Quadri Clinici di Celiachia nell'Adulto - Umberto Volta - Convegno Nazionale AIC
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Programma di attività scientifiche per il
quarantennale della nascita dell’Associazione
Italiana Celiachia (AIC)
(1979 – 2019)
Quadri Clinici di
Celiachia nell’Adulto
Umberto Volta
Dip. Scienze Mediche e Chirurgiche
Università di Bologna
già Responsabile SSO Malattia Celiaca
Policlinico S.Orsola-Malpighi - Bologna
Board Società Europea per lo studio della
Celiachia (ESsCD)
Board Associazione Italiana Celiachia (AIC)
Consulente Scientitifico AIC Emilia Romagna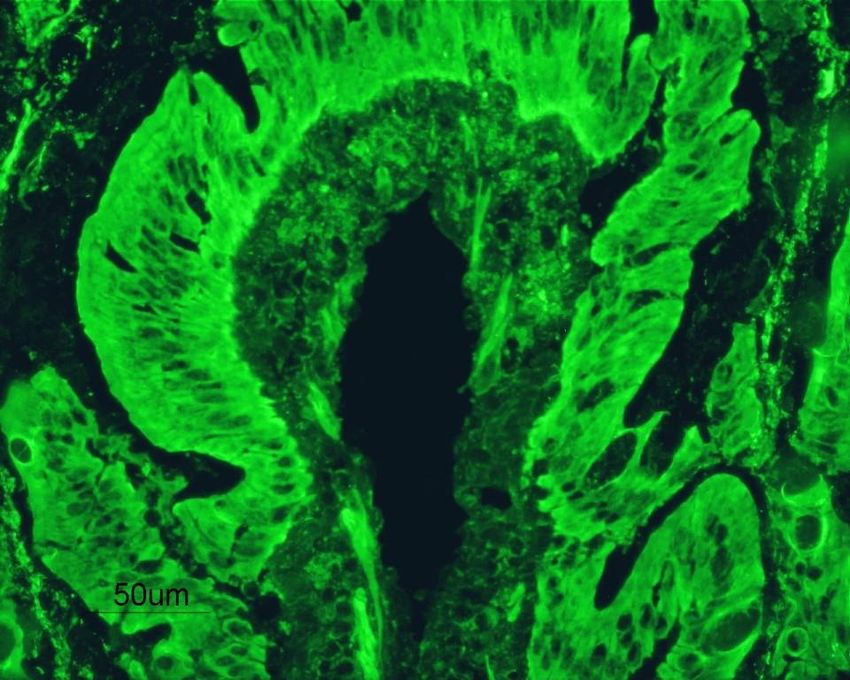
Coeliac disease (CD) in the second millenium • Until a few decades ago CD was still regarded as a rare food intolerance confined to childhood and to female gender • CD was thought to be always characterised by a severe malabsorption and flat mucosa. • The gold standard for CD diagnosis still remained intestinal biopsy, reinforcing the irreplaceable role of histology in CD diagnosis.
COELIAC DISEASE TODAY
autoimmune disorder
very frequent in the general population (≥ 1%)
onset at any age (even in the elderly)
a slight prevalence in the female gender (F/M 2:1)
polymorphic clinical presentation with intestinal and extraintestinal symptoms
diagnostic gold standard: both serology and histology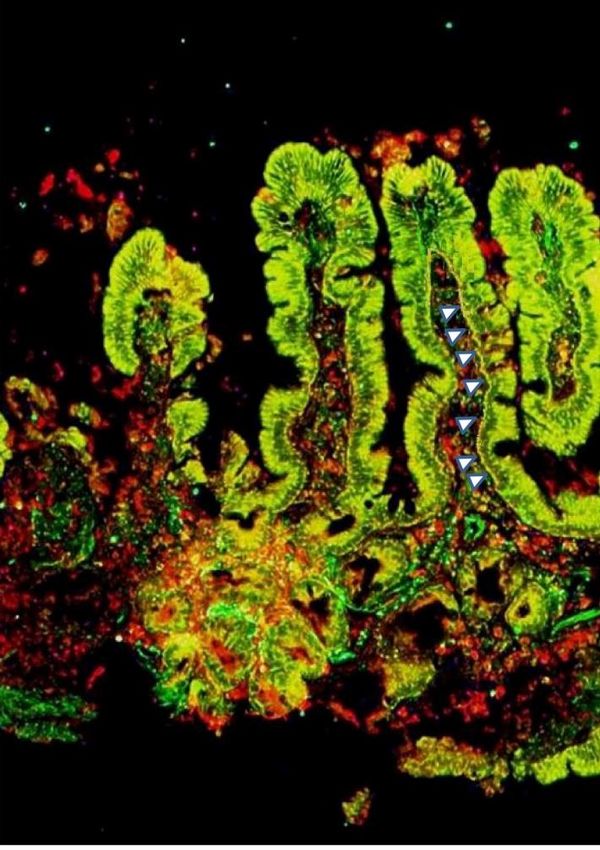
Changing pattern of presentation in adults
Diarrhea onset Different modes of presentation
as a percentage of the total pts
Delay in CD diagnosis
Clinical Significance
Fewer pts with CD present with diarrhea
More pts are detected by screening
Delay in diagnosis is markedly reduced
Fewer pts develop malignancies
Rampertab SD, AJM 2006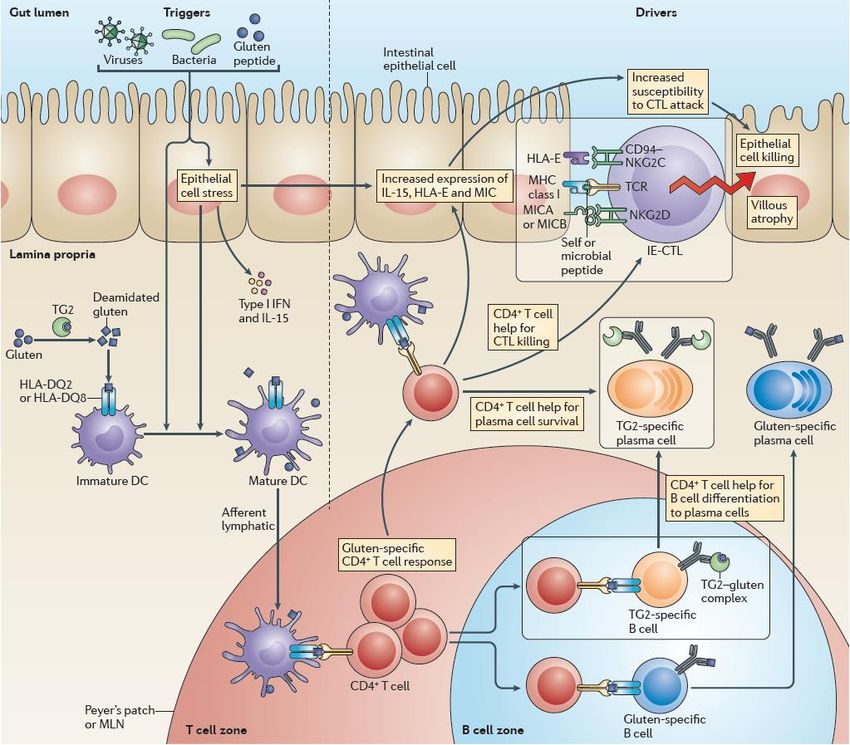
Has the clinical presentation really changed or rather has the
knowledge of celiac disease improved ?
Severe
• In the past only the tip of the celiac malabsorption
iceberg, represented by patients with
severe diarrhea, was identified and a extraintestinal manifestations
plenty of diagnoses were missed
• The discovery of serological biomarkers
(EmA and anti-tTG) has been the
turning point allowing to identfy at-risk
groups for CD missed in the past The New England Journal of Medicine
EDITORIALS
• Nowadays, CD is regarded as a clinical EmA At-risk
Anti-tTG groups
chameleon for the plenty of symptoms
underlying this disorders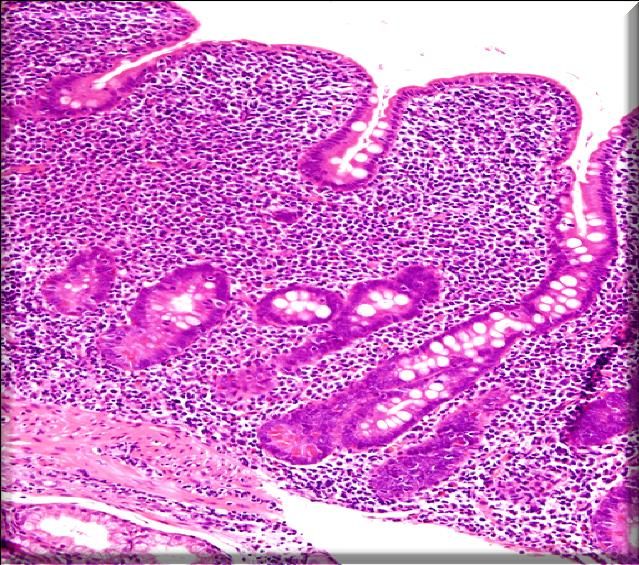
Clinical Features of Celiac Disease
Gastrointestinal symptoms Extra-intestinal manifestations
diarrhoea, abdominal pain, anaemia (iron, folate, vit. B12
bloating, dyspepsia, deficiency), short stature,
constipation, intestinal aphthous stomatitis, cryptogenic
subocclusion, irritable bowel hypertransaminasaemia,
syndrome, vomiting unexplained osteoporosis, dental
enamel defects, hemorragyc
syndrome due to vit. K
malabsorption, reproductive
Female/Male ratio 2:1 or 3:1 abnormalities in females (late
Onset age: at any age (more menarche, early menopause,
frequent in infancy and between recurrent miscarriages, premature
the age of twenties and thirties ) birth) and males (azoospermia,
High prevalence in 1st degree CD oligoospermia), arthromyalgia
relatives (up to 17%) (fibromyalgia)
Fasano A Catassi C, New Eng J Med 2012:367:2419-26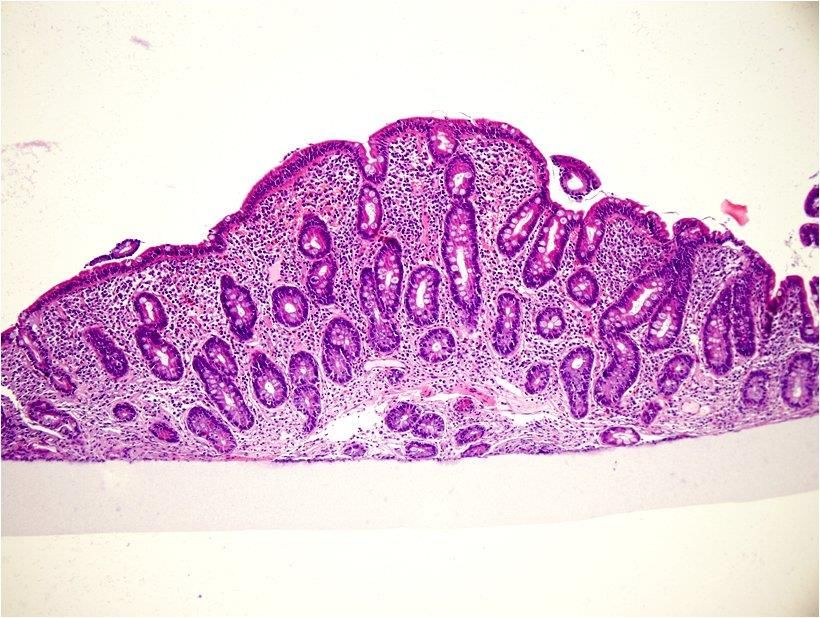
Coeliac disease: a systemic disorder
in and outside the gut
Pandora’s Box
Absent or mild
Potential Coeliac
Disease
Modified from Maki M,
Nat Rev Gastroenterol Hepatol 2012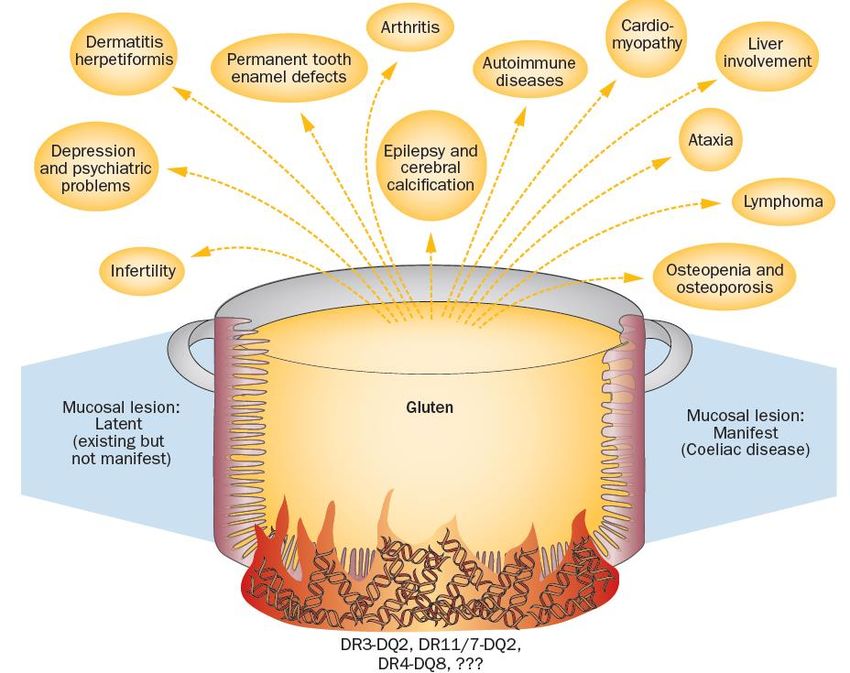
Prevalence of autoimmune disorders in celiac disease
according to the age of celiac disease diagnosis
Associated autoimmune diseases
• Hashimoto thyroiditis
• Grave’s disease
• Type 1 diabetes mellitus
• Dermatitis herpetiformis
• Selective IgA deficiency
• Sjogren ‘s syndrome
• Primary biliary cholangitis
• Autoimmune hepatitis
• Neurological disorders
• Alopecia areata
• Psoriasis
• Autoimmune atrophic gastritis
Ventura A et al, Gastroenterology 1999, 117:297-303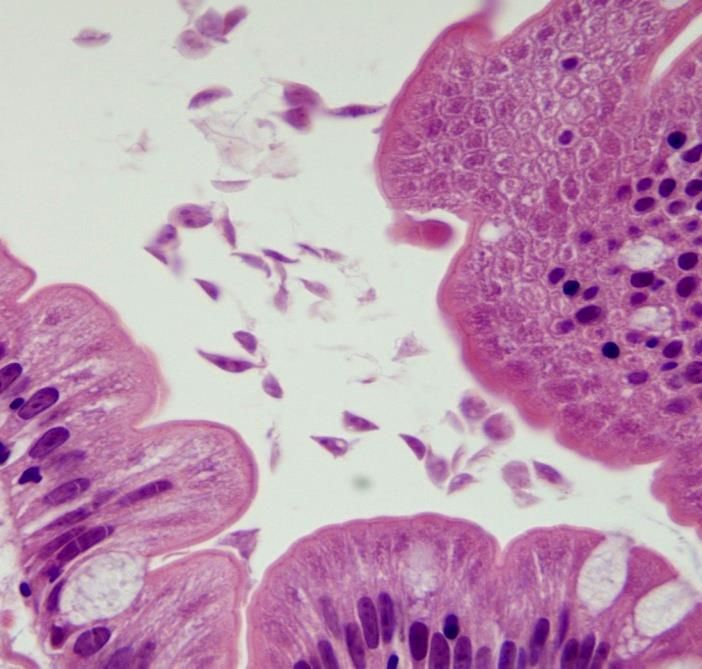
I numeri della Celiachia in Italia oggi
Trend diagnostico in aumento
198.427 diagnosi
Ma ancora l’iceberg delle diagnosi è ↑10%
sommerso perché si pensa poco a questa anno
patologia
su oltre 600.000 attese
40
35
Scarsa conoscenza di una 30 > 20% dopo i 50 anni
25
patologia che può insorgere 20
M+F
F
ad ogni età 15 M F/M 1.5-2
10
5
0
1-14aa 15-40aa 41-50aa 51-60aa 61-70aa >70aa
I numeri della Celiachia in Emilia-Romagna
Casi attesi Casi Casi Casi
diagnosticati diagnosticati diagnosticati
Marcato incremento
(tutte ledelle
età)diagnosi
14 anni
nell’ultimo decennio:
40000 4410 1390 2979
1:100 16.0201:906 1:356
celiaci diagnosticati su una 1:1157
popolazione di 4.448.146 abitanti
Range regionale
(0.33%, Range regionale
media nazionale 0.30%) Range regionale
1:580-1:1630
Relazione al Parlamento 1:290-1:514 1:634-1:2179
sulla Celiachia 2018
Indagine AIC Emilia-Romagna, coordinata da Brusa S., 2006Up-date on clinical forms of adult coeliac disease (CD)
Caio G, Giancola F, De Giorgio R, Volta U. It J Med 2017; 5:98-114
Oslo Classification
Ludvigsson J et al. Gut 2013, 62:43-52
NON-RESPONSIVE
(poor compliance
or associated GI
disorders)
CLASSICAL
NON -
CLASSICAL
SERONEGATIVE*
(DQ2/DQ8 flat
mucosa with clinical
and histological
response to GFD) CD
*Differential diagnosis with:
• Autoimmune enteropathy
SUBCLINICAL
• Giardiasis
• CVID REFRACTORY
• Olmesartan enteropathy POTENTIAL
• SIBO
• Tropical sprue
• Whipple disease
• HIV enteropathyThe experience of the Celiac Disease Center
of Bologna University in the period 1998-2012
318 diagnoses
(41.2%) in the first
10 years, 452
diagnose (58.8%) in
the last 5 years
Volta U et al, BMC Gastroenterol 2014; 14:194Clinical onset of Celiac Disease in the Celiac
Disease Center of St.Orsola-Malpighi Hospital
(1998-2012)
Classical Non Classical
evident malabsorption lack of malabsorption
diarrhea constipation
weight loss extraintestinal
failure to thrive manifestations
Subclinical
not detectable
symptoms
Volta U et al, BMC Gastroenterol 2014; 14:194Presentazione clinica della celiachia nei 770 celiaci
diagnosticati presso il Centro Celiachia di Bologna
(1998-2012)
52%
Stipsi
Anemia
Osteoporosi precoce 1998-2007
Alterazioni epatiche Classica Non classica Subclinica
47% 43% 10%
Aborti ricorrenti
2008-2012
Classica Non classica Subclinica
Volta U et al, BMC Gastroenterol 2014, 14:194 14% 58% 28%Clinical onset of symptomatic adult coeliac disease
Volta U et al, BMC Gastroenterol 2014; 14:194Prevalence of IgA tTGA and EmA
at celiac disease onset
Of the 26 pts (3.4%) without tTGA and EmA of IgA class, 12 (1.6%) had IgA
deficiency and were all positive for tTGA or deamidated gliadin antibodies
(DGP) of IgG Class. The remaining 14 seronegative cases were classified as
celiacs on the basis of villous atrophy responding to GFD and were all HLA-
DQ2 and/or –DQ8 positive.
Volta U et al, BMC Gastroenterol 2014; 14:194Histological findings* at celiac disease (CD) onset
-2
-2
*according to Marsh-Oberhüber classification Volta U et al, BMC Gastroenterol 2014; 14:194Prevalence of coeliac disease-associated disorders
Autoimmune thyroiditis
Dermatitis herpetiformis
Diabetes mellitus type 1
Neurological disorder
IgA deficiency
Autoimmune liver disease
Connective tissue disease
Chromosomal disorders
0 5 10 15 20 25 30
Volta U et al, BMC Gastroenterol 2014; 14:194Diagnosis of coeliac disease
in the elderly
770 CD patients
10%
>65 years
(70.1±4.3)
90.0%Frequency of presenting symptoms and signs in elderly and adult untreated coeliac patients Symptoms and signs Elderly (70 cases), % Adult (700 cases), % Diarrhoea 76.6** 30.9 Weight loss 60.0** 30.9 Anaemia 58.3** 34.0 Weakness 50.0* 32.3 Abdominal pain 45.0* 22.1 Muscle/cramp tetany 28.3** 8.8 Nausea/vomiting 25.0* 7.9 Osteopenia/Osteoporosis 60.0^ 48.9 Oedema 23.3* 11.9 Constipation 1.6 ^ 5.3 Aphthous stomatitis 12.5^ 13.3 *p
Laboratory parameters in elderly and
adult untreated coeliac patients
Elderly (70 cases), % Adult (700 cases), %
Hemoglobin, g/dL 11.0 1.8° 12.5 1.9
Albumin, g/dL 3.5 2.5° 4.5 1.8
Calcium, mg/dL 8.7 1.3* 9.1 0.8
Vitamin D, ng/mL 15.5 11.7° 20.9 122
Imunoglobulin A, mg/dL 334.1 221.3° 236.0 138.7
PTH, pg/mL# 80.5 96.1* 67.2 67.9
Alkaline Phosphatase, U/L 89.2 68.8* 65.7 40.8
° pThe experience of Bologna Coeliac Disease Center in potential celiac disease
77 cases (10.5%) over 735 celiac disease diagnoses (2004-2013)
IgA Endomysial Abs (EmA) HLA-DQ2 / -DQ8
Marsh 0 Marsh 1 DQ2
a5
DQA1*05
IgA tTGA antibodies DQB1*02
b2
DQ8
a3 DQA1*03
DQB1*0302
DGP antibodies b302
Diagnostic criteria for PCD
1) Positivity of CD-related antibodies (EmA pos. mandatory!)
2) Absent or minimal changes in intestinal mucosa(Marsh 0-1)
3) HLA-DQ2+ and/or DQ8+
Volta U et al. Clinical Gastroenterology and Hepatology 2016;14:686–693Increased trend of potential coeliac disease over the years
735 consecutive CD
patients
10.5%
PCD
77 PCD vs 658 ACD 18
6 18
F/M = 3.2:1 vs 3.5:1 14
Mean age: 25 vs 36 5 6 7
years
ACD: Active Coeliac Disease; PCD: Potential Coeliac Disease
Volta U, Caio G , De Giorgio R. CGH 2016Prevalence of symptoms in adult PCD
%
100
11 17
90 25 21 24
80
70
60
50
89 83 Asymptomatic
40 75 79 76
30
20 Symptomatic
10
0
Kurppa Biagi Zanini Volta Imperatore
Gastro Scand J CGH CGH DLD
2009 Gastroent 2013 2016 2017
2013How to manage potential coeliac disease
Volta U et al. Clinical Gastroenterology and Hepatology 2016;14:686–693Evidence of response to GFD in the 61
symptomatic PCD patients
25 pts with low lev- 8 pts referred
els of ferritin/folic disappearance
acid improved Hb 7 pts with hyper- of aphthae
levels within 6 transaminasemia
months of GFD normalized the
enzyme levels
after 3-6 months Only 8 pts with GERD
of GFD and IBS had a partial
improvement of
symptoms with their
recurrence
3 women with 10 pts did not
recurrent mis- experience
carriages carried more diarrhea
pregnancy to term after GFD wìth A total recovery was
after 1-2 years of weight gain observed in 87% of
GFD symptomatic PCD
pts after GFD
Volta U et al, Clin Gastroenterol Hepatol 2016; 14:686-93Suggested follow-up for asymptomatic
potential coeliac disease (PCD)
Asymptomatic PCD
Gluten containing diet
Re-biopsy every 2
Clinical/serological
years to assess the
follow-up every 6
progression to overt
months
coeliac disease*
*the biopsy must be anticipated in the event of
Volta U et al, Clin Gastroenterol Hepatol 2016; 14:686-93 symptom appearance and/or raising antibody titersIgA-TG2 deposits in potential coeliac disease A B C IgA deposits to TG2 (A), indicated by white arrows, were positive in 12 (60%) out of 20 PCD patients tested for these immune markers Their increase in intensity can predict the evolution towards active coeluac disease in the follow-up Volta U et al, Clin Gastroenterol Hepatol 2016
Evolution to active CD (villous atrophy)
in asymptomatic PCD patients left on GCD
%
50
46
45 39/253 pts
40 15%
(range 6-46)
35
mean follow-up
30 3 years
25
21
20
15
15
10 7
6
5
0
Biagi Auricchio Volta Kondala Imperatore
Scand J Gastr 2013 AJG 2014 CGH 2016 UEG 2016 DLD 2017
5/14 pts 23/153 pts 1/16 pts 4/57 pts 6/13 pts
F-up 2-yrs F-up 3-yrs F-up 3-yrs F-up 1-yr F-up 6yrsCeliachia sieronegativa
Celiachia senza anticorpi
Atrofia dei villi 2%
La maggioranza dei celiaci è positivo per: Una minoranza dei celiaci non ha anticorpi
Diagnosi differenziale con
EmA • Enteropatia autoimmune
• Giardiasi
• Immunodeficienza comune variabile
• Enteropatia da Olmesartan
tTGA • SIBO
98% • Enterite eosinofila
• Sprue tropicale
Gliadin • Morbo di Whipple
DGP-AGA • Morbo di Crohn
TG2 • Enteropatia da HIVCasi di atrofia sieronegativa della mucosa intestinale
identificati presso il CDC dell’Università di Bologna
nel periodo 1998-2014
50% n=14
40% 45 Nr°= 31 casi
Affected patients
30%
n=6
20% n=5 20
16 n=3
10%
n=1 n=1 10 n=1
0% 3 3 3
y
ID
lic sis
en IBO
y
D
is
th
th
C
rit
V
ia
pa
pa
te
C
S
e
op rd
iv
en
ro
ro
ia
at
te
te
G
eg
en
hi
on
n
e
er
ta
un
in
ar
S
m
os
es
m
E
lm
oi
ut
O
A
Volta U et al., DLD 2016;48:1018-1022Essential requirements for confirming
the diagnosis of seronegative CD
• Positivity for HLA-DQ2 and/or -DQ8
• Clinical improvement after gluten-free diet (GFD)
• Regrowth of intestinal villi after 1-year-GFDCome diagnosticare la celiachia sieronegativa
Atrofia dei villi senza anticorpi
HLA
HLA-DQ2/DQ8 - HLA-DQ2/DQ8+
Esclusa celiachia (CD ) Possibile CD
GFD trial
Ricerca di altre cause:
• Anti-enterociti (Enterop. autoimmune)
• Dosagggio immunoglobuline (CVID)
• Farmaci (e.g. olmesartan, FANS) Nessun risultato Miglioramento clinico
• Breath test (SIBO) ed istologico
• Giardia lamblia
• HIV
• Morbo di Whipple / Crohn etc……….
CD sieroneagtiva
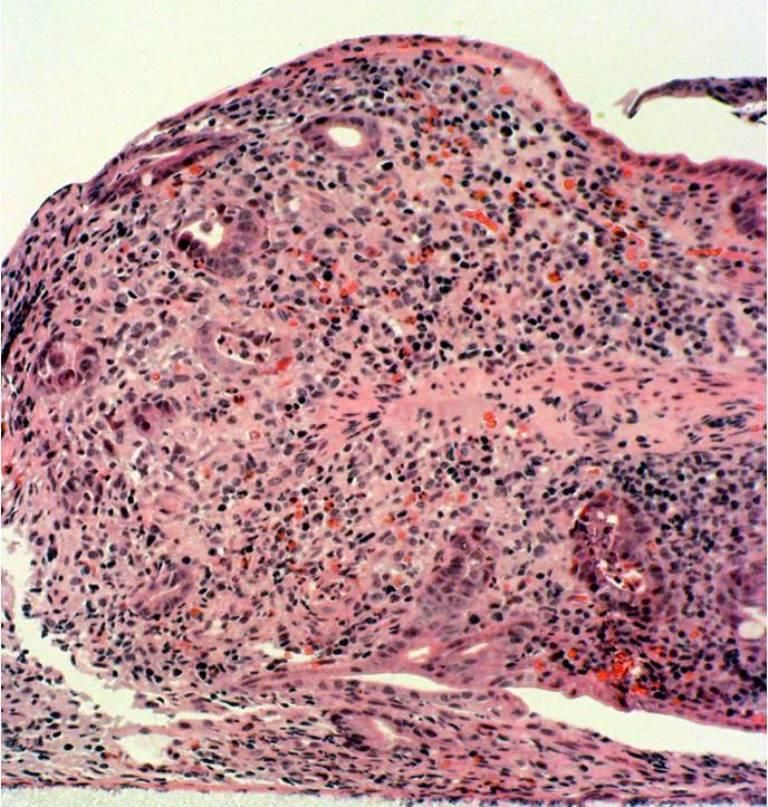
Volta U et al., DLD 2016;48:1018-22Dig Liver Dis 2006, 38:926-929
Severe malabsorption syndrome with diarrhea and weight loss
Total villous atrophy with marked inflammation and apoptotic bodies
IgG and IgA anti enterocyte autoantibodies
Frequent association with other autoimmune disorders
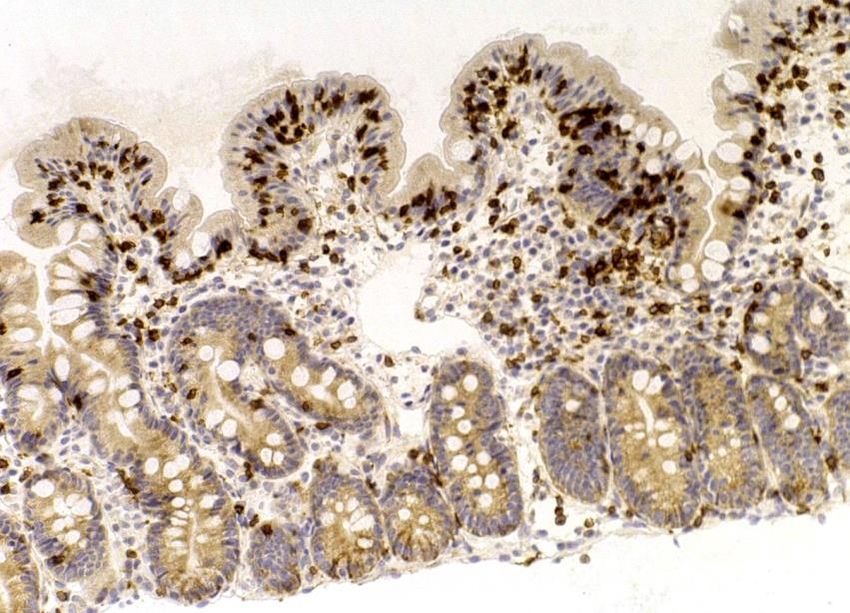
Good response to steroids and immunosuppressive treatmentGiardiasis • Clinical picture of severe malabsorption with diarrhea, abdominal pain, bloating, nausea, vomiting and weight loss • Villous atrophy (usually mild or partial) with an increased number of IELs mimicking celiac disease • The finding of Giardia Lamblia cysts in the small intestinal biopsy allows to distinguish giardiasis-related villous atrophy from seronegative celiac disease Granito A, Volta U et al Am J Gastroenterol 2004;99:2505-2506
Am J Gastroenterol 2010;105:2262-75
• CVID is characterized by decreased
levels of at least two serum
immunoglobulin isotypes
• Up to 50% of patients complain of
chronic diarrhea and malabsorption
.
• A minority of CVID cases can
have a concurrent CD. This
peculiar association can be
proven by a good
clinical/histological response to
GFDOlmesartan-induced malabsorption syndrome
• Angiotensin-2-receptor blockers
can determine a malabsorption
syndrome with diarrhea and
weight loss, mimicking celiac
disease
• Discontinuation of the drug
leads to resolution of the small
intestinal damage and sympto-
matology
Nielsen JA et al, WJG 2013 A- Flat intestinal mucosa during olmesartan treatment
B- Normal intestinal mucosa after stopping olmesartanComparison between seronegative
and seropositive celiac disease (CD)
Volta U et al., DLD 2016;48:1018-1022
A – Seronegative CD B – Seropositive CD
14 cases 796 cases
Female/Male ratio 6:1 3.5:1
Median age at CD diagnosis 49 years (range 19-75) 36 years (range 18-78)
Classical phenotype (diarrhea, 100% 34%
malabsorption)
Total villous atrophy 57% 36%
Autoimmune disorders 43% 30%
Family history of CD 29% 10%
Median Age at CD diagnosis in A vs B: P < 0.005; classical phenotype in A vs B: P < 0.001Histogical, genetic and autoimmune features in seronegative celiac disease (CD)
Gender/age HLA Duod. biopsy Associated Disorders Autoantibodies
Male 58 yrs DQ2 homoz. total atrophy Autoimm. thyroiditis ANAd
Female 34 yrs DQ2 mild atrophy Primary biliary cholang. AMA M2
Female 37 yrs DQ2 total atrophy none none
Female 75yrs DQ2 homoz. total atrophy none none
Female 45 yrs DQ2 mild atrophy none none
Female 55 yrs DQ2 homoz. total atrophy Gluten ataxia ANAs, CNS
Male 61 yrs DQ8 partial atrophy Peripheral neuropathy CNS, ENS
Female 48 yrs DQ2 total atrophy none none
Female 49 yrs DQ2 homoz. mild atrophy Autoimm. gastritis HPC, ANAs
Female 30 yrs DQ2 partial atrophy none ASMA
Female 63 yrs DQ2 total atrophy none ANAs
Female 46 yrs DQ2 homoz. total atrophy none ANAs
Female 19 yrs DQ2 total atrophy none ANAs
Female 46 yrs DQ8 partial atrophy Autoimm. thyroiditis ANAs
AMA: mithocondrial aantibodies; ANA: antinuclear antibodies; HPC: human parietal cell antibodies; CNS, ENS: central
and enteric nervous system antibodies
Volta U et al., DLD 2016;48:1018-1022Causes (%) of non-responsive celiac disease (CD)
affecting up to 30% of CD patients
Eating disorders
2-4%
Microscopic colitis CVID
6-11% 1-2%
Inflammatory
colitis 7%
Lactose intoleranca
7-8%
Gluten ingestion
RCD and other 36-45%
complications
9-10%
SIBO 6-9% Incorrect CD
IBS 10-22% diagnosis
12%
Leffler DA, Clin Gastroenterol Hepatol 2007; 5::445-50Response to gluten-free diet in adult
coeliac disease in the Bologna CD center
190 (24.7%) out of 770 CD
pts with non responsive CD
Main causes of non
responsive CD: poor
compliance with the diet, IBS,
GERD, SIBO, lactose
intolerance, fructose
intolerance, microscopic
colitis)
Only 10% of non-responsive
CD patients had a complicated
coeliac diseaseThe impact of misdiagnosing celiac disease
at an Italian referral centre
CD diagnosis
confirmed in
only 61/180
pts (34%)
The re-evaluation of celiac disease (CD) cases diagnosed at other instutions in a
referral CD centre did not confirm the diagnosis in a high number of cases
An incorrect diagnosis of CD represents both a risk for the health of the patient
and a considerable waste of money, time and resources for institutions
Biagi F, Can J Gastroenterol 2009Complicated Celiac Disease (CCD)
Refractory Celiac Disease Other complications
Type 1 Type 2
• Ulcerative jejunoileitis
Severe villous atrophy yes CCD is rare•(Complicated celiac disease (CCD):
30-year experience (1985-2015) at CD Center of Bologna University
• 18 cases (1.9%) of CCD
1.9%
over 950 CD patients
diagnosed in the period
1985-2015
CD
CCD
• 14 females and 4 males
98.1% • Median age at CD
diagnosis: 59 years;
median age at CCD
diagnosis 62 yearsComplicated celiac disease (CCD) cases at CD Center of Bologna University 11 Refractory Celiac Disease (RCD) (8 type 1 and 3 type 2) 5 Small Bowel Adenocarcinoma (SBA) 3 Enteropathy Associated T-cell Lymphoma (EATL) 1 Ulcerative Jejunoileitis (UJ) Some patients developed more than one complication: UJ was observed in a patient with RCD type 1 and one EATL was diagnosed in a patient with a previous diagnosis of RCD type 2
Clinical features of complicated CD cases diagnosed at Bologna CD Center Pts-Gender Age at CD Clinical phenotype HLA Age at complication Outcome # 1- F 67 classical *DQ2 69, RCD-1, UJ Dead, 73 # 2- M 66 classical *DQ2 67, RCD-1 Dead, 70 acute MI # 3-F 45 classical *DQ2 46, SBA Dead, 47 #4-M 35 classical DQ2 35, EATL Alive, 44 #5-F 35 classical DQ2 35, EATL Alive, 58 #6-F 63 classical DQ2 65, RCD-1 Alive, 75 #7-F 68 classical DQ2 72, SBA Alive, 83 #8-F 80 classical *DQ2 81, RCD-1 Dead, 83 #9-F 45 classical DQ2 45, SBA Dead, 50 #10-M 64 classical DQ2 69, RCD-1 Alive, 82 #11-M 61 classical *DQ2 66, RCD-2, EATL Dead, 66 #12-F 63 classical *DQ2 66, RCD-2 Dead, 74 #13-F 59 classical DQ2 60, SBA Alive, 79 #14-F 50 classical *DQ2 54, RCD-1 Alive, 55 #15-F 57 classical DQ2 62, RCD-1 Alive, 66 #16-F 76 classical *DQ2 77, RCD-1 Alive, 78 #17-F 36 classical *DQ2 47, RCD-1 Alive, 48 #18-F 38 classical DQ2 38, SBA Alive, 40 *DQ2 homozygosis
Outcome of complicated celiac disease (CCD) • Of the 18 patients with CCD, 7 died in a period ranging from 6 months to 8 years from CCD diagnosis (median 3 years). • The cause of death was related to the CCD in all cases except one (a patient with RCD-1 died for acute myocardial infarction). • The 7 dead patients were affected by SBA (2 cases), RCD type2 +EATL (1 case), RCD (4 cases including 3 type 1 and one type 2). • On the whole 28% of complicated patients died within 5 years and 39% within 8 years from CCD diagnosis.
Take home message • Nowadays the clinical presentation of celiac disease (CD) is extremely variable so that this disorder seems to be a new disease in comparison with the unique wasting malabsorption syndrome described in medicine books only some decades ago • This is mainly the result of an improved knowledge of the disease thanks to the identification of at-risk groups for CD favoured by the availability of highly predictive biomarkers • CD can be regarded as a multifactorial, systemic, autoimmune disorder with a frequent involvement of many other organs outside the gut • An early CD recognition is mandatory in order to prevent its clinical manifestations and to avoid the development of associated autoimmune disorders and complications which seem to be more frequent in the cases with a significant diagnostic delay
You can also read

















































