Respiratory illness linked to poor air quality at an indoor ice arena - BCMJ
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

March 2020: 62:2
Pages 41– 80
Respiratory illness
linked to poor
air quality at an
indoor ice arena
IN THIS ISSUE
Improving care for patients with 22q11.2 deletion syndrome
Incorporating the patient’s voice into QI activities
Canadian Blood Services: More than just blood
Exercising in pollution
Health impacts of sea level rise on coastal communities bcmj.org
BC Medical Journal vol. 62 no. 2 | march 2020
41
March 2020
Volume 62 | No. 2
Pages 41–80
How do we weigh the risk of exercising in pollution against the detrimental health effects of a sedentary lifestyle? Article on page 65.
The BCMJ is published by Doctors of BC. The
journal provides peer-reviewed clinical and review
44 Editorials Author replies, Mark Elliott, MD
articles written primarily by BC physicians, for Scents and sensibility, Jeevyn K. Doctor shortage, Jonathan M.
BC physicians, along with debate on medicine Chahal, MD Winner, MD
and medical politics in editorials, letters, and
essays; BC medical news; career and CME listings; Human nature in times of stress,
physician profiles; and regular columns. David Richardson, MD CLINICAL
Print: The BCMJ is distributed monthly,
other than in January and August.
46 President’s Comment 50 Cluster of respiratory illness
Web: Each issue is available at www.bcmj.org.
Amplifying value, Kathleen Ross, in British Columbia linked to
Subscribe to print: Email journal@doctorsofbc.ca.
Single issue: $8.00 MD poor air quality at an indoor
Canada per year: $60.00
ice arena: A case report, Hilary
Foreign (surface mail): $75.00
47 Letters
Subscribe to notifications: Drake, BSc, Courtney Zimmerman,
To receive the table of contents by email, visit
Re: The age of mushrooms is upon
BTech, Guy Osachoff, CPHI(C),
www.bcmj.org and click on “Free e-subscription.” us in medicine, Chris Little, MD,
Prospective authors: Consult the Edward Brooks, MD Greg Baytalan, BSc, Muddassir
“Guidelines for Authors” at www.bcmj.org
Author replies, Mark Elliott, MD Siddiqui, BDS, Gillian Frosst, BSc,
for submission requirements.
Re: The age of mushrooms is upon us Silvina C. Mema, MD
in medicine, Jeffrey Eppler, MD
On the cover Editor Managing editor Proofreader Printing
Respiratory illness linked to poor David R. Richardson, MD Jay Draper Ruth Wilson Mitchell Press
air quality at an indoor ice arena Editorial Board Associate editor Web and social media Advertising
A recent case of respiratory illness Jeevyn Chahal, MD Joanne Jablkowski coordinator Kashmira Suraliwalla
following a hockey practice in David B. Chapman, MBChB Amy Haagsma 604 638-2815
Senior editorial and
Kelowna spurred an investigation Brian Day, MB
Cover concept and
or journal@doctorsofbc.ca
production coordinator
that revealed toxic levels of carbon Caitlin Dunne, MD
Kashmira Suraliwalla art direction, Jerry Wong, ISSN: 0007-0556
monoxide, nitrogen dioxide, and David J. Esler, MD
Peaceful Warrior Arts Established 1959
Yvonne Sin, MD Copy editor
particulate matter in the arena due
Cynthia Verchere, MD Barbara Tomlin Design and production
to a confluence of contributing
Laura Redmond, Scout Creative
factors. Article begins on page 50.
42 BC Medical Journal vol. 62 no. 2 | march 2020
54 Taking steps to improve care
and planning for patients in
British Columbia with 22q11.2
deletion syndrome, Matthew
Boroditsky, BHSc, Rebecca
Courtemanche, MSc, Douglas
Courtemanche, MD, Sandra
Robertson, BSN, Christine Loock,
MD
61 GPSC
The Patient Experience Tool:
Incorporating the patient’s voice into
quality improvement activities, Alana
Godin
62 Special Feature
Canadian Blood Services: More than
just blood, E.M. Wong, MD Canadian Blood Services offer more than just blood donation services. It also operates a stem cell donation and
transplantation service, helps coordinate organ and tissue donation and transplantation, and operates a national
65 COHP formulary for plasma protein products. Article on page 62.
Exercising in pollution: How to
counsel patients, JoyAnne Krupa,
MD n Seeking external reviewers for BC 71 BCCDC
guidelines Health impacts of sea level rise on
66 Premise n Lupus patients who take their BC’s coastal communities, Kevin
Consciousness, Mark Elliott, MD medications at lower risk for type 2 Liang, BSc, Tom Kosatsky, MD
diabetes
68 News 72 CME Calendar
n Reminder to submit GPSC portals 70 WorkSafeBC
14070/71 WorkSafeBC resources for 74 Guidelines for Authors
n Research suggests no difference in community physicians, Ernest
morning versus evening dosing for Salcedo, Celina Dunn, MD, Olivia 76 Classifieds
warfarin Sampson, MD
n Ronald McDonald House expanding
with new family room at Royal
Inland Hospital
Environmental impact Postage paid at Vancouver, BC. Canadian Publications Mail, Product Sales Agreement #40841036. Return undeliverable copies
The BCMJ seeks to minimize its negative impact on the to BC Medical Journal, 115–1665 West Broadway, Vancouver, BC V6J 5A4; tel: 604 638-2815; email: journal@doctorsofbc.ca.
environment by:
Advertisements and enclosures carry no endorsement of Doctors of BC or BCMJ.
• Supporting members who wish to read online with an
e-subscription to bcmj.org © British Columbia Medical Journal, 2020. All rights reserved. No part of this journal may be reproduced, stored in a retrieval system, or trans-
• Avoiding bag use, and using certified-compostable plant-based mitted in any form or by any other means—electronic, mechanical, photocopying, recording, or otherwise—without prior permission in
bags when needed writing from the British Columbia Medical Journal. To seek permission to use BCMJ material in any form for any purpose, send an email to
• Working with Mitchell Press, ranked third in North America for journal@doctorsofbc.ca or call 604 638-2815.
sustainability by canopy.org Statements and opinions expressed in the BCMJ reflect the opinions of the authors and not necessarily those of Doctors of BC or the
• Printing with vegetable-based inks institutions they may be associated with. Doctors of BC does not assume responsibility or liability for damages arising from errors or omis-
• Using FSC-certified paper sions, or from the use of information or advice contained in the BCMJ.
• Printing locally in British Columbia The BCMJ reserves the right to refuse advertising.
BC Medical Journal vol. 62 no. 2 | march 2020 43
editorials
Scents and sensibility
I
t’s 2020 and I’m wearing perfume. I wear use of fragrances. The association can outright release of histamine from human peripheral
Very Irresistible by Givenchy. Very irresist- ban certain fragrances or conduct risk assess- blood basophils. This increased basophil reac-
ible to some but apparently toxic to others. ments for potential adverse health effects. tivity to perfume was found in patients with
It took an incident at a friend’s house to There have been numerous studies done to respiratory symptoms related to perfume but
make me realize the effects that fragrances can evaluate the health effects of fragrances. An the mechanism causing the increased reactivity
have on some individuals. I went to spend a article in Environmental Research, “Neuro- was not known. This study was limited by its
weekend with my friend, and on day 1 every- toxicity of fragrance compounds: A review,”1 small sample size.
thing was great, but on day 2 I awoke to a chill states that most fragrance compounds belong Regulatory Toxicology and Pharmacology
in the air. It was a crisp January morning and to one of three families: phthalates, synthetic cites a paper from 2019, “Fragrance inhala-
my friend had opened all the doors to her home. musks, or chemical sensi- tion and adverse health
She had developed a cough, headache, and mild tizers. Phthalates enable effects: The question of
nausea in response to my perfume. She told the slow evaporation of The extent to which causation.”3 The authors
me that this was a common occurrence for her. the fragrance allowing these compounds are state that although some
I’ve also had patients complain of being the scent to linger lon- found in consumer fragrances have the po-
sensitive to scents in their work environments, ger. Various studies have tential to cause skin sen-
some to the point of opening WorkSafeBC shown adverse effects of
products also remains sitization, they lack the
claims. I’ve always advocated for my patients phthalates, such as en- a mystery due to ability to induce allergic
but have questioned the validity of such claims. docrine disruption, bone lack of research and sensitization of the respi-
The word perfume derives from the Latin mineral density decline, deficient regulation. ratory tract. They suggest
word perfumare meaning “to smoke through.” sperm dysfunction, and that it is possible for asth-
The art of making perfume began in ancient neurotoxicity even at the matics and other suscep-
Egypt and China and was refined by the Ro- perinatal level. Fragrances usually fall into the tible individuals to have an exacerbation of
mans and the Arabs. Apparently all public places category of synthetic musks. There are four main their respiratory symptoms when exposed to
in Britain were scented during Queen Elizabeth groups of synthetic musks, and the newer poly- fragrances, but this would be more in keeping
I’s rule (1558–1603) as she could not tolerate bad cyclic musks are the most popular, but there are with an irritant effect of high levels of expo-
smells. The first scented colognes were brought still questions about their safety, specifically sure to the causative agent coupled with the
to America by French explorers. As of 2019, the concerning estrogenic agonism and a possible higher sensitivity of the exposed individual.
global fragrance market was estimated to be increase in the proliferation rate of human They state that the key feature of a commer-
worth approximately US$38 billion—expected breast cancer cells. These compounds have also cially successful fragrance is that it stimulates
to rise to over US$50 billion by 2025. been shown to accumulate in the environment olfactory receptors at low concentrations and
Perfume is a mixture of fragrant essential and their biodegradability is questionable. The some individuals may link these olfactory
oils or aroma compounds, fixatives, and solvents authors summarized that while we have consid- triggers with adverse effects, including respi-
used to give the human body, animals, food, erable data on the role of fragrance compounds ratory responses. They were unable to find a
objects, and living space an agreeable scent. and their general toxicity, and more specifically causative explanation in terms of allergy or
There has been limited information available endocrine disruption, less is known about their irritation and suggested that a neurological/
about the safety of fragrance compounds as neurotoxicity. The extent to which these com- psychological mechanism may be involved.
the manufacturers are not required to—nor pounds are found in consumer products also They felt that it was unhelpful to heighten
to do they want to—elaborate on the ingre- remains a mystery due to lack of research and consumer fears by unwarranted conclusions
dients of fragrance mixtures, which are clas- deficient regulation. The authors recommend drawn from questionnaire studies with meth-
sified as trade secrets. The FDA controls the additional studies elucidating the neurotoxicity odological weaknesses.
safety of fragrances through their ingredients of fragrance compounds. I was unable to find any robust studies link-
and requires that they meet the designation The authors of an article in Clinical and Ex- ing exposure to fragrances with adverse health
of “generally recognized as safe” (GRAS). The perimental Allergy, “Increased release of hista- effects. I believe research still needs to be con-
International Fragrance Association is one of mine in patients with respiratory symptoms ducted in this area, especially to develop vali-
the governing bodies attempting to produce related to perfume,”2 concluded that perfume dated diagnostic toxicological tests to evaluate
guidelines with the aim of safe production and induces a dose-dependent non-IGE mediated fragrances.
44 BC Medical Journal vol. 62 no. 2 | march 2020
Editorials
Human nature in times of stress
A
And I’ve decided that I need to be sen- few months ago, I read something contagious and is already close to doubling
sible when it comes to wearing scents. I have about the severe acute respiratory the number of SARS cases. Also troubling,
stopped wearing perfume to work or in any syndrome (SARS) outbreak of 2003 and making screening more difficult, is the
situations that will involve close interactions and I remember thinking, it’s only a matter of virus’s apparent ability to transmit prior to an
with others. I’ll reserve being very irresistible time until something else strikes. In case you individual being symptomatic. I am reminded
for hot nights in the city. n think I have some prophetic power, I should of the Spanish flu outbreak in 1918 (no, I’m
—Jeevyn K. Chahal, MD state that I have never won a lottery prize. not that old), which had a lower mortality rate
As I write this editorial in early February, than SARS but by the sheer number of people
References the novel Wuhan coronavirus has been de- infected was responsible for millions of deaths.
1. Pinkas A, Gonçalves CL, Aschner M. Neurotoxicity of clared a world health emergency by the World By the time this editorial makes it to print,
fragrance compounds: A review. Environmental Re- Health Organization. At this point, there have the trajectory of the Wuhan coronavirus will
search 2017;158:342-349.
2. Elberling J, Skovw PS, Mosbech H, et al. Increased re-
been about 14 000 documented cases in 23 likely have been decided. The purpose of my
lease of histamine in patients with respiratory symp- countries with over 300 deaths, all but one in editorial is to reflect on human nature and
toms related to perfume. Clinical Experimental Allergy China. It remains unclear if this virus is des- the hope I have for compassion and grace. It
2007;37:1676-1680. tined to become a global pandemic or fizzle is easy to be a positive influence in the world
3. Basketter DA, Huggard J, Kimber I. Fragrance inha-
out in the months to come. when everything is going well. Sadly, I have
lation and adverse health effects: The question of
causation. Regulatory Toxicology Pharmacology Fortunately, this virus appears to be less found that true human nature is often dem-
2019;104:151-156. virulent then SARS, which had a death rate onstrated during times of stress and difficulty.
of roughly 10%. However, it is much more Sporadic reports of racism directed toward
the Asian community have already begun to
surface. Viruses don’t care about human skin
pigment or geographic origin. This virus could
have just as easily originated in a town or city
on any other continent.
I have fielded a few questions about this
novel virus in my office, and I can feel the fear
building among my patients. I remain hopeful
that despite the challenges this virus might
bring that the world will react with decency
“Go big,
WHEN IT COMES TO toward those less fortunate. Now don’t get me
wrong, I don’t want my family or friends to be
don’t go home!” TRAVEL INSURANCE, infected, and I’m not immune to the anxiety
this potential pandemic might bring, but I will
WE GO BIG. strive to focus on the caring our profession is
known for. Increasingly, we live in a closely
connected global society, so this situation af-
fects all of us. I will strive to do my part with
Call to get 1.855.473.8029 empathy and respect when faced with any
a quote Johnson.ca/doctorsofbc threats this virus might bring. May the world
do the same. n
—David Richardson, MD
Johnson Insurance is a tradename of Johnson Inc. (“JI”), a licensed insurance intermediary, and operates as Johnson
Insurance Services in British Columbia and Johnson Inc. in Manitoba. MEDOC® is a Registered Trademark of JI. This
insurance product is underwritten by Royal & Sun Alliance Insurance Company of Canada (“RSA”) and administered by
JI. JI and RSA share common ownership. Valid provincial or territorial health plan coverage required. Travel Assistance
provided by Global Excel Management Inc. The eligibility requirements, terms, conditions, limitations and exclusions
which apply to the described coverage are as set out in the policy. Policy wordings prevail.
BC Medical Journal vol. 62 no. 2 | march 2020 45
president’s comment
Amplifying value
“Don’t it always seem to go,
that you don’t know what you’ve got
’til it’s gone.” —Joni Mitchell
T
he practice of medicine is evolving the shop that changes your tires lead to devalu- or cater to the will of the individual seeking ac-
at a pace unimaginable in previous ation? Yes. In some communities, social media cess to maximal everything for every ailment?
times. As this evolution unfolds, we has been used to aggressively blame and shame Depends on who you talk to. Virtual episodic
need to take a hard look at the basic tenets of health care services in a way that is leading to care is much more likely to address the latter.
care that, as health care providers, we want to the societal distrust and devaluation of physi- Current funding models leave those physicians
keep and work diligently to maintain, while cians’ knowledge and skillsets. It is difficult to dedicated to longitudinal care struggling to keep
acknowledging that this likely means excluding remain dedicated in an often toxic environment. the lights on while striving to remain healthy
other diagnostics or treatments. We need to remind our communities that they and engaged.
Right now in BC the strongest movement truly “don’t know what you’ve got ’til it’s gone.” As I have traveled around the province lis-
afoot is team-based care. This model has been Amplifying the value that physicians bring tening to the needs of patients, physicians, and
shown to improve access, freeing up physicians to the health care system health care management
to deliver services that only they can deliver. is challenging for a num- groups, it has become ap-
We know longitudinal, community-based care ber of reasons. Patients As the practice of parent there are gaps—
reduces hospital and ER admissions, removes are constantly bombarded medicine evolves, gaps in understanding on
duplication of services, and saves the system with conflicting informa- both sides of the equation
money. While the power of longitudinal care tion about best practices,
funding for supports about how more innova-
lies in the core relationship between the pro- the latest technologies, or and payment model tive funding and payment
vider and the patient, we need to ensure the procedures from multiple options needs to models can enhance care
care coordination piece is well supported. It sources, including expand- keep pace. delivery. The current situa-
takes time to collaborate and build treatment ing global social media tion has been described as
plans across areas of practice to improve the and celebrity-driven dis- the Wild West. No single
patient’s journey and outcomes. That said, our cussion forums. Although patients want to payment model is perfect, or a fit for every phy-
metrics and models of payment are not devel- participate more actively in their own care, pro- sician, at every stage of their career, or even
oped enough to fully capture the value of this viders are often not allowed funded time to within the same section. Certain workflow ex-
type of care in terms of future costs avoided. have the related discussions—discussions that pectations may seem reasonable to physicians
The value-add evidence is not apparent to the ensure the care provided is the most appropri- or administrators, yet be untenable to others for
general population. ate, guideline-driven plan for each individual unforeseen reasons. Where there is a knowledge
Increased use of remote telemedicine or vir- patient. Neither party walks away from these gap, confabulation and presumption fill the void.
tual care has transformed the way patients may situations feeling well served. Rumor and unfounded assumptions abound.
seek and receive care. While remote access to As the practice of medicine evolves, funding For our health care processes to remain sus-
telemedicine makes sense for those who would for supports and payment model options needs tainable and meet the needs of patients, admin-
otherwise have to leave their community to seek to keep pace. These systems must reflect the istrators, and physicians, we need to listen to all
care, what happens as health care becomes more change in how patients want to receive care, and perspectives. We must work collaboratively to
consumer-led? Does access to medical services the way in which physicians deliver that care. build models of compensation and workload ex-
delivered from the phone in your pocket, at For instance, do we continue to value episodic pectations based on the shared understanding of
any time of day, devalue those providing the or procedural treatments above longitudinal the short-, medium-, and long-term vision for
long-term committed care? I would say yes. care when we know that episodic care drives care delivery in each region. We must establish
Does the ability to instantly rate or critique the use and costs? Do we continue to fund a uni- a shared responsibility for cost containment and
services you receive the same way you evaluate versal level of basic, evidence-driven medicine,
Continued on page 48
46 BC Medical Journal vol. 62 no. 2 | march 2020
Letters to the editor We welcome
original letters of less than 300 words; we may edit them for clarity
Re: The age of mushrooms is
upon us in medicine
and length. Letters may be emailed to journal@doctorsofbc.ca, submitted I was pleased to see the BCMJ publish Dr Mark
online at bcmj.org/submit-letter, or sent through the post and must include Elliott’s piece, “The age of mushrooms is upon
your mailing address, telephone number, and email address. Please disclose us in medicine.” Psychedelics such as LSD and
psilocybin showed great promise as investiga-
any competing interests.
tional tools and, in the case of LSD, as a treat-
ment for addiction, until politics and irrational
fears essentially ended all research into these
Re: The age of mushrooms is reading, this theory appears to have no credible agents for decades. Fortunately, this is chang-
evidence to support it and has actually been ing and a number of studies, as imperfect as
upon us in medicine they are, suggest that psychedelics, combined
Thank you to Dr Mark Elliot for his article heavily criticized by the scientific community.
The long-running stigma associated with with appropriate psychotherapy, may hold great
outlining the potential benefits of psychedelic promise in treating end-of-life anxiety, depres-
compounds now being studied in certain disci- these psychotropic compounds is in part a reac-
tion to the ardent promotion of pseudoscience sion, and addiction.
plines of medicine and cognitive therapy [BCMJ Dr Elliott incorrectly states that psychedel-
2019;61:390-391]. While our colleagues in car- by advocates such as Timothy Leary. If these
compounds are to be incorporated into main- ics “seem to affect serotonin and/or monoamine
diovascular medicine, oncology, and surgery oxidase (MAO) receptors in the brain.” MAO is
seem to have enjoyed significant advances in stream medicine, we owe it to our colleagues
and especially our patients to present accurate not a receptor but rather an enzyme that is widely
their respective fields, the same cannot be said of distributed throughout the body (including the
those involved in treating depression, addiction, findings and reject unsubstantiated claims. It is
critical that we separate the potential medicinal CNS). It is generally agreed that the actions
and PTSD, and those working in palliative care. of psychedelic agents are primarily mediated
We share Dr Elliot’s enthusiasm for the po- benefits of these compounds from the cultural
and societal biases with which they are often through agonism at the 5-HT2A receptor (a
tential benefits of these therapies, but also wish class of serotonin receptor) in the brain. I sus-
to issue a reminder that as we proceed with an associated.
—Chris Little, MD, FRCPC
pect that Dr Elliott was referring to ayahuasca,
open mind we should also remain highly criti- a plant-derived psychoactive brew containing
Penticton
cal. The medical community must not legitimize Banisteriopsis caapi and DMT containing vines
unfounded theories, and must ensure that any —Edward Brooks, MD, FRCPC
Victoria (such as Psychotria viridis or Acacia sp). B. caapi
future studies of these compounds abide by contains natural MAO inhibitors that may have
the scientific method and prioritize the safety some minor CNS effects but act primarily by
of our patients. Author replies
preventing metabolism of DMT in the gut. This
These promising therapies are sure to come I couldn’t agree more with your cautionary note. allows the DMT to be absorbed and to exert
under scrutiny by many, both inside and outside Paul Stamets seems to be an extraordinary my- its effects on the CNS.
the medical community. With this being said, cologist with dozens of patents to his name, but Thank you for publishing this otherwise
we question Dr Elliot’s mention of the Stoned with enough publicity people like him can easily excellent brief overview of the emerging field
Ape Theory first postulated by Terence Mc become gurus, which is not good. I mentioned of psychedelic medicine.
Kenna and more recently propagated by Paul the Stoned Ape (Stone Age in his original ar-
—Jeffrey Eppler, MD
Stamets on the popular podcast The Joe Rogan ticle) hypothesis only because it is an interest-
Kelowna
Experience. Mr Stamets, a mushroom enthusiast, ing theory. Whether one day some experiment
seems to have one foot in the field of mycol- will come up with an observation to back it up
ogy as a science and the other in the realm of is doubtful. This is a problem in many areas of
Author replies
unfounded and seemingly far-fetched theories. science dealing with fundamental issues. But Thanks for pointing out my error about mono-
The Stoned Ape Theory postulates that during as Karl Popper said, “All observation is theory amine oxidase being an enzyme rather than
human evolution our primitive ancestors con- laden,” which means nature (theory) proposes a receptor. As a practising anesthesiologist I
sumed mind-altering mushrooms, the effects and the environment (observation from experi- don’t pay as much attention to pharmacologi-
acting as an evolutionary catalyst, supposedly ment) disposes, which is just stealing another cal acronyms as I should. Psychedelics may be
responsible for the higher-level development well-known saying from genetics. We will see helpful for treating opioid addiction, but it will
of language, religion, and music. We, the au- where it leads. be a small percentage of patients who will be
thors of this letter, have no formal training in cured. Going this psychedelic route is worth a
—Mark Elliott, MD, FRCPC
mycology or anthropology, but from our brief Vancouver shot when you look at our failure with how we
BC Medical Journal vol. 62 no. 2 | march 2020 47
letters to the editor president’s comment
handle the problem now, whereby a drug user find anybody to take over his extremely large Continued from page 46
gets an unknown white powder, which could practice consisting mainly of older patients. access to appropriate, equitable, culturally safe,
be fentanyl or heroin at markedly different The only way I could not leave my own pa- timely care. The general population should be
LD50s, and that is 90% contaminants, which is tients in the lurch when I retired from my made aware of what services, on what time-
then shoved into the right side of the circula- practice was to move my charts and practice line, a publicly funded health care system can
tion with horrific vascular/septic results. If the to a clinic that was a hybrid walk-in family deliver so they can adjust their expectations.
drug was clean and the dosage known there practice, which took over all my charts so I If British Columbians and our govern-
would be very few of these patients showing could walk away. ing bodies are to maximally benefit from
up in the operating rooms, but this is a politi- I believe that action should have been the unique knowledge and skillsets physi-
cal, not a medical issue. taken over 20 years ago, which may have cians bring to the table, then payment mod-
Microdosed psychedelics might become prevented the crisis we find ourselves in to- els should universally incorporate time for
a standard anesthetic preoperative medica- day. Full-service longitudinal family practice teaching, multidisciplinary simulation train-
tion someday. needs to become more attractive. Many young ing, research, quality improvement endeavors,
—Mark Elliott, MD, FRCPC physicians do not relish the thought of run- evaluation, and participation in health care
Vancouver ning a small business, which means acquir- system management.
ing somewhere to develop a medical office, I believe that with ongoing open dialogue,
Doctor shortage employing staff, ordering supplies, and paying visioning, and collaboration, we can continue
The current family doctor shortage is a crisis. a mortgage or rent, just to mention some of to build a health care system that is sustainable
It is especially bad where I live, in Parksville the expenses involved. It appears that many and meets the needs of patients, care providers,
on Vancouver Island. Why has the situa- young physicians prefer to work under a dif- and administrators alike. We need commit-
tion become so dire? In my opinion, it has ferent model, such as a salaried system with ment on all sides of this shared responsibility
happened because of gross incompetence at good benefits, vacation time, and paid con- to bring this to life. n
multiple levels of the medical profession and tinuing medical education in a team-based —Kathleen Ross, MD
government. I am a retired family physician. model with nurses, social workers, and other Doctors of BC President
I am a UK graduate. I was in full-time fam- support workers under the same roof. This
ily practice in Alberta for 6 years and BC for model has been shown to be successful in
28 years before semi-retiring to Parksville in many parts of Canada.
2012, where I worked as a rural locum and The government and the profession must
urgent care physician part-time until I fully work harder to find ways to provide every citi- British Columbia
Medical Journal
retired from practice in 2016, aged 69, after zen access to a local family physician. It does @BCMedicalJournal
46 years of medical practice. As far back as the not appear that this is happening now. Clearly,
late 1980s and early 1990s, it was well known inadequate numbers of family physicians are
British Columbia Medical Journal
that the average age of family physicians in being trained, and the trained physicians are
@BCMedicalJournal
BC was in the 50s. It was becoming clear to not coming to places like Parksville or Qua-
licum. It is difficult for young physicians who New DNA “clock” could help measure development in
us practising family doctors that the family young children
practice model we were all working in was trained overseas to return to Canada, their
home, to practise here. Canada is not pro- Scientists have developed a molecular “clock” that
becoming less attractive to the next generation could reshape how pediatricians measure and monitor
of doctors, who were able to work in walk-in viding enough places in medical schools to
childhood growth and potentially allow for an earlier
clinics, where they could see large numbers maintain the supply of physicians that the diagnosis of life-altering developmental disorders.
of people with relatively minor complaints country requires, which is one of the reasons
Read the article: bcmj.org/news/new-dna-clock-could-
and would not have to become involved with many young Canadians go overseas for their
help-measure-development-young-children
older patients with more chronic complaints, medical education.
who require care on a more longitudinal basis. Parksville is experiencing a building boom,
Since then, the Medical Services Plan has and in a few years, there will be thousands
made changes to increase the payments for more people living here. Who is going to look
older patients with chronic conditions, which after all of us?
certainly helped, but none of the changes have —Jonathan M. Winner, MD
turned the tide to attract more young physi- Parksville
cians to enter full-time family practice. In the
mid-2000s one of my partners tragically died
Follow us on Facebook for regular updates
in his early 60s of cancer. We were unable to
48 BC Medical Journal vol. 62 no. 2 | march 2020
Help families Confident Parents: Thriving Kids - Anxiety
is a free program helping BC families
team up overcome anxiety challenges
in children ages 3–12.
against This web- and phone-based
coaching service helps parents
and caregivers learn effective skills
ANXIETY and strategies for managing anxiety.
It’s available by referral from physicians,
clinicians and pediatricians.
Download referral forms at
confidentparents.ca
BC Medical Journal vol. 62 no. 2 | march 2020 49
Clinical
Hilary Drake, BSc, Courtney Zimmerman, BTech, CPHI(C), Guy Osachoff, CPHI(C), Greg Baytalan,
BSc, CPHI(C), Muddassir Siddiqui, BDS, MPH, Gillian Frosst, BSc, MPH, Silvina C. Mema, MD, MSc,
FRCPC
Cluster of respiratory illness
in British Columbia linked to
poor air quality at an indoor
ice arena: A case report
An example of the importance of health care providers reporting
disease clusters to public health authorities.
ABSTRACT: In February 2019, a 56-year-old male matter had accumulated in the indoor ice arena. [Table] and performed a descriptive analysis
was admitted to Kelowna General Hospital with a Numerous contributing factors were identified, of data collected from interviews and medical
respiratory illness following recreational hockey including the use of older-model ice resurfacing records. In addition, the team conducted envi-
practice at an indoor ice arena. During his hospi- and edging equipment, the unseasonably cold ronmental inspections of the arena.
talization, he disclosed that several of his hockey outdoor weather conditions at the time, and the The Interior Health team learned that af-
teammates had similar respiratory symptoms. This failure of heating, ventilation, and air conditioning ter 16 players attended a hockey practice on 8
prompted the hospitalist physician to contact an equipment. This case report highlights the impor- February, 12 reported becoming ill (attack rate:
Interior Health medical health officer regarding a tance of health care providers reporting disease 75%). The team interviewed 11 of the 12 play-
potential cluster of respiratory illness. The inves- clusters to public health authorities, even when ers; 1 player was out of the country and could
tigation that was launched found toxic levels of the causative agent may not be reportable under not be reached. Of the 11 players interviewed,
carbon monoxide, nitrogen dioxide, and particulate the British Columbia Public Health Act. all were nonsmokers and none reported any
recreational drug use. The age range of those
Case data affected was 35 to 58 years (mean 52 years).
On 12 February 2019, a hospitalist physician at The most commonly reported symptoms
Ms Drake is a medical student at
the Kelowna General Hospital contacted the were shortness of breath (91%), followed by
the University of British Columbia. Ms
Interior Health on-call medical health officer cough (64%) and hemoptysis (36%). Of the 11
Zimmerman is director of environmental
(MHO) to report a cluster of respiratory ill- individuals interviewed, 5 (45%) sought medical
public health at Interior Health. Mr
ness.1 A 56-year-old male had been admitted care and 4 (36%) obtained chest X-rays within
Osachoff is an environmental health
to hospital with acute respiratory distress on 9 24 to 72 hours from the onset of symptoms. Of
officer at Interior Health. Mr Baytalan is
February after playing hockey on 8 February at the individuals who obtained chest X-rays, 3
a specialist environmental health officer
an indoor ice arena. While recovering in hos- (75%), including the patient in the index case,
at Interior Health. Mr Siddiqui is a public
pital, the patient disclosed that several fellow had a hazy lung lesion of increased density,
health epidemiologist at Interior Health.
players had developed respiratory illness with which the radiologist reported as a patchy
Ms Frosst is manager of the epidemiology
similar symptoms on 8 and 9 February. ground-glass nodularity in pulmonary airspace.
and surveillance unit at Interior Health.
A cluster investigation team was struck im- The patient in the index case was the only
Dr Mema is a medical health officer at
mediately to determine if the players had been player to require hospitalization, with an initial
Interior Health and a clinical assistant
exposed to a disease-causing agent. The team presumptive diagnosis of community-acquired
professor in the School of Population and
was led by an Interior Health MHO and in- atypical pneumonia. The patient’s blood cell
Public Health at the University of British
cluded three environmental health officers, a count was normal and his chest X-ray showed
Columbia.
communicable disease specialist, and an epide- patchy multifocal airspace disease most
miologist. The team developed case definitions prominently involving the upper lung zones
This article has been peer reviewed.
50 BC Medical Journal vol. 62 no. 2 | march 2020Drake H, Zimmerman C, Osachoff G, Baytalan G, Siddiqui M, Frosst G, Mema SC Clinical
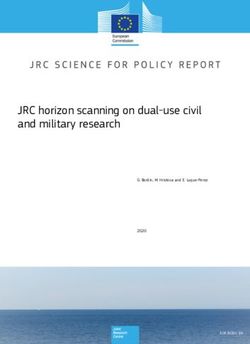
bilaterally. Follow-up chest X-rays showed rapid Table. Case definitions.
and significant improvement, and the patient
was fully recovered by the time of discharge Confirmed Any person present at the indoor ice arena and surrounding area on 8 February 2019
on 13 February. Nasopharyngeal swabs were case experiencing respiratory illness symptoms on or after that date:
• New or worsening cough
negative for influenza and respiratory syncytial
and
virus. Multiplex nucleic acid testing (NAT)
• Additional respiratory illness symptoms (may include shortness of breath, hemoptysis,
was negative for viruses and bacteria. Sputum
dizziness, headache, and/or fever)
culture was negative for tuberculosis after a
and
6-week incubation.
• Abnormal chest X-ray results
An inspection of the arena building and
ice rink on 12 February found a number of is- Probable Any person present at the indoor ice arena and surrounding area on 8 February 2019
sues. The ice resurfacing machine was in poor case experiencing respiratory illness symptoms on or after that date:
repair, the HVAC (heating, ventilation, and air • New or worsening cough
conditioning) system was malfunctioning, and and/or
two rooftop fans for the furnace and make-up • Additional respiratory illness symptoms (may include shortness of breath, hemoptysis,
dizziness, headache, and/or fever)
air were not working. Data from real-time air
quality monitors were not available. The West
Kelowna Fire Department and Fortis BC also
inspected the arena on the evening of 12 Feb-
ruary and at the time of their inspection were edging machines. Ice resurfacing machines or produces a variety of symptoms, including
unable to detect any noxious gases. Howev- resurfacers are primarily fossil-fueled vehicles headache, malaise, nausea/vomiting, and dizzi-
er, subsequent air monitoring on 4 March by for maintaining the entire ice surface and are ness.10,11 Signs and symptoms of nitrogen diox-
Technical Safety BC (previously BC Safety commonly referred to as Zambonis, regard- ide poisoning are primarily respiratory related,
Authority) identified levels of carbon monox- less of brand or manufacturer. Ice resurfacers including cough, hemoptysis, throat irritation,
ide (CO) well above the safety threshold, par- are used together with ice edgers, which shave dyspnea, and chest pain.4,6,12,13
ticularly near the ice surface where a four-cycle and level the edge of the ice rink near the sur- Indoor ice rinks are used most commonly
gasoline-powered edging machine was operat- rounding boards. Edging usually takes place for hockey, ringette, figure skating, and general
ing in idle mode. once daily or every other day and is typically recreation.3 During these exercise-related ac-
Arena staff reported that on 8 February sig- followed by ice resurfacing; however, ice resur- tivities, participants increase their respiratory
nificant ice maintenance had been conducted facing can take place independently of edging rate and risk inhaling more toxic gases and
from 8:15 a.m. to 2:00 p.m., with the ice resur- and is commonly done more frequently—as particulate matter, if present.4 Compared with
facing machine operating for about 3.5 hours. often as every hour.2 carbon monoxide uptake at rest, carbon mon-
A gasoline-powered ice edging machine was oxide uptake during exercise can increase up
also used at this time. Rink operators recalled Air pollutants to 400%.14 Furthermore, individuals exercising
that on 8 February the weather was unusually Older models of ice maintenance equipment on an ice rink are near the cold ice surface
cold for the Central Okanagan at -21 °C, which operate using an internal combustion engine where less-effective mixing of combustion
led to the bay door for the ice resurfacing ma- fueled by either propane or gasoline, which can emissions occurs with the warmer air above.15
chine being closed during maintenance on this produce high levels of air pollutants, includ- This puts athletes or recreational users at the
particular day. None of the staff members who ing carbon monoxide, nitrogen dioxide (NO2), highest risk for toxic exposure.3,4,6,9 Those
worked that day had respiratory symptoms. Of and ultrafine/fine particulate matter.3-5 Studies especially at risk for developing complica-
interest, the first player to arrive at the arena comparing outside air with air inside arenas tions from inhaling CO, NO2, and particulate
on 8 February noted that he saw a yellow haze that use ice resurfacing machines powered by matter are children, pregnant women, and
on the surface of the ice and around the ceiling fossil fuels have found a 60-fold to 300-fold individuals with pre-existing cardiovascular
lights. None of the other players interviewed increase in CO, a 10-fold increase in NO2, and or respiratory conditions such as congestive
reported seeing this haze. a 20-fold increase in small particulate matter.6-8 heart failure or asthma.8,9
These contaminants can result in significant
Discussion health risks.5 Factors influencing pollutant levels
Poor indoor air quality at indoor ice arenas is High concentrations of CO and NO2 have The construction of the indoor ice arena can
known to be a source of health complaints.2-9 been found in individuals who spend time influence pollutant levels. Arenas with poor
Ice rinks at indoor facilities are typically in indoor ice arenas, including workers and ventilation, including inadequate natural venti-
cleaned and smoothed by ice resurfacing and hockey players.4,8,9 Carbon monoxide poisoning lation or inadequate mechanical ventilation, as
BC Medical Journal vol. 62 no. 2 | march 2020 51Clinical Cluster of respiratory illness in British Columbia linked to poor air quality at an indoor ice arena
well as arenas with mechanical failure of exist- As well, the machines should be stored in a a chemical exposure as the most plausible cause,
ing ventilation systems, have increased levels of well-ventilated part of the arena with direct allowing the MHO to make recommendations
ambient CO and NO2.16 Furthermore, the size access to the outdoors or an exhaust hose to to mitigate the ongoing risk at the arena.
of an arena can influence pollutant levels, with extract and redirect the fumes outside. While suspected food or waterborne ill-
smaller arenas having higher NO2 levels than nesses or clusters of gastrointestinal illness are
larger arenas.17 Ice surfaces used for hockey have Monitoring reportable in BC, there is no requirement to re-
boards taller than many young skaters, thereby The incident described in this case report high- port illnesses with causes other than those listed
trapping the heavier-than-air NO2 within this lights the importance of real-time air quality in the regulation as “prescribed” infectious or
cooler dense air environment above the ice sur- monitoring in indoor ice arenas and the need hazardous agents. Therefore, a health care pro-
face at the inhalation height of many youths. to follow administrative vider could be dealing with
Far worse consequences could have resulted if protocols such as proper a significant illness cluster,
children rather than adult males had entered ventilation maintenance. Far worse consequences such as the one we investi-
the ice surface immediately after this prolonged While monitoring com- gated, yet not be required
could have resulted
ice maintenance activity. pliance with safety stan- to report to the MHO. In
In this particular cluster of respiratory ill- dards at indoor ice arenas if children rather contrast, the Alberta Pub-
ness, a number of factors likely contributed to is the shared responsi than adult males had lic Health Act (Section 26
poor air quality. Doors closed because of un- bility of employers, local entered the ice surface Notification of epidemics
seasonably cold weather conditions, prolonged governments, and Work- immediately after and other threats) requires
ice maintenance, and HVAC equipment failure SafeBC, a national or
18
that any disease occurring
created the perfect storm opportunity for toxic provincial guideline on
this prolonged ice in epidemic form or at an
levels of CO, NO2, and particulate matter to acceptable levels of CO maintenance activity. unusually high rate, or any
accumulate indoors. The higher respiratory rate and NO2, including pro- illness suspected to pose a
of players during exercise increased their expo- tocols to mitigate toxic public health threat, be re-
sure to pollutants over that of staff who did not gas levels, could help maintain public safety. ported to an MHO.21 Furthermore, in Alberta,
report symptoms.14 Of note, during the winter of 2020–21, Health reporting requirements extend beyond health
Carbon monoxide and nitrogen dioxide Canada will be testing the efficacy of two in- care workers to teachers and persons in charge
emissions result when fossil-fuel-powered terventions on air quality at indoor ice arenas, of an institution.
engines are used.3-5 Ways to prevent or mini- one in Ontario and one in Saskatchewan.19 This indoor ice arena incident highlights the
mize emissions include decreasing the time a The impact of fuel type on CO and NO2 con- benefit of front-line health care professionals
fossil-fuel-powered ice resurfacing machine is centrations will be assessed and the efficacy of collaborating with public health officials, and
in operation indoors,4 ensuring adequate ven- various ventilation strategies on CO and NO2 the importance of encouraging health care pro-
tilation to prevent buildup of toxic gas, and concentrations will be quantified. The impact viders to report unusual events with possible
transitioning to electric ice resurfacing ma- of other factors on indoor air quality will also public health implications. Efforts are under-
chines, although this last strategy can be cost be studied, such as arena volume, number of ice way to amend BC’s regulation using language
prohibitive. Other solutions include manually resurfacings, temperature, and relative humidity. similar to Alberta’s to require more inclusive
running the ventilation system longer, opening reporting.
doors during resurfacing, and ensuring that Reporting
the ventilation system is working properly. In- The case study described here illustrates the Summary
terestingly, shortly after the incident, the two importance of promptly reporting clusters of Several factors, including doors being closed
(and only) ceiling exhaust fans were repaired respiratory illness to an MHO. The BC Public due to cold weather, prolonged ice maintenance,
and deemed to be functioning properly. How- Health Act (Section 10, Mandatory reporting of and HVAC equipment failure, led to a build-
ever, many months later it was discovered that infection or exposure) requires that health care up of toxic gases in an indoor ice arena. This
the air ducts had been intentionally blocked, providers notify an MHO if they have reason caused 12 previously healthy adults to report
most likely for energy conservation purposes. to believe a patient is infected with a reportable respiratory symptoms. The treating physician
Therefore, the fans were not performing their communicable disease.20 This includes suspected contacted an Interior Health MHO about a
designed task until the blockages were removed. food or waterborne illnesses as well as clusters possible respiratory illness cluster, which led to
Studies show that CO levels are highest dur- of gastrointestinal illness, as detailed in the Re- a prompt investigation, despite this reporting
ing the use of an ice resurfacer and immediately porting Information Affecting Public Health not being mandated by the current BC Public
afterwards,5 suggesting that arenas should use Regulation. While a communicable disease was Health Act. The success of the investigation
the ventilation system throughout the proce- initially suspected in the index case, a prompt highlights the importance of including illness
dure and after resurfacing has been completed. and thorough cluster investigation pinpointed clusters in the reporting guidelines for health
52 BC Medical Journal vol. 62 no. 2 | march 2020Drake H, Zimmerman C, Osachoff G, Baytalan G, Siddiqui M, Frosst G, Mema SC Clinical
personnel. In addition, as public health orga- 2. Cox A, Sleeth D, Handy R, Alaves V. Characterization 12. Rosenlund M, Bluhm G. Health effects resulting from
nizations continue to promote healthy life- of CO and NO2 exposures of ice skating rink mainte- nitrogen dioxide exposure in an indoor ice arena. Arch
nance workers. J Occup Environ Hyg 2019;16:101-108. Environ Health 1999;54:52-57.
styles, including regular exercise, the buildings 3. Brauer M, Lee K, Spengler J, et al. Nitrogen dioxide in 13. Soparkar G, Mayers I, Edouard L, Hoeppner V. Toxic ef-
in which these activities take place need to be indoor ice skating facilities: An international survey. J fects from nitrogen dioxide in ice-skating arenas. CMAJ
monitored to ensure public safety. It is antici- Air Waste Manag Assoc 1997;47:1095-1102. 1993;148:1181-1182.
pated that Health Canada’s research in this 4. Rundell K. Pulmonary function decay in women ice 14. Forbes W, Sargent F, Roughton F. The rate of car-
hockey players: Is there a relationship to ice rink air bon monoxide uptake by normal men. American J
area will eventually inform the development quality? Inhal Toxicol 2004;16:117-123. Physiology-Legacy Content 1945;143:594-608.
of a document detailing national best practices, 5. Lee K, Yanagisawa Y, Spengler J, Nakai S. Carbon mon- 15. Brauer M, Spengler JD. Nitrogen dioxide exposures in-
monitoring, and response guidance for facility/ oxide and nitrogen dioxide exposures in indoor ice side ice skating rinks. Am J Pub Health 1994;84:429-433.
arena managers and public health professionals skating rinks. J Sports Sci 1994;12:279-283. 16. Pelham T, Holt LE, Moss MA. Exposure to carbon mon-
6. Guo H, Lee S, Chan L. Indoor air quality in ice skating oxide and nitrogen dioxide in enclosed ice arenas. Oc-
to reduce human health impacts. n
rinks in Hong Kong. Environ Res 2004;94:327-335. cup Environ Med 2002;59:224-233.
7. Rundell K. High levels of airborne ultrafine and fine 17. Miller RK, Ryan MC, Bilowus P. Carbon monox-
Acknowledgments particulate matter in indoor ice arenas. Inhal Toxicol ide poisoning in indoor ice skating arenas. Va Med
The authors would like to acknowledge Dr Jan 2003;15:237-250. 1989;116:74-76.
8. Spengler J, Stone K, Lilley F. High carbon monoxide 18 WorkSafeBC. Carbon monoxide. Accessed 17 Janu-
Jacobus Steyn Naude, Dr Trevor Corneil, and Ms
levels measured in enclosed skating rinks. J Air Pollut ary 2020. www.worksafebc.com/en/health-safety/
Nicole Lougheed for their contributions to the Control Assoc 1978;28:776-779. hazards-exposures/carbon-monoxide.
investigation of the case described and the devel- 9. Lévesque B, Dewailly E, Lavoie, et al. Carbon mon- 19. Wilson A. Air quality in ice arenas working group. Pre-
opment of this case report. oxide in indoor ice skating rinks: Evaluation of ab- sented at the Canadian Institute of Public Health In-
sorption by adult hockey players. Am J Public Health spectors (CIPHI0) Annual Education Conference, Halifax,
1990;80:594-598. NS, 11 September 2019.
Competing interests 10. Tomaszewski C. Carbon monoxide poisoning. Early 20. Province of British Columbia. Public Health Act. 2008.
None declared. awareness and intervention can save lives. Postgrad Accessed 17 January 2020. www.bclaws.ca/civix/
Med 1999;105:39-50. document/id/complete/statreg/08028_01#section10.
References 11. Raub J. Environmental health criteria 213: Carbon mon- 21. Province of Alberta. Public Health Act. 2000. Accessed
1. Seymour R. Hockey players accidentally gassed at oxide (second edition). Geneva: World Health Organi- 17 January 2020. www.qp.alberta.ca/documents/Acts/
game? The Daily Courier. 22 Feb 2019. www.kelowna zation; 1999. Accessed 17 January 2020. www.who.int/ P37.pdf.
dailycourier.ca/news/article_cc6d406c-3729-11e9 ipcs/publications/ehc/ehc_213/en.
-914b-b3120f5ed680.html.
BC Medical Journal vol. 62 no. 2 | march 2020 53Clinical
Matthew Boroditsky, BHSc, Rebecca Courtemanche, MSc, Douglas Courtemanche, MD, MS, FRCSC,
Sandra Robertson, BSN, RN, Christine Loock, MD, FRCPC
Taking steps to improve care
and planning for patients in
British Columbia with 22q11.2
deletion syndrome
No data, no problem, no action! Better institutional and provincial
data sharing is needed to ensure evidence-based recommendations
for the condition known as 22q11DS or DiGeorge syndrome can be
developed, implemented, and updated.
ABSTRACT Columbia required by individuals with 22q11DS, vices, with 13 new patients being seen each year
Background: Patients diagnosed with 22q11.2 we set out to determine which health care services and followed for an average of 7 years. Most of the
deletion syndrome, also known as 22q11DS or these patients access and what barriers in health pediatric care was provided by the Cleft Palate/
DiGeorge syndrome, have a diverse array of con- informatics affect institutional and provincial data Craniofacial Program, Cardiology, Endocrinology,
genital anomalies and chronic health conditions. sharing. and Otolaryngology. Using BC Women’s Hospital
Because no study has reported on the coordina- Medical Genetics 22q11DS data (n = 400), we were
tion of multidisciplinary health services in British Methods: A retrospective review of patient care able to corroborate the size of our study cohort
at BC Children’s Hospital (BCCH) was conducted and to estimate the prevalence of 22q11DS in BC
using the provincial discharge abstract database for the study period.
Mr Boroditsky is a student in the Faculty and databases from hospital specialty services
of Medicine at the University of British involved in the care of patients with 22q11DS. Data Conclusions: Barriers to data retrieval and sharing
Columbia. Ms Courtemanche is a clinical were collected for patients seen at the hospital at institutional and provincial levels were found to
research coordinator for pediatric from April 2001 to March 2018. This 17-year review limit care coordination for patients with 22q11DS,
plastic surgery in the Department of considered patient age at diagnosis, distribution who require ongoing, complex, multidisciplinary
Surgery at UBC. Dr Courtemanche is of patient ages within the study cohort, number management. Incongruent and incomplete data
a clinical professor in the Division of and type of specialty services accessed, and length systems in BC are hindering our ability to provide
Plastic Surgery at UBC and performs of follow-up. this coordinated care and plan transition, leav-
surgery for the BC Children’s Hospital ing us without the evidence needed by provincial
Cleft Palate/Craniofacial Program. Ms Results: A total of 293 patients with 22q11DS were health care providers, local experts, policymakers,
Robertson is nurse clinician/coordinator identified from the hospital discharge abstract and national and international 22q11DS research
of the BC Children’s Hospital Cleft Palate/ databases (DAD) and seven BCCH specialty clinic centres.
Craniofacial Program. Dr Loock is an databases. Data could not be retrieved from some
associate professor in the Department of clinic databases due to coding and reporting dis- Background
Pediatrics at UBC and medical director crepancies, which prevented the amalgamation of In 1965 Dr Angelo DiGeorge first described
of the Cleft Palate/Craniofacial Program data from all hospital specialty services. Data from the syndromic presentation of infants with thy-
and Social Pediatrics RICHER Initiative the DAD and seven BC Children’s Hospital specialty mic aplasia, hypoparathyroidism, and cardiac
(Responsive Intersectoral Children’s services were then amalgamated, and duplicates outflow tract anomalies.1,2 DiGeorge syndrome
Health, Education, and Research). were removed to identify 293 unique patients with was later grouped with other phenotypically
22q11DS. On average, patients accessed five ser- similar syndromes seen in clinical practice (e.g.,
This article has been peer reviewed.
54 BC Medical Journal vol. 62 no. 2 | march 2020You can also read