Retrograde intussusception post-total gastrectomy and small bowel resection with Roux-en-Y gastric bypass
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Int J Case Rep Images 2019;10:101022Z01TC2019. Chuang et al. 1
www.ijcasereportsandimages.com
CASE REPORT PEER REVIEWED | OPEN ACCESS
Retrograde intussusception post-total gastrectomy and
small bowel resection with Roux-en-Y gastric bypass
reconstruction
Tzu-Yi (Arron) Chuang, Mustafa Sher, Damian Fry,
Marissa Stilianos, Chung-Kwun Won
ABSTRACT How to cite this article
Intussusception is a rare cause of intestinal Chuang TYA, Sher M, Fry D, Stilianos M, Won CK.
obstruction, especially in adult populations. Retrograde intussusception post-total gastrectomy
Adult intussusception was traditionally thought and small bowel resection with Roux-en-Y gastric
to occur secondary to a pathological lead point bypass reconstruction. Int J Case Rep Images
such as a malignancy, inflammatory bowel 2019;10:101022Z01TC2019.
disease, or anatomic abnormality; for example,
a Meckel’s diverticulum. Intussusception is
a rare surgical complication post Roux-en-Y
Article ID: 101022Z01TC2019
gastric bypass. An increase in incidence is
found with increasing demand of bariatric
surgeries. The exact cause of intussusception is *********
unclear. We present a 86-year-old female with
retrograde small bowel intussusception post- doi: 10.5348/101022Z01TC2019CR
total gastrectomy and small bowel resection
with Roux-en-Y reconstruction.
Keywords: Gastrectomy, Retrograde intussus- INTRODUCTION
ception, Roux-en-Y gastric bypass
Intussusception occurs when a part of the bowel
telescopes into itself, leading to obstruction. The
telescoping segment often pulls the mesenteric vessels
Tzu-Yi (Arron) Chuang1, Mustafa Sher2, Damian Fry3,
Marissa Stilianos4, Chung-Kwun Won5 with it causing ischemic pain and effacement of the
draining veins. Sequelae of intussusception can include
Affiliations: 1General Surgical Principle House Officer, Depart-
bowel obstruction or bowel ischaemia. Intussusception
ment of General Surgery, QEII Hospital, Brisbane, Queens-
land, Australia; 2Medical Student, School of Medicine, Univer- is a rare complication after Roux-en-Y gastric bypass
sity of Queensland, Brisbane, Queensland, Australia; 3General (RYGB) and extremely rare after total gastrectomy [1].
Surgical Fellow, Department of General Surgery,QEII Hospi- We present a case report of 86-year-old female with
tal, Brisbane, Queensland, Australia; 4General Surgical Regis- retrograde small bowel intussusception post-total
trar, Department of General Surgery, QEII Hospital, Brisbane, gastrectomy and small bowel resection with Roux-en-Y
Queensland, Australia; 5General and upper gastrointestinal reconstruction.
Surgical Consultant, Department of General Surgery, QEII
Hospital, Brisbane, Queensland, Australia.
Corresponding Author: Dr. Tzu-Yi (Arron) Chuang, General CASE REPORT
Surgical Principle House Officer, Department of General
Surgery, QEII Hospital, Brisbane, Queensland, Australia; A 86-year-old lady presented to emergency
Email: thomas0227@hotmail.com department with three weeks history of worsening
generalised abdominal pain, increasing frequency
Received: 12 February 2019 of bowel motions and nausea. She denied signs of
Accepted: 26 February 2019 upper gastrointestinal bleeding, such as melena and
Published: 24 April 2019 haematemesis. Her past medical history included
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198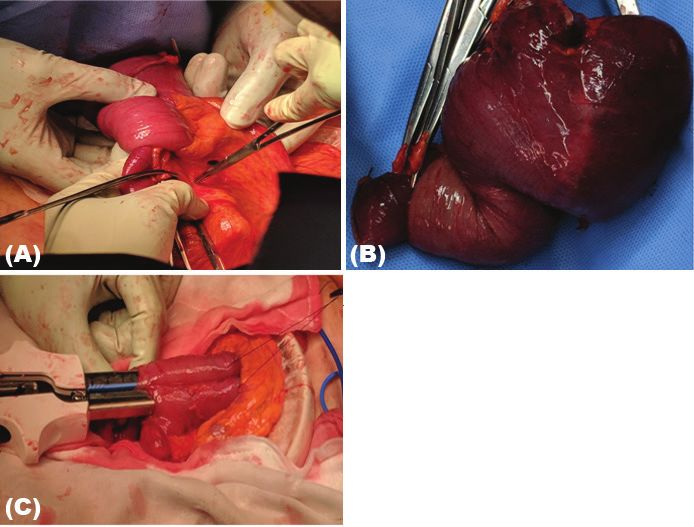
Int J Case Rep Images 2019;10:101022Z01TC2019. Chuang et al. 2
www.ijcasereportsandimages.com
total gastrectomy and small bowel resection with Roux
and Y bypass reconstruction for a bleeding foveolar
gastric adenoma, a rare form of Gastro-Intestinal
Stromal Tumour (GIST) 6 years ago. Her other medical
history included previous transient ischaemic accident,
ischemic heart disease, dyslipidaemia, hypertension,
knee replacements and pelvic organ prolapse requiring
a pessary. On presentation, her vital signs were all
within normal range. Her abdomen was soft and tender
over the central area. She had no rebound tenderness
or signs of peritonism or distension. Her biochemical
tests were unremarkable with normal white cell count,
haemoglobin, kidney function, and liver function tests.
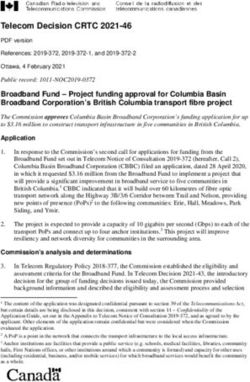
Computed tomography scan (CT) of the abdomen and
pelvis revealed small bowel intussusception around the
anastomosis site from previous surgery at the level of the
umbilicus; however could not identify any obvious leading
mass. There was no significant distension above or below
the intussusception and no significant distension of a
Roux loop was found (Figure 1).
She was admitted under a general surgical team Figure 1(A–C): Demonstrate the small bowel intussusception in
CT abdomen/pelvis with 3 respective views, ie, (A) Axial view
with appropriate fluid resuscitation, strict fluid balance,
(B) Coronal view (C) Sagittal view.
nasogastric tube insertion, pain relief, and in dwelling
urinary catheter insertion. Emergency surgery was
conducted the next day. Intra-operatively, laparoscopy
was performed, and a retrograde intussusception of
the common channel of Roux-En-Y was identified.The
decision was made to convert to open surgery with an
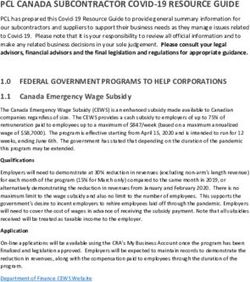
upper midline laparotomy. Approximately 15 centimetres
of distal small bowel had telescoped in a retrograde
fashion toward the anastomosis (Figure 2). No lead point
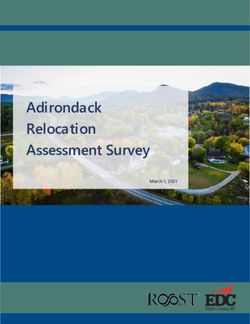
or retrograde peristalsis could be identified. Her anatomy
of Roux-En-Y reconstruction was unusual compared to
other total gastrectomies with Roux-En-Y reconstruction
because she also had small bowel resection at the
proximal jejunum for the bleeding of small bowel lesion
(Figure 3). Manual reduction of the intussusception was
not attempted in the patient.
The resection was conducted at all three limbs; from
proximal alimentary limb, biliopancreatic limb, and
Figure 2: (A) Shows the intra-operative finding of retrograde
the common channel distal to the intussusception, as intussusception distal to Y anastomosis; (B) Demonstrates
illustrated in Figure 3. The resections were conducted the resected intussusception with evidence of side-to-side
using a COVIDEN Endo GIA 80 mm x 3.8 mm linear anastomosis; (C) Demonstrates the side to side anastomosis
stapler. The stapler was also used to make a side-to- with stapler approach.
side isoperistaltic jejuno-jejunal anastomosis between
the proximal (oesophageal) limb and previous common
channel. The side-to-side anastomosis between the DISCUSSION
bilio-pancreatic limb and the common channel was
also conducted using staplers. The mesenteric window Adult intussusception is uncommon, making up only
was closed using 3’0 PDS. Her histopathological result 5% of total cases of intussusception and accounting for
showed ischemic necrosis of small bowel without any 1-5% of adult intestinal bowel obstructions [2]. Tumours
sign of recurrence of GIST. Post operatively, she was cause the majority of adult intussusception (benign
admitted to intensive care for two days. Her nasogastric 25% and malignant 27.3%) [3]. Other causes include
tube output was minimal and was removed on fourth day. inflammatory bowel disease and anatomic abnormalities,
She recovered well post-operatively and began tolerating such as a Meckel’s diverticulum or a mobile caecum
a free fluid diet on seven day. [4]. Intussusception after RYGB is a rare cause of
intussusception, with increasing incidence [3, 5,6].
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198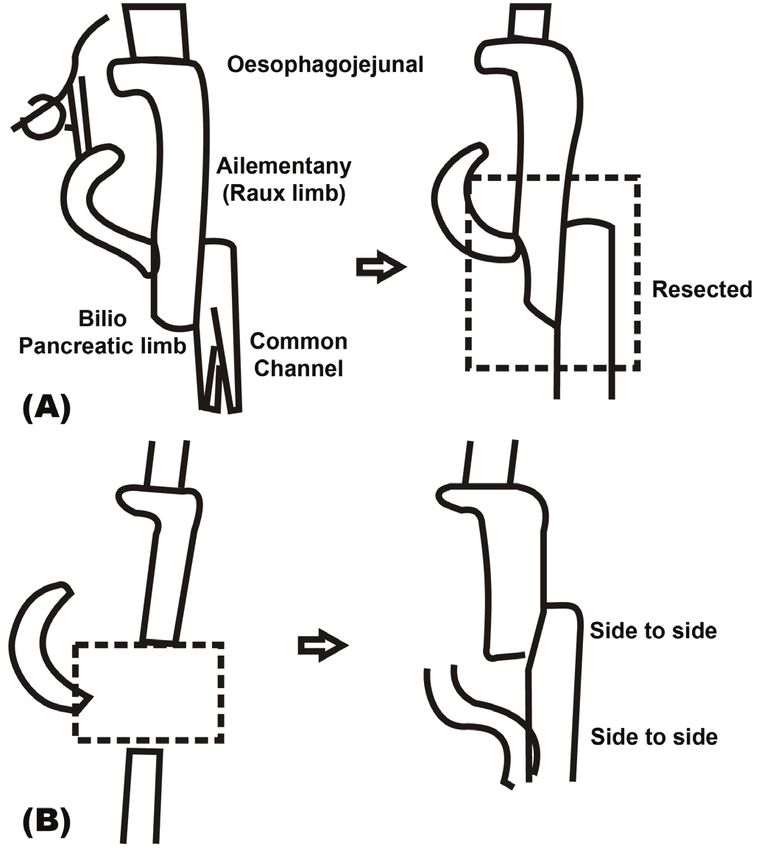
Int J Case Rep Images 2019;10:101022Z01TC2019. Chuang et al. 3
www.ijcasereportsandimages.com
surgery. Dr. Edward E Mason and Dr. Chikashi Ito were
the first to report using RYGB for weight loss surgery
in 1965 [9]. It was noted that approximately 20% of
complications occurred after RYGB [9]. Intussusception
is certainly a rare complication. The incidence of
retrograde intussusception has been reported as 0.07
to 0.6 % in RYGBs [5]. Jejunal intussusception after
gastrectomy was first reported by Bozzi et. al (1914) [9].
It is an uncommon complication affecting approximately
0.07-2.1% of patients who undergo gastrectomy [1].
Some authors have estimated intussusception to be a
cause of 10.8% of small bowel obstructions post RYGB
[8]. Given the rapid increase in the rate of bariatric
surgery, intussusception is becoming an increasingly
prevalent post-op complication, despite its rare incidence
post-RYGB [4].
Singla et. al (2012) reports that females make up
the overwhelming majority (92-98.6%) of patients to
suffer from intussusception after laparoscopic gastric
bypass surgery [5, 9, 13]. Singla et. al (2012) also found
the median patient age to be around 35 [5, 9, 13]. The
identified risk factors for developing intussusception
include female gender [5], younger age, and significant
weight loss after surgery [9].
Figure 3: A illustrates the Roux-En-Y reconstruction on Adult intussusception is usually treated by resection,
the left of diagram and the diagram on the right in (A)
as it is normally caused by a known lead point. However,
Demonstrates the area of small bowel resection in this
operation. (B) Demonstrates the method of re-anastomosis
in intussusception post- RYGB there is not usually a lead
in this operation. point. Currently, there is no consensus on definitive
treatment for intussusception post-RYGB. Manual
reduction with or without plication/pexy procedure has
been described in many previous studies [4, 5, 8]. It
A prompt diagnosis of intussusception is essential
was recommended that resection should be conducted
as it may lead to obstruction and bowel necrosis [7].
when there are signs of bowel necrosis. It was also found
Intussusception is often difficult to diagnose because of
that resection has statistically lower recurrence rates
its variable gastrointestinal symptoms and presentation.
compared to manual reduction (7.7% versus 31.5%) [9].
Common symptoms include non-specific abdominal
Kitasato et al. (2016) conducted a literature review
pain, nausea and vomiting and occasionally symptoms of
on intussusception post gastrectomy with RYGB
bowel obstruction, such as constipation or altered bowel
reconstruction [1]. It found 18 cases of intussusception
habits [8]. Symptoms may vary in acuity and severity
after total gastrectomy with Roux-en-Y reconstruction.
[5]. Stephenson et al. (2014) conducted a retrospective
Most patients were aged 60-70 years old. Only four cases
review of laparoscopic RYGB patients, finding that
were antegrade intussusception and rest were retrograde
91.7% of intussuscepted patients presented with upper
intussusception. There were six cases from the early
quadrant abdominal pain as a chief complaint and 8.3%
post-operative period, with the rest occurring between
presented with persistent nausea and vomiting [7]. The
1-22 years. Out of 18 cases, 12 had manual reduction and
abdominal examination may be non-specific. Only about
6 had bowel resection. It was found that recurrence was
10% of patients in the study presented with a palpable
more likely when only manual reduction was performed.
mass [9].
Kitasato believed Y leg side-to-side anastomosis in the case
Imaging is the tool of choice in diagnosing
of gastrectomy may prevent retrograde intussusception
intussusception. Radiological studies which have been
[1].
found to be useful include abdominal ultrasound, plain
In our case, the initial gastrectomy for this patient six
abdominal films, upper gastrointestinal contrast series,
years earlier was performed as part of emergency surgery
barium enema or CT abdomen/pelvis. Abdominal CT is
for gastrointestinal bleeding and gastric cancer. A separate
considered the most sensitive, reliable and useful way of
bleeding exophytic lesion was found in the proximal
diagnosing intussusception with a reported accuracy of
jejunum intra-operatively and was resected separately.
58–100% [10]. MRI abdomen/pelvis is recommended in
The proximal jejunum was resected to fashion a retrocolic
pregnant women to limit radiation exposure [11, 12].
roux loop with a 5 cm pouch at the proximal end which
Roux-En-Y bypass is performed for a variety of
was stapled to the oesophageal stump; the opposite end
indications and increasing commonly as part of bariatric
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:101022Z01TC2019. Chuang et al. 4
www.ijcasereportsandimages.com
was stapled side-to-side with the distal jejunum (common REFERENCES
channel) forming a jejuno-jejunostomy. The duodenal
stump was oversewn and attached side-to-side with the 1. Kitasato Y, Midorikawa R, Uchino Y, et al. A case of
common channel. The unique anatomy sets this case retrograde intussusception at Roux-en-Y anastomosis
apart from the 20 other reported cases of intussusception 10 years after total gastrectomy: Review of the
after total gastrectomy with roux-en-y reconstruction [1, literature. Surg Case Rep 2016;2(1):123.
2. Valentini V, Buquicchio GL, Galluzzo M, et al.
14, 15]. Our case demonstrates retrograde intussusception
Intussusception in adults: The role of MDCT in the
in a Roux-en-y reconstruction despite a side-to-side Y leg identification of the site and cause of obstruction.
anastomosis. Gastroenterol Res Pract 2016;2016:5623718.
Most intussusceptions occur in antegrade fashion, 3. Honore M, Chiow AKH, Bryant R. Retrograde
however, with RYGB, the intussusception is more often intussusception post Roux-en-Y gastric bypass. ANZ
retrograde in nature [1, 4, 11, 12]. All three limbs of the J Surg 2017;87(6):518–20.
Roux-en-Y anastomosis can be affected by intussusception, 4. Boudourakis LD, Divino C, Nguyen S. Retrograde
however in most cases published so far it has been the intussusception seven years after a laparoscopic
common channel that has invaginated through the Roux-en-Y gastric bypass. J Minim Access Surg
2013;9(2):82–3.
jejuno-jejunostomy [5]. The exact mechanism/cause
5. Carilli S, Arisoy M, Alper A. A rare complication
of intussusception post RYGB remains unclear [4]. The following laparoscopic Roux & Y gastric bypass:
most accepted theory is called the ‘Roux Stasis syndrome’ Intussusception-case report. Springerplus
hypothesis [4, 5]. It purports that ectopic pacemakers 2015;4:603.
are developed in the Roux limb to generate motor 6. Pauli EM, Haluck RS. Antiperistaltic (retrograde)
complexes that migrate both proximally and distally after intussusception after laparoscopic Roux-en-Y
bowel resection from the natural duodenal pacemakers gastric bypass procedure. Surg Obes Relat Dis
[9]. This may explain the high incidence of retrograde 2008;4(4):567–8.
intussusception in post-REYGB (69.8%) compared to 7. Stephenson D, Moon RC, Teixeira AF, Jawad MA.
Intussusception after Roux-en-Y gastric bypass. Surg
virgin abdomen (2.3%) [1].
Obes Relat Dis 2014;10(4):666–70.
Kitasato et al. divided the other causes into two 8. Yoshiyama S, Toiyama Y, Ichikawa T, et al.
groups; namely, mechanical and functional. Mechanical Laparoscopic diagnosis of retrograde peristalsis and
group causes include iatrogenic lead point created by intussusception in Roux-en-Y limb after laparoscopic
suture or staple line at the anastomosis, ptosis of the gastrectomy: A case report. Asian J Endosc Surg
gastrojejunal anastomosis, post-operative adhesions 2019;12(2):171–4.
and focal nodular hyperplasia. Functional causes include 9. Mukerji AN, Shah A, Parithivel VS. Retrograde
dysmotility, peristaltic abnormality, autonomic nervous intussusception after Roux-en-Y gastric bypass. Am
system abnormality, enteral nutrition, and a decrease in Surg 2016;82(9):e238–9.
10. Somma F, Faggian A, Serra N, et al. Bowel
gastric wall tension [1].
intussusceptions in adults: The role of imaging.
It has been noted there is a higher incidence of Radiol Med 2015;120(1):105–17.
intussusception in cases of RYGB for weight loss 11. Bhadra R, Somasundaram M, Nowak MM, Ravakhah
compared to cases of RYGB with gastrectomy [8, 9]. K. A near-fatal case of intussusception and ischaemic
This may be contributed to by thinning of the mesentery perforation of stomach in first-trimester pregnancy:
associated with weight loss, which increases the mobility Eight years after laparoscopic Roux-en-Y gastric
and instability of bowel, leading to a higher chance bypass. BMJ Case Rep 2018;11(1).
of intussusception [5, 9, 12]. Furthermore, the Roux 12. Khan K, Saeed S, Persaud A, Sbeih M, Gray S, Ahmed
limb in RYGB for obesity is much longer than in cases L. Retrograde jejunojejunal intussusception in a
pregnant female after laparoscopic Roux-en-Y gastric
with gastrectomy, which possibly increases the risk of
bypass. J Surg Case Rep 2018;2018(5):rjy094.
developing an intussusception [8]. 13. Singla S, Guenthart BA, May L, Gaughan J, Meilahn
JE. Intussusception after laparoscopic gastric bypass
surgery: An underrecognized complication. Minim
CONCLUSION Invasive Surg 2012;2012:464853.
14. Zhou Y, Wang F, Ji Y, Lv J. A CARE-compliant
An increase in incidence of intussusception article: A case of retrograde intussusception with
secondary to Roux-and-Y gastric bypass anastomosis is Uncut-Roux-en-Y anastomosis after radical total
noted; likely secondary to a rapid increase in bariatric gastrectomy: Review of the literature. Medicine
(Baltimore). 2017;96(48):e8982.
surgeries over the past 30 years. A prompt diagnosis of
15. Huang GS, Jin Y. Retrograde jejunal intussusception
intussusception is essential as it may lead to obstruction after total gastrectomy: A case report and literature
and bowel necrosis. Small bowel intussusception should review. Niger J Clin Pract 2016;19(3):411–3.
be considered as a differential diagnosis for abdominal
pain and gastrointestinal abnormalities in a patient with
a history of gastrectomy.
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:101022Z01TC2019. Chuang et al. 5
www.ijcasereportsandimages.com
********* Chung-Kwun Won – Conception of the work, Revising
the work critically for important intellectual content,
Author Contributions Final approval of the version to be published, Agree to be
Tzu-Yi (Arron) Chuang – Conception of the work, accountable for all aspects of the work in ensuring that
Design of the work, Acquisition of data, Analysis of data, questions related to the accuracy or integrity of any part
Interpretation of data, Drafting the work, Revising the of the work are appropriately investigated and resolved
work critically for important intellectual content, Final
approval of the version to be published, Agree to be Guarantor of Submission
accountable for all aspects of the work in ensuring that The corresponding author is the guarantor of submission.
questions related to the accuracy or integrity of any part
of the work are appropriately investigated and resolved Source of Support
Mustafa Sher – Conception of the work, Analysis of data, None.
Drafting the work, Final approval of the version to be
published, Agree to be accountable for all aspects of the Consent Statement
work in ensuring that questions related to the accuracy Written informed consent was obtained from the patient
or integrity of any part of the work are appropriately for publication of this article.
investigated and resolved
Conflict of Interest
Damian Fry – Conception of the work, Analysis of data,
Authors declare no conflict of interest.
Revising the work critically for important intellectual
content, Final approval of the version to be published,
Data Availability
Agree to be accountable for all aspects of the work in
All relevant data are within the paper and its Supporting
ensuring that questions related to the accuracy or integrity
Information files.
of any part of the work are appropriately investigated and
resolved
Copyright
Marissa Stilianos – Conception of the work, Interpretation © 2019 Tzu-Yi (Arron) Chuang et al. This article is
of data, Revising the work critically for important distributed under the terms of Creative Commons
intellectual content, Final approval of the version to be Attribution License which permits unrestricted use,
published, Agree to be accountable for all aspects of the distribution and reproduction in any medium provided
work in ensuring that questions related to the accuracy the original author(s) and original publisher are properly
or integrity of any part of the work are appropriately credited. Please see the copyright policy on the journal
investigated and resolved website for more information.
Access full text article on Access PDF of article on
other devices other devices
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Submit your manuscripts at www.edoriumjournals.com



You can also read