Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Research
JAMA Internal Medicine | Original Investigation
Risk Factors Associated With Acute Respiratory Distress Syndrome
and Death in Patients With Coronavirus Disease 2019 Pneumonia
in Wuhan, China
Chaomin Wu, MD; Xiaoyan Chen, MD; Yanping Cai, MD; Jia’an Xia, MD; Xing Zhou, MD; Sha Xu, MD;
Hanping Huang, MD; Li Zhang, MD; Xia Zhou, MD; Chunling Du, MD; Yuye Zhang, BD; Juan Song, BD;
Sijiao Wang, BD; Yencheng Chao, MD; Zeyong Yang, MD; Jie Xu, MD; Xin Zhou, MD; Dechang Chen, MD;
Weining Xiong, MD; Lei Xu, MD; Feng Zhou, MD; Jinjun Jiang, MD; Chunxue Bai, MD;
Junhua Zheng, MD; Yuanlin Song, MD
Supplemental content
IMPORTANCE Coronavirus disease 2019 (COVID-19) is an emerging infectious disease that
was first reported in Wuhan, China, and has subsequently spread worldwide. Risk factors for
the clinical outcomes of COVID-19 pneumonia have not yet been well delineated.
OBJECTIVE To describe the clinical characteristics and outcomes in patients with COVID-19
pneumonia who developed acute respiratory distress syndrome (ARDS) or died.
DESIGN, SETTING, AND PARTICIPANTS Retrospective cohort study of 201 patients with
confirmed COVID-19 pneumonia admitted to Wuhan Jinyintan Hospital in China between
December 25, 2019, and January 26, 2020. The final date of follow-up was February 13,
2020.
EXPOSURES Confirmed COVID-19 pneumonia.
MAIN OUTCOMES AND MEASURES The development of ARDS and death. Epidemiological,
demographic, clinical, laboratory, management, treatment, and outcome data were also
collected and analyzed.
RESULTS Of 201 patients, the median age was 51 years (interquartile range, 43-60 years), and
128 (63.7%) patients were men. Eighty-four patients (41.8%) developed ARDS, and of those
84 patients, 44 (52.4%) died. In those who developed ARDS, compared with those who did
not, more patients presented with dyspnea (50 of 84 [59.5%] patients and 30 of 117 [25.6%]
patients, respectively [difference, 33.9%; 95% CI, 19.7%-48.1%]) and had comorbidities such
as hypertension (23 of 84 [27.4%] patients and 16 of 117 [13.7%] patients, respectively
[difference, 13.7%; 95% CI, 1.3%-26.1%]) and diabetes (16 of 84 [19.0%] patients and 6 of 117
[5.1%] patients, respectively [difference, 13.9%; 95% CI, 3.6%-24.2%]). In bivariate Cox
regression analysis, risk factors associated with the development of ARDS and progression
from ARDS to death included older age (hazard ratio [HR], 3.26; 95% CI 2.08-5.11; and HR,
6.17; 95% CI, 3.26-11.67, respectively), neutrophilia (HR, 1.14; 95% CI, 1.09-1.19; and HR, 1.08;
95% CI, 1.01-1.17, respectively), and organ and coagulation dysfunction (eg, higher lactate
dehydrogenase [HR, 1.61; 95% CI, 1.44-1.79; and HR, 1.30; 95% CI, 1.11-1.52, respectively] and
D-dimer [HR, 1.03; 95% CI, 1.01-1.04; and HR, 1.02; 95% CI, 1.01-1.04, respectively]). High
fever (ⱖ39 °C) was associated with higher likelihood of ARDS development (HR, 1.77; 95% CI,
1.11-2.84) and lower likelihood of death (HR, 0.41; 95% CI, 0.21-0.82). Among patients with
ARDS, treatment with methylprednisolone decreased the risk of death (HR, 0.38; 95% CI,
0.20-0.72). Author Affiliations: Author
affiliations are listed at the end of this
CONCLUSIONS AND RELEVANCE Older age was associated with greater risk of development of article.
ARDS and death likely owing to less rigorous immune response. Although high fever was Corresponding Authors: Yuanlin
associated with the development of ARDS, it was also associated with better outcomes Song, MD, Department of Pulmonary
among patients with ARDS. Moreover, treatment with methylprednisolone may be beneficial and Critical Care Medicine,
Zhongshan Hospital, Fudan
for patients who develop ARDS.
University, 180 Fenglin Rd, Shanghai
200032, China (ylsong70_02@163.
com); Junhua Zheng, MD,
Department of Urology, Shanghai
General Hospital, Shanghai Jiao Tong
University School of Medicine,
JAMA Intern Med. doi:10.1001/jamainternmed.2020.0994 85 Wujin Rd, Shanghai 200080,
Published online March 13, 2020. China (zhengjh0471@sina.com).
(Reprinted) E1
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by Nicolas Minec on 03/26/2020Research Original Investigation Acute Respiratory Distress Syndrome and Death in Patients With COVID-19 in Wuhan, China
S
evere acute respiratory syndrome coronavirus 2 (SARS-
CoV-2) was first reported in Wuhan, Hubei Province, Key Points
China and has subsequently spread to other regions of
Question What clinical characteristics are associated with the
China and 37 countries, including the United States, Japan, Aus- development of acute respiratory distress syndrome (ARDS) and
tralia, and France.1 SARS-CoV-2, which belongs to a unique progression from ARDS to death among patients with coronavirus
clade of the sarbecovirus subgenus of the Orthocoronaviri- disease 2019 (COVID-19) pneumonia?
nae subfamily, was identified as the pathogen of coronavirus
Findings In this cohort study involving 201 patients with
disease 2019 (COVID-19) in January 2020.2 confirmed COVID-19 pneumonia, risk factors associated with the
As reported by Huang et al,3 patients with COVID-19 pre- development of ARDS and progression from ARDS to death
sent primarily with fever, myalgia or fatigue, and dry cough. included older age, neutrophilia, and organ and coagulation
Although most patients are thought to have a favorable prog- dysfunction. Treatment with methylprednisolone may be
nosis, older patients and those with chronic underlying con- beneficial for patients who develop ARDS.
ditions may have worse outcomes. Patients with severe ill- Meaning Risk for developing ARDS included factors consistent
ness may develop dyspnea and hypoxemia within 1 week after with immune activation; older age was associated with both ARDS
onset of the disease, which may quickly progress to acute re- development and death, likely owing to less robust immune
spiratory distress syndrome (ARDS) or end-organ failure.4 Cer- responses.
tain epidemiological features and clinical characteristics of
COVID-19 have been previously reported.3-5 However, these
studies were based on relatively small sample sizes, and risk ences, and Wuhan Institute of Virology of the Chinese Academy
factors leading to poor clinical outcomes have not been well of Sciences) as described previously.4 Other respiratory patho-
delineated. In this study, we report the clinical characteris- gens, including respiratory syncytial virus, adenovirus, para-
tics and factors associated with developing ARDS after hospi- influenza virus, influenza A virus, and influenza B virus, were
tal admission and progression from ARDS to death in patients also detected by real-time reverse transcriptase–polymerase
with COVID-19 pneumonia from a single hospital in Wuhan, chain reaction assays in 173 patients. Possible bacterial or fun-
China. gal pathogens were detected by sputum culture. Addition-
ally, patients underwent blood routine blood test, coagula-
tion, and biochemical tests and chest x-rays or computed
tomography. The most intense level of oxygen support dur-
Methods ing hospitalization (nasal cannula, noninvasive mechanical
Study Population ventilation [NMV], invasive mechanical ventilation [IMV], or
This is a retrospective cohort study of 201 patients aged 21 to IMV with extracorporeal membrane oxygenation [ECMO]) was
83 years with confirmed COVID-19 pneumonia hospitalized at recorded. The majority of the clinical data used in this study
Jinyintan Hospital in Wuhan, China. All patients were diag- was collected from the first day of hospital admission unless
nosed with COVID-19 pneumonia according to World Health indicated otherwise. To minimize interference of treatment
Organization interim guidance.6 According to hospital data, pa- during hospitalization, the highest patient temperature was de-
tients were admitted from December 25, 2019, to January 26, fined using the self-reported highest temperature prior to hos-
2020. Of 201 patients, 10 have been described previously by pital admission. Older age was classified as 65 years or older.
Chen et al4 and Huang et al.3 The ethics committee of Jinyin- Fever and high fever were classified as 37.3 °C or higher and
tan Hospital approved this study and granted a waiver of in- 39 °C or higher, respectively.
formed consent from study participants.
Outcomes
Procedures Two outcomes were evaluated: development of ARDS and
A trained team of physicians and medical students reviewed death among those with ARDS. World Health Organization in-
and collected epidemiological, clinical, and outcomes data from terim guidance was used to define ARDS.6
electronic medical records. Patients were followed up to Feb-
ruary 13, 2020. The individual components of all definitions Statistical Analysis
of clinical outcomes were recorded separately and checked by Descriptive analyses of the variables were expressed as me-
2 authors (C.W. and X.C.). Patient confidentiality was pro- dian (interquartile range [IQR]), or number (%). Differences in
tected by assigning a deidentified patient identification, and distributions of patient characteristics by outcome sub-
the electronic data was stored in a locked, password- groups are reported using differences with 95% CIs. Categori-
protected computer. cal data were compared using the χ2 test or the Fisher exact
To identify SARS-CoV-2 infection, throat swab samples test. Nonnormal distributed continuous data were compared
were obtained from all patients at admission and tested using using Mann-Whitney-Wilcoxon test.
real-time reverse transcriptase–polymerase chain reaction as- Bivariate Cox proportional hazard ratio (HR) models were
says according to the same protocol described previously.3 The used to determine HRs and 95% CIs between individual fac-
pathogenic detection was determined in 4 institutions (Chi- tors on the development of ARDS or progression from ARDS
nese Center for Disease Control and Prevention, Chinese Acad- to death. Sample size varied because of missing data (summa-
emy of Medical Sciences, Academy of Military Medical Sci- rized in Tables 1 and 2). Survival curves were developed using
E2 JAMA Internal Medicine Published online March 13, 2020 (Reprinted) jamainternalmedicine.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by Nicolas Minec on 03/26/2020Acute Respiratory Distress Syndrome and Death in Patients With COVID-19 in Wuhan, China Original Investigation Research
Table 1. Demographic Characteristics of Patients With Coronavirus Table 1. Demographic Characteristics of Patients With Coronavirus
Disease 2019 Pneumonia Disease 2019 Pneumonia (continued)
Study population No. (%) Study population No. (%)
No. of patients 201 Clinical outcomes
Age, median (IQR), y 51 (43-60) ARDS 84 (41.8)
≥65 40 (19.9) ICU admission 53 (26.4)Research Original Investigation Acute Respiratory Distress Syndrome and Death in Patients With COVID-19 in Wuhan, China
Table 2. Initial Laboratory Indices of Patients With Coronavirus Disease 2019 Pneumonia
No. of patients
No. of with value
Reference patients Value, deviation from
Tests in study population values tested median (IQR) reference (%)
Hematologic
White blood cells, ×109/mL 3.5-9.5 197 5.94 (3.80-9.08) 46 (23.4)a
9
Neutrophils, ×10 /mL 1.8-6.3 197 4.47 (2.32-7.70) 68 (34.5)a
9
Lymphocytes, ×10 /mL 1.1-3.2 197 0.91 (0.60-1.29) 126 (64.0)b
Monocytes, ×109/mL 0.1-0.6 197 0.33 (0.22-0.44) 18 (9.1)a
Platelets, ×109/mL 125-350 197 180.00 (137.00-241.50) 37 (18.8)b
CD3, /μL NA 97 607.00 (430.50-830.50) NA
CD4, /μL NA 97 353.00 (226.50-499.00) NA
CD8, /μL NA 97 236.00 (142.50-314.50) NA
Biochemical
Total bilirubin, mg/dL 0-26 198 11.45 (9.00-14.75) 10 (5.1)a
AST, U/L 15-40 198 33.00 (26.00-45.00) 59 (29.8)a
ALT, U/L 9-50 198 31.00 (19.75-47.00) 43 (21.7)a
Total protein, g/L 65-85 198 63.90(59.78-67.00) 113 (57.1)b
Albumin, g/L 40-55 198 32.75 (29.10-35.40) 195 (98.5)b
Globulin, g/L 20-40 198 30.65 (28.58-33.72) 8 (4.0)a
Prealbumin, mg/L 200-430 187 121.00 (87.00-157.00) 164 (87.7)b
Urea, mM 3.6-9.5 198 4.80 (3.68-6.10) 9 (4.5)a
Creatinine, μM 57-111 198 72.20 (57.68-83.00) 9 (4.5)a
Glucose, mM 3.9-6.1 197 6.00 (5.00-7.95) 89 (45.2)a
CK-MB, U/L 0-24 198 15.00 (12.00-20.00) 9 (4.5)a
Cholinesterase, U/L 5000-12000 185 7776.00 (6427.00-9216.50) 11 (6.0)b
Cystatin C, mg/L 0.6-1.55 182 0.88 (0.74-1.05) 10 (5.5)a
LDH, U/L 120-150 198 307.50 (232.25-389.25) 194 (98.0)a Abbreviations: α-HBDH,
a α-hydroxybutyric dehydrogenase;
α-HBDH, U/L 72-182 194 252.50 (195.25-337.50) 148 (76.3)
ALT, alanine aminotransferase; APTT,
LDL, mM 2.1-3.37 195 2.06 (1.60-2.58) 94 (48.2)b activated partial thromboplastin
Infection-related indices time; AST, aspartate
hs-CRP, mg/L 0-5 194 42.40 (14.15-92.68) 166 (85.6)a aminotransferase; CK-MB, creatine
kinase muscle-brain isoform; ESR,
IL-6, pg/L 0-7 123 6.98 (5.46-9.02) 60 (48.8)a
erythrocyte sedimentation rate;
ESR, mm/h 0-15 194 49.30 (40.00-66.88) 182 (93.8)a hs-CRP, high-sensitivity C-reactive
Serum ferritin, ng/mL 21.8-274.66 163 594.00 (315.69-1266.16) 128 (78.5)a protein; IL-6, interleukin-6; IQR,
Coagulation function interquartile range; LDH, lactate
dehydrogenase; LDL, low-density
PT, s 10.5-13.5 195 11.10 (10.20-11.90) 4 (2.1)a
lipoprotein; PT, prothrombin time.
APTT, s 21-37 195 28.70 (23.30-33.70) 19 (9.7)a a
Above reference.
D-dimer, μg/mL 0-1.5 189 0.61 (0.35-1.28) 44 (23.3)a b
Below reference.
cluding nasal cannula (n = 98 [48.8%]), NMV (n = 61 [30.3%]), [34.5%]) of patients had neutrophilia. Approximately one-quarter
IMV (n = 5 [2.5%]), or IMV with ECMO (n = 1 [0.5%]). Among (46 of 197 [23.4%]) of patients had leukocytosis. Some patients
201 patients, most (n = 196 [97.5%]) received empirical anti- demonstrated liver injury with elevated aspartate aminotrans-
biotic treatment and antiviral therapy (n = 170 [84.6%]), in- ferase (AST; 59 of 198 [29.8%]) and alanine aminotransferase (ALT;
cluding oseltamivir (n = 134 [66.7%]), ganciclovir (n = 81 43 of 198 [21.7%]). Most patients presented with an elevated myo-
[40.3%]), lopinavir/ritonavir (n = 30 [14.9%]), and interferon cardial indices: 194 of 198 (98.0%) had elevated lactate dehydro-
alfa (n = 22 [10.9%]). More than half (n = 106 [52.7%]) of pa- genase (LDH), and 9 of 198 (4.5%) had an elevated creatine kinase
tients received antioxidant therapy, including glutathione and muscle-brain isoform. Few patients had kidney injury indicated
N-acetyl-L-cysteine. Methylprednisolone was given to 62 by elevated plasma urea (9 of 198 [4.5%]) and serum creatinine
(30.8%) patients, and immunomodulators, including immu- (9 of 198 [4.5%]). Of 195 patients, 4 (2.1%) presented with pro-
noglobulin, thymosin, and recombinant human granulocyte longed prothrombin times (PTs).
colony stimulating factor, were given to 70 (34.8%) patients.
Clinical Outcomes
Laboratory Indices As of February 13, 2020, 144 of the total 201 patients (71.6%)
Laboratory findings on hospital admission are summarized in were discharged from the hospital. The median hospital stay
Table2.Of194patients,166(85.6%)demonstratedincreasedhigh- was 13 days (IQR, 10-16 days), and 13 (6.5%) patients were still
sensitivity C-reactive protein. More than half (126 of 197 [64.0%]) hospitalized. Of the entire cohort, 84 (41.8%) patients devel-
of this cohort had lymphocytopenia. About one-third (68 of 197 oped ARDS, 53 (26.4%) were admitted to the intensive care unit,
E4 JAMA Internal Medicine Published online March 13, 2020 (Reprinted) jamainternalmedicine.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by Nicolas Minec on 03/26/2020Acute Respiratory Distress Syndrome and Death in Patients With COVID-19 in Wuhan, China Original Investigation Research
67 (33.3%) received mechanical ventilation, and 44 (21.9%) portions of hypertension (difference, 18.9%; 95% CI, −2.0% to
died. Among the 67 patients who received mechanical venti- 39.7%; P = .05). The patients who died were less likely to be
lation, 44 (65.7%) died, 14 (20.9%) were discharged from the treated with antiviral therapy (difference, −40.7%; 95% CI,
hospital, and 9 (13.4%) remained hospitalized. The median time −58.5% to −22.9%; P < .001). Regarding the most intense level
from admission to developing ARDS was 2 days (IQR, 1-4 days). of oxygen support among the 44 ARDS patients who died, 38
All of the patients who died had developed ARDS and re- (86.4%) received NMV, 5 (11.4%) received IMV, and 1 (2.3%) re-
ceived mechanical ventilation. ceived IMV with ECMO.
Table 3 demonstrates that when compared with patients For patients with ARDS who died, the value of liver dam-
without ARDS, patients with ARDS were older (difference, 12.0 age indices (total bilirubin [difference, 2.60 mg/dL; 95% CI,
years; 95% CI, 8.0-16.0 years; P < .001) and had higher tem- 0.30-5.20 mg/dL; P = .03]), renal dysfunction indices (urea [dif-
perature prior to admission (difference, 0.30 °C; 95% CI, 0.00- ference, 1.50 mM; 95% CI, 0.50-2.70 mM; P = .004]), inflam-
0.50 °C; P = .004). More patients with ARDS presented with mation-related indices (IL-6 [difference, 3.88 pg/L; 95% CI,
initial symptoms of dyspnea compared with those without 2.20-6.13 pg/L; P < .001]), and coagulation function indices (D-
ARDS (difference, 33.9%; 95% CI, 19.7%-48.1%; P < .001). Com- dimer [difference, 2.10 μg/mL; 95% CI, 0.89-5.27 μg/mL;
pared with patients without ARDS, patients with ARDS had a P = .001]) were significantly elevated compared with pa-
higher proportion of comorbidities, including hypertension tients with ARDS who survived. However, lymphocyte counts
(difference, 13.7%; 95% CI, 1.3%-26.1%; P = .02) and diabetes (difference, −0.23 ×109/mL; 95% CI, −0.41 to −0.07 ×109/mL;
(difference, 13.9%; 95% CI, 3.6%-24.2%; P = .002). In addi- P = .004) and CD8 T cells (difference, −134 cells/μL; 95% CI,
tion, when compared with patients who did not have ARDS, −221 to −10 cells/μL; P = .05) were significantly decreased
patients who developed ARDS were less likely to be treated with (Table 3).
antiviral therapy (difference, −14.4%; 95% CI, −26.0% to −2.9%; Bivariate Cox models showed that several factors
P = .005) and more likely to be treated with methylpredniso- related to the development of ARDS were not associated
lone (difference, 49.3%; 95% CI, 36.4%-62.1%; P < .001). Of 84 with death, which included comorbidities, lymphocyte
patients with ARDS, 61 (72.6%) received NMV, 17 (20.2%) re- counts, CD3 and CD4 T-cell counts, AST, prealbumin, creati-
ceived nasal cannula, 5 (6.0%) received IMV, and 1 (1.2%) re- nine, glucose, low-density lipoprotein, serum ferritin, and
ceived IMV with ECMO. PT. However, IL-6 was statistically significantly associated
Compared with patients without ARDS, for patients with with death (Table 4). Although high fever was associated
ARDS, the value of liver damage indices (total bilirubin [dif- with higher likelihood of developing ARDS (HR, 1.77; 95%
ference, 1.90 mg/dL; 95% CI, 0.60-3.30 mg/dL; P = .004]), re- CI, 1.11-2.84), it was negatively associated with death (HR,
nal dysfunction indices (urea [difference, 1.69 mM; 95% CI, 0.41; 95% CI, 0.21-0.82).
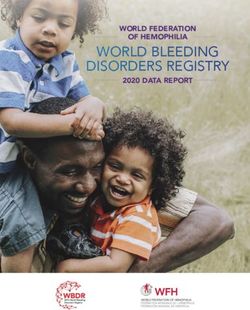
1.10-2.29 mM; P < .001]), inflammation-related indices (inter- Finally, among the patients with ARDS, of those who re-
leukin-6 [IL-6] [difference, 0.93 pg/L; 95% CI, 0.07-1.98 pg/L; ceived methylprednisolone treatment, 23 of 50 (46.0%) pa-
P = .03]), and coagulation function indices (D-dimer [differ- tients died, while of those who did not receive methylpred-
ence, 0.52 μg/mL; 95% CI, 0.21-0.94 μg/mL; P < .001]) were nisolone treatment, 21 of 34 (61.8%) died. The administration
significantly elevated. However, lymphocyte counts (differ- of methylprednisolone appears to have reduced the risk of
ence, −0.34 ×109/mL; 95% CI, −0.47 to −0.22 ×109/mL; P < .001) death in patients with ARDS (HR, 0.38; 95% CI, 0.20-0.72;
and CD8 T cells (difference, −66.00 cells/μL; 95% CI, −129.00 P = .003) (Figure).
to −7.00 cells/μL; P = .03) were significantly decreased.
As summarized in Table 4, older age (≥65 years old), high
fever (≥39 °C), comorbidities (eg, hypertension, diabetes), neu-
trophilia, lymphocytopenia (as well as lower CD3 and CD4 T-
Discussion
cell counts), elevated end-organ related indices (eg, AST, urea, In this cohort study, we reported the clinical characteristics and
LDH), elevated inflammation-related indices (high- risk factors associated with clinical outcomes in patients with
sensitivity C-reactive protein and serum ferritin), and el- COVID-19 pneumonia who developed ARDS after admission,
evated coagulation function–related indicators (PT and D- as well as those who progressed from ARDS to death. Patients
dimer) were significantly associated with higher risks of the who received methylprednisolone treatment were much more
development of ARDS. Patients who received treatment with likely to develop ARDS likely owing to confounding by indi-
methylprednisolone appear to have been sicker than patients cation; specifically, sicker patients were more likely to be given
who did not receive it. Specifically, a higher proportion of pa- methylprednisolone. However, administration of methylpred-
tients who received methylprednisolone were classified into nisolone appeared to reduce the risk of death in patients with
a higher grade on the Pneumonia Severity Index7 compared ARDS. These findings suggest that for patients with COVID-19
with patients who did not receive methylprednisolone (P = .01; pneumonia, methylprednisolone treatment may be benefi-
eTable 2 in the Supplement). cial for those who have developed ARDS on disease progres-
In the subgroup of patients who developed ARDS, pa- sion. However, these results should be interpreted with cau-
tients who ultimately died were older (difference, 18.0 years; tion owing to potential bias and residual confounding in this
95% CI, 13.0-23.0 years; P < .001) and had lower proportion of observational study with a small sample size. Double-
high fever (difference, −31.8%; 95% CI, −56.5% to −7.1%; blinded randomized clinical trials should be conducted to vali-
P = .007) than those who survived. They also had higher pro- date these results.
jamainternalmedicine.com (Reprinted) JAMA Internal Medicine Published online March 13, 2020 E5
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by Nicolas Minec on 03/26/2020E6
Table 3. Clinical Characteristics and Initial Laboratory Indices Among Patients With and Without ARDS
All patients Patients with ARDS
Without ARDS, With ARDS, No. (%) Difference P Alive, No. (%) Died, No. (%) Difference P
Clinical characteristics No. (%) (n = 117) (n = 84) (95% CI)a valueb (n = 40) (n = 44) (95% CI)a valueb
Age, median (IQR), y 48.0 (40.0 to 54.0) 58.5 (50.0 to 69.0) 12.0 (8.0 to 16.0)Table 3. Clinical Characteristics and Initial Laboratory Indices Among Patients With and Without ARDS (continued)
All patients Patients with ARDS
Without ARDS, With ARDS, No. (%) Difference P Alive, No. (%) Died, No. (%) Difference P
Clinical characteristics No. (%) (n = 117) (n = 84) (95% CI)a valueb (n = 40) (n = 44) (95% CI)a valueb
Biochemical
Total bilirubin, mg/dL 10.50 (8.60 to 13.65) 12.90 (9.50 to 17.05) 1.90 (0.60 to 3.30) .004 11.65 (9.33 to 15.15) 14.50 (10.35 to 19.80) 2.60 (0.30 to 5.20) .03
jamainternalmedicine.com
AST, U/L 30.00 (24.00 to 38.50) 38.00 (30.50 to 53.00) 9.00 (5.00 to 12.00)Research Original Investigation Acute Respiratory Distress Syndrome and Death in Patients With COVID-19 in Wuhan, China
Table 4. Bivariate Cox Regression of Factors Associated With ARDS Development or Progression
From ARDS to Death
ARDS Death
Patient characteristics and findings HR (95% CI) P value HR (95% CI) P value
Clinical characteristics
Age (≥65 vsAcute Respiratory Distress Syndrome and Death in Patients With COVID-19 in Wuhan, China Original Investigation Research
share the same cell entry receptors with SARS-CoV-2,17,18 could
Figure. Survival Curve in Patients With Acute Respiratory Distress
Syndrome Who Did and Did Not Receive Methylprednisolone Treatment infect immune cells, including T lymphocytes, monocytes, and
macrophages.19 The CD3, CD4, and CD8 T-cell counts decreased
1.0 at the onset of illness; this decrease persisted until the recovery
period of SARS-CoV pneumonia.19 In addition, CD4 and CD8 T-cell
Overall survival probability 0.8 counts decreased in the peripheral blood specimen of patients
+ + withfatalSARS-CoVpneumonia10,20,21,whichwasconsistentwith
0.6
+++ these results that patients with COVID-19 pneumonia and ARDS
++ + Methylprednisolone
+ + presented with lymphocytopenia (CD3, CD4, and CD8 T cells).
++ +++ ++ ++
0.4 Studies demonstrated that T-cell responses can inhibit the over-
++++ ++
No methylprednisolone activation of innate immunity.22 T cells were reported to help clear
0.2 SARS-CoV, and a suboptimal T-cell response was found to cause
pathological changes observed in mice with SARS-CoV.23 We hy-
0
0 5 10 15 20 25 30 35 40
pothesized that persistent and gradual increases in lymphocyte
Days after admission responses might be required for effective immunity against SARS-
No. at risk CoV-2 infection. Further studies are needed to characterize the
No methylprednisolone 34 28 17 4 0 0 0 0 0
Methylprednisolone 50 48 39 29 20 14 11 4 0 role of the neutrophil and lymphocyte response or that of CD4 and
CD8 T-cell immune response in SARS-CoV-2 infection.
Administration of methylprednisolone reduced the risk of death (hazard ratio,
0.38; 95% CI, 0.20-0.72; P = .003).
Limitations
important roles in disease severity.9 Neutrophilia was found in This study has several limitations. First, owing to limited medi-
both the peripheral blood10 and lung11 of patients with SARS-CoV. cal resources, only patients with relatively severe COVID-19
The severity of lung damage correlated with extensive pulmonary pneumonia were hospitalized during this period. Second, this
infiltration of neutrophils and macrophages and higher numbers study was conducted at a single-center hospital with limited
of these cells in the peripheral blood in patients with Middle East sample size. As such, this study may have included dispro-
respiratory syndrome.12-14 Neutrophils are the main source of portionately more patients with poor outcomes. There may also
chemokines and cytokines. The generation of cytokine storm can be a selection bias when identifying factors that influence the
lead to ARDS, which is a leading cause of death in patients with clinical outcomes. A larger cohort study of patients with
severe acute respiratory syndrome15 and Middle East respiratory COVID-19 pneumonia from Wuhan, China, other cities in China,
syndrome.14 In this study, patients with COVID-19 pneumonia and other countries would help to further define the clinical
who had developed ARDS had significantly higher neutrophil characteristics and risk factors of the disease.
counts than did those without ARDS, perhaps leading to the ac-
tivation of neutrophils to execute an immune response against
the virus, but also contributing to cytokine storm. This may partly
explain the positive association of high fever and ARDS found at
Conclusions
the early stages of COVID-19. In addition, considering that older Older age was associated with greater risk of developing ARDS
age is associated with declined immune competence,16 the results and death, likely because of less rigorous immune response.
of the present study showed that older age was associated with Although fever was associated with the development of ARDS,
both ARDS and death. Therefore, older age related to death may it was also associated with better outcomes. Several factors re-
be due to less robust immune responses. lated to the development of ARDS were not associated with
The results of this study show that higher CD3 and CD4 T-cell death, which indicates that different pathophysiological
counts might protect patients from developing ARDS, but simi- changes from hospital admission to development of ARDS and
lar results were not observed when examined for death, possi- from development of ARDS to death may exist. Moreover, treat-
bly because of limited sample size. CD8 counts were significantly ment with methylprednisolone may be beneficial for pa-
higher in those who were alive. These results indicate the impor- tients who develop ARDS. Double-blinded randomized clini-
tant roles of CD4 and CD8 T cells in COVID-19 pneumonia. Ear- cal trials to determine the most effective treatments for
lier studies have revealed that SARS-CoV, which was reported to COVID-19 are still needed.
ARTICLE INFORMATION Medicine, Zhongshan Hospital, Fudan University, General Hospital, Shanghai Jiao Tong University
Accepted for Publication: March 3, 2020. Shanghai, China (Wu, X. Chen, Y. Zhang, J. Song, School of Medicine, Shanghai, China (X. Zhou);
Wang, Chao, Jiang, Bai, Y. Song); Tuberculosis and Department of Critical Care Medicine, Ruijin
Published Online: March 13, 2020. Respiratory Department, Wuhan Jinyintan Hospital, Hospital, Shanghai Jiao Tong University School of
doi:10.1001/jamainternmed.2020.0994 Wuhan, China (Xia, Huang, L. Zhang, X. Zhou); Medicine, Shanghai, China (D. Chen); Department
Author Affiliations: Department of Pulmonary Department of Anesthesiology, International Peace of Respiratory Medicine, Shanghai Ninth People's
Medicine, QingPu Branch of Zhongshan Hospital Maternity and Child Health Hospital, Shanghai Jiao Hospital, Shanghai Jiao Tong University School of
Affiliated to Fudan University, Shanghai, China (Wu, Tong University School of Medicine, Shanghai, Medicine, Shanghai, China (Xiong); Department of
Du, F. Zhou, Y. Song); Infection Division, Wuhan China (Yang); Department of Infectious Diseases, Emergency Medicine, Shanghai Pudong New Area
Jinyintan Hospital, Wuhan, China (Wu, Cai, X. Zhou, Fengxian Guhua Hospital, Shanghai, China (J. Xu); Gongli Hospital, Shanghai, China (L. Xu); Shanghai
S. Xu); Department of Pulmonary and Critical Care Department of Pulmonary Medicine, Shanghai Respiratory Research Institute, Shanghai, China
jamainternalmedicine.com (Reprinted) JAMA Internal Medicine Published online March 13, 2020 E9
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by Nicolas Minec on 03/26/2020Research Original Investigation Acute Respiratory Distress Syndrome and Death in Patients With COVID-19 in Wuhan, China
(Bai, Y. Song); Department of Urology, Shanghai Fudan University for their data collection. They syndrome. Lancet. 2003;361(9371):1773-1778.
General Hospital, Shanghai Jiao Tong University were not compensated for their contributions. doi:10.1016/S0140-6736(03)13413-7
School of Medicine, Shanghai, China (Zheng); 12. Ng DL, Al Hosani F, Keating MK, et al.
National Clinical Research Center for Aging and REFERENCES Clinicopathologic, immunohistochemical, and
Medicine, Huashan Hospital, Fudan University, 1. World Health Organization. Coronavirus disease ultrastructural findings of a fatal case of Middle East
Shanghai, China (Y. Song). 2019 (COVID-19): situation report—37. February 25, respiratory syndrome coronavirus infection in the
Author Contributions: Drs Song and Zheng had full 2020. Accessed February 26, 2020. United Arab Emirates, April 2014. Am J Pathol.
access to all of the data in the study and take https://www.who.int/docs/default-source/ 2016;186(3):652-658. doi:10.1016/j.ajpath.2015.10.
responsibility for the integrity of the data and the coronaviruse/situation-reports/20200226-sitrep- 024
accuracy of the data analysis. Drs Wu, X. Chen, Cai, 37-covid-19.pdf?sfvrsn=6126c0a4_2. 13. Min CK, Cheon S, Ha NY, et al. Comparative and
and Xia contributed equally and share first 2. Zhu N, Zhang D, Wang W, et al; China Novel kinetic analysis of viral shedding and immunological
authorship. Drs Song and Zheng contributed Coronavirus Investigating and Research Team. A responses in MERS patients representing a broad
equally to the study. novel coronavirus from patients with pneumonia in spectrum of disease severity. Sci Rep. 2016;6:25359.
Study concept and design: Wu, X. Chen, Cai, Xia, China, 2019. N Engl J Med. 2020;382(8):727-733. doi:10.1038/srep25359
Zheng, Y. Song. doi:10.1056/NEJMoa2001017
Acquisition, analysis, or interpretation of data: X. 14. Kim ES, Choe PG, Park WB, et al. Clinical
Chen, Xing Zhou, S. Xu, Huang, L. Zhang, Xia Zhou, 3. Huang C, Wang Y, Li X, et al Clinical features of progression and cytokine profiles of Middle East
Du, Y. Zhang, J. Song, Wang, Chao, Yang, J. Xu, Xin patients infected with 2019 novel coronavirus in respiratory syndrome coronavirus infection.
Zhou, D. Chen, Xiong, L. Xu, F. Zhou, Jiang, Bai. Wuhan, China. Lancet. 2020;395(10223):497-506. J Korean Med Sci. 2016;31(11):1717-1725.
Drafting of the manuscript: X. Chen, Xia, Xing Zhou, doi:10.1016/S0140-6736(20)30183-5 doi:10.3346/jkms.2016.31.11.1717
S. Xu, Huang, L. Zhang, Xia Zhou, Du, Y. Zhang, J. 4. Chen N, Zhou M, Dong X, et al. Epidemiological 15. Lew TW, Kwek TK, Tai D, et al. Acute respiratory
Song, Wang, Chao, Yang, J. Xu, Xin Zhou, D. Chen, and clinical characteristics of 99 cases of 2019 distress syndrome in critically ill patients with
Xiong, L. Xu, F. Zhou, Jiang, Bai. novel coronavirus pneumonia in Wuhan, China: severe acute respiratory syndrome. JAMA. 2003;
Critical revision of the manuscript for important a descriptive study. Lancet. 2020;395(10223):507- 290(3):374-380. doi:10.1001/jama.290.3.374
intellectual content: Wu, X. Chen, Cai, Xia, Du, 513. doi:10.1016/S0140-6736(20)30211-7 16. Goronzy JJ, Fang F, Cavanagh MM, Qi Q,
Zheng, Y. Song. 5. Wang D, Hu B, Hu C, et al Clinical characteristics Weyand CM. Naive T cell maintenance and function
Statistical analysis: X. Chen, Y. Song. of 138 hospitalized patients with 2019 novel in human aging. J Immunol. 2015;194(9):4073-4080.
Obtained funding: Wu, Zheng, Y. Song. coronavirus-infected pneumonia in Wuhan, China. doi:10.4049/jimmunol.1500046
Administrative, technical, or material support: Cai, JAMA. Published online February 7, 2020. doi:10.
Xia, Xing Zhou, S. Xu, Huang, L. Zhang, Xia Zhou, 17. Zhou P, Yang XL, Wang XG, et al. A pneumonia
1001/jama.2020.1585 outbreak associated with a new coronavirus of
Yang, J. Xu, Xin Zhou, D. Chen, Xiong, L. Xu, F. Zhou,
Jiang, Bai, Zheng, Y. Song. 6. World Health Organization. Clinical probable bat origin. Nature. Published online
Study supervision: Zheng, Y. Song. management of severe acute respiratory infection February 3, 2020. doi:10.1038/s41586-020-2012-7
when novel coronavirus (nCoV) infection is 18. Hoffmann M, Kleine-Weber H, Krüger N, Müller
Conflict of Interest Disclosures: None reported. suspected: interim guidance. January 28, 2020. M, Drosten C, Pöhlmann S. The novel coronavirus
Funding/Support: This study was supported by a Accessed March 5, 2020. https://www.who.int/ 2019 (2019-nCoV) uses the SARS-coronavirus
grant from Prevention and Treatment of Infection in publications-detail/clinical-management-of-severe- receptor 2 ACE2 and the cellular protease TMPRSS2
Novel Coronavirus Pneumonia Patients from the acute-respiratory-infection-when-novel- for entry into target cells. Preprint. Posted online
Shanghai Science and Technology Committee (to Dr coronavirus-(ncov)-infection-is-suspected. January 31, 2020. bioRxiv. doi:10.1101/2020.01.31.
Yuanlin Song), the Special Fund of Shanghai 7. Fine MJ, Auble TE, Yealy DM, et al. A prediction 929042
Jiaotong University for Coronavirus Disease 2019 rule to identify low-risk patients with
Control and Prevention (2020RK47 to Dr Junhua 19. Gu J, Gong E, Zhang B, et al. Multiple organ
community-acquired pneumonia. N Engl J Med. infection and the pathogenesis of SARS. J Exp Med.
Zheng), and Academic Leader of Shanghai Qingpu 1997;336(4):243-250. doi:10.1056/
District Healthcare Commission (WD2019-36 to Dr 2005;202(3):415-424. doi:10.1084/jem.20050828
NEJM199701233360402
Chaomin Wu). 20. Li T, Qiu Z, Zhang L, et al. Significant changes of
8. Schell-Chaple HM, Puntillo KA, Matthay MA, Liu peripheral T lymphocyte subsets in patients with
Role of the Funder/Sponsor The funders had no KD; National Heart, Lung, and Blood Institute Acute
role in the design and conduct of the study; severe acute respiratory syndrome. J Infect Dis.
Respiratory Distress Syndrome Network. Body 2004;189(4):648-651. doi:10.1086/381535
collection, management, analysis, and temperature and mortality in patients with acute
interpretation of the data; preparation, review, or respiratory distress syndrome. Am J Crit Care. 2015; 21. Cui W, Fan Y, Wu W, Zhang F, Wang JY, Ni AP.
approval of the manuscript; and decision to submit 24(1):15-23. doi:10.4037/ajcc2015320 Expression of lymphocytes and lymphocyte
the manuscript for publication. subsets in patients with severe acute respiratory
9. Channappanavar R, Perlman S. Pathogenic syndrome. Clin Infect Dis. 2003;37(6):857-859. doi:
Additional Contributions: We thank Weibing human coronavirus infections: causes and
Wang, PhD, from the Department of Epidemiology, 10.1086/378587
consequences of cytokine storm and
School of Public Health, Fudan University; Yan Liu, immunopathology. Semin Immunopathol. 2017;39 22. Kim KD, Zhao J, Auh S, et al. Adaptive immune
MD, and Hongcai Shang, PhD, from Key Laboratory (5):529-539. doi:10.1007/s00281-017-0629-x cells temper initial innate responses. Nat Med.
of Chinese Internal Medicine of Ministry of 2007;13(10):1248-1252. doi:10.1038/nm1633
Education, Dongzhimen Hospital, Beijing University 10. Wang YH, Lin AS, Chao TY, et al. A cluster of
patients with severe acute respiratory syndrome in 23. Zhao J, Zhao J, Perlman S. T cell responses are
of Chinese Medicine; Xiaojia Huang, PhD, from the required for protection from clinical disease and for
Institute of Biomedical Engineering and Health a chest ward in southern Taiwan. Intensive Care Med.
2004;30(6):1228-1231. doi:10.1007/s00134-004- virus clearance in severe acute respiratory
Sciences, Changzhou University; and Yaohui Li, MD, syndrome coronavirus-infected mice. J Virol. 2010;
from Zhongshan Hospital, Fudan University for 2311-8
84(18):9318-9325. doi:10.1128/JVI.01049-10
their statistical analysis discussion. We also thank 11. Nicholls JM, Poon LLM, Lee KC, et al. Lung
Dongni Hou, MD, Sucheng Mu, MD, Donghui Zhang, pathology of fatal severe acute respiratory
MD, and Ke Lang, BD, from Zhongshan Hospital,
E10 JAMA Internal Medicine Published online March 13, 2020 (Reprinted) jamainternalmedicine.com
© 2020 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by Nicolas Minec on 03/26/2020You can also read