Pelvic Floor Health Patient Information Leaflet - Derriford Hospital
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Patient Information Leaflet
Pelvic Floor Health
University Hospitals Plymouth NHS Trust
Derriford Road
Plymouth
PL6 8DH
Tel: 01752 202082
www.plymouthhospitals.nhs.uk
1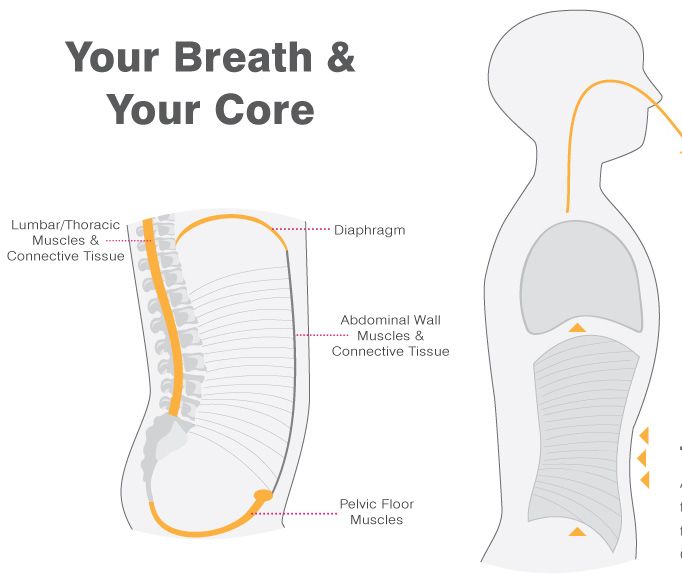
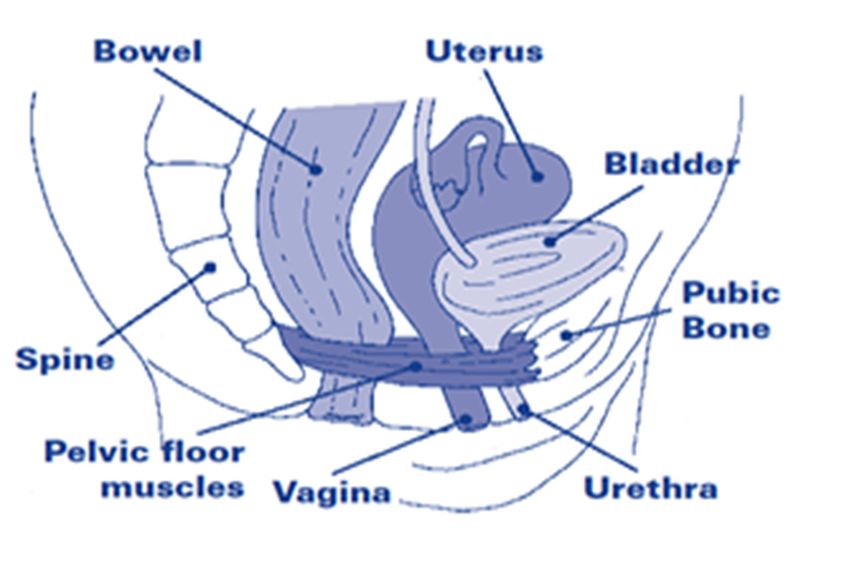
What is the pelvic floor?
The pelvic floor is made up of layers of muscle and soft tissue
which form a sling, like a hammock, from the pubic bone at
the front of the pelvis to the base of the spine at the back. The
supportive muscles are called the pelvic floor muscles. Along
with the ligaments and soft tissue, they help to keep the
bladder, womb and bowels in the right place and working
normally.
How does the pelvic floor work?
The pelvic floor muscles usually work without us having to
think about them. The muscles are kept firm and slightly
tense to stop leakage (incontinence) of urine from the
bladder or faeces from the bowel. When you empty your
bladder or bowel the pelvic floor muscles relax. Afterwards,
they tighten again to restore control. The pelvic floor muscles
help to keep your pelvic organs in the correct position
(preventing prolapse). They work in combination with other
core muscles to support our lower back and trunk and also
provide support to the vaginal wall; they can also help you
feel more sensation during sex.
Our pelvic floor muscles should silently do their job, allowing
us to function without interruption throughout the day and
night. There are many factors and life events however that
can weaken the muscle, and yet many people are unaware or
do nothing to ensure good health of these very important
muscles.
2
Picture of female pelvic floor muscles
Image used with kind permission from POGP
Why does the pelvic floor become weak?
Pelvic floor muscles can become weak due to:
• Pregnancy and childbirth.
• Lack of exercise.
• The menopause.
• Weight gain.
• Increasing age.
• Previous surgery.
• Straining to empty bowels (constipation).
• Persistent heavy lifting.
3
Signs and symptoms of a weak Pelvic Floor
Incontinence:
Incontinence is the involuntary loss of urine. There are two
different types of incontinence.
Stress Urinary Incontinence
The complaint of involuntary leakage of urine on effort,
exertion, or on cough or sneeze.
Physical movements or straining causes extra pressure
in the abdomen and this puts more pressure on the
bladder. If the pelvic floor muscles that support and close
off the bladder’s opening don’t work properly, urine leaks
out.
Urge Urinary Incontinence
Involuntary urine leakage accompanied by or
immediately preceded by an urgency to urinate.
This is also called Over-active Bladder.
Some people have both types which we term Mixed
Incontinence.
4Pelvic Organ Prolapse
Prolapse
A pelvic organ prolapse refers to the drop, bulging or
herniation of one or more of the pelvic organs into the vagina.
It occurs when the muscles, ligaments and other soft tissue,
called fascia, weakens and is unable to support the organs.
Symptoms include:
A heavy dragging feeling in the vagina and sometimes in
the back.
A feeling of a lump in or coming out of the vagina. Some
people report it feeling like a loose tampon or small golf
ball.
Changes to urinary flow, it may slow down or feel like you
don’t completely empty your bladder. Some people
experience increase in frequency or urgency and some
stress incontinence.
Bowel symptoms such as not being able to empty
properly, or needing to press on the vaginal wall to empty
the bowel.
Prolapse symptoms are often worse at the end of the
day, with prolonged standing.
A prolapse can be mild causing little or no bother, or may be
severe causing many problems and affecting a person’s
quality of life.
5Causes of prolapse
A number of life factors can cause damage to the muscles,
ligaments fascia and nerves.
The main causes are from:
Pregnancy and childbirth (1 in 3 ladies are affected). The
weight of the developing baby puts strain on the
structures. An episiotomy, tear or delivery requiring
forceps can add to the weakening of the soft tissue.
Aging and the menopause may further weaken the pelvic
floor structures.
Obesity, chronic cough, chronic constipation, heavy lifting
and straining are all conditions that can cause excessive
pressure on the pelvic floor.
Some conditions such as Ehlers-Danlos Syndrome and
Marfans Syndrome affect the strength of connective soft
tissues.
Where do prolapses occur?
The prolapse is usually described according to the area of the
vagina in which it occurs.
An anterior vaginal prolapse generally involves the
bladder, and sometimes the urethra. The term cystocele
is used by the medical profession. This is the most
common prolapse.
A posterior vaginal prolapse occurs when the lower
part of the large bowel (Rectum) bulges into the back
wall of the vagina, often referred to as a Rectocele.
An apical prolapse occurs when the uterus drops down
into the vagina. Often called a uterine prolapse. If you
have had a hysterectomy your vagina can drop
downwards, this is known as a vaginal vault.
Many women can have more than one prolapse.
6What you can do
Pelvic organ prolapses are unfortunately common. It is
estimated that approximately 40% of woman over 50 have
some form of prolapse.
Woman with prolapses have been found to have weaker
pelvic floor muscles. It therefore makes sense, and evidence
has shown that a pelvic floor exercise programme can be
effective in reducing the prolapse symptoms.
Follow all the advice in this booklet with regards to
strengthening your pelvic floor muscle. In addition, make
sure you follow all the bowel and life style advice. Try to
break your daily activities into shorter periods of standing,
taking regular breaks to sit for a while. Keep active, but
consider exercises which are lower impact such as low
impact aerobics, cycling, swimming and Pilates.
7Why should you exercise your pelvic floor?
As has been discussed, weak or untrained muscles can
give you less control and support of your bladder or bowel,
and so can be the cause of urinary leakage, faecal leakage
or prolapse.
Pelvic floor exercises can strengthen these muscles so that
they once again give support. This can improve your
prolapse, and helps you to regain control of your bladder and
bowel to improve or stop leakage.
You may find the exercises difficult at first, but with patience
and perseverance over 3 to 4 months you should notice a
difference. Like other muscles in the body the more you
regularly use and exercise them the stronger they will be.
Evidence has shown that effective strength training of the
pelvic floor muscle three to five times a day, every day; over
12 weeks can alter and improve muscle function.
Your physiotherapist will guide you on how to do a
proper/good pelvic floor muscle contraction, and how to build
fast and slow endurance holds. They will guide you through
appropriate challenges to maximise your results and enable
you to carry out your everyday activities with minimal
problems.
8Learning to do pelvic floor exercises
Squeeze/tighten the muscles around your back passage,
as if you were trying to stop yourself from passing wind.
Tighten/lift the muscles at the front as if you were trying
to stop the flow of urine.
Now squeeze/tighten/lift both the back and front together
as tight as you can. We call this your maximum hold.
You should feel your lower tummy muscles gently
working, but your thighs and buttocks should not be
working.
Make sure you breathe normally and do not hold your
breath.
Burrell 2018
My best cure for a pelvic floor contraction is:
9How to check
If you are unsure that you are exercising the right muscles,
check the exercises by putting one or two fingers into the
vagina. If you are tightening the pelvic floor muscles, you
should feel a gentle squeeze and inward lift.
Practising your exercises
To change the quality and strength of your pelvic floor muscle
you will need to practice your exercises 3 times a day for 3-4
months. After that, to ensure you maintain the improvement
you have made in this time, you will need to do your pelvic
floor exercises once a day for life.
It is good to practice your exercises in different positions. Try
standing, sitting and lying down. Start with the position that is
easiest until you have the hang of it.
Many women find it useful to make a list of activities that will
prompt them to do their exercises
• Whilst having a tea break.
• When watching TV.
• After using the toilet.
• When washing your hands or the dishes.
• Driving to work/school run.
I will do my exercises:
1)
2)
3)
10‘The knack’:
Quickly tighten the pelvic floor before exertion
When the pelvic floor is working as it should it will
automatically contract before, and during any increase in
pressure in the abdomen; such as during a cough, a sneeze,
when blowing your nose, stepping down heavily, going from
sit to stand or when lifting.
Woman often lose the reflex to contract the pelvic floor
muscles just before a cough/sneeze. This often happens
after pregnancy and childbirth, after prolonged straining to
open bowels, or after pelvic surgery.
They will often leak with any increase in pressure from above.
By learning to actively contract the pelvic floor muscles just
before the increase in abdominal pressure, woman can learn
to overcome the bladder leakage. This has become known as
“The Knack”.
The contraction of pelvic floor muscles will help to close the
urethra (urine tube), and protect the pelvic organs, minimising
prolapse and urine leakage.
Practice makes perfect: practise the knack initially with an
empty bladder. After you have emptied your bladder, do the
knack and have a light cough. Over the next few days
challenge yourself with a stronger cough.
Once you are feeling happy with this, leave an hour after
emptying your bladder (the bladder will have filled a little) and
try again with progressively stronger coughs.
As well as with coughs, put the knack into practice with daily
activities which are prone to cause you difficulties, such as
lifting.
11With practice you will have trained a learned habit, your brain
will be used to the sequence of prepare, protect, cough, and
you will start to do it on auto pilot.
Sneezes, coughing fits and vomiting are harder to resist with
the knack due to the increased abdominal pressure. Work on
getting the lighter coughs sorted first and with on-going
practice the rest will follow.
12Exercise Diary
Slow pull-ups
Hold your pelvic floor maximal squeeze for as long as
possible (up to 10 seconds) and then let go. Then see how
many times you can do that in a row with a 3-4 second rest
between each squeeze.
I managed a hold of ______seconds, repeated _____times
My goal is to hold for seconds, repeat times.
Fast pull-ups
Maximally squeeze tightly and then relax your pelvic floor,
count how many times you can do this in a row until the
muscles tire.
I managed ______ fast contractions in a row
My goal is to do fast contractions.
13Progressing your exercises
Be realistic about how often you can do the exercises, but
aim to do them three times daily.
Over the weeks try to beat the score (length of hold) you had
previously. If you started with 5 repetitions of a 3 second
hold, after a few days try 6 repetitions of a 3 second hold,
over time slowly increase.
The aim is that by the end of each session your pelvic floor
will feel tired. As the muscles get stronger, you will find that
you can tighten for longer and do more exercises.
Build up to being able to hold for 10 seconds and repeat 10
times slow endurance holds, and 10 fast.
Record your progress on the Exercise Diary provided.
It takes time for exercises to make the muscles stronger. You
may not notice improvement for several weeks, so stick at it!
Record in the chart (page 15) how many seconds hold and
how many repetitions of each exercise you manage on a daily
basis.
For example:
Wed
6 sec x 3
8 fast
14Exercise Diary Record
Mon Tue Wed Thurs Fri Sat Sun
15Normal Bladder
A healthy bladder can hold around 400-600ml, it is normal to
go to the toilet approximately 7 to 9 times a day and once
during the night. As you age (over 70yrs) it is normal to go to
the toilet twice a night.
As the bladder starts to fill it sends warning messages to the
brain. You will normally feel the first warning that you need
the toilet when there is roughly 200ml of urine in your bladder.
If you decide it is not convenient to go to the toilet your brain
will send messages to your bladder to not respond and you
can continue with whatever you are doing at the time.
Normally we can hold on for a little longer until your bladder
has filled a bit more and it is an appropriate time to visit the
toilet. Once sitting on the toilet the pelvic floor muscles will
relax and the bladder muscle will squeeze until all the urine
has been emptied.
16What is Overactive Bladder (OAB)
If your bladder is Overactive you are likely to feel you
desperately need to rush to the toilet (Urgency), and
sometimes you may leak before you get there (Urge
incontinence).
You may go to the toilet more than once at night (nocturia),
and a lot more during the day than those around you
(frequency).
Some people get into the habit of going to the toilet more
often than they need to in an attempt to prevent unwanted
accidents. This, however, has the potential to make things
worse in the long run.
If you go to the toilet often the bladder gets used to being less
full, so overtime the bladder can become more sensitive and
overactive when it is only stretched a little.
It is not fully understood what causes OAB, but there are
steps you can take to resolve or improve your symptoms.
17What you can do to help keep a healthy bladder
Use of Frequency Volume Chart
The first step is to be aware of what your bladder habits are.
Frequency volume charts can be used to increase this
awareness.
Over three days you will need to take note of what you are
drinking, how much you are drinking, and using a measuring
jug note how much volume you urinate. If you have to wake
at night to go to the toilet this is also noted, as are any leaks.
The overall pattern can then be discussed with your
physiotherapist or any other health care professional involved
in your bladder control care.
Filling in the chart should also make you aware of which
aspects of the healthy bladder training are most important for
you.
Making small changes in your daily habits can start to show
positive changes in your symptoms.
Re-doing the fluid diary 6 weeks later should hopefully show
you how far you have progressed and improved.
If your physiotherapist has not issued you a frequency volume
chart you can print one off from University Hospitals
Plymouth Website.
https://www.plymouthhospitals.nhs.uk/physio-patient-information
18Bladder retraining
The purpose of bladder retraining or bladder drill is to learn to
supress or ignore the desire to pass urine, and enable the
bladder to tolerate being stretched and steadily increase its
capacity. Over time this will lead to a reduction in the
frequency and urgency of needing the toilet and a more
normal pattern of going to the toilet.
The ideal time between visits to the toilet is 3 to 4 hours, and
the average volume of urine should be approximately 300ml.
Training your bladder to be able to tolerate this takes effort
and time.
Your brain has a big part to play in bladder retraining. The
brain has to make a sensible story of all the information it
receives, it is the brain that decides how much urgency you
feel, not your bladder. The brain will use various centres of
the brain to work out what it needs to do. Past memories,
emotional centres, thought and learning centres are all
involved in the decision to empty your bladder. If the brain
uses all these centres and perceives you are in danger of
losing control of your bladder, it will communicate this to your
spinal cord, and you will act on the urge and rush to the toilet.
If we always give into our urge our bladder and brain get used
to the bladder holding less and the brain will continue to
trigger the urgency mechanism.
The aim and goal of Bladder Retraining or Bladder Drill is
to quieten the nervous system and allow “normal” messages
to travel between the brain and the bladder.
19Tips to help hold for longer:
• Keep calm. Stop and stand still if the urge is strong.
• Go up and down on your toes, or curl your toes.
• Take a few deep breaths.
• Distract your mind i.e.: count backwards from 50.
• Do 5 quick pull ups.
• Pull up your pelvic floor muscle and hold for 10 seconds.
Squeezing your pelvic floor muscles sends messages to your
brain which can help to suppress the urge.
Set realistic targets; when you feel the need to go to the toilet
try to hold on for an extra 5 -10 mins using the techniques
mentioned above. Try to gradually increase the time between
visits to the toilet, eventually you will be able to leave around
3 to 4 hours between visits. Remember, when you have
regained control, do not go longer than 4-5 hours without
passing urine (except of course overnight).
Stop going to the toilet for “just in case” wees. Many people
do these before work or before getting into the car. It is better
to listen to your bladder and go when it is full even if it means
finding a toilet when you are out.
It may take several weeks or months to get to this stage.
Retraining your bladder habits requires considerable will
power and determination, and only you can do it, just
remember giving in to your bladder will only make things
worse.
20Relationships and OAB
Overactive bladders can often affect a women’s sexual
health. It can cause discomfort and leaking during sexual
intercourse, and can reduce the desire and ability to achieve
orgasm. Visiting the toilet before intercourse may help. It is
worth talking to your partner so they understand, and you
may want to try different positions that put less pressure on
your bladder.
Medications for OAB
There is a range of medication that can help with the
symptoms of OAB. Used in combination with bladder
drill/retraining and lifestyle changes they may improve
symptoms. If you have been prescribed any OAB
medications you may need to take it for a few weeks before
you notice a difference. Your GP will inform you how long you
will need to take this medicine for.
How do the medications work?
Medications called Anticholinergics (e.g. Oxybutynin,
fesoterodine, solifenacin) reduce the contractions by blocking
the messages sent to the bladder. This will reduce the feeling
of needing to go to the toilet and cuts down on the number of
leaks. Anticholinergics can have side effects, 1 in 3 people
will experience a dry mouth, less common side effects are
constipation, taste disturbances, dry eyes, blurred vision and
drowsiness. If you experience side effects you may be given
an alternative medicine called Mirabegron. Mirabegron
relaxes the bladder muscle reducing the activity of the muscle
and therefore decreasing the urge, it can take up to 8 weeks
to take effect.
21Other life style changes that can help
Do pelvic floor exercises
Doing regular pelvic floor exercises have been shown to
improve bladder control.
Watch what you drink
Try to reduce coffee, tea, and fizzy drinks and anything
containing alcohol or caffeine as these can increase bladder
activity and lead to leakage. Other known bladder irritants are
drinks with artificial sweeteners, citrus juices, blackcurrant
juice and tomatoes. Moderation is the key. If you are
planning on cutting out caffeine, do so gradually so you don’t
get a headache.
A good amount of fluid to consume is 6-8 cups of liquid each
day (about 1.5 to 2 litres). If you drink too little it can lead to
concentrated urine which can irritate the bladder and cause
urgency or incontinence. Too little fluid can also cause
constipation. However drinking excessive amounts can also
cause a problem with frequency. If you are pregnant, breast
feeding, exercising or it is hot you will require more fluid.
Try to drink non irritable drinks which include water, fruit or
herbal teas, milk, soups, and diluted juice drinks.
Try to spread your drinks out in the day and avoid drinking
late into the night. Stop drinking 2 hours before you go to
bed.
22Avoid irritating foods
Some foods can worsen incontinence in certain people.
Watch out for chocolate (another source of caffeine), as well
as spicy food or acidic foods like tomatoes and citrus fruits as
these are common irritants to the urinary tract.
To identify potential culprits, eliminate one type of food every
two to three weeks to see if your symptoms improve.
Do not underestimate the effect of food and drink
and its effects on your bladder and bowel.
Don’t smoke
Cigarette smoke and nicotine act as immediate bladder
irritants. Smoking can also increase the risk of bladder cancer
over the long term. The chronic cough often associated with
smoking can also lead to accidental leakage and weaken the
pelvic floor. If you need help quitting visit:
www.smokefree.nhs.uk
http://www.oneyouplymouth.co.uk/
Protect yourself from UTIs
Urinary Tract Infections (UTIs) can cause temporary episodes
of incontinence because of the bacteria that commonly invade
the bladder and weaken the muscles in the urethra. A UTI will
not trigger incontinence for most people, but it can make a
difference if you are incontinence prone.
Empty your bladder before and after intercourse to cut your
risk of UTIs.
Keep a healthy weight
The heavier you are the more weight presses on the pelvic
floor muscle and bladder. Maintaining a healthy weight can
reduce the pressure on the bladder.
http://www.oneyouplymouth.co.uk/
23Avoid constipation
Constipation can place added pressure on the bladder and
increases the need to urinate more urgently and frequently.
Common causes of constipation are irregular meals and not
enough fibre in the diet, a lack of physical activity,
dehydration and some medications.
The word constipated can mean different things to different
people. Constipation is generally defined by doctors as a
person having any of the following features:
Opening of the bowels fewer than 3 times a week.
Needing to strain to pass stools.
Hard and lumpy stools which may be large or small in
size.
Finding it difficult or are unable to completely empty your
bowels.
Having to use a finger or hand to help you to pass stool.
You may also experience stomach aches and cramps, feeling
bloated, diarrhoea alternating with constipation, and
backache.
Don’t ignore the body’s signals to have a bowel movement.
This often occurs after a meal, particularly breakfast. A hot
drink in the morning may stimulate the contractions of the gut
and encourage a bowel movement.
If you have any of the following symptoms for more than 6
weeks, then you need to see your GP: a continuing change in
bowel habit, unexplained bleeding from the back passage,
abdominal (stomach) pain or discomfort, weight loss or
tiredness.
24What causes constipation and what to do to
improve
The exact cause of constipation may be difficult to identify,
however there are a number of things that may contribute to
the condition, including:
Not drinking enough: the body needs around 2 litres of fluid
a day to function efficiently. Without sufficient fluids, stools dry
out making them harder to move through the bowel.
Diet: dietary fibre provides the bulk that helps to speed the
passage of waste food through the bowel. Lack of fibre
results in harder, more compacted stools which take longer to
pass. Keep the bowels running smoothly with a healthy intake
of fibre 20 to 35mg a day. Eat regular meals to get your
bowels working. Do not skip meals especially breakfast, as it
can make your bowel sluggish or irregular. Avoid hurrying
your meals and chew your food properly. Avoid processed
foods and foods with a high fat content. Eat a diet with a
healthy amount of both soluble (vegetables and fruit) and
insoluble (cereals /wholegrains) fibre. Try to eat at least 5
portions of fruit and / or vegetables a day.
Lack of exercise: if you don’t exercise regularly, things can
slow down, including muscle contractions that move stools
through the gut.
Pregnancy: Hormonal changes in pregnancy can slow down
the gut movements, and in later pregnancy, the baby pushes
the bowel making it more difficult for stools to move. New
mothers may find they cannot respond to the urge to open the
bowels and they run into problems through a lack of routine.
25Some medications: can cause constipation as a side effect.
For example, painkillers like co-codamol, codeine and
morphine slow down the bowel. Iron tablets and some of the
medication used to treat heartburn, high blood pressure, heart
problems, depression and Parkinson’s disease.
A decrease in thyroxine levels in the blood, due to a
condition called hypothyroidism, can slow down the bowel.
Similarly, increased levels of calcium in the blood called
hypercalcaemia can slow down the bowel leading to
constipation.
Following any major surgery: this is due to a variety of
factors such as painkillers, an inability to push due to pain
following surgery, decreased food intake and damage to
various nerves in the pelvis following some major pelvic
operations.
Eating disorders: patients with an eating disorder cannot be
expected to have regular bowel actions due to a lack of
roughage. They may continue to have constipation even after
normalisation of eating behaviour, due to the inability of their
bowel to fully recover.
Lifestyle: people sometimes feel unable to open their bowels
due to various reasons, for example stress, poor toilet access
or their busy life schedule. Consequently, they tend to ignore
the sensation of needing to go to the toilet to open their
bowels and over the years, their bowel slows down, resulting
in constipation.
Psychological disturbances: major events in life such as
bereavement can result in constipation. Constipation is
common in people suffering with anxiety and depression.
26Sit correctly on the toilet
Sitting correctly on the toilet will enable efficient emptying of
the bladder and bowel and will prevent straining.
The best way to open your bowels is by using your abdominal
(stomach) muscles to push. Feet up on a footstool, leaning
forward, supporting your elbows on your thighs and bulge
your abdominals outwards (make your waist go wide). Now
use these abdominal muscles as a pump to push backwards
and downwards into your bottom. Relax your back passage.
Some people see some improvement in their symptoms
within a few weeks; however, have patience as for many it
can take a few months.
If you have any further questions please do ask your Doctor,
Practice/District Nurse, Health Visitor, Continence Adviser or
Physiotherapist for help.
27This leaflet is available in large print and other
formats and languages.
Contact: Administrator
Tel: 01752 432233
Ref: GDRIVE, Physiotherapy, MSK OUTPATIENTS, CLINICAL, PATIENT INFORMATION
HANDOUTS, WOMANS HEALTH, Pelvic Floor Health
University Hospitals Plymouth NHS Trust does not tolerate any form of
discrimination, harassment, bullying or abuse and is committed to ensuring that
patients, staff and the public are treated fairly, with dignity and respect.
University Hospitals Plymouth NHS Trust operates a smoke-free, policy,
including e-cigarettes. You cannot smoke anywhere on site. For advice on
quitting, contact your GP or the NHS smoking helpline free, 0800 169 0169
Date issued: October 2019
For review: October 2021
Ref: C-387/VWH/Physiotherapy/Pelvic Floor Health
28You can also read