Donor Specific Antibody (DSA) Monitoring - Early Detection. Optimal Outcomes.
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Donor Specific Antibody
(DSA) Monitoring
Early Detection. Optimal Outcomes.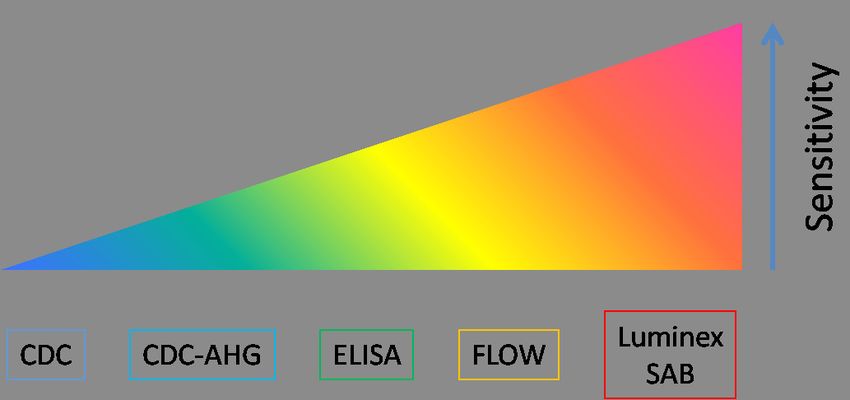
DSA Monitoring
The Role of anti-HLA Antibodies in Transplantation
There are over 100,000 solid organ transplants per- post-transplant development of clinically relevant anti-
formed annually worldwide, 29,000 of which are per- bodies directed against donor specific HLA class I and
formed in the United States.1 Despite significant im- class II mismatches has been a significant area of inter-
provements in post-transplant care, long term graft est within the transplant community. Whether detect-
function is less than optimal. In the United States, ed pre- or post-transplant, the presence of antibodies
adjusted 10 year allograft survival rates for deceased directed against antigens expressed on donor organs,
and living donor kidney transplants are only 40.8% and when not treated clinically, results in an immune attack
57.9%, respectively.2 Late stage graft failure, secondary on the transplanted organ, and increases risk of graft
to antibody mediated rejection (AMR) is a primary loss and/or rejection. DSA attacks the endothelium
cause of poor graft survival. of the allograft, resulting in subsequent AMR.4,5 The
progression of DSA development and the correspond-
Historically, anti-Human Leukocyte Antigen (HLA) ing clinical events compound to damage the allograft,
antibodies were defined as preformed circulating anti- resulting in chronic changes over time that ultimately
bodies present in the recipient’s immune system which compromise graft function and survival.
were the result of a sensitization event pre-transplant
(blood transfusion, previous transplant, or pregnancy).
In more recent years, the concept of monitoring for the
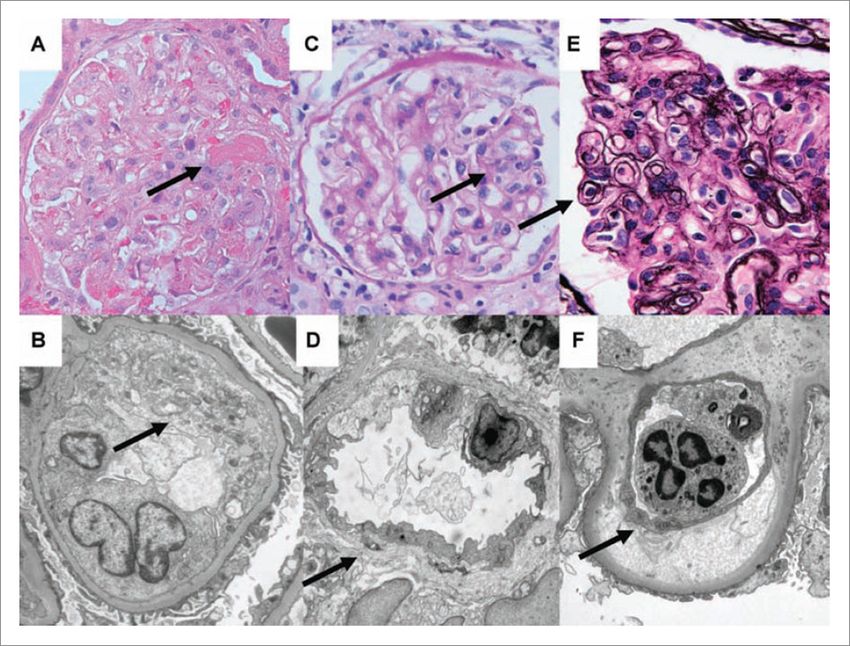
Spectrum of Antibody-Mediated Allograft Injury(Renal)6
(A, B) Acute antibody-mediated injury characterized by glomerular microthrombus, glomerular capillary endothelial cell activation
(arrows) (A: Hematoxylin/Eosin, 400×; B: EM, 7500×).
(C, D) Chronic active antibody-mediated rejection showing glomerular endothelial cell swelling and early peritubular capillary
basement membrane lamellation (arrows) (C: PAS, 400×; D: EM, 4200×).
(E, F) Chronic antibody-mediated rejection characterized by glomerular basement membrane duplication (arrows)
(E: Jones, 600×; F: EM, 7500×).
1Large cohort studies of over 5000 transplant recipients indicate that at any given time, approximately 25% of trans-
plant recipients have antibodie(s).1 Moreover, previous data in renal transplantation have shown that up to 96% of
rejected allografts develop some level of detectable DSA.
Percentage of Transplant Patients that Develop
Antibodies Post-transplant
100%
90%
Patients with HLA Antibody
80%
70%
60%
50%
40%
30%
20%
25%
10%
0%
By center
Results from the 15th International Workshop
While traditional markers can aid in diagnosing the One Lambda, Inc. offers highly sensitive and specific
clinical status of solid organ transplant recipients, they solid-phase assays allowing for the accurate identifica-
are generally non-specific and most often identifiable tion of DSA both pre- and post- transplant. This plat-
only after graft damage has occurred. There is strong form is currently being used as the standard-of-care
evidence that anti-HLA antibodies contribute to the diagnostic testing methodology in most transplant
development of chronic renal failure, the leading cause centers within the US.
of renal allograft failure.8 The early identification and
subsequent removal of clinically harmful DSA associ-
ated with AMR, both pre- and post-transplant, may
prevent allograft loss.8
2DSA Monitoring
The Spectrum of Antibody Mediated Rejection
Antibody mediated rejection can present as an early Chronic rejection is one of the leading causes of death-
acute process, often resulting from an anamnestic re- censored graft loss. Often described as a smoldering
sponse, or as a late and chronic process due to de novo process, repeat cycles of alloantibody-mediated injury
antibody production. In the acute phase, it is often pre- and repair result in distinct changes in the microvas-
formed antibodies that cause early rejection. De novo culature of the allograft. Patients with preformed DSA
DSA can also develop in the early post-transplant peri- and those who develop de novo DSA are at an increased
od, resulting in acute rejection. Patients with preformed risk of having chronic rejection.
DSA are at significantly greater risk of having an acute
AMR and have significantly lower graft survival.9
Sub-Clinical Antibody Mediated Rejection
DSA may also develop without an immediate impair- Microcirculation inflammation is more common in late
ment of graft function. This type of rejection, or sub- kidney biopsies after one year post-transplant, reflect-
clinical antibody mediated rejection (SAMR), has been ing the high frequency of de novo DSA. SAMR is also a
reported to have an impact on long-term graft dysfunc- frequent finding in patients with preformed DSA, some
tion and deterioration, instead of having an immediate of which the C4d stain is negative for SAMR. Typically,
impact. Loupy et al. demonstrated that the acute le- non-adherence to immunosuppressive therapy is asso-
sions were largely unabated, from 3 months to 3 years, ciated with the aforementioned pathological findings.10
whereas, the chronic lesions increased steadily and sig-
nificantly over a 3 year period.24
Evolution of acute (A) and chronic lesions (B) in DSA positive patients (group A) according to time of screening biopsy
(mean + SEM, data including nine additional screening biopsies performed at 3 years).
De Novo DSA in Post-Transplant Solid Organ
Transplant Recipients
The development of de novo donor-specific HLA an- • 62% of liver transplant patients19
tibodies (dnDSA) post-transplantation has been as- • 56% of lung transplant patients16
sociated with higher graft failure rates.10 The range of • 33% of heart transplant patients17
dnDSA is 24% to 62% with the highest presence in post • 27% of multivisceral transplant patients18
liver transplant recipients. • 24% of kidney-pancreas transplant patients24
3Proposed model for patients developing
de novo donor-specific antibodies as they
evolve from transplantation to graft fail-
ure. IFTA, interstitial fibrosis and tubular
atrophy; TG, transplant glomerulopathy.
Adapted from reference.20
DE NOVO RESPONSE IN CARDIAC ALLOGRAFTS21
• Development of de novo antibodies during the first year post-transplant has been shown to result in
15-year graft survival at 52%.
• Development after 1 year post-transplant results in worse outcomes, with 15 year graft survival at 40%.
• Strong association between Grade 3, worse ACR and subsequent development of de novo antibodies
after 1 year has been observed.
De Novo Antibody Production34
• De novo antibody production
may cause sub-clinical AMR
that is associated with long-
term graft dysfunction.
• Negative outcomes can take
several years to occur after
de novo antibody production.
Chronic rejection in patients (n=14) who did not have preformed HLA antibodies prior to transplantation (Ab-) and who were
examined for antibodies at 6-month intervals. All the patients developed antibodies (Ab+) (red bars). Antibodies persisted for a
period of 6 months to 8 years before the kidney was rejected.20
Several prospective and retrospective studies have As clinicians gain a more thorough understanding of
demonstrated that de novo DSA development in renal the role of post-transplant de novo DSA development, it
transplant patients, predominately directed at Class II has become clear that this phenomenon has been mis-
donor HLA mismatches, is associated with poor out- understood or underestimated in the past, likely due to
comes, and is often detectable well before graft failure.13 its delayed clinical manifestation post-transplant.14
4DSA Monitoring
DSA is Predictive of Lower Graft Survival
Over time, the risk of developing chronic rejection leading to AMR increases with the presence of anti-HLA-Class
II antibodies. Several studies have demonstrated that the presence of HLA antibodies predicts kidney graft loss.
Effect of DSA on Renal Allograft Survival
(A) The graft survival of patients with de novo donor- (B) The graft survival of pre-transplant human leukocyte
specific antibodies (dnDSA) versus those without. antigen (HLA) antibodies, post-transplant de novo HLA
antibodies, or no antibodies compared to patients with
dnDSA.
The Effect of Transplant Glomerulopathy (TG) on Renal Allograft Survival
Risk of developing TG according to anti-HLA-II levels. Graft Survival in patients: without TG (n=530), patients
The patients groups include: no anti-HLA-II antibodies in with C4d-negative TG (n=52), and patients with C4d
pre-transplant sera; anti-HLA-II antibodies and NV>2000 positive TG (n=16).
(n=40); NV 2001-10,000 (n=42); and NV>10,000 (n=39).
5DSA is Predictive of Lower Patient Survival
In addition to rejection and graft loss, a significant as- Survival Curve: Cardiac Transplantation
sociation between the presence of anti-HLA antibody 1.0
and patient survival has been demonstrated. A recent No DSA
study by Dunn et al. found that actuarial survival was
Probability of Patient
0.9 DSA
significantly decreased at 5-years post-transplant in
Survival
DSA positive patients compared to DSA negative pa- 0.8
tients (p=0.0006, HR = 10.0).3
0.7
Smith et al. observed that persistant, de novo DSA
was an independent predictor of poor patient survival 0.6
(p < 0.0001, HR = 4.763).17
0 5 10
Years since transplantation
Predicted survival curve for the time dependent variable de novo
DSA from fitted Cox model for patients producing DSA at the out-
set and patients with no detectable DSA at any time point follow-
ing cardiac transplantation.17
Liver Transplantation
Early AMR in liver transplants is often difficult to iden-
tify as an immunological event. This is due to the lack
of clear clinical, histological, and immunohistological
criteria for diagnosing AMR. Other factors that may
contribute to misdiagnosing AMR include the lack of
crossmatch results at the time of organ implant, posi-
tive crossmatch results at the time of transplant, and
the nonspecific clinical and pathological findings of
cholestasis that are similar to AMR. The recipients that
maintain a positive crossmatch after transplantation
are at high risk of AMR. Recent data suggest that the
diagnosis of AMR in liver transplant recipients may be
based on the presence of DSA in the recipient serum.14
O’Leary et al. demonstrated for the first time the asso-
ciation of DSA and chronic rejection after liver trans-
plantation. This group evaluated the total MFI, (Mean
Fluorescence Intensity, defined as the sum of distinct
DSA), and determined that preformed class I antibod-
Number of sustained DSAs after transplantation. In the D-AMR
ies were more detrimental to graft survival than class group, liver recipients maintained their positive flow cross-
II antibodies. The presence of de novo DSA within the matches. Crossmatches corresponded with the presence of DSAs
first year of liver transplants was more common in pa- during follow-up. Despite efforts to eliminate the antibodies,
only 1 or 2 DSAs were either eliminated or reduced significantly
tients that presented with a chronic rejection; 92% had in patients’ sera. In the ND-AMR group the conversion of the
detectable DSA before chronic-rejection-induced graft crossmatch coincided with the elimination of DSAs. Patient
failure occurred.19 ND-1 cleared 3 DSAs within the first 12 months. Her last DSA
(A-2 specificity) was still at the 3000 channel shift on single anti-
gen beads in month 12. It was no longer detectable in
6
month 24.14DSA Monitoring
DSA Is Associated With Bile Duct Injury in C4d+ Liver
Transplant Recipients15
In liver transplant patients, DSA is associated with negative outcomes, indicating that AMR may contribute to
interlobular bile duct injury and loss.
• 40% of patients had significant circulating DSA associated with diffuse portal C4d deposition.
• 70% of patients with ductopenia had DSA.
• 60% of ductopenia cases had DSA associated with diffuse portal C4d.
• 53.6% of ACR (acute cellular rejection) cases had evidence of concurrent humoral alloreactivity based on
detection of circulating DSA with diffuse portal C4d.
• DSA+/diffuse C4d+ patients had a significantly higher frequency of ACR (88% vs. 50%), p=0.02.
• DSA+/diffuse C4d+ patients had a significantly higher frequency of steroid resistant rejection
(41% vs. 19%), p=0.03.
Pancreas Transplantation
Pancreas
Recent studies in pancreas allograft recipients suggest Cantarovich et al. reported that long-term pancreas
that the development of post-transplant DSA is sig- graft survival is inferior to survival of other solid organ
nificantly associated with worse outcomes, including transplants because the diagnosis of pancreas graft re-
increased incidence of rejection and decreased graft jection is biologically and clinically complex. However,
survival. identifying markers such as post-transplant DSA may
be utilized as an independent risk factor for
graft survival.25 7Islet Cell and Multi-Visceral Transplantation
Current data in pancreas and islet cell transplantation The role of DSA monitoring in pancreas, multi-visceral
suggest that the presence of pre-transplant DSA is as- and small bowel transplants is a valuable diagnostic
sociated with poor outcomes after transplant. Multi- tool in early diagnosis and treatment of acute rejection.
visceral transplantation (MVT) is the concurrent trans-
plantation of the small bowel and liver with 1 or more
of the following organs: stomach, pancreaticoduodenal
complex, jejunum, ileum and/or colon. Rejection after
small bowel and MVT transplant is a serious compli-
cation affecting both patient and graft survival. The
presence of DSA indicates that the patient is at a higher
risk of rejection.17 Early diagnosis of acute rejection in
small bowel transplant is essential to control the rejec-
tion process.
Distribution of acute rejection:
small bowel allograft biopsies
Distribution of rejection severity
(A) Distribution of acute rejection (AR) in
small bowel allograft biopsies. In this study,
total 291 biopsy samples were obtained
and the distribution was: 80 no rejection
(27.79%), 148 grade indeterminate (50.86%),
44 mild grade (15.12%), 2 moderate grade
(0.69%), and 17 severe grade (5.84%). (B)
Distribution of rejection severity in biopsy
samples showing AR with and without
donor-specific antibody (DSA). In presence
of DSA, percentage of severe rejection is sig-
nificantly higher (43.33 vs. 12.12%, P=0.009)
8DSA Monitoring
Lung Transplantation
Patient Survival in Lung Transplant BOS-Free Cumulative Survival and
Antibody Presence in Lung Transplantation26
Bronchiolitis Obliterans Syndrome (BOS)
is a complication in lung transplantation.
Due to the high prevalence of BOS and the
poor prognosis and shorter graft survivals in
patients with BOS, it is imperative to detect
DSA sooner.
Anti-HLA antibodies are associated with a
higher prevalence of BOS than absence of
anti-HLA antibodies – 71% vs. 24%.
In one study, the detection of anti-HLA an-
tibodies preceded diagnosis of BOS by ap-
proximately 1.1 years. 26
BOS-free cumulative survival was significantly lower in patients with
HLA-specific antibodies (Ab) versus no HLA-specific antibodies (No Ab).
Cardiac Transplantation Freedom from CAV: Patients +/- DSA
Cardiac allograft vasculopathy (CAV) is the
primary cause of death and re-transplant in
long-term heart transplant survivors.
Circulating antibody can result in comple-
ment activation and fixation on the graft en-
dothelium, thereby predisposing the patient
to graft loss, accelerated CAV, and death.
In a study reported by Kazmerek et al., free-
dom from CAV in DSA(+) patients was
94.4%, 81.0%, 41.2% and 10.3% at 1, 5, 10
and 15 years post-transplant compared with
96.2%, 83.4%, 67.3% and 34.7% in DSA(-)
patients.5
9The Future of DSA Monitoring: Effect of C1q DSA
on Allograft Survival
The detection of anti-HLA antibody in transplant re-
cipients allows the clinician to better predict AMR in
the post- transplant patient. Since not all DSAs are
complement fixing, and may not be clinically relevant
to organ rejection, it is imperative to identify those that
are complement fixing in order to treat transplant pa-
tients properly. A novel C1q assay designed to detect
immunoglobulin G (IgG) antibodies capable of fixing
complement has been studied in the post-transplant
setting in combination with existing methodologies
utilized to define a patient’s immunologic profile. In a
recent study of pediatric heart transplant recipients, all
patients with C1q (+) DSA after transplant had AMR at
the next biopsy, suggesting DSA monitoring is effective
in predicting AMR.27
Kaplan-Meier death-censored graft survival based on presence or
absence of donor-specific antibodies as detected by C1q.
The role of complement fixation, as detected by C4d
staining, in predicting AMR is not as widely accepted
now as it had been in the past for the post-transplant
monitoring of solid organ transplant recipients. Addi-
tionally, the proper identification of recipient HLA an-
tibody specificity is critical in the assessment of those
antibodies that can activate the classical complement
pathway. Research has suggested that the evaluation of
the C1q assay provides a further layer of immunologic
antibody information that may prove to be an adjunct
in optimizing post-transplant care.
In a study reported by Yabu et al., kidney transplant
recipients with C1q (+) DSA were nearly 6 times more
likely to lose their grafts than those with C1q (-) DSA.10
Chin et al. found that heart transplant patients with
C1q (+) DSA after transplant had AMR at the next bi- The presence of C1q (+) DSA was associated with a sig-
opsy, demonstrating that complement binding DSA is nificantly greater incidence of acute allograft rejection,
predictive of AMR. 27 and patients with C1q (+) DSA were significantly more
likely to have C4d deposition found on biopsy. The C1q
assay preferentially detects antibodies that have the ca-
pacity to fix and activate complement.28
10DSA Monitoring
Post-transplantation Monitoring
Many transplant recipients are DSA (-) pre-transplant Studies have shown that when DSA is identified early
and develop DSA post-transplant, typically within the through routine monitoring, the initiation of anti-hu-
first 2 years of the transplant.28 moral therapy may begin sooner, allowing for DSA to
clear and improving overall survival rates.
Fifty percent of AMR is currently overlooked, with
biopsy findings and clinical phenotypes attributed
Antibody-Directed Therapy After
to chronic allograft nephropathy.29 It may take many
Lung Transplantation
months or even years for the antibodies to produce the
chronic vascular changes that ultimately result in graft
failure. Serial monitoring of the alloantibodies follow-
ing transplantation may facilitate early diagnosis of
chronic rejection.40
The routine monitoring of DSA may provide early
identification of those patients at risk for rejection due
to insufficient immunosuppression as a result of poor
compliance with immunosuppressive therapy.
DSA monitoring may be useful in the adjustment of
immunosuppressive therapy post-transplant. The close
surveillance of humoral immunity is mandatory for
the precise adjustment of anti-humoral therapy and
optimal outcomes.18
Survival was significantly worse in recipients who
had persistent DSA than in those who had cleared the
DSA.16
Reduction of Donor Specific Antibody Levels in AMR Prevents Renal Allograft Loss 31, 32
Death-censored allograft survival stratified by percent reduction Renal allograft survival stratified on ability to yield antibody
in immunodominant DSA at 14 days post-biopsy reduction
11Why Monitor DSA Post-Transplant?
• Ten-year renal allograft survival in early antibody developers (DSA Monitoring
Optimizing DSA Monitoring Strategies
While implementation of routine post-transplant mon- Kimball et al. performed quarterly monitoring of pa-
itoring becomes increasingly recognized as a standard- tients for 3 years post-transplant and reported that 65%
of-care practice, the frequency of testing is highly vari- of patients eliminated antibody within the first year of
able. The frequency of post-transplant monitoring will transplant due to early detection and subsequent treat-
be patient-specific. Choosing a monitoring frequency ment. In those patients that exhibited pre-transplant
based on a patient’s individual risk of developing AMR DSA against Class I and II HLA, antibody levels de-
post-transplant will be the most efficient and clinically clined by 90% at 6 months and were undetectable at 1
relevant strategy. year with effective treatment.7
Serial monitoring of DSA is more valuable than single-
point testing, particularly in the post-transplant set-
ting, and is crucial in optimizing patient outcomes.9
Conclusion
Since the first solid organ transplant in 1954, the field Historically, the immunologic profile obtained from
of transplantation has witnessed several milestones that the assays conducted in the histocompatibility labora-
have significantly modified the solid organ transplant tory was utilized strictly in the pre-transplant setting,
recipient treatment paradigm and positively impacted as a means to minimize or avoid post-transplant rejec-
both graft and patient survival. Surgical innovation tion. More recently, data has been reported, indicat-
and advancement has been complemented by the in- ing that the identification and subsequent treatment of
troduction and optimization of novel immunosuppres- DSA in the post-transplant setting, for all solid organ
sive and infectious disease regimens. For immunologic types, may be an important consideration in the long-
monitoring, cytotoxic assays have given way to solid- term treatment of the transplant patient. Reported data
phase methodologies with higher levels of sensitivity demonstrate the potential benefit of routine DSA mon-
and specificity. Having evolved over time, emerging itoring in post-transplant patient outcomes. The rou-
technologies are now available for the detection of the tine monitoring of DSA in the post-transplant setting
presence of anti-HLA antibodies, and more important- offers promise in long term graft and patient survival.
ly, the identification of specific anti-HLA DSA.
13For additional information on DSA monitoring
please visit www.onelamba.com
14DSA Monitoring
References
1. OPTN & SRTR 2010 Annual Data Report. www.srtr-org/annual_reports/2010 Accessed 20 May 2012.
2. Sutherland SM et al. Complement-fixing donor-specific antibodies identified by a novel C1q assay are
associ ated with allograft loss. Pediatric Transplantation 2011.
3. Dunn TB, et al. Revisiting traditional risk factors of rejection and graft loss after kidney transplantation.
American Journal of Transplantation 2011.
4. Colvin RB, et al. Antibody-mediated organ allograft rejection. National Review of Immunology 2003;
5(10): 807-817.
5. Kaczmarek I, et al. Donor-specific HLA alloantibodies: long-term impact on cardiac allograft vasculopathy
and mortality after heart transplant. Experimental and Clinical Transplantation 2008; 6: 229-235.
6. Issa N, et al. Transp ation 2008: 86(5): 681-685.
7. Terasaki, et al. Humoral theory of transplantation. American Journal of Transplantation 2003; 3: 665-673.
8. Kimball PM, et al Surveillance of alloantibodies after transplantation identifies the risk of chronic
rejection. Internal Society of Nephrology 2011 ; 79: 1131-1137.
9. Lefaucheur, et al. Clinical relevance of preformed HLA donor-specific antibodies in kidney
transplantation. American journal of transplantation : official journal of the American Society of
Transplantation and the American Society of Transplant Surgeons 2008; 8(2): 324-331.
10. Wiebe C, et al Evolution and clinical pathologic correlations of de novo donor-specific HLA antibody post
kidney transplant. American Journal of Transplantation 2012; 12: 1157-1167.
11. Yabu JM, et al. C1q-fixing human leukocyte antigen antibodies are specific for predicting transplant
glomerulopathy and late graft failure after kidney transplantation. Clinical and Translational Research
2011; 91 (3):342-347.
12. Lachmann N, et al. Anti-human leukocyte antigen and donor-specific antibodies detected by Luminex®
post-transplant serve as biomarkers for chronic rejection of renal allografts. Transplantation 2009;
87(10):1505-1513.
13. Fotheringham J, et al Natural history of protienuria in renal transplant recipients developing de novo
human leukocyte antigen antibodies. Clinical and Translational Research 2011; 91 (9): 991-996.
14. Kozlowksi T, et al Liver allograft antibody-mediated rejection with demonstration of sinusoidal C4d
staining and circulating donor-specific antibodies. Liver Transplantation 2011; 17: 357-368.
15. Musat AI, et al. The significance of donor-specific HLA antibodies in rejection and ductopenia
development in ABO compatible liver transplantation. American Journal of Transplantation 2011;
11(3):500-510.
16. Hachem RR, et al. Anti-human leukocyte antigen antibodies and preemptive antibody-directed therapy
after lung transplantation. Journal of Heart and Lung Transplantation 2010; 29:973-980.
17. Smith JD, et al. De novo donor HLA-specific antibodies after heart transplantation are an independent
predictor of poor patient survival. American Journal of Transplantation 2011; 11:312–319.
18. Tsai HL, et al. Association between donor-specific antibodies and acute rejection and resolution in small
bowel and multivisceral transplantation. Clinical and Translational Research 2011; 92 (6): 709-715.
19. O’Leary, et al. High mean fluorescence intensity donor-specific anti-HLA antibodies associated with
chronic rejection post liver transplant. American Journal of Transplantation 2011; 11: 1868-1876.
20. Smith, et al. Four stages and lack of stable accommodation in chronic alloantibody-mediated renal allograft
rejection in cynomolgus monkeys. American Journal of Transplant 2008; 8: 1662-1672.
15References
21. Ho EK, et al. Pre- and post-transplantation all sensitization in heart allograft recipients: major impact of
de novo alloantibody production on allograft survival. Human Immunology 2011; 72(1):5-10.
22. Lee PC, et al. All chronic rejection failures of kidney transplants were preceded by the development of HLA
antibodies. Transplantation 2002; 74(8):1192-1194.
23. Sis B, et al. A new diagnostic algorithm for antibody –mediated microcirculation inflammation in kidney
transplants. American Journal of Transplantation 2012.
24. Loupy A, et al. Outcome of subclinical antibody-mediated rejection in kidney transplant recipients with
preformed donor-specific antibodies. American Journal of Transplantation 2009; 9: 2561-2570.
25. Cantarovich D, et al. Post-transplant donor-specific Anti-HLA antibodies negatively impact pancreas
transplantation outcome. American Journal of Transplantation 2011; 11: 2737-2746.
26. Girnita AL, et al. HLA-specific antibodies are risk factors for lymphocytic bronchiolitis and chronic lung
allograft dysfunction. American Journal of Transplantation 2005; 5(1):131-138.
27. Chin C, et al. Clinical usefulness of a novel C1q assay to detect immunoglobulin G antibodies capable of
fixing complement in sensitized pediatric heart transplant patients. The Journal of Heart and Lung
Transplantation 2011; 30 (2): 158-163.
28. Sutherland SM, et al. Complement-fixing donor-specific antibodies identified by a novel C1q assay are
associated with allograft loss. Pediatric Transplantation 2011.
29. Sellares J, et al Understanding the causes of kidney transplant failure: the dominant role of antibody-
mediated rejection and nonadherence. American Journal of Transplantation 2011.
30. Kimball PM, et al Surveillance of alloantibodies after transplantation identifies the risk of chronic rejection.
Internal Society of Nephrology 2011; 79: 1131-1137.
31. Everly, et al. Reducing de novo donor-specific antibody levels during acute rejection diminishes renal
allograft loss. American Journal of Transplantation 2009; 9(5):1063-1071.
32. Everly MJ, et al. Beyond histology: lowering human leukocyte antigen antibody to improve renal allograft
survival in acute rejection. Transplantation 2010; 89(8):962-967.
33. Lee PC, et al. HLA-specific antibodies developed in the first year post-transplant are predictive of chronic
rejection and renal graft loss. Transplantation 2009; 88(4):568-574.
34. Gloor JM, et al. Histologic findings one year after positive cross match or ABO blood group incompatible
living donor kidney transplantation. American Journal of Transplantation 2006; 6(8): 1841-7.
35. Stegall MD, et al. Deciphering antibody-mediated rejection: new insights into mechanisms and treatment.
Current Opinion in Organ Transplantation 2010; 15(1):8-10.
36. Terasaki P, et al. Predicting kidney graft failure by HLA antibodies: A prospective trial. American Journal of
Transplantation 2004; (4): 438-443.
37. Belperio JA, et al. Chronic lung allograft rejection: mechanisms and therapy. Proceedings of the American
Thoracic Society 2009; 6(1): 108-121.
38. Terasaki P et al. Predicting kidney graft failure by HLA antibodies: a prospective trial. American Journal of
Transplantation 2004; (4): 438-443.
16You can also read

















































