Patients Benefit While Surgeons Suffer: An Impending Epidemic
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Patients Benefit While Surgeons Suffer:
An Impending Epidemic
Adrian Park, MD, FACS, Gyusung Lee, PhD, F Jacob Seagull, PhD, Nora Meenaghan, MD,
David Dexter, MD
BACKGROUND: The widely held belief that laparoscopy causes greater strain on surgeons’ bodies than open
surgery is not well documented in scope or magnitude. In the largest North American survey to
date, we investigated the association of demographics, ergonomics, and environment and
equipment with physical symptoms reported by laparoscopic surgeons.
STUDY DESIGN: There were 317 surgeons identified as involved in laparoscopic practices who completed the
online survey. Data collected from this comprehensive 23-question survey were analyzed using
chi-square.
RESULTS: There were 272 laparoscopic surgeons (86.9%) who reported physical symptoms or discomfort.
The strongest predictor of symptoms was high case volume, with the surprising exceptions of
eye and back symptoms, which were consistently reported even with low case volumes. High
rates of neck, hand, and lower extremity symptoms correlated with fellowship training, which
is strongly associated with high case volume. Surprisingly, symptoms were little related to age,
height, or practice length. The level of surgeons’ awareness of ergonomic guidelines proved to be
somewhere between slightly and somewhat aware. A substantial number of respondents re-
quested improvements in regard to both the positioning and resolution of the monitor.
CONCLUSIONS: Far beyond previous reports of 20% to 30% incidence of occupational injury, we present
evidence that 87% of surgeons who regularly perform minimally invasive surgery suffer such
symptoms or injuries, primarily high case load-associated. Additional data accrual and analysis
are necessary, as laparoscopic procedures become more prevalent, for improvement of surgeon-
patient and surgeon-technology interfaces to reverse this trend and halt the epidemic before it
is upon us. (J Am Coll Surg 2010;210:306–313. © 2010 by the American College of Surgeons)
Twenty years after the introduction of the first laparoscopic of MIS in the form of productivity gains related to a faster
techniques to North American surgical audiences, mini- return to work after laparoscopic surgery. In addition, in a
mally invasive surgery (MIS) has become mainstream. Al- time of increasingly constrained health care resources, MIS
though no longer considered revolutionary, laparoscopic has facilitated a greater number of patients having opera-
surgery is still widely acknowledged to have revolutionized tions without a concomitant rise in hospital bed occupancy
the delivery of surgical care.1 By mid 2009, it could safely because many procedures can be performed on an outpa-
be claimed that millions of patients around the world have tient basis.
benefited from the reduced perioperative morbidity, the Yet, even though the benefits of MIS are now plain for all to
enhanced postoperative recovery, and the cosmetic advan- see, it is increasingly apparent in this success story that a con-
tages associated with laparoscopic over open surgical tech- siderable unforeseen cost is borne by one key stakeholder—
niques.2 Society at large has derived benefit from the advent the surgeon. The same vital procedures are performed in both
MIS and open surgery, but surgeons who perform a majority
of their cases laparoscopically have been aware for years that
Disclosure Information: Nothing to disclose.
Presented at the American College of Surgeons 94th Annual Clinical Con-
they encounter physical stress and mental strain beyond that
gress, San Francisco, CA, October 2008. which they experience performing open surgery. Reports of
such findings began emerging in the early years of the laparo-
Received September 12, 2009; Revised October 22, 2009; Accepted October
27, 2009. scopic revolution.3,4
From the Department of Surgery, University of Maryland School of Medi- In MIS, surgeons operate with reduced access to the
cine, Baltimore, MD. patient, reduced degrees of freedom in their interventions,
Correspondence address: Adrian Edward Park, MD, FACS, University of
Maryland Med Center, Room S4B14, 22 South Greene St, Baltimore, MD and lack of direct visualization of the surgical field; an ever
21201-1595. growing body of literature speaks to the unique physical
© 2010 by the American College of Surgeons ISSN 1072-7515/10/$36.00
Published by Elsevier Inc. 306 doi:10.1016/j.jamcollsurg.2009.10.017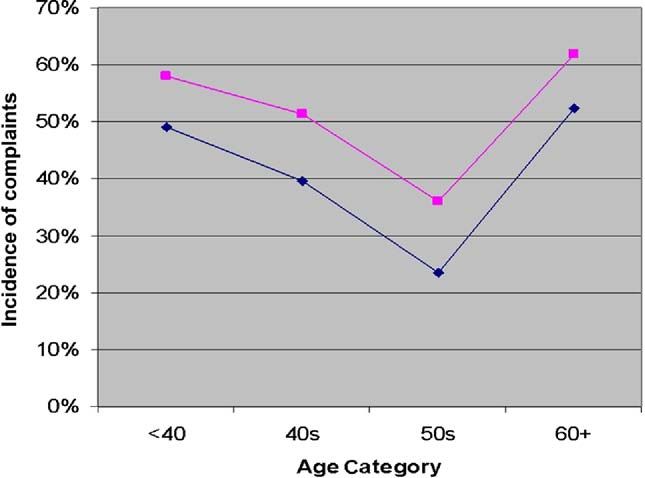
Vol. 210, No. 3, March 2010 Park et al Patients Benefit While Surgeons Suffer 307
and cognitive ergonomic challenges posed to the laparo- Survey structure
scopic surgeon.4-8 Among the documented ergonomic lim- This comprehensive ergonomic survey consisted of 23
itations affecting the minimally invasive approach are op- questions grouped into 4 categories: demographics, physi-
erational issues with instrument design,9 stresses caused by cal symptoms, ergonomics, and environment or equip-
monitor placement,10 and perceptual challenges.11 Signifi- ment (Table 1). Some questions required single answers
cant ergonomic comparisons characterizing both open and such as “Have you ever had any physical discomfort or
laparoscopic surgical performance have appeared. They are symptoms you would attribute to your laparoscopic oper-
exemplified by studies of Berguer and colleagues12 showing ating? Yes/no;” other questions allowed selection of multi-
surgical posture—as measured by a force plate system and ple applicable answers such as “Where did you acquire the
signified by the significantly reduced range of motion of recommendations made by the field of surgical ergonom-
the center of pressure—during laparoscopic procedures to ics? Literature, grand rounds, surgical training, online, re-
be less dynamic than during open procedures. They also gional or national meetings, laparoscopic product repre-
demonstrated muscular activation levels from several upper sentative, other.”
extremity muscle groups and body part discomfort scores
to be significantly higher in the case of laparoscopic com- Statistical analysis
pared with open technique in repeated knot-tying tasks.13 All data from this survey instrument were exported into
Through use of mental stress skin conductance levels, Microsoft Excel format and then analyzed using the Statis-
electro-oculograms, eye blink rates, and subjective reports, tical Package for the Social Sciences (SPSS). Data were
an earlier study also investigated surgeons using both lapa- analyzed using chi-square and logistic regression. Univari-
roscopic and open surgical techniques to perform knot- ate analysis was used to examine distribution in regard to
tying tasks; it found that the laparoscopic approach re- questions allowing a single answer. Multiple response anal-
sulted in fewer tied knots and correlated with significantly ysis was used with questions allowing multiple answers, the
higher mental stress.14 resultant percentage sum of which may exceed 100%. His-
Some authors have reported MIS-related surgeon dis- tograms were used to analyze frequency distribution. Cor-
comfort rates of 40%15 to 60%7; larger survey studies on relation analysis between two questions of interest was used
the subject have reported symptoms (often persistent) re- to investigate how one variable affected another variable’s
lated to MIS in the 12% to 18% range.16,17 A 15% rate distribution. For example, correlation analysis was applied
(approximately) of injury or symptoms suffered by sur- to the first question (What is your age?) in relation to the
geons is often quoted in discussions on the ergonomic risks eighth question (Have you ever had any physical discom-
of MIS, as though it were the conventional wisdom on the fort or symptoms you would attribute to your laparoscopic
subject. For this and other reasons, we sought through this operating?).
study to confirm the prevalence of MIS-related operator
symptoms and discomforts within a broader population of
laparoscopic surgeons. RESULTS
Three hundred seventeen surgeons identified as being ac-
tively and regularly involved in laparoscopic practices
METHODS completed the online survey (response rate of 14.4%).
Data collection The demographics of the participants are summarized in
The protocol for this research study was approved by the Table 2.
University of Maryland Internal Review Board. An e-mail
inviting ergonomic survey participation was sent to 2,000 Physical symptoms
active (ie, board certified) gastrointestinal and endoscopic Two hundred seventy-two laparoscopic surgeons (86.9%)
surgeons in North America and abroad who are members reported that they had experienced physical discomfort or
of the Society of American Gastrointestinal and Endo- symptoms they would attribute to performing MIS. This
scopic Surgeons (SAGES) to collect data representative of a rate of reported symptoms was then correlated with each of
wide-ranging population of skilled, experienced laparo- our survey’s seven demographic factors to calculate
scopic or minimally invasive practitioners. The invitation influence.
included the information that completion of the survey The study revealed a lack of symptom correlation to
was voluntary and that the survey was for research purposes measures of years in practice or age. Only hand symptoms
only and was devoid of any personal identifiers. A link in showed any significant relationship to age, with younger
the e-mail permitted access to the online survey. A week surgeons or those over 60 years of age at highest risk for
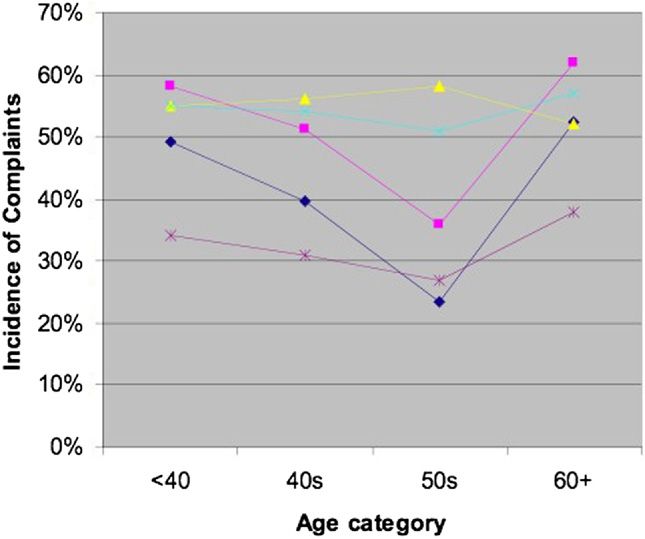
before the survey deadline, a follow-up e-mail was sent. exhibiting hand problems (left hand p ⬍ 0.006, right hand308 Park et al Patients Benefit While Surgeons Suffer J Am Coll Surg
Table 1. Survey Structure Table 2. Demographic Information
Question Answer* Demographic factors Data
Demographics Age, y, mean (SD) 44.3 (8.4)
1. What is your age? S Height, cm, mean (SD) 69.6 (3.4)
2. What is your height? S Gender, n (%)
3. What is your gender? S Male 261 (83)
4. What is your dominant hand? S Female 54 (17)
5. How many laparoscopic cases do you perform a Dominant hand, n (%)
year? S Right 272 (86)
6. Have you completed a laparoscopic fellowship? S Left 21 (7)
7. How many years have you been practicing Ambidextrous 24 (7)
laparoscopic surgery? S Annual case volume, mean (SD) 212 (127)
Physical symptoms Fellowship experience, n (%)
8. Have you ever had any physical discomfort or Fellowship 110 (35)
symptoms you would attribute to your
laparoscopic operating? S No fellowship 207 (65)
9. If you answered yes to question 8, which of the Practice length, y, mean (SD) 9.8 (5.6)
following apply? (numbness, stiffness, fatigue,
pain, and history of treatment received for each
individual body part†) M significant correlations were discovered with regard to
10. Please describe any other injuries or conditions symptoms in the neck (p ⬍ 0.05), right hand (p ⬍ 0.001),
that were not included above. D and lower extremities (p ⬍ 0.005). Increased case volume
11. When do these symptoms or discomforts also predicted the incidence of symptoms in both upper
bother you? M and lower extremities (all p ⬍ 0.05, Fig. 2). Symptoms
12. How have you attempted to minimize these were reported with higher incidence for the surgeon’s dom-
problems or conditions? M
inant hand (significant at p ⬍ 0.05 only for right-handed
13. To which of these factors do you attribute your
physical complaints? M
surgeons).
Ergonomics
Data confirmed generally accepted gender demograph-
14. How aware are you of the recommendations
ics. Women were shorter than men (65.3 inches versus 70.4
made by the field of surgical ergonomics, its inches, p ⬍ 0.001) and reported a smaller glove size (aver-
studies and research? S age size 6.57 versus 7.85, p ⬍ 0.001). Gender was also a
15. Where did you acquire this information? M factor in that women reported more arm symptoms and
16. Have you applied any of this information to men reported more lower extremity problems.
your surgical practice? S Survey question 10 asked about physical conditions or
Environment and equipment injuries not covered by the physical discomfort and symp-
17. What references do you use when adjusting the toms addressed in questions 8 and 9. Responses varied
operating room table height? M from headaches and finger calluses to disc problems. Sev-
18. What kind of display system do you use? S eral injuries were reported by more than one participant.
19. How is your display system mounted? S Among them were carpal tunnel syndrome (4 responses),
20. Improving which of these display parameters disc problems (4), headache (3), tennis elbow (2), and
would be most helpful to you? M
shoulder muscle spasm (2).
21. What size surgical gloves do you wear? S
22. Do you feel that the laparoscopic instrument
handles are: S Symptom timing and minimization
23. If available, would you utilize laparoscopic Efforts to specifically isolate the times that symptoms were
instruments in more lengths? S bothersome are illustrated in Table 3. Overall, 58% (184 of
*Answer: (S) single answer, (M) multiple selections available, (D) descriptive. 272 of the 317 participants) reported they were aggravated
†
Body parts: eyes, neck, upper back, lower back, hips, knees, ankles, feet, (the by symptoms or discomforts that they associated with per-
left and right side of ) shoulder, elbow, wrist, thumb, other fingers.
forming MIS. Sixty-two percent of those also reported that
their symptoms or discomforts continued after performing
p ⬍ 0.029; Fig. 1). Annual case volume of laparoscopic operations. About a quarter of those who experience symp-
procedures did, however, provide a key to predicting phys- toms or discomforts while and after performing surgery
ical symptoms. When fellowship was equated in terms of also reported having these problems persistently. Twenty-
case volumes (average volume nonfellow, 192; fellow, 249), four percent of all participants indicated that symptoms orVol. 210, No. 3, March 2010 Park et al Patients Benefit While Surgeons Suffer 309
Figure 2. Reports of symptoms in neck and upper and lower ex-
tremities as plotted against increasing annual case volume of lapa-
Figure 1. Age and incidence of complaints for right and left hand roscopic procedures. Left hand, blue diamond; right hand, pink
(showing significant age effects) and neck, back and lower extremity square.
symptoms, which did not show age-related differences. Left hand,
blue diamond; right hand, pink square; neck, yellow triangle; back,
turquoise stars; lower extremity, purple star.
Asked what operating room factors they would attribute
their physical complaints to, 74.4% of all participants in-
dicated instrument design. Two factors—operating room
discomforts were experienced immediately after but not table setup and display monitor location—were cited by
while performing operations, although the majority of 40% of participants, and type of display system was iden-
these respondents (95%) did not relate that these problems tified as contributory by 12% of all those reporting.
were persistent. About 15% of all participants answered
that they did not experience symptoms or discomfort at Ergonomic knowledge
any time. Five discrete levels (not aware to very aware) were available
When asked how they have attempted to minimize these to describe the degree of awareness the responding sur-
problems or conditions, 84% of participants answered that geons possessed in regard to recommendations that have
they did so by changing postural position. For approxi- been put forth by researchers in the field of surgical ergo-
mately 30% of all survey respondents, actions such as nomics. Participant answers are shown in Figure 3. More
changing instruments or taking a break were reported as than half (58.7%) of participating surgeons reported being
minimization techniques. Forty percent of all participants slightly or not aware of the recommendations. The average
answered that they would just ignore any such problem. level of awareness at 2.37 fell between slightly and some-
Table 3. Time Frames Associated with Symptom Experience
When do the symptoms or discomforts
bother you? Frequency, n %
While performing surgery, immediately after,
and persistently 26 8.2
While performing surgery, immediately after
but not persistently 88 27.8
While performing surgery, not immediately
after, still persistently 4 1.3
Only while performing surgery 66 20.8
Not while performing surgery but immediately
after and persistently 4 1.3
Only immediately after and not persistently 71 22.4
Nothing bothers me 47 14.8
Not answered 11 3.4
Figure 3. Surgeon respondents’ reported levels of awareness in
Total 317 regard to ergonomic knowledge.310 Park et al Patients Benefit While Surgeons Suffer J Am Coll Surg
Table 4. Instrument Handle Size Preferences
Instrument handle Too big, % Just right, % Too small, %
Standard graspers 11 75 14
Needle drivers 15 76 9
Energy/coagulation
devices 21 68 11
Stapler 40 59 1
respondents rated the handles of four types of instruments
as “just right” for their hands. Significant differences were
evident among tool types (p ⬍ 0.001). Graspers and needle
drivers had the highest ratings as being “just right;” staplers
Figure 4. Sources from which surgeon respondents acquired job-
relevant ergonomic information. were reported as too big by 40% of respondents, with only
1% reporting them as too small. Seventy-nine percent of
what aware. Overall, grand rounds were revealed to be the respondents reported that they would use instruments of
least effective source for learning about ergonomic recom- different lengths if such instruments were available.
mendations (Fig. 4). Surgeons who reported any level
(slightly aware to very aware) of ergonomic knowledge had DISCUSSION
primarily acquired such information from literature For surgeons who have been doing laparoscopic surgery for
(66.8%) and from regional or national meetings (54.6%). most of the past 2 decades, it will come as no surprise that
The correlation of the responses given in regard to aware- the initially reported rates of MIS-related symptoms far
ness level with the responses given about source of infor- underestimate the reality experienced and reported by the
mation indicated that those who had rated themselves as contemporary MIS surgeon. As we continue 20 years later
very aware had obtained their ergonomic information from to use instruments not “purpose designed” for laparoscopy,
surgical training (43.8%). The correlation rate significantly but hastily borrowed and adapted from our otolaryngology
decreased when surgical training as a source of ergonomic colleagues,18 it is hardly surprising that a physical toll has
knowledge was calculated for those reporting a lower level been exacted from surgeons. We continue to contort our-
of awareness (11.9%). When all participants reporting any selves on a daily basis—often working around or accom-
level of ergonomic knowledge were taken into account, modating MIS instruments and equipment—to ensure our
only 60% answered that they had applied such information patients the best outcomes possible. It is within the context
to their surgical practices. When we isolated only those of this accepted—albeit challenging—baseline existence
who were very aware of ergonomic information, however, that our survey explores the potential ergonomic impact of
the rate of application to practice significantly increased, to MIS on the surgeon.
93.3%. That 87% of surgeons who regularly perform MIS suffer
performance-related symptoms is without a doubt the
Environment and equipment most startling finding in this study and underscores the
A total of 67.4% of participants reported using a liquid urgent need for applicable ergonomic research. Recent data
crystal display system, with 25% of them still using that from limited studies suggest that between 40% and 60% of
type of monitor mounted on a cart. Our study data showed MIS surgeons experience occupational injuries.7,19 Previ-
that the percentage of participants experiencing eye strain ously published surveys comparably sized to ours have re-
and neck stiffness did not differ based on use of display type ported rates of MIS-related symptoms and injury in the
or mounting (p ⬎ 0.05, p ⬎ 0.05). Seventy-one percent of 12% to 20% range.16,17 These latter percentages are often
stationary display users and 48% of mobile mount display those quoted in meetings during which issues of symptoms
users requested improvements in regard to monitor posi- and injury related to laparoscopic performance are dis-
tioning. Sixty-five percent of cathode ray tube users in ad- cussed. Why then is there a disparity in terms of the
dition to 48% of liquid crystal display users asked for im- number—86.9%—we now report? The continuing rise in
proved resolution. No significant differences in terms of MIS technique adoption rates, with more surgeons over
demands for improvements in regard to display monitor greater lengths of time performing more MIS procedures,
size, color or number were found between cathode ray tube might be considered, even more than survey methodolo-
and liquid crystal display users. gies, to be a factor of influence.
Responses to questions about instrument handle size Throughout the time that this study was conducted and
revealed a general satisfaction (Table 4). Overall, 69% of during its presentation at the Clinical Congress of theVol. 210, No. 3, March 2010 Park et al Patients Benefit While Surgeons Suffer 311 American College of Surgeons in 2008, a surprising num- Although ergonomic sizing has been incorporated into ber of surgeons from across the country have communi- objects as mundane as office equipment, it has yet to be cated personally with the senior author, sharing anecdotally achieved with respect to surgical instruments. Surgical the extent to which their MIS-related occupational symp- gloves are produced in eight sizes, from 5.5 to 9.0, in in- toms have affected or even limited their (general) surgical crements of 0.5, with all surgeons knowing their exact practices. Such accounts, though not reportable, are glove size. Yet even with such well-documented and well- noteworthy. understood differences in hand size, surgical instruments The data presented in this article serve as a clarion call to are produced in a single size. Resolve for such equipment improve operative working conditions for the MIS sur- issues would benefit from studies grounded in anthropo- geon. Saying this does not divert us from being mindful of metric data characterizing the population of laparoscopic study limitations. Our low initial response rate might have surgeons in terms of body size and proportion. occurred for any of a number of reasons. E-mail filtering The main predictor of surgeon symptoms in our study systems might have blocked our initial invitation. Our sur- was MIS case volume. Surgeon gender, age, height, or vey was lengthy because it was comprehensive, so perhaps it handedness did not independently correlate with develop- was not easily responded to by surgeons caught in busy ment or existence of MIS-related symptoms. Analysis of schedules and other time demands. We might have distrib- these four subgroups presents a consistent message about uted our survey at surgical conferences in addition to the risk factors: the number of cases performed per year is a e-mail. Although we cannot limit the overall effects pre- stronger predictor of symptomology than either age or sented by the self-selection bias that is unavoidable in any years in practice. Some of the subgroup analyses, such as voluntary survey methodology, we did attempt to collect correlation of effects of handedness with dominant hand demographic data on the respondents so that we could symptoms were limited because of the small number of assess symptom prevalence in well-described cohorts. We participants in the left-handed subgroup (n ⫽ 20 left also attempted to include all relevant factors suspected of handed). Other results are likely the result of a weak or contributing to symptom prevalence to be able to deter- nonexistent effect of the nonsignificant variables. The find- mine the effects of such factors. Our sample does include ings are important because they suggest that the stresses of respondents of both genders, with a range of ages, years in surgery do not discriminate between young and old: if a practice, and case volumes. Examining these four contrib- surgeon performs a sufficient volume of cases, he or she is uting factors does limit selection bias effects in the suba- likely to suffer symptoms. nalysis of groups. Our data suggest that high case volume, That there are risk factors outside of personal demo- for example, will lead to more symptoms, though this re- graphics is already well documented. van Veelen and col- lationship cannot be proved to be causal within the current leagues22 developed ergonomic guidelines for the laparo- methodology. scopic surgeon with five areas of focus: instrument Routinely, laparoscopic surgeons face challenges in con- (handheld) design; monitor position; use and placement of ducting operations that are not encountered by their col- foot pedals; operating room table height; and surgeon leagues performing open procedures. Having lost direct (static) body posture. Although their suggestions derived visual connection to the operative field, MIS surgeons from an appropriately comprehensive approach and may work in three dimensions while guided by two dimensional provide helpful direction, the supporting data are not deep. images, meaning that their visual axes (eyes to monitor) are Hallbeck and associates23 point to new international stan- at odds with working or motor axes (instruments to target dards governing the usability of medical instruments and anatomy).20 The surgeon must move the instrument han- devices with the hope of increasing patient and surgeon dle “south,” and to dissect in an “easterly” direction the safety. From an ergonomic and human factors perspective, hand pieces must be moved “westward” (the fulcrum ef- such efforts must be expanded to optimize the interface of fect), as laparoscopic instruments are fixed in the abdomi- surgeon, machine, and patient. nal wall by means of a trocar such that to move a grasper tip Changing postural position clearly presented as the fa- “north.” These most fundamental movements are counter- vored method used by our respondents to minimize their intuitive to those learned for open surgery performance, reported symptoms and discomforts. Given the static pos- still laparoscopic surgeons daily perform marvelous, com- tures required by MIS performance, this is not surprising. plex procedures, having adjusted to the loss of the more Fatigue decrease has been ergonomically demonstrated as than 20 degrees of freedom associated with the hand and possible when laparoscopic surgeons shift posture.24 Other used during open surgery, with the result being that they research indicated that the strategic movements of a are limited to fewer than six degrees of freedom.21 surgeon—with an identified wrist complication—could
312 Park et al Patients Benefit While Surgeons Suffer J Am Coll Surg
appear to indicate postural instability yet actually be nec- range, including investigation of whether deleterious ergo-
essary for the achievement of successful task performance.25 nomic impact on surgeons ever results in patients suffering
Postural adjustments can be identified and correlated with adverse events; accumulation of knowledge about the
skill level through the recently identified analytic tool com- health and physical activity experienced by surgeons out-
prised of postural stability demand data combined with side the operating room; review of occupational data relat-
center of mass and center of pressure data.26 The discom- ing ergonomics to unfavorable effects (eg, shortened prac-
fort accompanying static laparoscopic surgical posture has tices and disability claims); and determination of the
been addressed by Albayrak and colleagues,27 who re- incidence of ergonomic-related work leave or case cancel-
examined fundamentally the surgeon-patient “interface,” lation. A similar survey in terms of open surgery perfor-
with the result being their design of a new ergonomic body mance could, in the future, be a source of valuable addi-
support for surgeons. Although it will take time to know tional data. Also vital to improving the design of operative
whether such a fresh approach will gain traction, this type work space, laparoscopic or open, is an understanding of
of creativity directed toward MIS ergonomics will be nec- optimal surgical movement. Yet there is a marked paucity
essary on a broad front to solve the problems our study of such knowledge. Sadly, a surgeon can much more easily
identifies. obtain a detailed ergonomic assessment and direction for
Our findings differ from those of others10 in terms of the improvement of his or her golf swing31,32 than of his surgi-
relative impact of monitor position (tower or suspended) or cal “stance” or movement. Much work remains to be done
type (cathode ray tube or flat screen) in regard to surgeon in the establishment of a “matrix of surgical movement.”
symptoms. The reasons for this are unclear. Few would Now, especially in the face of an impending shortage of
argue against the recommendation that correct placement general surgeons in the US,33 the last thing that we as a
of an optimized surgical image or screen plays a significant society can afford is surgical careers shortened by occupa-
role in surgeon comfort. Several ergonomic studies have tionally related symptoms and conditions. That research
compared different laparoscopic display monitor locations must more clearly and emphatically define the ergonomic
impact of MIS on the practicing surgeon (then set about
(in front of, to the left, or to the right of the surgeon) and
improving it) is now all too painfully clear.
heights (eye level and hand level).28-30 These studies showed
that the surgeons’ task performance was better with a dis-
Author Contributions
play monitor either placed in front rather than to the left or
right of the surgeon or at the surgeon’s hand rather than eye Study conception and design: Park Lee, Dexter
level. Yet another study demonstrated that when the mon- Acquisition of data: Park Lee
itor was at eye compared with hand level, muscular activi- Analysis and interpretation of data: Park Lee, Seagull,
ties of the neck measured by electromyography were lower Meenaghan
than expected, indicating less stress.19 We found MIS sur- Drafting of manuscript: Park, Lee, Seagull
geons continuing to experience eye and neck issues and Critical revision: Park, Lee, Seagull
seeking improvements both in terms of the currently used
boom mount and higher resolution liquid crystal displays. Acknowledgments: We thank Rosemary Klein for her edit-
Our results suggest that more detailed ergonomic studies ing contributions.
investigating this still unresolved and ergonomically risky
surgeon-technology interface are necessary.
An encouraging finding of our survey was that those REFERENCES
possessing knowledge of MIS ergonomic recommenda- 1. Cuschieri A. Whither minimal access surgery: tribulations and
tions were very inclined to apply such guidelines in their expectations. Am J Surg 1995;169:9–19.
practices. Still, our respondents’ low awareness level about 2. Cuschieri A. The spectrum of laparoscopic surgery. World J Surg
existing research recommendations to ergonomically im- 1992;16:1089–1097.
prove MIS surgical performance and associative symptoms 3. Kant IJ, de Jong LC, van Rijssen-Moll M, et al. A survey of static
and dynamic work postures of operating room staff. Int Arch
and discomforts makes clear that such guidelines must be Occup Environ Health 1992;63:423–428.
more appropriately and widely disseminated to practicing 4. Patkin M, Isabel L. Ergonomics, engineering and surgery of
surgeons. endosurgical dissection. J R Coll Surg Edinb 1995;40:120–132.
Inevitably, many more questions are raised than are an- 5. Berguer R, Forkey DL, Smith WD. Ergonomic problems asso-
ciated with laparoscopic surgery. Surg Endosc 1999;13:466–
swered by a study such as ours. Future research needs to go 468.
more deeply yet broadly into the effects of surgery-related 6. Matern U, Kuttler G, Giebmeyer C, et al. Ergonomic aspects of
ergonomic difficulties. Such studies should span a wide five different types of laparoscopic instrument handles underVol. 210, No. 3, March 2010 Park et al Patients Benefit While Surgeons Suffer 313
dynamic conditions with respect to specific laparoscopic tasks: 20. Matern U, Faist M, Kehl K, et al. Monitor position in laparo-
an electromyographic-based study. Surg Endosc 2004;18: scopic surgery. Surg Endosc 2005;19:436–440.
1231–1241. 21. Albanese CT. Making it easier. Pediatr Endosurg Innovat Tech
7. van Veelen MA, Nederlof EAL, Goossens RHM, et al. Ergo- 2002;6:171.
nomic problems encountered by the medical team related to 22. van Veelen MA, Jakimowicz JJ, Kazemier G. Improved physical
products used in minimally invasive surgery. Surg Endosc 2003; ergonomics of laparoscopic surgery. Min Invas Ther Allied Tech-
17:1077–1081. nol 2004;13:161–166.
8. Matern U. Ergonomic deficiencies in the operating room: ex- 23. Hallbeck MS, Koneczny S, Büchel D, et al. Ergonomic usability
amples from minimally invasive surgery. Work: A Journal of testing of operating room devices. Studies in health technology
Prevention, Assessment, and Rehabilitation 2009;33:165–168. and informatics 2008;132:147–152.
9. Matern U, Waller P. Instruments for minimally invasive surgery:
24. Uhrich ML, Underwood RA, Standeven JW, et al. Assessment of
principles of ergonomic handles. Surg Endosc 1999;13:174–
fatigue, monitor placement, and surgical experience during sim-
182.
ulated laparoscopic surgery. Surg Endosc 2002;16:635–639.
10. van Det MJ, Meijerink WJHJ, Hoff C, et al. Optimal ergonom-
ics for laparoscopic surgery in minimally invasive surgery suites: 25. Lee G, Kavic SM, George IM, et al. Postural instability does not
a review and guidelines. Surg Endosc 2009;23:1279–1285. necessarily correlate to poor performance: case in point. Surg
11. Kranenburg G. Ergonomic problems encountered during Endosc 2007;21:471–474.
video-assisted thoracic surgery. Minim Invasive Ther Allied 26. Lee G, Park AE. Development of a more robust tool for postural
Technol 2004;13:147–155. stability analysis of laparoscopic surgeons. Surg Endosc 2007;
12. Berguer R, Rab GT, Abu-Ghaida H, et al. A comparison of 22:1087–1092.
surgeons’ posture during laparoscopic and open surgical proce- 27. Albayrak A, van Veelen MA, Prins JF, et al. A newly designed
dures. Surg Endosc 1997;11:139–142. ergonomic body support for surgeons. Surg Endosc 2007;21:
13. Berguer R, Chen J, Smith WD. A comparison of the physical 1835–1840.
effort required for laparoscopic and open surgical techniques. 28. Hanna GB, Shimi SM, Cuschieri A. Task performance in endo-
Arch Surg 2003;138:967–970. scopic surgery is influenced by location of the image display.
14. Berguer R, Smith WD, Chung YH. Performing laparoscopic Ann Surg 1998;227:481–484.
surgery is significantly more stressful for the surgeon than open 29. Omar AM, Wade NJ, Brown SI, et al. Assessing the benefits of
surgery. Surg Endosc 2001;15:1204–1207. “gaze-down” display location in complex tasks. Surg Endosc
15. Lawther RE, Kirk GR, Regan MC. Laparoscopic procedures are 2005;19:105–108.
associated with a significant risk of digital nerve injury for gen- 30. van Veelen MA, Jakimowicz JJ, Goossens RH, et al. Evaluation
eral surgeons. Ann R Coll Surg Engl 2002;84:443–444. of the usability of two types of image display systems, during
16. Berguer R. Surgery and ergonomics. Arch Surg 1999;134: laparoscopy. Surg Endosc 2002;16:674–678.
1011–1016.
31. McHardy A, Pollard H. Muscle activity during the golf swing.
17. van Veelen MA, Meijer DW. Ergonomics and design of laparo-
scopic instruments: results of a survey among laparoscopic sur- Br J Sports Med 2005;39:799–804.
geons. J Laparoendosc Adv Surg Tech A 1999;9:481–489. 32. McHardy A, Pollard H, Bayley G. A comparison of the modern
18. Edmonson JM. History of the instruments for gastrointestinal and classical golf swing: A clinician’s perspective. South Afr
endoscopy. Gastrointest Endosc 1991:37:S27–S56. J Sports Med 2006;18:80–92.
19. Reyes DAG, Tang B, Cuschieri A. Minimal access surgery 33. Polk HC Jr, Vitale DS, Qadan M. The very busy urban surgeon:
(MAS)-related surgeon morbidity syndromes. Surg Endosc another face of the evermore obvious shortage of general sur-
2006;20:1–13. geons. J Am Coll Surg 2009;209:144–147.You can also read