Region 9 Healthcare Coalition Preparedness Plan - June 2018
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Region 9 Healthcare Coalition Preparedness Plan June 2018
The mission of the Washington State Region 9 Healthcare Coalition is to prepare for, respond
to, and recover from crisis using all available resources, providing patient care at the
appropriate level and in the most efficient manner.
The Region 9 Healthcare Coalition (R9 HCC) strives to build emergency preparedness and
response planning across the healthcare system to create resilient communities within the ten
counties and three tribes of eastern Washington. The R9 HCC collaborates with healthcare
partners on various projects and topics for regional healthcare system preparedness with the
goal to provide quality patient care during medical surge events. The activities of the R9 HCC
are funded under the United States Department of Health and Human Services through the
Office of the Assistant Secretary for Preparedness & Response (ASPR) Healthcare Preparedness
Program grant and administered through a cooperative agreement between the Washington
State Department of Health (DOH) and the Spokane Regional Health District (SRHD).
Region 9 Healthcare Coalition
509.324.1673 | hcc@srhd.org | srhd.org/hccRegion 9 Healthcare Coalition Preparedness Plan – Member Review Draft
PLAN APPROVAL AND REVIEW
The plan has been developed with member, stakeholder, and staff input. Region 9 Healthcare Coalition
core members approve the preparedness plan through a majority vote of quorum of the R9 HCC Core
Member Advisory Group and maintain involvement in annual reviews.
iRegion 9 Healthcare Coalition Preparedness Plan – Member Review Draft
RECORD OF CHANGES
Version No. Description of Change Date Entered Posted By
1.0 Approved by Core June 30, 2018 Travis Nichols
Member Advisory
Group email vote
iiRegion 9 Healthcare Coalition Preparedness Plan – Member Review Draft
TABLE OF CONTENTS
PLAN APPROVAL AND REVIEW ...................................................................................................................... i
RECORD OF CHANGES ................................................................................................................................... ii
1 INTRODUCTION ..................................................................................................................................... 1
1.1 Purpose of Plan ............................................................................................................................. 1
1.2 Compliance Requirements ............................................................................................................ 1
1.3 Planning Assumptions ................................................................................................................... 2
2 COALITION OVERVIEW .......................................................................................................................... 3
2.1 Mission and Scope ........................................................................................................................ 3
2.2 History ........................................................................................................................................... 5
2.3 Governance Structure & Organization.......................................................................................... 5
2.4 Roles & Responsibilities ................................................................................................................ 6
3 RISKS AND GAPS .................................................................................................................................... 8
3.1 Hazard Vulnerability Assessment.................................................................................................. 8
3.2 Key Gaps........................................................................................................................................ 9
4 COALITION OBJECTIVES....................................................................................................................... 10
4.1 Strategic Objectives: 2018-2022 ................................................................................................. 10
4.2 Operational Objectives: January 2018 – June 2019 .................................................................... 11
5 COALITION ACTIVITES AND SERVICES ................................................................................................. 12
5.1 Consultation and Subject Matter Expertise ................................................................................ 12
5.2 Information Sharing .................................................................................................................... 13
5.3 Communication ........................................................................................................................... 14
5.4 Resource Coordination ............................................................................................................... 15
5.5 Training ....................................................................................................................................... 15
5.6 Planning....................................................................................................................................... 15
5.7 Exercise Coordination ................................................................................................................. 17
5.8 After-Action Reviews .................................................................................................................. 17
iiiRegion 9 Healthcare Coalition Preparedness Plan – Member Review Draft
1 INTRODUCTION
1.1 Purpose of Plan
The Washington State Region 9 Healthcare Coalition (R9 HCC) preparedness plan documents how the R9
HCC plans and works collectively with members to promote communication, information sharing,
resource coordination, and operational response and recovery to emergencies and disasters. This plan
describes the roles and functions of the R9 HCC, members, and partners in preparing for emergencies
and unplanned events. The plan also addresses the coalition governance structure, roles and
responsibilities in preparedness, and strategic and operational objectives. R9 HCC will update the plan as
necessary after exercises and planned and real-world incidents. The review will include identifying gaps
in the preparedness plan and working with R9 HCC members and external partners to define strategies
to address the gaps.
The plan also meets the requirement set forth in the Office of the Assistant Secretary for Preparedness
and Response 2017-2022 Health Care Preparedness and Response Capabilities, published November
2016:
• Capability 1. Foundation for Health Care and Medical Readiness
o Objective 3. Develop a Health Care Coalition Preparedness Plan
1.2 Compliance Requirements
1.2.1 Legal and Regulatory Requirements for Preparedness
Health and Human Services Assistant Secretary of Preparedness and Response (ASPR) recognizes that
there is shared authority and accountability for the health care delivery system's readiness that rests
with private organizations, government agencies, and Emergency Support Function-8 (ESF-8, Public
Health and Medical Services) lead agencies. Given the many public and private entities that must come
together to ensure community preparedness, HCCs serve an important communication and coordination
role within their respective jurisdiction(s).
The HCC should:
• Understand federal, state, or local statutory, regulatory, or national accreditation requirements
that impact emergency medical care.
• Understand the process and information required to request necessary waivers and suspension
of regulations.
o Primarily 1135 waivers/CMS waivers
• Support crisis standards of care planning, including the identification of appropriate legal
authorities and protections necessary to support crisis standards of care activities.
1.2.2 Legal and Regulatory Requirements for Response
The HCC should:
• Maintain awareness of standing agreements for resource support during emergencies.
o Washington State Hospital Association Memorandum of Understanding
1Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
o Spokane Skilled Nursing Providers Disaster Plan Agreement
o East Region (Region 9) Memorandum of Understanding
o St. Joseph’s Regional Medical Center MOU
• Maintain awareness of relevant state and local ordinances, statutes, and rules that may affect
the coalition and its response as required including state and local emergency powers that may
affect the coalition response.
o Washington Article XI COUNTY, CITY, AND TOWNSHIP ORGANIZATION, § 11 of
Constitution
o RCW 70.05.060: Powers and Duties of Local Board of Health
o Washington DOH ESF 8 Plan – June 2015
o Washington DOH Medical Surge Response (ESF 8 Appendix 2)
o Washington DOH Basic Plan Annex 11 Medical Surge
o Spokane Comprehensive Emergency Management Plan and ESF-8 Document
1.3 Planning Assumptions
• The Secretary of Health may direct the statewide public health, healthcare, and EMS response
as necessary and is authorized by state law to protect the health of the public (RCW 43.70.130
and 43.70.020(3)).
• Healthcare organizations that are part of this plan follow the National Incident Management
System (NIMS) using the Incident Command System (ICS).
• Washington DOH is the lead agency for responding to multijurisdictional public health
emergencies in Washington.
• Local public health agencies serve as the ESF-8 lead in county Comprehensive Emergency
Management Plans (CEMPs). R9 HCC should be part of the ESF 8 list of response partners.
• Healthcare providers must meet CMS Emergency Preparedness Conditions of Participation and
maintain good standing under DOH licensing process.
• Physicians are expected to meet Institute of Medicine guidance for “duty to plan.” During
ordinary times, facilities providing acute medical care have a duty to serve patients; in
anticipation of extraordinary times, such facilities have a “duty to plan” for catastrophic
incidents, including planning for delivery of care along the continuum from conventional to crisis
surge response.1
• Washington is both a Home Rule and a Dillon’s Rule state. Washington’s constitution allows
cities to exercise all the police powers possessed by the state government, so long as local
regulations do not conflict with general laws adopted by the legislature.
• The delegation of authority for disasters and emergencies is under the County Sheriff or Deputy.
1
Institute of Medicine of the National Academies. 2012. Crisis Standards of Care A Systems Framework for
Catastrophic Disaster Response. Report Brief. March 2012. Url: https://www.nap.edu/resource/13351/CSC_rb.pdf
2Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
2 COALITION OVERVIEW
2.1 Mission and Scope
The R9 HCC works to strengthen emergency preparedness and response for all aspects of healthcare
through community coordination and collaboration. Healthcare coalition participation is appropriate for
all types of healthcare providers, mental health providers, EMS professionals, public health
professionals, emergency managers and related services.
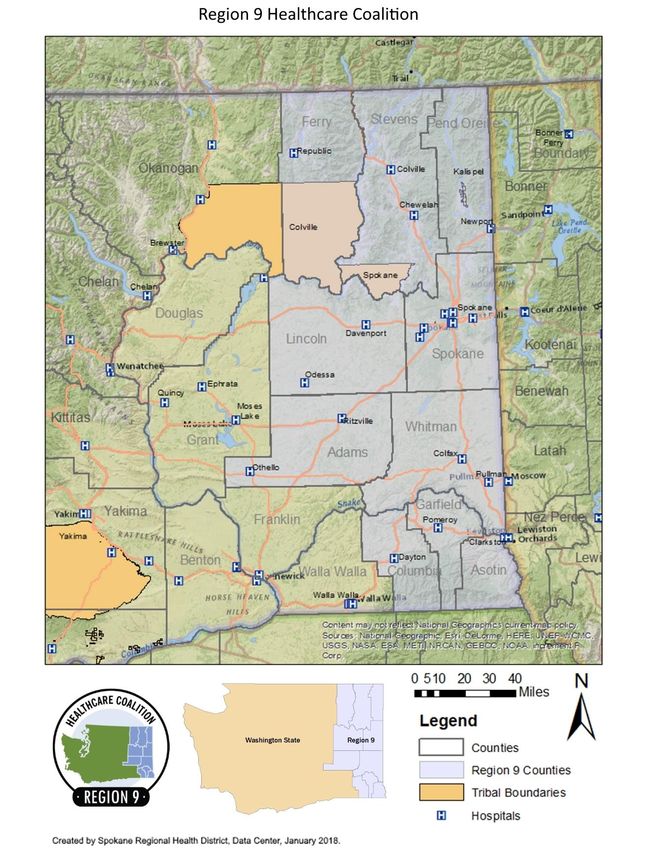
The R9 HCC serves as an emergency preparedness and response resource for ten counties and three
tribal areas in eastern Washington:
• Adams County • Lincoln County • Colville Tribe
• Asotin County • Pend Oreille County • Kalispel Tribe
• Columbia County • Spokane County • Spokane Tribe
• Ferry County • Stevens County
• Garfield County • Whitman County
The Region 9 area population is 10% of Washington’s total population at 671,178 residents, and covers
25% of the state’s land base at 16,454 square miles. The region has an average of 37.4 persons per
square mile and includes some of the most rural counties in the state, with Garfield, Ferry, and Columbia
counties all having less than 5 people per square mile; Garfield County is the least populated county in
Washington with 3.2 persons per square mile. 2
Regional planning efforts include the whole community, including individuals with access and functional
needs and vulnerable populations. Vulnerability to hazards is influenced by many factors, such as age or
income, the strength of social networks, and neighborhood characteristics. Understanding the region’s
geography and community profile can help the R9 HCC better prepare for and respond to emergency
events and hazards by identifying areas with higher vulnerabilities and higher rates of access and
functional needs. The coalition utilizes data to determine these populations and inform planning efforts.
Link: Region 9 Healthcare Coalition Regional Community Vulnerability Profile
The R9 HCC defines its boundaries based on a geographic region, but also acknowledges that the R9 HCC
must work with neighboring states and counties outside of the region as appropriate to address the
daily health care delivery patterns and natural patterns of patient movement during an incident.
2
U.S. Census Bureau. 2012-2016 American Community Survey.
3Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
4Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
2.2 History
• Community-based healthcare emergency preparedness planning started in 1985 under the
leadership of Ben Hayworth at Sacred Heart Hospital and Linda Cox at Deaconess Hospital. A
fatal helicopter crash at the Bloomsday Road Race catalyzed development of the Spokane
County EMS hospital subcommittee that was devoted to disaster planning.
• After Spokane County Firestorm 1991, Fairchild Air Force Base active shooter MCI in 1994,
Fairchild B-52 crash MCI and Ice storm 1996 it was clear that healthcare disaster planning
needed to inclusively cover a regional network of counties.
• In 1997 East Region EMS Organization formed the Hospital Planning Subcommittee, under the
leadership of Spokane Regional Health District (SRHD) through discussions around emergency
preparedness for hospitals at a regional level.
• In 2002 after the September 11, 2001 attacks and the 2002 anthrax attacks, the National
Bioterrorism Hospital Preparedness Program (NBHPP) in the Health Resources and Services
Administration (HRSA) at HHS funded healthcare emergency and disaster planning.
• The Region 9 Healthcare Coalition is formed in 2005 under the leadership of Ed Dzedzy as East
Region EMS Hospital Planning Committee chair, taking guidance from the “2004 Medical Surge
Capacity and Capability: A Management System for Integrating Medical and Health Resources
During Large-Scale Emergencies (MSCC Handbook).”
• In 2008, the Region 9 Healthcare Coalition administration shifts from East Region EMS to SRHD
under the leadership of Susan Sjoberg.
• In 2010, the R9 HCC hired its first employee, Erika Henry, to advance several objectives of the
HCC, from conducting a complete regional assessment of current capabilities and gaps, to
growing the membership beyond its core of hospital partners. A second employee, Travis
Nichols, was hired in 2014.
• Since 2014, the R9 HCC has been steadily growing its membership and staff to support
preparedness and response activities across the region, including hiring a coordinator, training
and exercise coordinator, information specialist, communications specialist, and planner
between 2014 and 2017. Recent response activities have included Ebola, seasonal influenza,
windstorms, and wildfires.
Link: Region 9 Healthcare Coalition History
2.3 Governance Structure & Organization
Washington State Department of Health (DOH) is funded under the United States Department of Health
and Human Services (DHHS) through the Office of the Assistant Secretary for Preparedness & Response
(ASPR) Healthcare Preparedness Program (HPP) grant. Spokane Regional Health District currently serves
as the fiduciary agent for the HPP funding from DOH in a July 1 – June 30 grant cycle to administrate the
R9 HCC.
The R9 HCC uses a customer-focused service model to identify opportunities to serve the needs of
members and partners in alignment with the ASPR HPR 2017-2022 Health Care Preparedness and
Response Capabilities. The R9 HCC is not a stand-alone organization (nonprofit or otherwise);
5Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
accordingly, it is governed by the programmatic, division and Spokane County Board of Health
expectations and requirements of SRHD.
The HCC structure executes activities related to healthcare delivery system readiness and coordination.
The R9 HCC has a diverse membership, that includes, at a minimum, hospitals, emergency medical
services (EMS), emergency management organizations, and public health agencies. Other members
include healthcare clinics, blood centers, dialysis, long-term care and skilled nursing facilities, behavioral
health services and organizations, home health agencies, and non-governmental organizations.
Coalition Chair:
• The chair shall provide leadership for the R9 HCC. He/She shall act as chair over all R9 HCC
General Meetings and assist in developing agendas and content.
• The chair or designee shall also serve as the official representative and spokesperson of the R9
HCC and act as the liaison to other support foundations and agencies.
• The chair shall lead and facilitate the Core Member Advisory Group.
• A Coalition Chair shall be appointed for a two-year term by the Core Member Advisory Group.
The Chair can be re-appointed up to three terms.
HCC Staff:
The HCC staff are responsible for:
• Planning, implementing and evaluating HCC activities;
• Sharing information and resources with members and partners;
• Managing HPP grant documentation requirements, such as work plan deliverables and
state/national reporting;
• Providing assistance to healthcare organizations to improve capabilities; and,
• Coordinating planning, response and recovery amongst HCC members and partners.
Link: Region 9 Healthcare Coalition Structure
2.4 Roles & Responsibilities
2.4.1 Members
Membership in the R9 HCC is defined as any healthcare entity within the ten counties and three tribal
nations of eastern Washington that actively contribute to strategic planning, operational planning and
response, information sharing, and resource coordination and management. HCC membership does not
begin or end with attending meetings.
In practice this means completing the following elements within one calendar year:
• Participation in R9 HCC Essential Elements of Information Response Process.
o Provision of three deep contact list for EEI participation
o Provision of situational report distribution contacts
• Share in writing; incident, regulatory survey findings, or exercise outcomes and lessons learned
with R9 HCC that can be distributed to members.
• Participation in one of the following options:
o Attendance and contribution to a planning or advisory workgroup.
6Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
o Attendance or participation at R9 HCC sponsored training or exercise.
o Presentation at a R9 HCC meeting or submit newsletter article.
Members will receive a participation letter at the end of the calendar year that acknowledges their
contributions and community coordination to assist with fulfillment of Center for Medicare and
Medicaid Services (CMS) Emergency Preparedness condition of participation requirements.
Link: Region 9 Healthcare Coalition Membership Definition
2.4.2 Core Members
Core members in R9 HCC consist of all hospitals (including critical access hospitals and specialty
hospitals), and delegate representatives from East Region EMS & Trauma Care Council, R9 Public Health
Emergency Preparedness and Response Group, and Region 9 Emergency Management
CoordinatingGroup. Through the representative model all EMS, public health and emergency
management organziations in Reigon 9 are represented.
Link: Region 9 Healthcare Coalition Core Organization Letter
2.4.3 Partners
A coalition partner is defined as stakeholders recognized by ASPR, CMS, NIMS, or other community
structures who could benefit from the mission and work of the R9 HCC.
2.4.4 Core Member Advisory Group
• The Core Member Advisory Group informs and reviews HCC priorities and approves outputs like
preparedness and response plans.
• It is the responsibility of the member to relay information as appropriate to their healthcare
sector and to maintain contact with their healthcare sector so that they are representative of
their sector and not just their agency.
• It is the responsibility of any healthcare sector to communicate with their representative and
assure that their representative speaks on their behalf.
• The meeting follows a formal meeting structure and is led by the Chair.
Link: Core Member Advisory Group Charter
2.4.5 Strategic Advisory Group
• The Strategic Advisory Group is tasked with advising Healthcare Coalition leadership in
developing, refining, and implementing strategic direction and priorities to advance and sustain
the mission of the coalition.
• This group seeks to advance the coalition as a group of vested agencies and the coalition as an
agency, and will provide recommendations on proposals that advance the R9 HCC mission and
organizational structure. This group seeks opportunities and strategies to sustain the broader
inclusive and holistic work of healthcare emergency preparedness planning in the region.
• Representatives of the Strategic Advisory Group are asked to act on the behalf of the shared
interests and well-being of all R9 HCC stakeholders and members, including but not limited to
their agency, discipline or provider type.
7Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
• The Advisory Group leverages the experience, expertise, and insight of each member and their
unique perspective to develop strategic direction and priorities for the R9 HCC.
• Representatives are invited and appointed to participate in the advisory group by R9 HCC
leadership. Members typically serve a one-year term at the pleasure of the R9 HCC leadership
and are asked to nominate replacements if they need to step down.
2.4.6 Workgroups
• Workgroups consist of a group of experts working together to achieve specified goals. The
groups are domain-specific and focus on discussion or activity around a specific subject area.
• The workgroup has a clear purpose, an achievable objective and timeline for completion. The
lifespan of a working group can last anywhere between a few months up to two years.
• Upon reaching specified goals, the group is intended to disband.
3 RISKS AND GAPS
The R9 HCC identifies and plans for risks, in collaboration with the ESF-8 lead agency, by conducting
assessments or using and modifying data from existing assessments for healthcare readiness purposes.
These assessments can determine resource needs and gaps, identify individuals who may require
additional assistance before, during, and after an emergency, and highlight applicable regulatory and
compliance issues. The R9 HCC and its members may use the information about these risks and needs to
inform training and exercises and prioritize strategies to address preparedness and response gaps in the
region.
3.1 Hazard Vulnerability Assessment
The 2017-2022 Regional Healthcare Hazard Vulnerability Assessment (HVA) evaluated vulnerability to
specific hazards and addressed anticipated and unanticipated risks that are most likely to have an
impact on healthcare’s ability to provide services. The assessment focused on the input of healthcare
partners as the primary stakeholder. It utilized an all-hazards approach that includes naturally-occurring
events, human-related events, hazardous materials events, and technologic and utility events.
Top 10 Hazards Weighted by Risk Response:
1. Mass Casualty (Trauma)
2. Pandemic Influenza
3. Highly/Acute Infectious Disease Outbreak
4. Wildfire
5. Severe Blizzard/Snow Fall
6. Mass Electrical Failure
7. Potable Water Failure
8. High Winds
9. Chemical, Biological, Explosives, Radiological, and Nuclear Events (CBRNE)
10. Water-/Foodborne Disease Outbreak
Link: Region 9 Healthcare Coalition Regional Healthcare Hazard Vulnerability Assessment
8Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
Through a series of two surveys and a webinar, healthcare partners reviewed and rated 39 hazards
based on the probability of the event as measured in response and occurrence, and the impact of those
hazards to healthcare services. The hazards are weighted by risk response to reflect the estimated
priority for a regional response. The list was developed with input from R9 HCC members with an
emphasis on healthcare and EMS partners. As such, it is not a comprehensive assessment of all
members or disciplines, and does not provide details regarding the unique attributes and risks for
individual counties or facilities. The regional hazard vulnerability assessment is not a replacement for an
organization- or facility-specific HVA.
3.2 Key Gaps
A gap analysis consists of three components: prioritizing response objectives (utilizing the Coalition
Assessment Tool, an HHS assessment tool); identifying response capability gaps (utilizing the After-
Action Reviews and Improvement Plans and Training Needs Assessments); and inventorying durable
medical equipment (DME). Each component has a unique timeline for updating, which is adaptable to
changes in the coalition’s capacity, design, and needs.
Link: Eastern Washington Training Needs Assessment
For the first component, the R9 HCC determines a level of importance score for each of the seventeen
Healthcare Preparedness and Response Capabilities objective using a five-point scale ranging from not
relevant to critical. The R9 HCC focuses on the areas scored as “highly important” and “critical” to the
success of the R9 HCC’s response as an agency. Reviewing the priority score will be completed in line
with strategic planning processes, however little change is anticipated.
Five areas from the ASPR 2017-2022 Health Care Preparedness and Response Capabilities were
identified as highly important, where the R9 HCC has a major role in coordinating the work,
• Capability 1, Objective 1: Establish and Operationalize a Healthcare Coalition
• Capability 1, Objective 3: Develop a Healthcare Coalition Preparedness Plan
• Capability 2, Objective 1: Develop and Coordinate Healthcare Organization and HCC Response
Plans
• Capability 4, Objective 1: Plan for a Medical Surge
• Capability 4, Objective 2: Respond to a Medical Surge
Three areas were identified as critical, the core of the R9 HCC’s mission and functions:
• Capability 1, Objective 4: Train and Prepare the Healthcare and Medical Workforce
• Capability 1, Objective 5: Ensure Preparedness is Sustainable
• Capability 2, Objective 2: Utilize Information Sharing Procedures and Platforms
The priorities go through a further analysis utilizing ASPR’s Coalition Assessment Tool (CAT). The CAT is
conducted bi-annual to track progress. The coalition assesses the work completed related to each
objective, and is provided with a percentage progress score for each objective. The combination of
priority and progress further refines what areas the HCC should focus attention.
9Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
The second component of the gap analysis focuses on identifying coalition capabilities gaps. This
information is gather through two sources: exercise and real-world event improvement plans and a
training needs assessment. Improvement plans highlight both regional and facility planning, training and
coordination gaps. This information is not only used to update plans, policies and procedures, but also
integrated into training and exercise plans. Annually, a focused training needs assessment is conducted
based on the exercises planned for that year. Every four years a comprehensive training needs
assessment is conducted to identify general training gaps across the region and used to develop a multi-
year training and exercise plan (MYTEP).
The Training Needs Assessment uses a capabilities-based approach. The capabilities included in the
survey are primarily identified through ASPR 2017-2022 Health Care Preparedness and Response
Capabilities. Additional areas included in the assessment are based on foundational ICS principles,
regional priorities, and known areas of interest. HCC members are asked to rate the proficiency of their
key staff on a range of preparedness functions. Respondents are also asked to rate the level of priority
they would rank the stated capability described. Respondents are self-selected representing single
facilities or multi-facility organizations. Emails are sent to all coalition members and other healthcare
partners by their respective coalition through the coalition’s contact database. The data is analyzed to
determine the training gaps: capabilities that have the highest priority and lowest proficiency combined
score. Training gaps that are relevant across partners and aligns with coalition priorities are integrated
into the Training and Exercise Plan.
The third component of the gap analysis is the durable medical equipment (DME) survey. Every year, the
HCC edits the DME survey for language continuity and missing opportunities by reviewing the following
resources:
• CMS COOP equipment requirements
• WATrac Specialties
• Russell Phillips DMCC Toolkit
• Supply Chain Workgroup Assessment – Northwest Healthcare Response Network
• ASPR Tracie Resource Management Logistics
Once finalized with input from members and coordination with NWHRN, the survey is distributed to all
R9 HCC agencies with a 2-3-week window for completion.
4 COALITION OBJECTIVES
4.1 Strategic Objectives: 2016-2022
1. Achieved in 2016 and ongoing priority: Responsive to the needs of partner agencies (Healthcare,
Public Health and Emergency Management) in disaster events, specifically related to gathering,
aggregating and delivering timely accurate situational awareness that contains the Essential
Elements of Information needed for users to make critical decisions.
a. Develop the HCC response plan by June 2019, and review the response plan on an
annual basis.
10Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
2. Achieved in 2017 and ongoing priority: Provides meaningful engagement with Hospital
Administrators, clinicians, Emergency Managers, Security and Facilities Staff such that it is able
to support the “meaningful use”, Centers for Medicare and Medicaid Services and Joint
Commission emergency preparedness accreditation and licensure requirements for emergency
preparedness and response. Strategies will include:
a. Clinical Engagement in crisis standards of care development through a local Disaster
Clinical Advisory Committee.
b. Target partner (Blood, Dialysis, Hospitals, Skilled Nursing, etc.) engagement through
education and training coupled with lessons learned from real world events and
information sharing utilizing the Healthcare System Operational Response Committee &
WATrac.
c. Administrative Engagement: Implement Exploratory Healthcare Coalition Board of
Directors to guide sustainability and implementation.
3. 2018 target: Serve the healthcare system as the primary coordination center for disaster and
emergency planning with healthcare partners including Hospitals, Blood Centers, Dialysis and
Skilled Nursing Facilities. A regional healthcare system that feels that they would be less
effective in a disaster without the presence of a regional Healthcare Coalition.
4. 2020 target: Has a stable funding model that includes community support as a portion of its
budget.
4.2 Operational Objectives: January 2018 – June 2019
By June 2019, the R9 HCC will:
1. Have a comprehensive, clean, and up-to-date contact database with a process for ongoing
maintenance.
2. Improve the Coalition’s understanding of current resources, capabilities and member needs
through ASPR, DOH, and coalition driven assessments.
3. Effectively expand the Coalition to 60% of the geography of Washington State through the
integration of R7, R8 and R9 healthcare coalitions, using the Operational Strategy for Coalition
Integration.
4. Identify the gaps in our region’s ability to evacuate and place 20% of total regional staffed acute
care beds utilizing the R9 DMCC plan and facility EOPs.
5. Expand and improve the use of WATrac among hospitals and other healthcare providers.
6. Increase the number of active HCC members
7. Improve members’ ability to implement patient tracking procedures as described in the Patient
Tracking Plan
8. Effectively respond to real events utilizing appropriate regional, state, and federal plans, policies
and procedures.
11Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
5 COALITION ACTIVITES AND SERVICES
The R9 HCC uses a customer-focused service model to identify opportunities to serve the needs of
members and partners in alignment with the ASPR HPR capabilities. Member feedback to advise the
work of the R9 HCC is gathered through methods like advisory group meetings, planning workgroups,
survey and assessment findings, staff interactions with partners, exercise and incident after action
reports. Input is collected and used to inform the deliverables and work of R9 HCC staff.
The Washington preparedness program is funded largely by a grant for public health emergency
preparedness and response from the Centers for Disease Control and Prevention and a hospital
preparedness program grant from the Assistant Secretary for Preparedness and Response. The two
grants require Washington DOH to develop domains and capabilities that will help increase readiness for
any emergency. These deliverables drive the HCC work in preparedness and response.
5.1 Consultation and Subject Matter Expertise
5.1.1 Convening and Interviews
R9 HCC acts as a meeting convener at a local, regional or state level to assist organizations who may not
work together, or may be perceived as competitors, to identify shared benefit in collaboration or
cooperation. During response periods R9 HCC will utilize a network of contacts to assess, inform and
understand challenging incidents that may benefit from local or regional solutions. Informational
interviews are used to identify the challenges, needs and available resources to inform the collective
response.
5.1.2 CMS Workgroups
A forum for provider types to coordinate on their compliance activities with the CMS Emergency
Preparedness Condition of Participation. Sharing plans, survey findings, exercise coordination and
sharing of knowledge comprise activities of these workgroups.
5.1.3 Policy and Analysis
DOH Hospital Capacity Workgroup: To address excessive patient loads and limited hospital bed capacity
resulting in long waits in emergency departments, the Washington DOH and Public Health—Seattle &
King County convened a statewide workgroup in 2017 that consisted of representatives from hospitals,
the Washington State Hospital Association, EMS providers, and state and local officials. The workgroup
concluded that sharing standardized data on hospital capacity with regional partners is an essential step
to better manage regional demands on our healthcare facilities and to improve our understanding of the
magnitude, root causes and potential solutions to the problem of excessive patient loads and surge
demands.
Link: Hospital Capacity Assessment Report
12Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
5.2 Information Sharing
5.2.1 WATrac
The Washington System for Tracking Resources, Alerts, and Communication (WATrac) is a web-based
application serving the Washington healthcare system by providing two distinct functions: 1) daily
tracking of patient care bed availability and agency status; and 2) incident notification and situational
awareness for disaster response. WATrac is a tool that assists healthcare across the state to provide
coordinated patient care in an incident involving patient placement and tracking. The R9 HCC serves as
the WATrac Regional Lead for Region 9 and manages user accounts.
Link: WATrac Information
5.2.2 Patient Tracking Coordination
The Region 9 Patient Tracking Concept of Operations was developed for coordination of patient tracking
information in an emergency. Patient tracking determines and documents the identity of the patient,
the patient’s whereabouts, and the patient’s condition as they move from the scene to the hospital.
Patient tracking also helps facilitate family reunification and supports the Family Assistance Center. The
concept of operations is applicable for events ranging from smaller MCI events when a centralized
regional coordinating group may not be necessary, as well as, catastrophic events when a regional
coordinating agency will be vital in centralizing patient tracking information and ensuring the
appropriate and timely dissemination of information.
Link: Patient Tracking Concept of Operations and Procedures
5.2.3 Situational Awareness Response Process
The R9 HCC Situational Awareness Response Process is an information sharing process used during an
incident to develop inter-agency situational awareness regarding the operational status of the
healthcare system. This process gathers Essential Elements of Information (EEI) from healthcare
partners to create and maintain relevant Situational Awareness (SA) / Common Operating Picture (COP)
during an incident, through the collection, aggregation and distribution of information to R9 HCC
partners. Phone, email or other communication formats may be used by R9 HCC to seek clarification to
the data received, seek out missing information, or inquire about needs identified in the EEI collection
process.
The R9 HCC Situational Awareness Response Process is not meant to replace the communications
between first responders, hospitals or other agencies in the initial hours of an incident. Historically the
highest use has been in long duration incidents, incidents with broad geographic impact or across
multiple types of healthcare providers.
Link: EEI Process Information
5.2.4 Coordination Calls
Coordination calls occur as necessary with healthcare organization senior executives with institutional
decision-making authority. Titles of health care executives may include but are not limited to, President,
Chief Executive Officer, Chief Operating Officer, Chief Medical Officer, Chief Nursing Officer, and Medical
Director.
13Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
5.2.5 Executive Objectives
The R9 HCC seeks feedback and direction from healthcare executive leadership to ensure that the
strategic priorities of healthcare providers are aligned with the products and services of the healthcare
coalition. Feedback formats are currently informal and intermittent.
5.3 Communication
The R9 HCC strives to keep members engaged in emergency preparedness information and activities
through a variety of methods including email newsletters and bulletins, bi-monthly general meetings,
and information shared on our website and social media platforms. The R9 HCC aims to provide the
most accurate and timely information as possible to keep members well-informed.
5.3.1 24/7 Contact List
R9 HCC maintains and updates a comprehensive regional list of healthcare, emergency management
and public health 24/7 contact information.
Link: Region 9 24/7 Contact List
5.3.2 Electronic Communications
The Coalition Connection Newsletter is a bi-monthly e-publication containing information on status of
R9 HCC workgroups and committees, updates and stories regarding emergency preparedness and best
practices, general membership meeting previews and summaries, along with a list of upcoming events
around the region, including training opportunities and conferences. The R9 HCC sends a smaller e-
publication, the Coalition Connection Bulletin. These more frequent publications serve as timely, but
succinct reports on immediate information such as cyber alerts, webinars, new resources, current
incident response updates, and other regional and national news.
5.3.3 Bi-Monthly General Meetings
The R9 HCC hosts bi-monthly general membership meetings on the fourth Thursday of odd months of
the year that are open to all types of healthcare providers, emergency medical services, mental health
providers, public health professionals, emergency managers and related services. Meetings provide
partners with the opportunity to network, understand the roles and responsibilities of partner agencies,
and sharing of information, best practices and lessons learned from responses.
Link: General Meetings Agendas
5.3.4 Educational Materials
R9 HCC shares and produces regional information sheets designed to inform and educate R9 HCC
partners on plans, response, process’ or events. Formats can include whitepaper, one-page information
sheet or infographics.
Link: Region 9 Healthcare Coalition Website
14Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
5.3.5 Annual Report
R9 HCC produces an annual report that displays the full scope of work R9 HCC members and the agency
have created during the R9 HCC year (July 1 – June 30).
Link: Region 9 Healthcare Coalition Annual Report
5.3.6 Survey and Evaluation
The R9 HCC conducts occasional assessments and evaluation methods to gather information and
feedback on member participation, satisfaction, and the value of the Coalition activities.
5.4 Resource Coordination
5.4.1 Durable Medical Resource Inventory
R9 HCC maintains a list of services and essential equipment that may be needed by your facility or
others during an emergency response. This information is compiled into an Emergency Support Function
(ESF) 8 Resource Manual and database. Access to this information at time of need allows requesting
agencies to focus on their local emergency and providing immediate patient care while the HCC works to
locate the needed resources. The data may also be used to anticipate situation specific resource needs
and begin the process of identifying availability at the local, regional and state levels.
5.4.2 Alternate Care Facilities (ACF) Trailer
Purchased with HHS ASPR HPP funding, ACF trailers serve as a resource that can be utilized to augment a
burdened healthcare system. During a public health emergency or disaster, there may be times when
hospitals, ambulatory care or long-term care facilities are not able to accommodate all those who need
care. Depending on the reason behind the reduced capacity, an ACF may provide one or more types of
care, including in-patient, ambulatory, and/or palliative care. The Local Health Officer at SRHD
authorizes the opening of an ACF that is independent of a healthcare facility or set up in support of or
with the assistance of the Red Cross.
5.5 Training
The R9 HCC makes training opportunities available to healthcare coalition members and partners.
Trainings are provided based on member needs and coalition priorities. Trainings that demonstrate a
gap in R9 HCC members’ preparedness competency, are not facility specific, and have been prioritized
based on the MYTEP are provided by the Coalition. The Coalition provides regular trainings on WATrac,
periodic trainings on regional plans, and organizes one or two additional priority trainings when
possible. Additionally, the R9 HCC shares other regional and national training opportunities through a
monthly training calendar, with priority trainings highlighted in R9 HCC’s online Bulletin.
5.6 Planning
The R9 HCC leads planning activities that enhance preparedness for disasters and emergencies, including
preparedness and response planning as well as planning for specific topics or events.
15Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
The R9 HCC participates in and attends local, regional, and state planning meetings. In addition, the R9
HCC participates and contributes to regional and state planning processes around topics including
medical surge, patient movement, supply chain, and WATrac. Below is a list of meetings and processes
that the R9 HCC participates in.
• Local Planning
o Local Emergency Planning Committee (LEPC)
o EMS Trauma Council
• Regional Planning
o County partner agency site visits
o Disaster Medical Coordination Center (DMCC)
o Region 9 Disaster Behavioral Health Response Plan Meetings
o R9 Emergency Management Coordinating Group meetings
o R9 Local Health Jurisdiction Public Health Emergency Preparedness Meetings
o East Region EMS
• State Planning
o State patient placement (DMCC) planning
o Mass patient movement planning
o Catastrophic incident planning
o Supply chain planning
o WATrac Advisory Board
o EVD Planning and Region X EVD
5.6.1 Disaster Medical Coordination Center
The Disaster Medical Coordination Center (DMCC) system attempts to place patients based on need
during a mass casualty incident (MCI) or healthcare facility evacuation at the healthcare facility most
appropriately able to care for them in the most efficient amount of time using the guidance provided by
hospitals. The R9 HCC supports local DMCC and healthcare organizations within the region as
appropriate.
Link: Region 9 Healthcare Coalition DMCC Plan
5.6.2 Crisis Standards of Care
Established in 2016 the Spokane County, the Spokane County Disaster Clinical Advisory Committee
(DCAC) was established in 2016 guides clinical decision-making working toward clinical policy
recommendations, guidance, protocols and expertise to support healthcare system emergency planning
and response on key issues such as medical surge, resource conservation and management, and clinical
care strategies, including altering the standards of care in a disaster.
Link: Disaster Clinical Advisory Committee Draft Charter (2016)
16Region 9 Healthcare Coalition Preparedness Plan – Member Review Draft
5.7 Exercise Coordination
R9 HCC leads or participates in exercises that evaluate coordinated healthcare system responses. As
appropriate, R9 HCC exercises follow the Homeland Security Exercise and Evaluation Program. Common
elements that may be evaluated during an exercise include SOPs, organizational structure, or the
effectiveness of specific technologies used by the Coalition during emergency response. Single facility
exercises are not in the R9 HCC’s scope of practice, but the R9 HCC may occasionally assist in single
facility exercise design as subject matter experts.
Feedback for the exercise evaluation may be gathered in the form of assessments from the evaluators,
role players, and the exercise participants.
• Post-exercise “hot wash”: This activity is usually conducted immediately following an exercise to
identify key successes or challenges while they are still “fresh” in the minds of the participants.
Representatives from all entities that participated in the exercise should be included.
• After Action Report (AAR) process: The AAR process is a formal and comprehensive process
conducted after the exercise to analyze data and observations, positive and negative, related to
system performance.
5.8 After-Action Reviews
After exercises or real-world incidents, the R9 HCC facilitates After-Action Review Meetings to assist in
collection of post exercise, or incident, information. The information collected during After-Action
Reviews contribute to the development of After-Action Reports. All R9 HCC lead exercises include After
Action Review Meetings and After-Action Reports. In the case of real-world incidents, the R9 HCC may
lead After-Action Review Meetings if the incident had a significant impact on the healthcare system.
Link: After Action Reports
17You can also read

















































