.D., M. Sc, Ph.D; Michael Carter, M.D., Ph. D; Hala Faragalla, M.D., FRCPC; Louis
Gaboury, M.D., Ph. D., FRCPC, FCAP; John Gartner, M.D. CM, FRCPC; Laurette Geldenhuys, MBBCH,
FFPATH, MMed, FRCPC, MAEd, FIAC; Zeina Ghorab, M.D.; Nadia Ismiil, MBChB, FRCPC; Jason
Karamchandani, M.D.; Adriana Krizova, M.D., M. Sc, FRCPC; David Munoz, M.D., M. Sc, FRCPC;
Christopher Naugler, M.D., FRCPC; Tony Ng, M.D., Ph. D., FRCPC; Sharon Nofech-Mozes, M.D.; Maria
Pasic, Ph. D., FCACB; Aaron Pollett, M.D., M. Sc, FRCPC; Rola Saleeb M.D.; Harman Sekhon, M.D., Ph.
D, FCAP; Monalisa Sur, MBBS, FCPath, MMed., MRCPath, FRCPC; Aducio Thiesen, M.D., Ph. D, M. Sc,
FRCPC; Stephen Yip, M.D., Ph. D, FRCPC.
CoMité DE RéDaCtioN iNtERNatioNal
Emma H. Allott, Ph. D, Université de North Carolina, É.-U.; Fredrik Bosman, M.D., Ph. D., Université de
Lausanne, Suisse; Daniel Chan, Ph. D., DABCC, FACB, faculté de médecine de l’Université Johns Hopkins,
É.-U.; Runjan Chetty, MB BCh, FRCPA, FFPath, FRCPath, FRCPC, FCAP, Dphil, Université de Toronto,
Canada; Kumarasen Cooper ,MBChB, Dphil, FRC path, Université de la Pennsylvania, É.-U.; Brett Delahunt,
B. Sc Hons BMedSc MB ChB MD FRCPA FFSc FRCPath, Université d’Otago, Nouvelle-Zélande; Sunil R
Lakhani, B. Sc (Hon), MBBS, MRCPath, M.D., FRCPath, FRCPA, Université de Queensland, Australie;
Virginia A. LiVolsi, M.D., MASCP, Université de la Pennsylvanie, É.-U.; Ricardo Lloyd, M.D., Ph. D,
Université du Wisconsin, É.-U.; Jesse Mckenney, M.D., Clinique de Cleveland, É.-U.; Chris Meijer, M.D.,
Ph. D., Université VU, Pays-Bas; George Netto, M.D., Ph. D., faculté de médecine de l’Université Johns
Hopkins, É.-U.; Isobel Scarisbrick, Ph. D., Clinique Mayo, É.-U.; Manfred Schmitt, Dr. rer. nat., Dr. med.
habil. (Ph. D., M.D. sci.), Dipl.-Biologist, Université polytechnique, Munich, Allemagne; Iris Schrijver, M.D.,
Université Stanford, É.-U.; Andreas Scorilas, Ph. D., Université d’Athènes, Grèce; Ming Tsao, FRCPC, M.D.,
Université de Toronto, Canada; Mark Wick, M.D., Université de la Virginie, É.-U.
8 Canadian Journal of Pathology | Volume 10, Issue 3 | www.cap-acp.org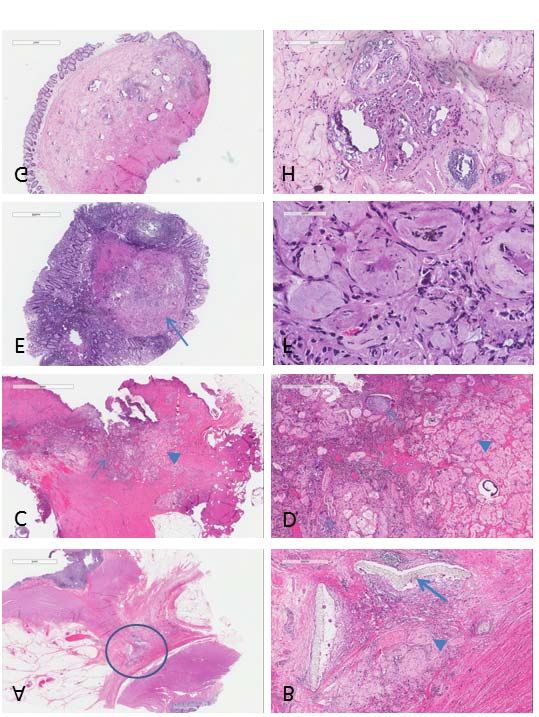
moleCulaR pathology CoRneR
This article was peer-reviewed.
KeywoRds:
gist, molecular: cKit, pdgfRa.
MolECUlaR tEStiNg iN
gaStRoiNtEStiNal StRoMal tUMoURS –
WE’vE got thE giSt oF it, NoW lEt’S go
FoRWaRD
authors: Caroline S Allen1 and Catherine J Streutker2 MD, MSc, FRCPC.
1
affiliations: Faculty of Arts and Science, Queen’s University, Kingston, ON, Canada.
2
Department of Laboratory Medicine, St. Michael’s Hospital and the University of Toronto, Toronto,
ON, Canada.
The authors declare that there are no conflicts of interest regarding the publication of this paper.
All authors have provided CAP-ACP with non-exclusive rights to publish and otherwise deal with or make use of this
article, and any photographs/images contained in it, in Canada and all other countries of the world.
ABSTRACT
Molecular testing in gastrointestinal stromal tumours has expanded beyond the
original discovery of cKIT mutations. Molecular analysis is essential for diagnosis,
prognostication and treatment of these tumours.
Review recognized that these tumours are a cell membrane (exon 11, most common),
specific entity, likely arising from the just outside the membrane in the
In the days prior to effective interstitial cells of Cajal (reviewed in 3). extracellular ligand binding domain (exon
immunohistochemistry and molecular Shortly afterward, the tyrosine kinase 9, second most common, and exon 8,
testing (i.e. the late 1990s and early 2000s), inhibitor imatinib (STI571, Gleevec, very rare) and in the kinase enzymatic site
gastrointestinal stromal tumours (GISTs) Glivec, Novartis Pharmaceuticals Corp) (exons 13, 17, less commonly).6 It was
were given a wide variety of names – GIST, was proposed as a treatment which also recognized that, while the majority of
gastrointestinal autonomic nerve tumour subsequently showed considerable effect in GISTs (80-90%) contained cKIT
(GANT), leiomyoma/leiomyosarcoma, trials.4 mutations, a proportion (‘wild-type’
etc. These tumours were difficult to GIST) did not. Clearly, cKIT was not the
diagnose, unpredictable in behaviour and Early studies on molecular testing only gene involved. A gene coding for
resistant to chemotherapy and focussed on diagnosis as well as the another TK protein, platelet-derived
radiotherapy, leaving surgery as the only relationship of cKIT mutations to growth factor-alpha (PDGFRA) was
useful treatment option. With the survival, basically attempting to predict noted to be mutated in 5-7% of GIST
recognition of gain-of-function mutations malignant behaviour.5 It was found that cases. Activating PDGFRA mutations
in the tyrosine kinase (TK) gene cKIT in a the mutations tend to cluster into specific tend to be focussed in the tyrosine kinase
majority of these tumours1 and the advent areas of the gene: in the (TK) activity areas (exon 18, exon 14) as
of the CD117/c-kit antibody for regulatory/autoinhibitory area in the well as in the juxtamembrane (exon 12)
immunohistochemistry in 1998,2 we juxtamembranous zones just inside the and rarely in the proximal extracellular
Revue canadienne de pathologie | volume 10, numéro 3 | www.cap-acp.org 9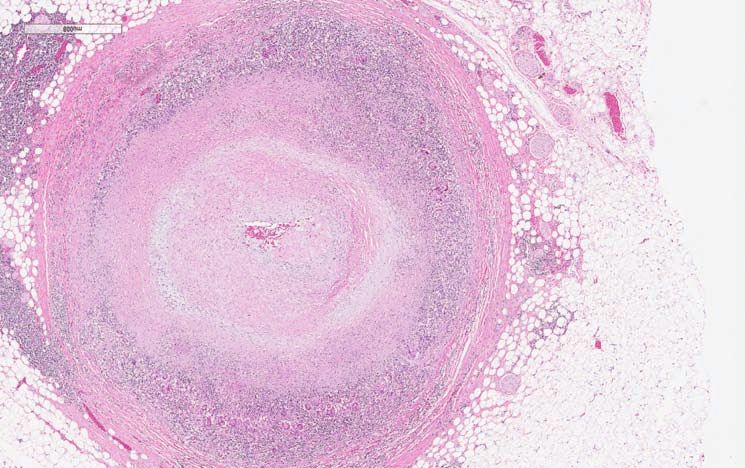
moleCulaR pathology CoRneR
MolECUlaR tEStiNg (cont.)
cáÖìêÉ=NK=
Which mutation is present also matters
with respect to prediction of response to
tyrosine kinase inhibitors (TKI) such as
imatinib and related medications such as
sunatinib. cKIT mutations in exon 11, 13
and 17 were shown to have a high
response rate (80-100%) while exon 9
mutations showed a response rate
approaching 50%.7 Some exon 11
mutations (particularly L576P) show lesser
response to imatinib.13 The PDGFRA-
mutated tumours are generally responsive
to imatinib, though the D842V mutation
in exon 18 is more often unresponsive.14,15
In tumours with mutations considered to
be ‘resistant’, response can still be obtained
with higher doses of targeted therapy, i.e.
cKIT exon 9 mutations (Figure 1).16
Most common primary cKIT and PDGFRA mutations. *: Decreased response to tyrosine kinase inhibitors
(TKI). **: Often lacks response to TKI. ***: May respond to TKI but requires increased dose.14,15
While it was originally thought that each
GIST contained only one characteristic
zones (exon 10) (Figure 1). The presence SDHC and SDHD. Silencing by promoter TK mutation, treatment with imatinib
of the cKIT and PDGFRA mutations tend methylation appears relatively common.10 brought evidence of the development of
to be mutually exclusive.7 resistance to treatment. Sequencing of
Further investigation of the remaining these metastatic lesions demonstrated
Studies continued to demonstrate a “wild-type” cases where the cKIT, secondary cKIT mutations, particularly in
proportion of cases that were wild-type PDGFRA and SDH genes are all normal exon 17, exon 13 and exon 14.11
for both cKIT and PDGFRA. One subset has discovered rare causal mutations in
of these, particularly those involved in the NF1, BRAF, NRAS and PIK3CA genes, Currently, molecular testing of all GISTs is
Carney triad/Carney-Stratakis syndromes leaving relatively few cases as true “wild suggested at diagnosis, though surgery
(gastric GIST, extra-adrenal type” GISTs.11 remains the primary modality of treatment.
paraganglioma and pulmonary This allows for diagnosis as well as
chondroma/GIST plus paraganglioma), The specific mutations, to a considerable immediate molecular testing. Neo-adjuvant
were discovered to harbour abnormalities extent, predict clinicopathologic therapy to shrink large gastric tumours
in the succinate dehydrogenase (SDH) behaviours. cKIT exon 9 mutation GISTs prior to definitive surgery can minimize the
gene.8 SDH is involved in the respiratory are generally noted to be aggressive small loss of gastric tissue, allowing a wedge
complex, and has 4 subunits (SDHA, bowel tumours.12 cKIT exon 11 deletions resection rather than a gastrectomy.
SDHB, SDHC and SDHD). In contrast to lead to aggressive, high risk gastric Adjuvant therapy is used for patients with
the gain-of-function mutations of cKIT tumours while exon 11 single nucleotide high-risk GISTs to reduce the risk of
and PDGFRA, SDH-associated GIST substitutions are generally small, lower metastasis. Here the molecular testing is not
demonstrate silencing or loss of the gene, risk tumours. cKIT exon 13 mutations are only relevant to predict response and
either by mutations or promoter higher risk when in the stomach. Overall, therefore dose of imatinib or related drug;
methylation – damage to any of the PDGFRA-associated tumours, almost the mutation with attendant risk of
subunits causing loss of the entire always gastric cases, tend to have indolent progression is part of the decision making
complex. Therefore, immuno- behaviour and generally do not require on high-risk features, driving the use of
histochemistry for SDHB where there is adjuvant therapy. The SDH-related adjuvant therapy. Patients who progress
total/near complete loss of the normal subgroup of GISTs tends to occur in the while on therapy may need repeat biopsy
strong granular cytoplasmic staining stomach in younger patients and has a of the metastatic lesion to determine if there
(mitochondrial staining) can be particular gross appearance of multi- is a treatable secondary mutation present.
diagnostic; immunohistochemistry for nodular infiltrating masses in the gastric
SDHA is also available.9 Mutations are wall, sometimes separated by fibrous While surgery remains a mainstay,
most commonly found in SDHA septae. While even small SDH-associated endoscopic needle core biopsies (EUS-FNB)
(approximately 28%), with GISTs may metastasize, they are still or tunnel or sink (single incision needle
approximately 20% each in SDHB, relatively indolent.9 knife) endoscopic biopsies are increasingly
10 Canadian Journal of Pathology | Volume 10, Issue 3 | www.cap-acp.orgmoleCulaR pathology CoRneR
MolECUlaR tEStiNg (cont.)
being used to obtain tissue from Cajal in health and disease. Part II: 10. Miettinen M, Lasota J. Succinate
submucosal/muscularis propria lesions. ICC and gastrointestinal stromal dehydrogenase deficient
Molecular testing for GIST cases has been tumours. Histopathology. gastrointestinal stromal tumours – a
predominantly performed by Sanger 2007;50(2):190-202. review. Int J Biochem Cell Biol.
sequencing and pyrosequencing for 2014;53:514-519.
hotspots. However, next generation 4. Tuveson DA, Willis NA, Jacks T,
sequencing (NGS) is becoming more widely Griffin JD, Singer S, Fletcher CD, et 11. Szucs Z, Jones RL. Perspectives on
available, with kits covering panels of all the al. STI571 inactivation of the the evolving state of the art
major involved genes. Sequencing can be gastrointestinal stromal tumor c-KIT management of gastrointestinal
done on these relatively small biopsy oncoprotein: biological and clinical stromal tumours. Transl Gastro and
specimens as long as there is reasonable implications. Oncogene. Hepatol. 2018;3:21-32.
sampling of viable tumour, similar to issues 2001;20(36):5054-8.
in lung adenocarcinomas and colon cancer.17 12. Antonescu CR, Besmer P, Guo T,
5. Singer S, Rubin BP, Lux, ML, Chen Arkun K, Hom G, Koryotowski B, et
Since many of the genes involved in the CJ, Demetri GD, Fletcher CDM, et al. Acquired resistance to imatinib in
development of GISTs can occur as al. Prognostic value of KIT mutation gastrointestinal stromal tumour
germline mutations associated with other type, mitotic activity and histologic occurs through secondary gene
tumours/findings, the possibility of subtype in gastrointestinal stromal mutation. Clin Cancer Res.
underlying familial syndromes (i.e. Carney tumors. J Clin Oncol. 2002; 2005;11(11):4182-90.
triad, cKIT germline mutations) should be 20(18):3898-905.
kept in mind. 13. Noujaim J, Gonzalez D, Thway K,
6. Huss S, Kunstlinger H, Wardelmann Jones RL, Judson I. p.(L567P)-KIT
Overall, the progress made over the past E, Kleine MA, Binot E, Merkelback- mutation in GIST: Favorable
20 years in the pathologic and molecular Bruse S, et al. A subset of prognosis and sensitive fo imatinib?
diagnosis of GISTs is a remarkable success gastrointestinal stromal tumours Cancer Biol Ther. 2016;17(5):
story. Molecular analysis contributes to previously regarded as wild-type 543-5.
diagnosis and has both predictive and tumors carries somatic activating
prognostic implications for treatment and mutations in KIT exon 8 14. von Mehren M, Joensuu H.
outcomes, with new options for adjuvant (p.D419des). Mod Pathol. Gastrointestinal stromal tumours. J
and neo-adjuvant therapy. Pathologists 2013;16:1004-1012. Clin Oncol. 2018:36(2):136-143.
continue to contribute to the diagnosis
and appropriate treatment of these cases, 7. Heinrich MC, Corless CL, Demetri 15. Lasota J, Miettinen M. Clinical
in conjunction with gastroenterologists, GD, Blanke CD, von Mehren M, significance of oncogenic KIT and
surgeons and medical oncologists. Joensuu H, et al. Kinase mutations PDGFRA mutations in
and imatinib response in patients gastrointestinal stromal tumours.
References: with metastatic gastrointestinal Histopathology. 2008;53:245-266.
stromal tumour. J Clin Oncol.
1. Nakahara M, Isozaki K, Hirota S, 2003;21(23):4342-9. 16. Heinrich MC, Owzar K, Corless CL,
Miyagawa J, Hase-Sawada N, Hollis D, Borden EC, Fletcher CD,
Taniguchi M, et al. A novel gain of 8. Miettinen M, Wang ZF, Sarlomo- et al. Correlation of kinase genotype
function mutation of c-kit gene in Rikala M, Osuch C, Rutkowski P, and clinical outcome in the North
gastrointestinal stromal tumours. Lasota J. Succinate dehydrogenase- American Intergroup Phase III trial
Gastroenterology. deficient GISTs: a clinicopathologic, of imatinib mesylate for treatment of
1998;115(5):1090-5. immunohistochemical, and molecular advanced gastrointestinal stromal
genetic study of 66 gastric GISTs tumour. J Clin Oncol.
2. Sarlomo-Rikala M, Kovatoch AJ, with predilection to young age. Am 2008;26(33):5360-7.
Barusevicius A, Miettinen M. J Surg Pathol. 2011;35(11):1712-21.
CD117: a sensitive marker for 17. Zheng G, Tsai H, Tseng LH, Illei P,
gastrointestinal stromal tumours 9. Janeway KA, Kim SY, Lodish M, Gocke CD, Eshleman JR, et al. Test
that is more specific than CD34, Nose V, Rustin P, Gaal J, et al. feasibility of next-generation
Mod Pathol. 1998;11(8);728-34. Defects in succinate dehydrogenase sequencing assays in clinical
in gastrointestinal tumours lacking mutation detection of small biopsy
3. Streutker CJ, Huizinga JD, Driman KIT and PDGFRA mutations. Proc and fine needle aspiration specimens.
DK, Riddell RH. Interstitial cells of Natl Acad Sci USA. 2011;108:314-318. AJCP. 2016;145:696-702.
Revue canadienne de pathologie | volume 10, numéro 3 | www.cap-acp.org 11RubRiQue de pathologie molÉCulaiRe
Cet article a été révisé par des pairs.
mots-ClÉs :
tsgi, moléculaire, c-kit, pdgfRa
tEStS MoléCUlaiRES Et tUMEURS
StRoMalES gaStRo-iNtEStiNalES : lE
tEMPS ESt vENU DE PaSSER à la
PRoChaiNE étaPE
auteurs : Caroline S. Allen1 et Catherine J. Streutker, M.D., M. Sc., FRCPC2.
affiliations : 1Faculté des arts et des sciences, Université Queen’s, Kingston, Ontario, Canada
2
Département de médecine de laboratoire, Hôpital St. Michael et Université de Toronto, Toronto,
Ontario, Canada
La version originale du présent manuscrit a été soumise en anglais,
puis traduite en français par Éliane Fréchette, traductrice agréée.
Les auteurs ne déclarent aucun conflit d’intérêts relativement à la publication de cet article.
De plus, ils ont tous accordé à la CAP-ACP le droit non exclusif de publier et d’utiliser cet article, et toute image ou
photographie qu’il renferme, ou d’en disposer autrement, au Canada et partout ailleurs dans le monde.
RÉSUMÉ
Les tests moléculaires réalisés en cas de tumeurs stromales gastro-intestinales
servent désormais à bien plus que la simple mise en évidence de mutations de c-kit.
En effet, les analyses moléculaires sont maintenant essentielles au diagnostic, au
pronostic et au traitement de ces tumeurs.
Article radiothérapie, étaient difficiles à
diagnostiquer et leur comportement était
Avant l’arrivée des analyses imprévisible. L’intervention chirurgicale
immunohistochimiques et moléculaires était alors considérée comme la seule
efficaces (vers la fin des années 1990 et option de traitement utile. À la suite de
le début des années 2000), divers noms la découverte de mutations de gain de
ont été donnés aux tumeurs stromales fonction dans le gène de la tyrosine
gastro-intestinales (TSGI) : TSGI, kinase c-kit dans la majorité de ces
tumeurs du système nerveux autonome tumeurs1, et de l’avènement de
du tube digestif (GANT), léiomyomes, l’anticorps CD117 (c-kit) à des fins
léiomyosarcomes, etc. Ces tumeurs, d’immunohistochimie en 19982, on a
résistantes à la chimiothérapie et à la reconnu les TSGI comme des entités
12 Canadian Journal of Pathology | Volume 10, Issue 3 | www.cap-acp.orgRubRiQue de pathologie molÉCulaiRe
tEStS MoléCUlaiRES (suite)
propres, qui prenaient mettre en relief une proportion de cas de
vraisemblablement naissance dans les « type sauvage » tant pour c-kit que
cellules interstitielles de Cajal (voir pour PDGFRA. On a découvert que l’un
référence no 3). Peu de temps après, des sous-ensembles de ces mutations,
l’imatinib, un inhibiteur de la tyrosine particulièrement celles associées à la
kinase (STI-571, Gleevec®, Glivec®, triade de Carney et au syndrome de
Novartis Pharmaceuticals Corp.) a été Carney-Stratakis (TSGI, paragangliome
proposé pour traiter les TSGI. Des extrasurrénalien et chondrome
répercussions considérables ont été pulmonaire ou TSGI accompagnée d’un
observées lors des essais cliniques paragangliome), entraîne des anomalies
réalisés à cet effet4. du gène succinate déshydrogénase
(SDH)8. Le SDH, qui présente quatre
Les premières études portant sur les tests sous-unités (SDHA, SDHB, SDHC et
moléculaires étaient axées sur le SDHD) joue un rôle dans le complexe
diagnostic et la relation entre les respiratoire. Contrairement aux
mutations de c-kit et les chances de mutations de gain de fonction de c-kit et
survie, et tentaient essentiellement de de PDGFRA, les TSGI associées à SDH
prédire la malignité des tumeurs5. On a démontrent un silençage ou une perte
constaté que les mutations avaient d’expression génique, attribuable soit à
tendance à toucher des régions précises des mutations ou à la méthylation du
du gène : la région régulatrice/ promoteur. Les dommages occasionnés
autoinhibitrice des zones à l’une ou l’autre des sous-unités
juxtamembranaires situées à l’intérieur entraînent la perte du complexe en
de la membrane cellulaire (exon 11, entier. Par conséquent, une
région la plus courante); la région située immunohistochimie pour SDHB qui
tout juste en dehors de la membrane, présente une absence totale ou quasi
dans le domaine extracellulaire de totale de coloration cytoplasmique
liaison au ligand (exon 9, deuxième granulaire (coloration mitochondriale)
région la plus courante, et exon 8, très normalement intense peut être
rare); et dans le site enzymatique diagnostique. Une immunohistochimie
tyrosine kinase (exons 13 et 17, région peut aussi être réalisée pour SDHA9. On
moins courante)6. On a également observe des mutations dans environ 28
conclu que, bien que la majorité (80 à 90 % des SDHA et dans près de 20 % des
%) des TSGI présentaient des mutations SDHB, SDHC et SDHD. Le silençage dû
de c-kit, ce n’était pas le cas de toutes les à la méthylation du promoteur semble
tumeurs (TSGI de « type sauvage »). C- être assez courant10.
kit n’était donc manifestement pas le
seul gène en cause. On a alors observé D’autres études des cas restants de « type
qu’un gène codant pour une autre sauvage », où les gènes c-kit, PDGFRA
protéine tyrosine kinase, le facteur de et SDH sont tous normaux, ont permis
croissance dérivé des plaquettes alpha de révéler des mutations causales rares
(PDGFRA), avait subi des mutations dans les gènes NF1, BRAF, NRAS et
dans 5 à 7 % des cas de TSGI. PIK3CA. Le nombre de cas véritables de
L’activation des mutations de PDGFRA TSGI de « type sauvage » est donc plutôt
survient principalement dans les zones restreint11.
d’activité de la tyrosine kinase (exon 18,
exon 14) de même que dans la région Les mutations permettent, dans une
juxtamembranaire (exon 12) et, plus large mesure, de prédire les
rarement, dans les zones extracellulaires comportements clinicopathologiques.
proximales (exon 10) (figure 1). Les Par exemple, les TSGI qui présentent une
mutations de c-kit et de PDGFRA sont mutation de l’exon 9 du gène c-kit
généralement mutuellement exclusives7. correspondent généralement à des
tumeurs agressives de l’intestin grêle12.
Les études continuent cependant de Les délétions de l’exon 11 de c-kit sont
Revue canadienne de pathologie | volume 10, numéro 3 | www.cap-acp.org 13RubRiQue de pathologie molÉCulaiRe
tEStS MoléCUlaiRES (suite)
cáÖìêÉ=NK=
c-kit ont été associées à un taux de
réponse élevé (80 à 100 %), alors que
celles subies par l’exon 9 démontrent un
taux de réponse de près de 50 %7.
Exon 8 : 1 %
Domaine extracellulaire
Certaines mutations de l’exon 11
Exon 9 : 10 %
AY502-503*** (particulièrement la mutation L576P)
Membrane cellulaire
sont associées à un taux de réponse à
Exon 11 : 67,5 %
l’imatinib moins élevé13. Les tumeurs
Domaine juxtamembranaire
V559D, L576P*
Exon 12 : 1 %
attribuables à des mutations de
Exon 13 : 1 %
Domaine tyrosine kinase (TK1)
VD61D PDGFRA répondent généralement bien
K642E
Exon 14 : 0,3 %
N569K
à l’imatinib, bien que la mutation
Domaine d’insertion kinase
D842V de l’exon 18 n’y réponde
souvent pas efficacement14,15. Chez les
Exon 17 : 0,5 %
N822H, N822K,
patients où les tumeurs ayant subi des
Domaine tyrosine kinase (TK2)
D820Y Exon 18 : 6,3 %
D842V**, D843Y
mutations sont considérées comme «
résistantes » (par exemple, les mutations
de l’exon 9 de c-kit), une réponse peut
être obtenue à l’aide de plus fortes doses
Mutations primaires les plus courantes de c-kit et de PDGFRA * : Diminution de la réponse aux
inhibiteurs de la tyrosine kinase ** : Réponse irrégulière aux inhibiteurs de la tyrosine kinase
du traitement ciblé (figure 1)16.
*** : Réponse aux inhibiteurs de la tyrosine kinase si dose accrue14,15
Si les chercheurs croyaient à l’origine
que chaque TSGI contenait une seule
quant à elles associées à des tumeurs mutation caractéristique de la tyrosine
gastriques agressives qui comportent un kinase, l’imatinib a mis en évidence le
niveau de risque élevé, tandis que les développement d’une résistance au
substitutions mononucléotidiques de traitement. Le séquençage de ces lésions
l’exon 11 sont habituellement liées à des métastatiques a révélé la présence de
tumeurs de petite taille qui présentent un mutations secondaires de c-kit,
plus faible risque. Les mutations de particulièrement dans les exons 17, 13
l’exon 13 de c-kit représentent un risque et 1411.
plus élevé quand elles se trouvent dans
l’estomac. De façon générale, les À l’heure actuelle, l’analyse moléculaire
tumeurs associées à PDGFRA, des cas de l’ensemble des TSGI est suggérée au
qui sont presque toujours gastriques, ont moment du diagnostic, bien que
tendance à adopter un comportement l’intervention chirurgicale demeure la
indolent et ne nécessitent généralement principale méthode de traitement.
pas de traitement adjuvant. Le sous- L’opération permet le diagnostic et la
groupe de TSGI associées à SDH a réalisation immédiate de tests
tendance à survenir dans l’estomac des moléculaires. La mise en place d’un
patients moins âgés et se présente traitement néoadjuvant visant à réduire
macroscopiquement sous forme de la taille des tumeurs gastriques avant
masses multinodulaires infiltrantes l’intervention chirurgicale définitive peut
situées dans la paroi gastrique, parfois minimiser la perte de tissu gastrique,
séparées par des cloisons fibreuses. Bien permettant la réalisation d’une résection
que même les TSGI de petite taille cunéiforme au lieu d’une gastrectomie.
associées à SDH puissent métastaser, Un traitement adjuvant est proposé aux
elles demeurent relativement indolentes9. patients qui présentent des TSGI
associées à un niveau de risque élevé afin
Le type de mutation présente influe de diminuer le risque de métastase. Dans
également sur la prévision de la réponse de tels cas, les tests moléculaires ne sont
aux inhibiteurs de la tyrosine kinase pas seulement utiles pour prédire la
comme l’imatinib et les médicaments réponse au traitement et déterminer la
connexes, dont le sunatinib. Les dose d’imatinib ou du médicament
mutations dans les exons 11, 13 et 17 de prescrit à administrer. En effet, la
14 Canadian Journal of Pathology | Volume 10, Issue 3 | www.cap-acp.orgRubRiQue de pathologie molÉCulaiRe
tEStS MoléCUlaiRES (suite)
mutation, et le risque afférent de TSGI sont le séquençage Sanger et le de lignée germinale de c-kit) devrait être
progression, font partie des composantes pyroséquençage, qui permet la mise en prise en considération.
à risque élevé du processus de prise de évidence des hotspots mutationnels. Or,
décisions qui encouragent le recours au le séquençage de nouvelle génération Globalement, les progrès réalisés au
traitement adjuvant. Les patients dont la devient de plus en plus accessible; les cours des 20 dernières années en lien
maladie progresse en cours de traitement trousses offertes couvrent désormais avec le diagnostic pathologique et
peuvent devoir subir une autre biopsie de l’ensemble des principaux gènes en moléculaire des TSGI sont un
la lésion métastatique pour déterminer si cause. Le séquençage peut être réalisé sur remarquable exemple de réussite. Les
une mutation secondaire traitable est des échantillons de biopsie relativement analyses moléculaires contribuent au
présente. petits, tant et aussi longtemps que la diagnostic et ont des répercussions
taille des échantillons de tumeurs viables prédictives et pronostiques sur le
Bien que l’intervention chirurgicale est raisonnable, comme c’est le cas pour traitement et les résultats, proposant de
demeure la principale marche à suivre, les adénocarcinomes des poumons et le nouvelles options de traitement adjuvant
les biopsies endoscopiques au trocart cancer du côlon17. et néoadjuvant. Enfin, les pathologistes,
(EUS-FNB) et celles avec incision unique de concert avec les gastroentérologues,
par aiguille bistouri (single incision Comme bon nombre des gènes qui les chirurgiens et les oncologues,
needle-knife ou SINK) sont de plus en participent au développement des TSGI continuent de contribuer au diagnostic
plus utilisées pour prélever des tissus à peuvent se présenter sous forme de et au traitement adéquat de ces cas.
partir de lésions de la sous-muqueuse ou mutations de lignée germinale associées
de la couche longitudinale. Les deux à d’autres tumeurs, la possibilité de Pour consulter les références, reportez-
principales méthodes d’analyse syndromes familiaux sous-jacents (par vous à la page 11.
moléculaire employées dans les cas de exemple, triade de Carney ou mutations
All peer-reviewed articles appearing in this publication have undergone a double blind
peer-review process. The views or opinions expressed in this Journal are those of the
authors and contributors, and do not necessarily reflect those of this Journal, the editors,
the editorial board, the publisher of this Journal, or the Canadian Association of
Pathologists (CAP-ACP).
Although the CAP-ACP has made reasonable efforts to ensure accuracy the articles
herein, the Journal, the editors, the editorial board, the publisher of this Journal, or the
CAP-ACP, take no responsibility whatsoever for any errors, omissions, or any
consequences of reliance on any material or the accuracy of any information contained
in this publication. In the event of a discrepancy, between the original and translated
versions of the texts, the original version shall take precedence.
The mention of trade names, commercial products or organizations, and the inclusion
of advertisements in the Journal does not imply endorsement by this Journal, the editors,
the editorial board, the publisher of this Journal or the CAP-ACP.
This publication is copyright in its entirety. Material may not be reprinted, stored in a
retrieval system, or copied without the written permission of CAP-ACP. Contact
through www.cap-acp.org.
Revue canadienne de pathologie | volume 10, numéro 3 | www.cap-acp.org 15JOIN US FOR THE OAP’S
80TH ANNIVERSARY
September 28-29
ONTARIO ASSOCIATION OF PATHOLOGIST 2018 ANNUAL MEETING
SAVE THE
The OAP is the oldest pathology organization in the country and has been
holding Annual General Meetings since 1937. As a not-for-profit medical society
DATE
organized for educational and scientific purposes, the purpose of the meeting
is to foster excellence in the practice of pathology and laboratory medicine in
Ontario.
Conference Venue: Quartier Tremblant – Base Camp,
1000 Chemin des Voyageurs, Tremblant, Québec J8E 1T1
Accommodations: LeWestin Resort & Spa, Tremblant, Quebec
ROYAL COLLEGE ACCREDITATION
This conference is an Accredited Group Learning Activity (Section 1) as defined
by the Maintenance of Certification program of the Royal College of Physicians
and Surgeons of Canada. This activity was approved by the Canadian Association
of Pathologists.
Through an agreement between the Royal College of Physicians
and Surgeons of Canada and the American Medical Association,
physicians may convert Royal College MOC credits to AMA PRA
Category 1 Credits™. Information on the process to convert Royal
College MOC credit to AMA credit can be found at:
www.ama-assn.org/go/internationalcme.
TO REGISTER:
https://ontariopathologists.org/2018-annual-meeting/pathologists’ assistants CoRneR
Key woRds:
Choroidal, melanoma, sclera, ciliary body
CaSE oF thE MoNth
EyE MElaNoMa
authors: Martin Grealish1, MLT, MTM, PA(CCCAP).
1
affiliation: Senior Pathologists’ Assistant, University Health Network.
The author would like to thank Dr. Danny Ghazarian, Dr. Margaret Redpath, and Dr. Zoya Volynskaya
for contributions to this paper.
The author declares that there are no conflicts of interest regarding the publication of this paper.
The author has provided CAP-ACP with non-exclusive rights to publish and otherwise deal with or make use of this
article, and any photographs/images contained in it, in Canada and all other countries of the world.
CASE PRESENTATION Surgical History: childhood
tonsillectomy.
The patient is a 53-year-old male who
found a small freckle in the left eye. The Medical History: family history of
patient’s optometrist identified an intra- malignant hyperthermia, smoker with
ocular mass after the patient complained one previous ER visit for chest pain.
of three weeks of blurry vision.
Examination showed a choroidal mass Imaging Studies: ultrasound showed a
in the superior temporal quadrant of the 2.1cm elevated choroidal mass in the left
fundus with inferior retinal detachment eye. CT of the chest, pelvis and abdomen
and subretinal fluid. showed no distant mets.
cáÖìêÉ=NK==bñíê~çÅìä~ê=jìëÅäÉë
Credit: OpenStax College [CC BY 3.0 (http://creativecommons.org/licenses/by/3.0)], via Wikimedia Commons.
Revue canadienne de pathologie | volume 10, numéro 3 | www.cap-acp.org 17You can also read