Predictive Factors for Differentiating Between Septic Arthritis and Lyme Disease of the Knee in Children
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
721
C OPYRIGHT 2016 BY T HE J OURNAL OF B ONE AND J OINT S URGERY, I NCORPORATED
A commentary by Elan J. Golan, MD, and
Jeffrey D. Thomson, MD, is linked to the
online version of this article at jbjs.org.
Predictive Factors for Differentiating Between
Septic Arthritis and Lyme Disease of the
Knee in Children
Keith D. Baldwin, MD, MSPT, MPH, Christopher M. Brusalis, BA, Afamefuna M. Nduaguba, MD, and Wudbhav N. Sankar, MD
Investigation performed at The Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania
Background: Differentiating between septic arthritis and Lyme disease of the knee in endemic areas can be challenging
and has major implications for patient management. The purpose of this study was to identify a prediction rule to dif-
ferentiate septic arthritis from Lyme disease in children presenting with knee pain and effusion.
Methods: We retrospectively reviewed the records of patients younger than 18 years of age with knee effusions who underwent
arthrocentesis at our institution from 2005 to 2013. Patients with either septic arthritis (positive joint fluid culture or synovial white
blood-cell count of >60,000 white blood cells/mm3 with negative Lyme titer) or Lyme disease (positive Lyme immunoglobulin G on
Western blot analysis) were included. To avoid misclassification bias, undiagnosed knee effusions and joints with both a positive
culture and positive Lyme titers were excluded. Historical, clinical, and laboratory data were compared between groups to identify
variables for comparison. Binary logistic regression analysis was used to identify independent predictive variables.
Results: One hundred and eighty-nine patients were studied: 23 with culture-positive septic arthritis, 26 with culture-
negative septic arthritis, and 140 with Lyme disease. Multivariate binary logistic regression identified pain with short arc
motion, history of fever reported by the patient or a family member, C-reactive protein of >4 mg/L, and age younger than
2 years as independent predictive factors for septic arthritis. A simpler model was developed that showed that the risk of
septic arthritis with none of these factors was 2%, with 1 of these factors was 18%, with 2 of these factors was 45%, with
3 of these factors was 84%, or with all 4 of these factors was 100%.
Conclusions: Although septic arthritis of the knee and Lyme monoarthritis share common features that can make them
difficult to distinguish clinically, the presence of pain with short arc motion, C-reactive protein of >4.0 mg/L, patient-
reported history of fever, and age younger than 2 years were independent predictive factors of septic arthritis in pediatric
patients. The more factors that are present, the higher the risk of having septic arthritis.
Level of Evidence: Diagnostic Level III. See Instructions for Authors for a complete description of levels of evidence.
Peer Review: This article was reviewed by the Editor-in-Chief and one Deputy Editor, and it underwent blinded review by two or more outside experts. The Deputy Editor
reviewed each revision of the article, and it underwent a final review by the Editor-in-Chief prior to publication. Final corrections and clarifications occurred during one or
more exchanges between the author(s) and copyeditors.
A
cute bacterial septic arthritis is most often a surgical present with fever, joint effusion, irritability, and inability to
emergency. However, differentiating septic arthritis of the bear weight on the affected extremity. In addition, laboratory
knee from Lyme disease in children with symptoms of measurements, including erythrocyte sedimentation rate (ESR),
knee pain and swelling can be very challenging. Clinical pre- C-reactive protein (CRP), and peripheral and synovial white
sentations of both conditions can be quite similar. Often patients blood-cell (WBC) counts, may be elevated in both conditions1-4.
Disclosure: One author of this study (K.D.B.) received funds from JBJS for manuscript preparation. On the Disclosure of Potential Conflicts of Interest
forms, which are provided with the online version of the article, one or more of the authors checked “yes” to indicate that the author had a relevant financial
relationship in the biomedical arena outside the submitted work.
J Bone Joint Surg Am. 2016;98:721-8 d http://dx.doi.org/10.2106/JBJS.14.01331722
TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG
d
P R E D I C T I O N A L G O R I T H M F O R S E P T I C A R T H R I T I S C O M PA R E D WITH
V O LU M E 98 -A N U M B E R 9 M AY 4, 2 016
d d
LY M E D I S E A S E O F T H E K N E E I N C H I L D R E N
TABLE I Patient Data
Groups
Lyme Disease Culture-Negative Septic Arthritis Culture-Positive Septic Arthritis
No. of cases* 140 26 23
Mean age† (yr) 8.03 ± 4.0 2.1 ± 1.7 5.6 ± 1.6
Sex*
Male 93 13 12
Female 47 13 11
*The values are given as the number of patients. †The values are given as the mean and the standard deviation.
In spite of the overlap in both clinical presentation and take several days to be finalized. As a result, frontline clinicians
laboratory testing, it is imperative that the treating physician are often faced with a challenging scenario: a child with knee
makes an accurate diagnosis because each condition has very pain and effusion and indeterminate serum and synovial lab-
different implications for treatment. Because pyogenic septic oratory values. In these circumstances, one must weigh the risk
arthritis can result in rapid articular cartilage destruction, of delayed or untreated septic arthritis against the potential for
emergent irrigation and drainage in the operating room are an unnecessary surgical procedure or serial aspirations, which
warranted. In contrast, Borrelia burgdorferi, the causative organ- are less than ideal in a children’s hospital where anxiety at
ism in Lyme disease, stimulates an immune complex-mediated multiple needle sticks is undesirable.
inflammatory reaction that does not endanger the articular car- In the absence of a quick and accurate test to defini-
tilage to the same degree, but does cause systemic immune- tively diagnose Lyme disease, prediction algorithms that
driven medical complications5. Standard treatment generally combine multiple clinical and laboratory factors have been
involves an appropriate course of antibiotics and observation developed to identify patients at high risk for pyogenic ar-
for other sequelae of systemic Lyme disease. thritis and to help to guide treatment decisions 6-9. Although
In most pediatric medical centers, confirmatory testing these models have proven helpful in differentiating septic
for Lyme disease involves serum Western blot analysis for Lyme arthritis from transient synovitis of the hip, their utility in
immunoglobulin G (IgG), but the results of this testing may differentiating septic arthritis from Lyme disease of the knee
TABLE II Univariate Analysis of Culture-Positive Septic Arthritis Compared with Lyme Arthritis for Clinical and Laboratory Findings
Culture-Positive Septic Arthritis* (N = 23) Lyme Disease* (N = 140) P Value
Duration of symptoms (d) 3.2 ± 2.1 6.1 ± 9.3 0.268
History of antibiotic use 21.7% 6.4% 0.019
History of fever 73.9% 40.7% 0.001
Radiographic effusion 78.3% 95% 0.999
Micromotion tenderness 86.4% 6.3%723
TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG
d
P R E D I C T I O N A L G O R I T H M F O R S E P T I C A R T H R I T I S C O M PA R E D WITH
V O LU M E 98 -A N U M B E R 9 M AY 4, 2 016
d d
LY M E D I S E A S E O F T H E K N E E I N C H I L D R E N
TABLE III Univariate Analysis of Culture-Negative Septic Arthritis Compared with Lyme Arthritis for Clinical and Laboratory Findings
Culture-Negative Septic Arthritis* (N = 26) Lyme Disease* (N = 140) P Value
Duration of symptoms (d) 4.5 ± 3.2 6.1 ± 9.3 0.625
History of antibiotic use 23.1% 6.4% 0.030
History of fever 76.9% 40.7% 0.001
Radiographic effusion 96.2% 95% 0.999
Micromotion tenderness 58.8% 6.3%724
TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG
d
P R E D I C T I O N A L G O R I T H M F O R S E P T I C A R T H R I T I S C O M PA R E D WITH
V O LU M E 98 -A N U M B E R 9 M AY 4, 2 016
d d
LY M E D I S E A S E O F T H E K N E E I N C H I L D R E N
Materials and Methods logical testing, blood and joint fluid cultures, Gram stains of the joint fluid,
ESR, and CRP.
W e conducted a retrospective study of individuals younger than 18 years of
age who presented to the emergency department of a large tertiary care
children’s hospital between 2005 and 2013 and in whom an arthrocentesis was Statistical Analysis
performed for knee joint effusion. The study was approved by our institutional Data were analyzed using SPSS version 22.0 (IBM). Descriptive elements of the
board review prior to data collection. Study patients were identified through a data are presented as means (and ranges) and categorical variables are presented
query of the laboratory database of our electronic medical record system for all as counts (and percentages). Cutoff values for continuous variables, CRP of
patients in the emergency department for whom joint or synovial fluid analysis >4 mg/L and age younger than 2 years, were determined with receiver operating
was ordered. Identified patients were then cross-referenced with the labo- characteristic curve analysis. Mann-Whitney U tests were used to evaluate
ratory results of Gram-staining, microbial culture, and synovial WBC count to differences between groups in continuous or ordinal variables in cases where
identify patients with septic arthritis and were cross-referenced with the the data were not normally distributed and to identify variables for multi-
results of the Lyme Western blot analysis to identify patients diagnosed with variate analysis. A chi-square test was used to determine significance in the
Lyme disease. case of binary or categorical data. Level of significance was established at a two-
The emergency department records of each identified patient were sided alpha level of p < 0.05. Variables that significantly influenced the diag-
reviewed to confirm the diagnosis of either pyogenic septic arthritis or Lyme nosis of septic arthritis were included in a binary logistic regression with a
arthritis and to extract clinical and laboratory data. To create the cleanest stepwise backward elimination method (with a cutoff for elimination of 0.1) to
cohort to minimize misclassification bias, we defined septic arthritis as either determine factors predictive of septic arthritis. Simpler dichotomized models
the presence of a positive joint fluid culture irrespective of synovial cell were generated using the risk factors and were confirmed using 22 log like-
count (culture-positive septic arthritis) or synovial WBC count of >60,000 lihood methodology. Models were generated for Lyme disease compared with
white blood cells/mm3 in a joint with a negative Lyme titer (culture-negative culture-positive septic arthritis and for Lyme disease compared with all cases
septic arthritis). Lyme disease was defined as the presence of a positive serum of septic arthritis.
Lyme IgG on Western blot based on our reference laboratory definitions.
Patients who did not meet the criteria for a diagnosis of septic arthritis and Patient Demographic Characteristics
who did not have a Lyme titer sent within the same emergency department During the study period, a total of 841 children were identified as having had an
evaluation were excluded from the study. To avoid misclassification bias, arthrocentesis performed in the emergency department, of which 498 were
undiagnosed knee effusions and joints with both a positive culture and positive knee aspirations. After cross-referencing identified patients with the results
Lyme titers were excluded. In patients with multiple peripheral blood of the microbial culture and Lyme disease immunoblot assays and applying
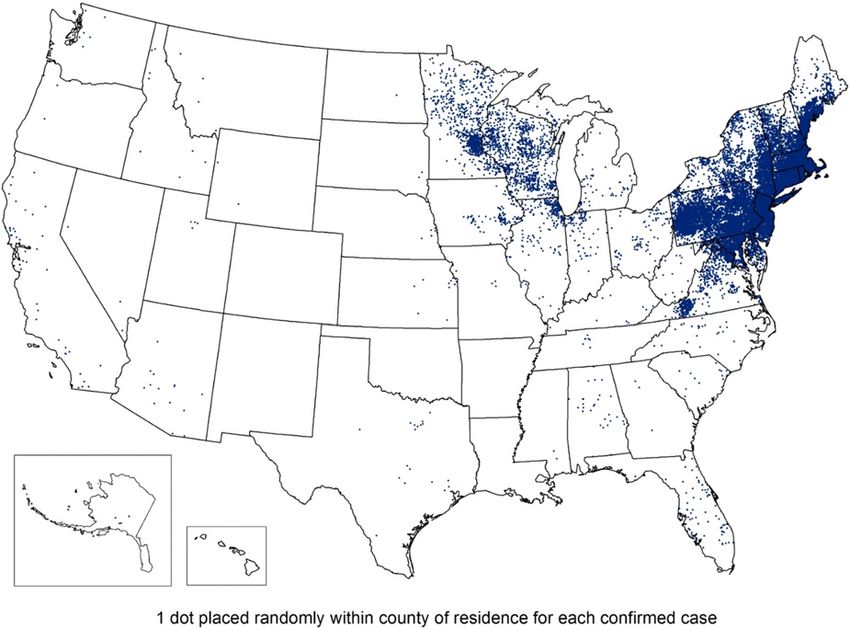
analyses and joint aspirations during the same hospitalization, we limited our further exclusion criteria (Fig. 1), we identified 189 patients as our study
data analysis to the first peripheral laboratory values and to the initial aspirate cohort (49 with septic arthritis and 140 with Lyme disease) (Table I).
sample. Of the 23 patients with culture-positive septic arthritis, organisms in-
For each patient, we recorded data on demographic characteristics, cluded methicillin-susceptible Staphylococcus aureus (MSSA) (11 patients),
medical comorbidities, historical elements, physical examination findings, and methicillin-resistant Staphylococcus aureus (MRSA) (4 patients), Propionibacterium
results of laboratory testing, including complete blood-cell count, Lyme sero- acnes (2 patients), Clostridium bifermentans (1 patient), Streptococcus pneumoniae
Fig. 1
Consolidated Standards of Reporting Trials (CONSORT) diagram of the study population. SA = septic arthritis, CNSA = culture-negative septic arthritis,
Dx = diagnosis, WB1 = positive white blood-cell count, and Hx = medical history.725
TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG
d
P R E D I C T I O N A L G O R I T H M F O R S E P T I C A R T H R I T I S C O M PA R E D WITH
V O LU M E 98 -A N U M B E R 9 M AY 4, 2 016
d d
LY M E D I S E A S E O F T H E K N E E I N C H I L D R E N
TABLE V Univariate Analysis of Operatively Treated Lyme Arthritis Compared with Nonoperatively Treated Lyme Arthritis
Operative Group* (N = 46) Nonoperative Group* (N = 94) P-Value
Temperature (F) 99.3 ± 1.3 99.1 ± 1.2 0.08
Serum WBC count (·109 cells/L) 11.2 ± 3.6 9.6 ± 2.8 0.010
Absolute neutrophil count (cells/mm3) 5,727 ± 2,122 5,726 ± 2,121 0.061
ESR (mm/hr) 52 ± 21 37 ± 21726
TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG
d
P R E D I C T I O N A L G O R I T H M F O R S E P T I C A R T H R I T I S C O M PA R E D WITH
V O LU M E 98 -A N U M B E R 9 M AY 4, 2 016
d d
LY M E D I S E A S E O F T H E K N E E I N C H I L D R E N
count alone may lead to a high rate of unnecessary surgical Three previous studies have specifically sought to identify
procedures. Furthermore, the results of Lyme-specific serologi- predictive factors for differentiating septic arthritis from Lyme
cal testing can take several days and therefore are not helpful for disease. Thompson et al.11 evaluated 179 patients with mono-
making an urgent surgical decision. As a result, Lyme disease is arthritis of different joints (not just the knee) and identified
often mistaken for culture-negative septic arthritis and is history of fever and elevated CRP to be negative predictors of
treated as such with incision and drainage, unnecessarily ex- Lyme arthritis and knee involvement to be a positive predictor
posing these patients to the risks of a surgical procedure4. (model sensitivity of 88% and specificity of 82%). In spite of
In the absence of an easily administered test with high this, the authors concluded that there was too much overlap in
sensitivity and specificity for definitively diagnosing septic ar- the data to create a clinically useful predictive model. Milewski
thritis, previous studies have used multiple physical examina- et al.15 compared 123 patients with Lyme disease with 51 pa-
tion and laboratory factors to create prediction models that tients with culture-positive septic arthritis, although several
help to identify patients at high risk for pyogenic arthritis. different joints were included in their analysis. Based on mul-
Kocher et al.8 developed a widely used set of criteria to differ- tivariate analysis, the authors found that refusal to bear weight
entiate septic arthritis from transient synovitis of the hip using was the most predictive factor, with weaker predictors being
4 independent clinical variables: history of fever, non-weight- presence of a fever, WBC count of >12 · 1,000/mL, and nu-
bearing status, ESR of ‡40 mm/hr, and serum WBC count of cleated cell count of >100,000 cells/mm3. Interestingly, CRP
‡12 · 109 cells/L. This model has since been validated internally and ESR were not found to be useful predictors, although the
and externally, and updated to reflect the additional diagnostic study was limited by a very low CRP collection rate during the
benefit of CRP6. Although the Kocher model is often applied to study period. A recent study by Deanehan et al. is the only
multiple joints even in the setting of Lyme disease, this pre- previous one, to our knowledge, that compared predictive
dictor was not originally intended to distinguish between factors for Lyme disease with those for septic arthritis specifi-
septic arthritis and Lyme disease and was not validated for the cally of the knee10. Unlike the aforementioned studies (and
knee. The septic arthritis cohort studied by Kocher et al. con- ours), the authors found ESR to be an independent predictor of
sisted of all patients with synovial leukocyte counts in excess of septic arthritis in Lyme disease-endemic areas; the other factor
50,000 cells/mm3 regardless of bacterial culture results and that they found to be predictive was an absolute neutrophil
therefore may have inadvertently included patients with Lyme count of ‡10,000 cells/mm3, which we also did not detect in our
disease and other misclassification biases. Indeed, a recent study study. However, their data were limited by a low CRP collection
by Deanehan et al. demonstrated synovial WBC counts in excess rate (77%) and a small number of patients with septic arthritis
of 50,000 cells/mm3 to be quite common in Lyme arthritis16, (19). In addition, the Lyme disease cohort included a significant
and these findings were reiterated by this current study. proportion of patients (58%) who did not undergo arthrocentesis.
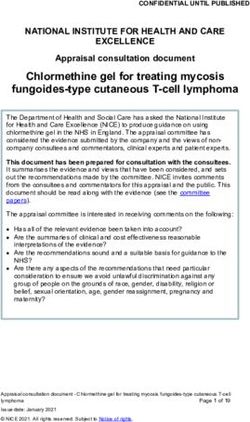
Fig. 2
Map of reported cases of Lyme disease in the United States, 2014. (Reproduced from: CDC, National Center for Health Statistics. Lyme Disease. 2015
Oct 2. http://www.cdc.gov/lyme/stats/index.html. Accessed 2016 Jan 26.)727
TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG
d
P R E D I C T I O N A L G O R I T H M F O R S E P T I C A R T H R I T I S C O M PA R E D WITH
V O LU M E 98 -A N U M B E R 9 M AY 4, 2 016
d d
LY M E D I S E A S E O F T H E K N E E I N C H I L D R E N
These latter types of patients can typically be triaged to ob- To provide a clinically useful prediction model, we de-
servation by the treating physician and are rarely, by clinical fined septic arthritis as either the presence of a positive joint
examination, suspected of having septic arthritis. These patients culture or as a synovial WBC count of >60,000 white blood
may therefore not represent the types of clinical presentations cells/mm3 with negative Lyme serological results. Although there
that are easily confused with those having true pyogenic arthritis. is a small risk of misclassification bias using this second def-
In this present study aimed at differentiating septic ar- inition, ignoring the large number of patients who present to
thritis of the knee from Lyme monoarthritis, we found several emergency departments with culture-negative septic arthritis
independent predictive factors for pyogenic arthritis: patient or would limit the clinical applicability of any prediction rule.
family-reported history of fever, pain with short arc motion, This study had several limitations. First, as a chart review,
CRP of ‡4 mg/L, and age younger than 2 years. The probability it had the potential loss of data fidelity associated with retro-
of septic arthritis with any one factor present was 18% com- spective analysis. Second, as a single-center study in a Lyme
pared with 100% with all 4 factors present. Logistic regression disease-endemic area, the results of this study may not be ap-
of predictor variables showed that 87% of cases were correctly plicable to all geographical regions, particularly those with a low
predicted with our model. In our series, a patient with no risk prevalence of Lyme disease. The Centers for Disease Control and
factors had a 2% chance of being diagnosed with septic ar- Prevention (CDC) has reported that, in 2014, 96% of confirmed
thritis, and a patient with 4 factors had a 100% chance of septic cases of Lyme disease occurred in 14 U.S. states, concentrated in
arthritis. Notably, of 46 patients with Lyme disease who un- the Northeast and upper Midwest (Fig. 2)17. Therefore, the find-
derwent a surgical procedure, 11 patients had no clinical pre- ings of this study may be most applicable to these geographic
dictors. Thus, applying this clinical prediction rule may have regions. The strengths of the study include rigorous definitions
avoided a surgical procedure in 23.9% of patients in this of the cohorts and data acquisition and statistical analysis methods
cohort. Of the remaining 35 patients with Lyme disease who that limit misclassification and observer bias. Additionally, to our
underwent a surgical procedure, 19 had one clinical predictor, knowledge, our study is the first to identify predictive risk factors
14 had 2 predictors, 2 had 3 predictors, and no patient had all that, in our cohort, ensured the diagnosis of septic arthritis when
4 predictors. It is important to note that the results of this study all were present (i.e., the diagnosis was septic arthritis in 100%
may not be applicable in a non-endemic area with a lower of cases) and resulted in only one case of septic arthritis when
prevalence of Lyme disease. all 4 risk factors were absent (2%).
Interestingly, we found pain with short arc motion to be In conclusion, our study offers a useful prediction algo-
the most clinically useful test for septic arthritis, with a sensi- rithm for septic arthritis compared with Lyme disease of the
tivity of 0.78 and a specificity of 0.92. Multivariate analysis knee. We believe that a patient older than 2 years of age without
showed that the adjusted odds of having septic arthritis with history of fever, no short arc pain, and CRP of728
TH E JO U R NA L O F B O N E & JO I N T SU RG E RY J B J S . O RG
d
P R E D I C T I O N A L G O R I T H M F O R S E P T I C A R T H R I T I S C O M PA R E D WITH
V O LU M E 98 -A N U M B E R 9 M AY 4, 2 016
d d
LY M E D I S E A S E O F T H E K N E E I N C H I L D R E N
7. Jung ST, Rowe SM, Moon ES, Song EK, Yoon TR, Seo HY. Significance of labo- 12. Bennett OM, Namnyak SS. Acute septic arthritis of the hip joint in infancy and
ratory and radiologic findings for differentiating between septic arthritis and transient childhood. Clin Orthop Relat Res. 1992 Aug;(281):123-32.
synovitis of the hip. J Pediatr Orthop. 2003 May-Jun;23(3):368-72. 13. Forlin E, Milani C. Sequelae of septic arthritis of the hip in children: a new
8. Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and classification and a review of 41 hips. J Pediatr Orthop. 2008 Jul-Aug;28(5):
transient synovitis of the hip in children: an evidence-based clinical prediction al- 524-8.
gorithm. J Bone Joint Surg Am. 1999 Dec;81(12):1662-70. 14. Gillespie R. Septic arthritis of childhood. Clin Orthop Relat Res. 1973 Oct;
9. Molteni RA. The differential diagnosis of benign and septic joint disease in chil- (96):152-9.
dren. Clinical, radiologic, laboratory, and joint fluid analysis, based on 37 children 15. Milewski MD, Cruz AI Jr, Miller CP, Peterson AT, Smith BG. Lyme arthritis in
with septic arthritis and 97 with benign aseptic arthritis. Clin Pediatr (Phila). 1978 children presenting with joint effusions. J Bone Joint Surg Am. 2011 Feb 2;
Jan;17(1):19-23. 93(3):252-60.
10. Deanehan JK, Kimia AA, Tan Tanny SP, Milewski MD, Talusan PG, Smith BG, 16. Deanehan JK, Nigrovic PA, Milewski MD, Tan Tanny SP, Kimia AA, Smith BG,
Nigrovic LE. Distinguishing Lyme from septic knee monoarthritis in Lyme disease- Nigrovic LE. Synovial fluid findings in children with knee monoarthritis in Lyme dis-
endemic areas. Pediatrics. 2013 Mar;131(3):e695-701. Epub 2013 Feb 18. ease endemic areas. Pediatr Emerg Care. 2014 Jan;30(1):16-9.
11. Thompson A, Mannix R, Bachur R. Acute pediatric monoarticular arthritis: dis- 17. CDC, National Center for Health Statistics. Lyme Disease. 2015 Oct 2. http://
tinguishing Lyme arthritis from other etiologies. Pediatrics. 2009 Mar;123(3):959-65. www.cdc.gov/lyme/stats/index.html. Accessed 2016 Jan 26.You can also read