WHAT DO GLOBAL EXPERTS SAY? - ROSA BRAGA-MELE, MD, MED, FRCSC, MODERATOR THOMAS KOHNEN, MD, PHD, FEBO MARIUS SCHEEPERS, MD JERRY HU, MD JEFF HORN ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Sponsored by
Supplement to January 2020
PanOptix Trifocal IOL:
What do Global
experts say?
Rosa Braga-Mele, MD, Med,
FRCSC, Moderator
Thomas Kohnen, MD, PhD, FEBO
Marius Scheepers, MD
Jerry Hu, MD
Jeff Horn, MD
PanOptix
Trifocal IOL
Trifocal IOLs: What do
Global experts say?
E
volution is continuous in all things, and the science outcomes, but we are defined by the outcomes of the most
of cataract surgery is no exception. Every time results challenging cases. As eye care providers, we must offer a
improved, patients and surgeons themselves demanded solution that provides a range of vision to meet these higher
to see how outcomes could be even better. In light of patient expectations.
the approval of the PanOptix Trifocal IOL (Alcon) in
the United States, several cataract surgeons with clinical Marius Scheepers, MD: To meet our
experience using the PanOptix Trifocal IOL participated patients’ expectations, we must listen to
in a roundtable. Rosa Braga-Mele, MD; Marius Scheepers, their needs and provide resources and
MD; Jeff Horn, MD; Jerry Hu, MD; and Thomas Kohnen, comprehensive education. We have a
MD, PhD, discussed patient needs from both the patient responsibility to inform our patients about
and the surgeon perspective, available IOL options to all lens options available, and we are very fortunate to
mitigate presbyopia, and the global experience with the have technologies available to us that mitigate presbyopia
PanOptix Trifocal IOL. and provide patients with good vision at multiple working
distances. However, we must select the right implant for
What are the needs of the cataract patient today, each patient because there is no single solution that is good
and how can the refractive cataract surgeon meet for everyone.
these needs?
Rosa Braga-Mele, MD: When we ask Dr. Braga-Mele: The bottom line is that we need to
ourselves what our patients need, we must educate ourselves and then provide our patients with true
understand their expectations, which have informed consent for all the options that are available.
been shaped by multiple factors. Digital
access to medical information has produced What presbyopia-mitigating options and approaches
a well-informed patient generation with high expectations exist in the United States, and what are the
for their health and treatment options. Patients today have limitations?
these higher expectations because they are often paying Dr. Braga-Mele: We’ve been able to offer presbyopia-
out-of-pocket costs for health care, prompting patients correcting intraocular lenses (PCIOLs) for well over a decade.
to expect more than the good distance vision afforded by We have also seen a definite progression in premium IOLs
monofocal IOLs. The digital era has also created a generation over those 10 years. However, a 2018 ASCRS survey of US
with increased demand for intermediate vision. Patients surgeons indicated only a 9% market penetration of PCIOLs.1
expect clear vision at distance, but also want to see their We need to figure out how we can improve this statistic.
computers and tablets, as well as be able to read a book in What are the current presbyopia-mitigating options in the
most lighting conditions. This brings us to the question: How United States?
do we best meet the needs of these patients?
Dr. Hu: There are a number of available technologies.
Jerry Hu, MD: Twenty years ago, the visual The pseudo-accommodating IOL was the first generation
outcomes after cataract surgery were good, of PCIOLs. The lens was designed to move anteriorly or
and patients were happy. Today, we are posteriorly depending on the accommodative forces of
doing an even better job, yet some patients the eye, thus providing distance and some intermediate
seem not as happy. I think this is because vision. However, this technology has not been widely
the bar of patient expectations has risen so high that it adopted because this lens type provided limited near and
has become a different ballgame. We deliver outstanding intermediate vision improvements.
2 SUPPLEMENT TO CATARACT & REFRACTIVE SURGERY TODAY | JANUARY 2020
PanOptix
Trifocal IOL
The multifocal IOL splits light energy into two focal
points. The two focal points are simultaneously presented
to the retina providing distance and near or intermediate
vision, depending on the add power. Essentially, we are
talking about bifocal implants, which consequentially
require patients to choose between having near or
intermediate vision.
The extended depth of focus (EDOF) IOL introduces an Figure 1. One approach to achieve trifocality is the application of sequential diffractive optics.
elongated depth of focus and a range of vision from distance This is used with traditional trifocal IOLs.
to intermediate. Yet, in order to achieve both functional
distance and intermediate vision, we typically need to use
some form of monovision to widen the depth of focus.
What other approaches exist to provide a range of
vision to our patients?
Dr. Braga-Mele: Trifocal IOLs are the latest addition to
the global PCIOL landscape. Trifocal IOLs produce a range
of vision by splitting light energy into three focal points:
near, intermediate, and far. Different optical approaches
Figure 2. A theoretical IOL with four focal points (40 cm, 60 cm, 120 cm and distance)
can be used to achieve trifocality in an IOL. Dr. Horn, may not provide sufficient light energy for distance, possibly effecting distance vision
would you elaborate more on the distinct features of each performance, however when the 120-cm focal point is redirected to distance, you get
optical approach and what it means to the patients? ENLIGHTEN technology.
Dr. Horn: One way to achieve trifocality is
to use the principal of sequential diffractive
optics. Sequential diffractive optics creates
an intermediate focal point that is located
at 2 times the distance of the near focal
point. For example, if the near focal point is at 40 cm, then
intermediate is located at 80 cm (Figure 1). However, the
most common intermediate vision activities are performed
at arm’s length, or about 60 cm for the average height Figure 3. The PanOptix Trifocal IOL with ENLIGHTEN technology has three focal points
(40 cm, 60 cm, and distance).
person.2,3
Dr. Braga-Mele: How do we get to an intermediate focal result is a near foci at 40 cm, intermediate at 60 cm and
point of 60 cm? distance, thus creating a way around sequential diffractive
optics to optimize intermediate performance, while
Dr. Horn: Using the principal of sequential diffractive maintaining excellent near and distance performance of the
optics, one would need to place the near focal point at IOL. This design is ENLIGHTEN technology (Alcon).
30 cm to achieve an intermediate of 60 cm, which may The PanOptix Trifocal IOL utilizes 88% of the usable light
be too close for the vast majority of patients. We simply energy at a 3-mm pupil size, which is higher than the ReSTOR
cannot outrun physics, and we need a way around the multifocal IOLs (Alcon).4 The 4.5-mm diffractive zone with
limits of sequential diffractive optics. A way around the ENLIGHTEN technology is designed to be less dependent on
challenge is to use the non-sequential diffractive order pupil size or lighting conditions. The PanOptix Trifocal IOL
approach, which leads to four focal points: a near at 40 cm, (Figure 3) allocates 50% of the available light to distance, 25%
a first intermediate at 60 cm, a second intermediate at to intermediate, and 25% to near.5
120 cm, and distance (Figure 2). However, creating four
foci may negatively impact distance performance. The far PanOptix Trifocal IOL performance
intermediate foci at 120 cm was redirected to distance Dr. Braga-Mele: The PanOptix Trifocal IOL has been
which preserves an excellent distance performance. The investigated in a number of published studies. The lens
JANUARY 2020 | SUPPLEMENT TO CATARACT & REFRACTIVE SURGERY TODAY 3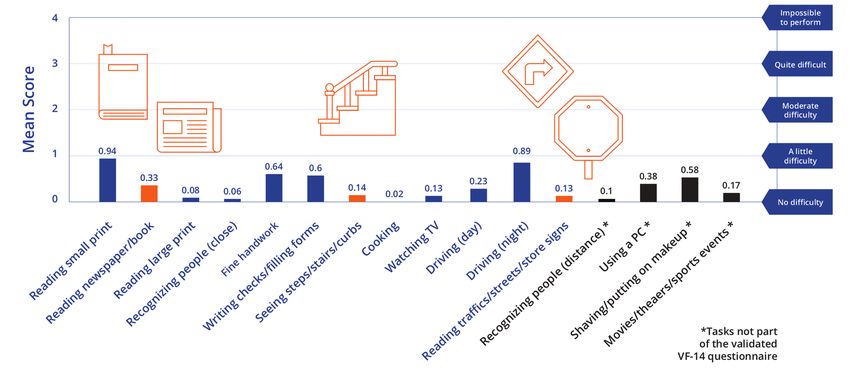
PanOptix
Trifocal IOL
Table: Visual Acuity at 12 months postimplantation with PanOptix Trifocal IOL.
The clinical study enrolled 149 patients at 17 sites in Europe, Latin America, and Australia.
LogMAR Snellen
Binocular Uncorrected Visual Acuity At distance 0.02 ± 0.11 ~20/20
At near (40cm or 16 inch) 0.07 ± 0.11 ~20/25
Binocular Distance Corrected Visual Acuity At intermediate (80 cm or 31 inch) 0.08 ± 0.14 ~20/25
At intermediate (60 cm or 24 inch) 0.04 ± 0.12 ~20/20
received CE mark in Europe in 2015 and became available in Dr. Hu: I was a clinical investigator in the PanOptix
Canada in 2017. I have personally been using the PanOptix Trifocal IOL US registration study, and in my experience
Trifocal IOL since 2017. Dr. Kohnen, being the first surgeon from the trial, I noticed that my patients can read very well,
to implant the PanOptix in the world, can you share some even in dim light at near and intermediate ranges.10 This may
of the visual outcomes that patients may experience with be attributed to the allocation of available light, with 50%
PanOptix Trifocal IOL implanted in both eyes? dedicated to distance vision, and then 50% equally divided
between intermediate (25%) and near (25%).
Prof. Kohnen: A post-market clinical
study conducted across 17 sites in Europe, How does the PanOptix Trifocal IOL compare to
Latin America, and Australia demonstrated EDOF IOLs?
that, at 12 months postoperatively, the Dr. Braga-Mele: The clinical defocus curve assessment by
PanOptix Trifocal IOL consistently provided Cochener et al.9 indicates that when the diffractive EDOF
a visual acuity of 0.02 to 0.08 logMAR (approximately and PanOptix Trifocal IOL defocus curves are superimposed
20/25 or better) under uncorrected and distance-corrected on each other at the near vision range, PanOptix remains
conditions at distance, 60 cm, 80 cm, and 40 cm, with an above 20/25, whereas the diffractive EDOF lens tapers down
overall postoperative spherical equivalent of -0.34 D ± 0.36 to 20/40 as we progress closer toward the near focal point
(Table).7 of 40 cm. Could you expand upon the range of vision of the
PanOptix Trifocal IOL versus a diffractive EDOF?
Range of vision with the PanOptix Trifocal IOL
Dr. Braga-Mele: Dr. Horn, can you talk about the range of Dr. Hu: There are important differences between the
vision with the PanOptix Trifocal IOL? defocus curve for the diffractive EDOF IOL and PanOptix
Trifocal IOL. With diffractive EDOF, intermediate and
Dr. Horn: We looked at the defocus curve of 134 patients, distance is at an appropriate level but drops off after 50 cm.
who were implanted bilaterally with the PanOptix On the other hand, the defocus curve for the PanOptix
Trifocal IOL (Figure 4).7 A defocus curve assesses the visual Trifocal IOL is wider and steadier. On the near end, even as
performance of an IOL that is designed to provide a number you bring the focal point to 16 inches (40 cm), visual acuity
of foci. To obtain a defocus curve, both eyes of a patient are is still above 20/25 (Figure 4). With PanOptix, 20/20 near,
fully distance corrected, and a series of positive and negative intermediate, and distance vision is now possible.
powered lenses are placed in front of the patient bilaterally
to simulate different distances. At each simulated distance, Prof. Kohnen: Defocus curve studies comparing the
the visual acuity of the patient is measured, which is plotted diffractive EDOF IOL to the PanOptix Trifocal IOL have
as the defocus curve. For example, a -2.5 D lens placed into all shown that, in the range from intermediate to near,
a trial frame simulates how the patient will see at 40 cm or there is a decline of one to two lines of visual acuity with
16 inches. the diffractive EDOF IOLs.9,11,12 For some of my patients,
When we look at the PanOptix Trifocal IOL defocus diffractive EDOF technology is used, but only in certain
curve (Figure 4), we see a relatively flat curve that extends patients with the right expectations about spectacle wear
even beyond infinity (0 Diopter, D). It’s really quite postoperatively. Some of the EDOF patients will still require
remarkable. +1 to +1.5 diopter reading glasses to read a book.
4 SUPPLEMENT TO CATARACT & REFRACTIVE SURGERY TODAY | JANUARY 2020
PanOptix
Trifocal IOL
Dr. Hu: I learned how to successfully incorporate mono- to need reading glasses. For our patients who demand
vision and mix-and-match approaches with multifocal or near, intermediate, and distance vision, we use trifocal
EDOF IOLs. My go-to approach was to implant the ReSTOR technology. The PanOptix IOL is expected to offer the
2.5 D with ACTIVEFOCUS design (Alcon) in the dominant benefit of increased freedom from the need of spectacles
eye and a ReSTOR +3 D in the nondominant eye. When I or contact lenses, at a range of near to distance vision.
participated in the PanOptix Trifocal IOL US registration
study, I was both pleasantly surprised and encouraged. Based Dr. Braga-Mele: I used the mix-and-match approach for
on my experience, with the PanOptix Trifocal IOL I am able about six months. Once the PanOptix Trifocal IOL came out,
to deliver excellent near, intermediate, and distance vision I also found it was no longer necessary to complicate my
without having to mix and match IOLs.10 I love the simplicity decision making with mix-and-match approaches. With the
of PanOptix. PanOptix Trifocal IOL, you don’t have to think through and
speculate as to which IOL power was the best choice for the
Prof. Kohnen: I would like to elaborate on this a little nondominant eye.
bit. With multifocal IOLs, one can mix and match to close
the intermediate vision gap as seen in the defocus curves. Dr. Scheepers: It is so much easier to implant the same
We were just studying the mix-and-match approach with lens in both eyes because, when patients have different
bifocal IOLs in Europe when trifocal technology came to lenses in each eye, they tend to compare and complain
the market. We immediately stopped the mix-and-match more about halo or differences in acuity. This does not
approach because we simply do not need it anymore. It happen when we have the same lenses in both eyes.
is so much easier to put the same IOL in both eyes with
full distance correction than to try and figure out eye Patient-reported outcomes with the PanOptix
dominance, distance power off-sets, or which add powers Trifocal IOL
to use in each situation. I am careful to tell patients who Dr. Braga-Mele: All of this leads us to the patient
are considering diffractive EDOF lenses that they are likely perspective. Dr. Scheepers, can you talk to us about patient
International Post-Marketing Study
Figure 4. Binocular distance-corrected defocus curve at 6 months postimplantation with PanOptix Trifocal IOL of n = 134 eyes as assessed in a prospective, single-arm study.7
JANUARY 2020 | SUPPLEMENT TO CATARACT & REFRACTIVE SURGERY TODAY 5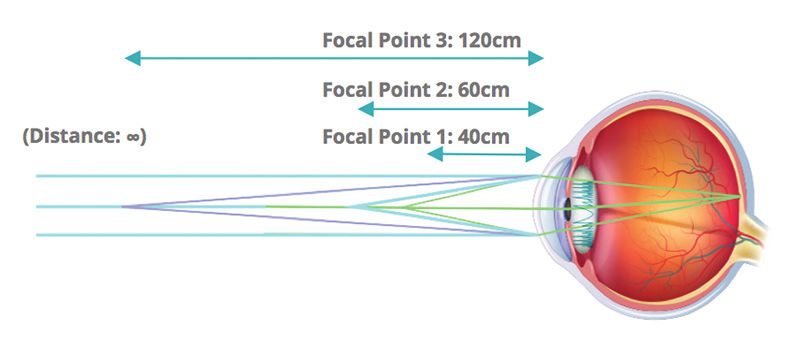
PanOptix
Trifocal IOL
outcomes with respect to the need for spectacles after Prof. Kohnen: Yes, and you touched on an important
PanOptix Trifocal IOL implantation? point. If you do scientific studies and ask really specific
What data do we have on patient reported outcomes? questions of each patient, begin to pay attention to their
reaction time. Do they have to put effort into thinking
Dr. Scheepers: If we look at the study by Akman and about it? Over time, patients adjust and forget about the
colleagues,14 they reported that 48 patients implanted phenomena unless we remind them with our questions.
bilaterally with PanOptix Trifocal IOLs had a high
vision-related quality of life. The study utilized the Visual Summary
Function Questionnaire-14 from the National Eye Institute Dr. Braga-Mele: There are several IOL modalities and
and four additional questions, and patients reported that approaches available in the United States to help patients
the tested vision-related tasks could be performed with see well at various distances. While there is no technol-
either no difficulty or a little difficulty (Figure 5). ogy today that will give a patient back their youthful
And finally, in a prospective, single-arm, post-market vision, PanOptix Trifocal IOL technology consistently
clinical study including 145 eyes across 17 clinical sites in provides good visual acuity at distance, intermediate,
Europe, Latin America, and Australia, only 2 to 3% of these and near. As with any diffractive IOL technology, there
patients reported unsolicited visual disturbances of halos are optical phenomena, however most patients are not
and glare after PanOptix Trifocal IOL implantation.7 bothered by them and adapt to their presence espe-
cially if the appropriate patient is chosen for the lens.
Dr. Braga-Mele: We talked a little bit about visual PanOptix Trifocal IOL patients are highly satisfied with
disturbances, such as halo and glare. When we look their vision.6,13 This is a technology that has the potential
at studies, we should differentiate between solicited increase the overall usage of PCIOLs. n
(surgeon-prompted) and unsolicited (self-reported). Prof. 1. Sixth Annual ASCRS Clinical Survey. eyeworld.com. http://supplements.eyeworld.org/eyeworld-supplements/
Kohnen, I believe you did a study where you looked at december-2018-clinical-survey. Accessed August 15, 2019.
visual disturbances. Can you talk to us with respect to visual 2. Charness N, Dijkstra K, Jastrzembski T, et al. Monitor viewing distance for younger and older workers. Proc Hum Factors
Ergon Soc. 2008;3:1614-1617.
disturbances?
Figure 5. Vision-related task questionnaire scores of 48 patients implanted bilaterally with PanOptix Trifocal IOL as assessed with the National Eye Institute Visual Function
Questionnaire-14 in a prospective, single-arm study.13 Patients were asked to score tasks that they perform on a daily basis with either 0 = no difficulty; 1 = little difficulty;
2 = moderate difficulty; 3= quite difficult; or 4 = impossible to perform task.
6 SUPPLEMENT TO CATARACT & REFRACTIVE SURGERY TODAY | JANUARY 2020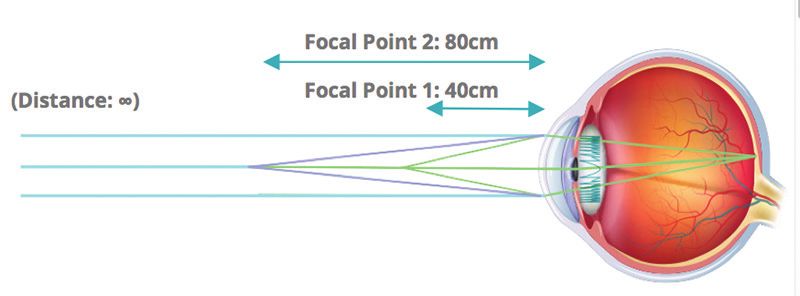
PanOptix
Trifocal IOL
3. Positioning the Monitor. ccohs.ca. https://www.ccohs.ca/oshanswers/ergonomics/office/monitor_positioning.html. extended depth of focus intraocular lenses. J Refract Surg. 2018;34(8):507-514.
Accessed August 15, 2019. 10. Hu JG, Rendon, A, Hu GY, et al. Scotopic near and intermediate vision results with a new advanced technology one
4. Kohnen T. First implantation of a diffractive quadrafocal (trifocal) intraocular lens. J Cataract Refract Surg. piece acrylic trifocal design IOL. Presented at: ASCRS. May 2019, San Diego, California.
2015;41(10):2330-2332. 11. Monaco G, Gari M, Di Censo F, et al. Visual performance after bilateral implantation of 2 new presbyopia-correcting
5. Alcon Data on File. intraocular lenses: trifocal versus extended range of vision. J Cataract Refract Surg. 2017;43(6):737-747.
6. Kohnen T, Herzog M, Hemkeppler E, et al. Visual performance of a quadrifocal (trifocal) intraocular lens following 12. Ruiz-Mesa R, Abengózar-Vela A, Ruiz-Santos M. A comparative study of visual outcomes between a new trifocal and an
removal of the crystalline lens. Am J Ophthalmol. 2017;184:52-62. extended depth of focus intraocular lens. Eur J Ophthalmol. 2018;28(2):182-187.
7. Kohnen T, Martinez AA. Multicenter visual outcomes evaluation of a novel trifocal presbyopia-correcting IOL. Presented 13. Böhm M, Hemkeppler E, Herzog M, et al. Comparison of a panfocal and trifocal diffractive intraocular lens after
at: ESCRS. Sept. 2018, Vienna, Austria. femtosecond laser-assisted lens surgery. J Cataract Refract Surg. 2018;44(12):1454-1462.
8. Scheepers M. Initial results of clinical visual outcomes of a trifocal IOL and an extended depth of focus (EDOF) IOL 14. Akman A, Asena L, Ozturk C, et al. Evaluation of quality of life after implantation of a new trifocal intraocular lens.
implantation following bilateral cataract surgery. Presented at: ASCRS. May 2019, San Diego, California. J Cataract Refract Surg. 2019;45(2):130–134.
9. Cochener B, Boutillier G, Lamard M, et al. A comparative evaluation of a new generation of diffractive trifocal and
ROSA BRAGA-MELE, MD, MED, FRCSC (MODERATOR) MARIUS SCHEEPERS, MD
n P rofessor of Ophthalmology, Faculty of Medicine, University of Toronto, Canada n C onsultant Ophthalmologist, Trail, British Columbia, Canada
n r bragamele@rogers.com n mascheepers@gmail.com
n F inancial disclosure: Consultant (Alcon, Zeiss); No financial interest in n F inancial disclosure: Consultant (Alcon)
any product
JERRY HU, MD
n T exas Eye and Laser Center, Fort Worth, Texas, USA
THOMAS KOHNEN, MD, PHD, FEBO
n j erryganghu@hotmail.com
n P rofessor and Chair, Department of Ophthalmology, Goethe University,
n F inancial disclosure: Consultant (Alcon, Allergan, Bausch & Lomb, Ivantis,
Frankfurt, Germany
n kohnen@em.uni-frankfurt.de Shire, Sun)
n F inancial disclosure: : Consultant and research (Abbott/J&J, Alcon/Novartis,
Avedro, Oculentis, Oculus, Presbia, Schwind, Zeiss); Consultant (Allergan, Bausch JEFF HORN, MD
n V ision For Life, Nashville, Tennessee, USA
& Lomb, Dompé, Geuder, Merck, Rayner, Santen, Staar, Thea, Tear Lab, Thieme,
n j dh@comcast.net
Ziemer); Research (Hoya)
n F inancial disclosure: Clinical Investigator (Alcon, Bausch + Lomb), Consultant
and speaker (Alcon)
Roundtable participants are paid Alcon consultants.
JANUARY 2020 | SUPPLEMENT TO CATARACT & REFRACTIVE SURGERY TODAY 7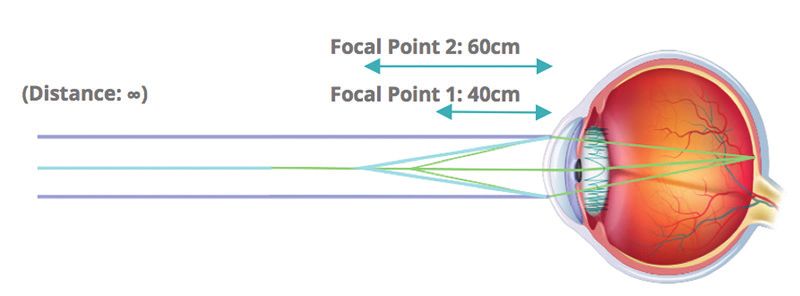
PanOptix
Trifocal IOL
AcrySof®IQ PanOptix®Family of Trifocal maintaining comparable distance visual acuity that the patient will request explant of the
IOLs with a reduced need for eyeglasses, compared multifocal IOL. A reduction in contrast sensitiv-
IMPORTANT PRODUCT INFORMATION to a monofocal IOL. In addition, the AcrySof®IQ ity as compared to a monofocal IOL may be ex-
PanOptix®Toric Trifocal IOL is indicated for the perienced by some patients and may be more
CAUTION: Federal (USA) law restricts this de-
reduction of residual refractive astigmatism. prevalent in low lighting conditions. Therefore,
vice to the sale by or on the order of a physician.
patients implanted with multifocal IOLs should
The AutoSert® IOL Injector Handpiece achieves WARNINGS/PRECAUTIONS: Careful preop-
exercise caution when driving at night or in
the functionality of injection of intraocular erative evaluation and sound clinical judgment
poor visibility conditions. Patients should be
lenses. The AutoSert® IOL Injector Handpiece should be used by the surgeon to decide the
advised that unexpected outcomes could lead
is indicated for use with the AcrySof® lenses risk/benefit ratio before implanting a lens in a
to continued spectacle dependence or the
SN6OWF, SN6AD1, SN6AT3 through SN6AT9, patient with any of the conditions described
need for secondary surgical intervention(e.g., in-
as well as approved AcrySof® lenses that are in the Directions for Use labeling. Physicians
traocular lens replacement or repositioning). As
specifically indicated for use with this inserter, should target emmetropia and ensure that
with other multifocal IOLs, patients may need
as indicated in the approved labeling of those IOL centration is achieved. For the AcrySof®IQ
glasses when reading small print or lookingat
lenses. PanOptix®Toric Trifocal IOL, the lens should not
small objects. Posterior capsule opacification
be implanted if the posterior capsule is rup-
INDICATIONS: The AcrySof®IQ (PCO) may significantly affect the vision of pa-
tured, if the zonules are damaged or if a primary
PanOptix®Trifocal IOLs include AcrySof®IQ tients with multifocal IOLs sooner in its progres-
posterior capsulotomy is planned. Rotation can
PanOptix®and AcrySof®IQ PanOptix®Toric and sion than patients with monofocal IOLs. Prior to
reduce astigmatic correction. If necessary, lens
are indicated for primary implantation in the surgery, physicians should provide prospective
repositioning should occur as early as possible
capsular bag in the posterior chamber of the patients with a copy of the Patient Information
prior to lens encapsulation. Some visual effects
eye for the visual correction of aphakia in adult Brochure, available from Alcon, informing them
may be expected due to the superposition of
patients, with less than 1 diopter of pre-existing of possible risks and benefits associated with
focused and unfocused multiple images. These
corneal astigmatism, in whom a cataractous the AcrySof®IQ PanOptix®Trifocal IOLs.
may include some perceptions of halos or star-
lens has been removed. The lens mitigates the bursts, as well as other visual symptoms. As with ATTENTION: Reference the Directions for Use
effects of presbyopia by providing improved other multifocal IOLs, there is a possibility that labeling for each IOL for a complete listing of
intermediate and near visual acuity, while visual symptoms may be significant enough indications, warnings and precautions.
© 2019 Alcon Inc. 10/19 US-ACP-1900067

You can also read

















































