Royal Borough of Kingston upon Thames Lesbian, Gay, Bisexual and Transgender (LGBT) Sexual Health Needs Assessment
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Royal Borough of Kingston upon Thames
Lesbian, Gay, Bisexual and Transgender
(LGBT) Sexual Health Needs Assessment
Dee Wang
Research & Performance Officer
Contributions by Karen Skipper, Oliver Gilbody & Daniel Winstanley
West London Gay Men’s Project (WLGMP)
February 2013
Kingston upon Thames LGBT Needs Assessment
1 Executive Summary
The local authority of the Royal Borough of Kingston upon Thames has identified a gap in
knowledge in relation to the health and well-being needs and experiences of lesbian, gay,
bisexual and transgender (LGBT) people living in the borough. The health needs of the
LGBT community are often overlooked at a strategic level and in the design and delivery of
services. Thus, in consultation with the LGBT communities and key health and well-being
organisations in Kingston, the West London Gay Men’s Project (WLGMP) was
commissioned by NHS Kingston to develop the LGBT Sexual Health and Wellbeing Needs
Assessment as a tool to gather reliable information from which to assess and make
recommendations for effective local services going forwards.
Project aims
To understand the sexual health and well-being needs of LGBT people, to explore their
experiences of accessing health services in the borough of Kingston and to make
recommendations that would enable organisations to develop services that are effective,
evidence based, appropriate and sensitive to the needs of LGBT people.
In order to accomplish this WLGMP consulted with the LGBT community and key health
organisations in the design and distribution of the questionnaire. The questionnaire included
a range of question formats from multiple choice to open ended questions in order to gather
both quantitative and qualitative data. A short focus group discussion was held with support
from Kingston LGBT Forum to gather further qualitative information.
The Findings
Sample profile
A total of 125 LGBT people completed the questionnaire.
The gender balance was 22 women and 103 men, with 9 identifying as transgender.
12.0% identified as lesbian, 76.8% as gay men, 8.0% as bisexual and 0.8% each for
others including men who has sex with men (MSM), heterosexual transgender man,
not sure and not given.
Women were more strongly represented in the 20 – 29 age group, whereas men
were more strongly represented in the 20 – 59 age groups.
87.2% identified as various white backgrounds and 6.4% from the Black Asian and
Minority Ethnic (BAME) community
ii WLGMP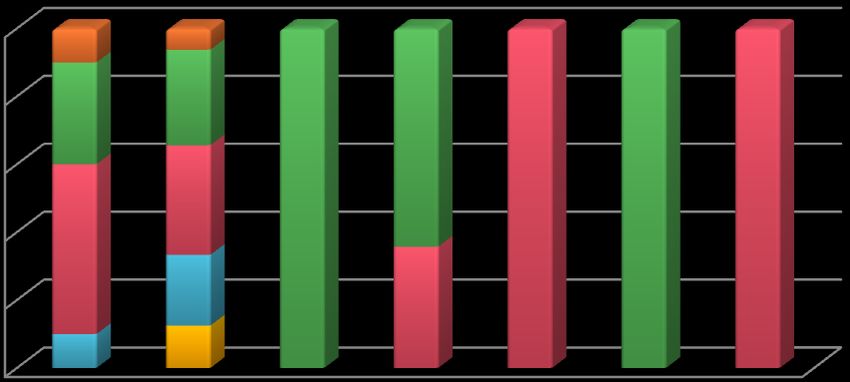
The most popular places for LGBT people to socialise are social gatherings at home
or visiting friends, general bars and clubs and LGBT exclusive bars and clubs,
followed by theatre /Cinema /Restaurants and dating/hook up websites.
96.8% of respondents are out to all or some of their friends, 88.0% are out to all or
some of their family with only 64.2% out to their GP/doctor.
Health & Wellbeing
80.8% of the respondents claimed having experienced certain mental health
problems. The most common issues include stress, anxiety and depression. A high
number, 29.6%, disclosed having experienced suicidal thoughts.
28.8% of respondents smoke.
24.8% regularly binge drink.
38.4% use drugs.
33% of gay respondents had more than 5 sexual partners in the past 6 months
compared to lesbian respondents who had 1 or fewer sexual partners.
Most respondents do not believe external factors impact their choice to have safer
sex. Within those who agree that external factors do affect their choice, alcohol,
drugs, depression and loneliness have had a negative influence when making safer
sex decisions.
30.4% had never used any sexual health services in Kingston. The most popular
sexual health service providers for male respondents are: K2 clinic, GUM clinic(s)
and the Wolverton Centre’s sexual health service. The most popular sexual health
service providers for female respondents are: GPs, family planning clinics and GUM
clinic(s).
5.6% had never used any sexual health service at all; many of these are female
respondents. For those who seek services outside Kingston, the most popular
services are STI screening/treatment, HIV screening/treatment, free condoms (and
lube) and information/support.
Use of Services
Only slightly more than a quarter of the respondents used the local LGBT
services/groups. “I’ve lived in RBK for 40 years and was totally unaware that there
are LGBT services here now! How can this be? What's gone wrong?”
84.8% used LGBT services outside Kingston, mainly for social groups, community
groups and condom (and lube) services.
iii WLGMPKingston upon Thames LGBT Needs Assessment
Experience with health Care
42.4% hadn’t come out to their GP/doctor. 77.8% of transgender respondents hadn’t
been given relevant information by a healthcare professional. 56.8% didn’t think that
their needs were fully understood by health staff.
The most important consideration in choosing a service is confidentiality (91.2%),
opening times (91.2%), comprehensive sexual health screening (88.8%) and location
(88.8%).
12 people participated in the focus group discussion and raised issues such as
bullying in school, assault and physical threat and parenthood that are facing LGBT
people.
Homophobia and heteronormativity (presumption of heterosexuality)1 are witnessed
within health and social care services. Lesbian participants reported more experience
of heteronormativity and found it harder to find specific health care services for their
needs.
Recommendations
GP and Primary Care
It is essential to improve accessibility and appropriateness of mainstream services.
Mainstream health care providers should revisit diversity training to ensure that it
raises awareness of how to effectively meet the needs of LGBT people, given that 42%
of respondents had not disclosed their sexual identity to their doctor, and 78% of
transgender respondents were offered no relevant information, with 57% saying their
needs were not fully understood.
Health and social care staff should be equipped with the skills to work more
sensitively with their LGBT patients, and adopt a standard of care to ensure that all
LGBT people are treated fairly, appropriately and respectfully. Health and social care
professionals should be trained to focus on the health issues that specifically relate to
LGBT people.
Mainstream health care providers should review EVERYTHING YOU ALWAYS WANTED TO
KNOW ABOUT SEXUAL ORIENTATION MONITORING... BUT WERE AFRAID TO ASK, a practice
guide to monitoring sexual orientation commissioned by NHS North West, aimed at
the public sector carrying out monitoring of staff and service users1.
iv WLGMPMental health and well-being
Services need to target LGBT people specifically for lifestyle issues, i.e. smoking;
alcohol and drug use. Treating service users holistically will ensure appropriate and
effective signposting and service delivery with better health outcomes for individuals.
An assessment of lifestyle issues at the time of other assessments for risk taking
behaviours, e.g. sexual risk taking, should be integrated into pathways.
Increase access and availability to mental health (i.e. counselling) support. Promotion
should target positive mental well-being across LGBT communities given that 80% of
respondents experienced mental health issues, with 29% having suicidal thoughts.
Assessments of clients’ mental health needs could usefully be integrated into any
assessment of their sexual health need, with robust signposting and referrals
pathways identified.
Younger LGBT respondents report higher levels of eating disorders and self harm and
identification of these additional issues need to be worked into individual risk
assessments when working with this group.
To combat bullying and heteronormactivity, integrate awareness of LGBT rights and
health and well-being issues into school education. This can be delivered by including
LGBT specific resources and signposting and including an LGBT element into general
health and well-being literature.
Sexual Health
With 26% of MSM having 5+ sexual partners in the last 6 months, and 35% having 2
to 4 sexual partners, and 12% of MSM HIV positive there are is clear evidence of
sexual health risk taking behaviour. A one to one behaviour change intervention for
high risk MSM, designed along NICE guidelines for effective interventions could
benefit this group.
Sexual Health Promotion needs to be targeted at lesbian and bisexual women as well
as gay men, recognising that they may attend different services to MSM. Service
providers should develop practical strategies that narrow the gap between an
understanding of safer sex and actual practices. It is important to identify, develop and
disseminate sexual health information aimed at lesbian and bisexual women as well
as for MSM
v WLGMPKingston upon Thames LGBT Needs Assessment
Targeted work with the 40% of MSM who use hook up websites or apps to meet other
MSM. This could be via online outreach (Netreach).
Local LGBT specific services are perceived to be very limited. LGBT specific health
promotion in popular venues (including those outside the borough) where LGBT
people socialise can raise the profile of the local LGBT groups and services, and also
increase awareness of LGBT health and well-being.
Integration of HIV testing availability into general activities such as saunas, clubs and
groups, and faster test results offered.
Condoms and lubricant are sought outside the borough currently but could be made
more readily available to Kingston residents via sexual health services and 24s
condom scheme, both of which were praised by respondents.
Raise awareness of local LGBT groups and services with LGBT people and other
mainstream services; develop and strengthen service networks in-between. This can
be achieved through many different methods including allowing general health
promotion with LGBT representation and distribution into mainstream outlets/services.
Service Access and integration
Organisations should undertake sexuality impact assessments to review polices,
practices and procurement to ensure they are meeting the needs of the LGBT
community and are not being discriminated against. Anti homophobic/ transphobic
bullying policies should be enforced in schools and workplaces, and clear
safeguarding concerns used to promote LGBT concern.
Confidentiality, timing and location of services is deemed of greater importance to
LGBT people than having LGBT specific services and all agencies need to review
their service design accordingly.
Health care professionals should be trained in order to raise awareness of LGBT
issues, increase knowledge and skills and to challenge homophobia and
heteronormativity.
The rate of mental distress among the LGBT community is significant and services
need to recognise and develop to suit the needs of LGBT people. Promotion should
target positive mental well-being across LGBT communities.
vi WLGMPService Models
Kingston residents travel outside the Borough to use STI/HIV screening services,
receive HIV treatment, condoms and lube and information and support. Services
within the Borough should be supported to promote their services more effectively
Social groups, LGBT groups, café spaces and counselling services in Kingston should
be promoted and developed as preferred areas where LGBT people can receive
services and one to one interventions.
Intensive one to one behaviour change interventions with those assessed as having
high risk taking behaviour is recommended. There is clearly unmet need around
positive and negative factors influencing safer sex practice that could be capitalised
on to provide positive health outcomes for individuals, particularly MSM.
LGBT service users should be engaged and consulted with to devise creative
solutions to problems identified by improving and developing services.
vii WLGMPKingston upon Thames LGBT Needs Assessment
2 Acknowledgements
Thanks are due to the following individuals and organisations for their assistance with this
needs assessment:
Iain Runcie-Unger, Screening Officer at WLGMP
Amy Leftwich, Sexual Health Promotion Specialist; Julia Waters, Public Health
Programme Lead; Nathalie Wilson, Community Development Worker for
Marginalised Groups; Helen Terry, Senior Worker for Youth Support Services
and Nighat Taimuri at Royal Borough of Kingston upon Thames
Charlie Parker, Chair of Kingston LGBT Forum as well as all members of
Kingston LGBT Forum
Joan Coy, Community Health Specialist Nurse at Your Healthcare CIC
Peter Vittles, LGBT Development Worker at Ealing CVS
Members of the West London Transgender Drop-in Group
West 5 pub in Ealing
K2 Clinic at Wolverton Clinic in Kingston
Special credit and thanks is given to everyone who took time to respond to the questionnaire
and participated in the needs assessment.
viii WLGMPContents
1 Executive Summary ........................................................................................................ii
2 Acknowledgements ...................................................................................................... viii
3 Introduction .................................................................................................................... 1
4 Methodology .................................................................................................................. 2
5 Findings ......................................................................................................................... 4
5.1 Respondents Profile................................................................................................ 4
5.2 Health & Wellbeing ................................................................................................. 9
5.3 Sexual Health Services ......................................................................................... 13
5.4 LGBT Community Services ................................................................................... 15
5.5 Experience ............................................................................................................ 16
5.6 Needs ................................................................................................................... 18
5.7 Focus group .......................................................................................................... 20
6 Conclusion and Recommendations .............................................................................. 23
6.1 Conclusion ............................................................................................................ 23
6.2 Recommendations ................................................................................................ 25
7 References .................................................................................................................. 28
ix WLGMPKingston upon Thames LGBT Needs Assessment List of Table Table 1 Source of participant recruitment .............................................................................. 4 Table 2 Sexual orientation Vs gender identity ....................................................................... 6 Table 3 Venue of preference and sexual identity (%) ............................................................ 7 Table 4 Venue of preference and age groups (%) ................................................................. 8 Table 5 Whom participants had come out/open about sexual/gender identity to ................... 9 Table 6 Non-prescription drug and Sexual orientation ......................................................... 10 Table 7 Gender of sexual partner and sexual identity.......................................................... 11 Table 8 Use of sexual health services inside Kingston ........................................................ 13 Table 9 Occurrence of issues in the last 5 years ................................................................. 16 Table 10 Criteria for choosing a service .............................................................................. 18 Table 11 Interested in accessing particular service ............................................................. 19 List of Figure Figure 1Respondents' connection to Kingston ...................................................................... 4 Figure 3 Sexual orientation of participants ............................................................................ 5 Figure 2 Gender distribution of respondents ......................................................................... 5 Figure 4 Age distribution of respondents ............................................................................... 6 Figure 5 Mental health issue and age group ......................................................................... 9 Figure 6 Numbers of sex partners in the past 6 months and sexual orientation ................... 11 Figure 7 Effect on Safer sex choice..................................................................................... 12 Figure 8 Use of sexual health services inside/outside Kingston .......................................... 14 Figure 9 Use of LGBT services/groups inside/outside Kingston .......................................... 15 x WLGMP
WLGMP
3 Introduction
Sexual health is not equally distributed among the population. There is a strong correlation between
sex orientation and gender identity and STIs/HIV, sexual behaviour and drug use. LGBT people
(particularly MSM) are at greater risk of contracting an STI; building up longer-term physical and
mental health problems; and becoming addicted to alcohol and drugs. The 2006 UK Gay Men’s
Sexual Health Survey by Sigma Research suggests high levels of risky behaviours among MSM in
Kingston. The incidence of syphilis infection among MSM in Kingston was reported the second
highest in the entire South West London network2. Although there is a lack of detailed data
documenting the prevalence of HIV/STIs and new diagnoses within the LGBT community in
Kingston upon Thames, it is believed that these sexual health concerns are mirrored in the West
London area where there are increasing levels of STIs and an increase in the number of HIV
infections among the LGBT population and particularly amongst MSM.
The West London Gay Men’s Project (WLGMP) works to empower individuals and communities to
make positive, informed choices about their sexual health and overall well-being. In undertaking the
Kingston upon Thames LGBT Sexual Health Needs Assessment, WLGMP began a process of
consultation with the LGBT community in order to produce a detailed profile of their health needs
and experiences. It also represents a significant first step in raising awareness of the identified
health needs and experiences of the LGBT community and in making recommendations that will
improve new and existing services so that they are better able to meet the needs of the LGBT
people who live, work, study or socialise in Kingston upon Thames.
Aims of Kingston upon Thames LGBT Sexual Health Needs Assessment
Gather information on the use of sexual health services by LGBT people, what type of
services are accessed and what reasons lie behind their choices
Identify good and bad experiences of LGBT people in order to determine ways to make
sexual health services more inclusive and to encourage LGBT people to utilise the services
offered
Identify current practises by sexual health providers and identify any gaps in knowledge or
service provision
Produce an evaluation report and provide constructive and implementable feedback and
recommendations as to how good practise can be built and advertised
1Kingston upon Thames LGBT Needs Assessment
4 Methodology
This needs assessment was commissioned by the Royal Borough of Kingston upon Thames (RBK).
The project was undertaken over a period of three months, from mid November 2012 to mid
February 2013.
Quantitative Method
A sexual health needs questionnaire was specially designed. This included 32 questions over 10 A5
pages, which were broken down into 6 sections: demographics, health and wellbeing, sexual health
services, community services, experience and needs. A peer review and pilot survey was engaged
prior to the main survey via a small group of LGBT participants to ensure a suitable and user-
friendly questionnaire design.
The questionnaire was administered for a short period between mid November 2012 and the end of
January 2013. Potential respondents to the questionnaire were contacted through:
The contact lists and databases of the WLGMP
Online survey using Google platform, and signposting to the questionnaire via WLGMP’s
website, RBK website and other websites including social media outlets and gay specific
chat sites
Targeted outreach sessions at the Kingston gay club night Escape*, West 5 pub and the K2
clinic, conducted by outreach workers employed by WLGMP
Existing social and support groups and services
Snowballing and word of mouth
*Participants from the outreach sessions were incentivised with a raffle to win a £20 voucher given
out at the end of the night, plus a bag of condoms and lubricant.
Qualitative Method
A special session for the purpose of the needs assessment was held with full support from the
Kingston LGBT Forum on 11 Dec, 2012. The session lasted 30 minutes. All members of the forum
were invited. A total of 12 people participated, with a breakdown as follows:
Gay, bisexual men and men who have sex with men: 8 attendees
Lesbian women: 2 attendees
Not disclosed: 2 attendees, one from local Police force and the other, an employee of
RBK
2WLGMP
During the focus group discussion, three main activities were purposely designed for the needs
assessment, which were:
Issues facing LGBT people
The best and worst designed clinics for LGBT people
Experiences of sexual health services
3Kingston upon Thames LGBT Needs Assessment
5 Findings
125 valid responses to the questionnaire were received (68 via direct submission online and 57
completed paper questionnaires).
Participants were asked how they had first heard about or got hold of the questionnaire. Table 1
details the results.
Table 1 Source of participant recruitment
Source Number %
Email 13 10.4%
Friend 4 3.2%
Health professional 1 0.8%
K2 Gay and Bisexual Men's Clinic at Wolverton Centre 27 21.6%
Kingston LGBT Facebook group 1 0.8%
Kingston LGBT Forum 2 1.6%
Kingston University LGBT Society 1 0.8%
Online 35 28.0%
Outreach worker 27 21.6%
Staff email 1 0.8%
Surrey Comet Newspaper 1 0.8%
West 5 10 8.0%
WLGMP Trans Drop-in Group 2 1.6%
Total 125 100.0%
5.1 Respondents Profile
5.1.1 Connection to the borough
The respondents provide a solid base of LGBT community participants who have strong
associations with Kingston upon Thames. 56.8% (n=71) live in Kingston. Among those who live
outside the borough, 16.0%
(n=20) work or study and 71
80
60
21.6% (n=27) socialise in 55
60
Kingston. Another 5.6% (n=7) 40
40
come to Kingston primarily to
use its health care services. 20 7
Figure 1 shows the 0
respondents’ absolute I live here I socialise I study I use I work
here here health here
connections to Kingston. services
here
Figure 1Respondents' connection to Kingston
4WLGMP
5.1.2 Gender
Of 125 respondents, 82.4% were defined as male and 17.6% as female. 7.2% (n=9) stated that they
had a gender variant experience and 2.4% (n=3) preferred not to state the details.
4.0%
14.4%
Male Female
3.2%
Female without Transgender experience
Female with Transgender experience
Male without Transgender experience
78.4%
Male with Transgender experience
Figure 2 Gender distribution of respondents
5.1.3 Sexual orientation
12.0% of the respondents identified as lesbian, 76.8% as gay, 8.0% as bisexual and 3.2% as otheri.
Figure 3 demonstrates such a composition of our sample and Table 2 displays the gender of
respondents against their declared sexual identity.
Lesbian
8.0%
76.8% 0.8% 0.8% Gay
3.2% Bisexual
0.8% 0.8%
12.0% MSM
Heterosexual
Not sure
N/A
Figure 3 Sexual orientation of participants
i
1 each of MSM (Man who has sex with Men), heterosexual, not sure and not available.
5Kingston upon Thames LGBT Needs Assessment
Table 2 Sexual orientation Vs gender identity
Female
Male without Female with Male with
without
Sexual Orientation Transgender Transgender Transgender
Transgender
experience experience experience
experience
Bisexual 4 22.2% 2 2.0% 2 50.0% 2 40.0%
Gay 0 0.0% 94 95.9% 0 0.0% 2 40.0%
Heterosexual 0 0.0% 0 0.0% 0 0.0% 1 20.0%
Lesbian 13 72.2% 0 0.0% 2 50.0% 0 0.0%
MSM (Man who has sex with men) 0 0.0% 1 1.0% 0 0.0% 0 0.0%
Not sure 1 5.6% 0 0.0% 0 0.0% 0 0.0%
N/A 0 0.0% 1 1.0% 0 0.0% 0 0.0%
Total 18 100.0% 98 100.0% 4 100.0% 5 100.0%
5.1.4 Age
The age of respondents varied from 17 to 70, with a median age of 32. The majority were between
20 and 29 (n=44), followed by those between 30 and 39 (n=31) and between 40 and 49 (n=21).
4.2%
3.4%
11.8%
37.0%WLGMP
5.1.6 HIV status
At the time the questionnaires were collected, 12.0% (n=15) had tested HIV positive, all of which
self-identified as gay, male. 38.4% (n=48) had tested HIV negative within 6 months and 31.2%
(n=39) had tested more than 6 months ago. 14.4% (n=18) had never tested for HIV before; among
which 8 (6.4%) identified as gay male (8% of gay, bisexual men and MSM), 6 (4.8%) as lesbian
female, 3 (3.4%) as bisexual female and one heterosexual transsexual male. There were also 3.2%
(n=4) who were not sure about their HIV status and another participant refused to disclose his HIV
status.
5.1.7 Disability
85.6% (n=107) identified as having no disability. Among the 13.6% (n=17) who identified as having
a disability, including physical illness, such as Arthritis, Dyspraxia, M.E. and Diabetes, and mental
health problems.
5.1.8 Ethnicity
The majority of respondent are from White backgrounds. 49.6% (n=62) were White British; 30.4%
(n=38) were White European including 26.4% (33) Western European and 4.0% (5) Eastern
European; 7.2% (n=9) are from other White backgrounds, such as Irish and South Africa. Mixed or
Minority Ethnic groups were in low numbers with a sum of 12.0% (n=15), which includes 4.8% (6)
Mixed, 3.2% (4) Asian, 1.6% (2) Black, 1.6% (2) Chinese and 0.8% (1) Latino.
5.1.9 Social Preferences
The most popular places for our respondents to socialise and meet people are: social gatherings at
home or visiting friends (66.4%, n=83), general bars & clubs (62.4%, n=78), LGBT exclusive bars &
clubs (56.8%, n=71) and theatre /cinema /restaurants (51.2%, n=64). Table 3 and Table 4 display
comparative analyses of socialising preference between different declared sexual identities and age
groups.
Table 3 Venue of preference and sexual identity (%)
Lesbian Bisexual Gay Heterosexual MSM Not sure Total
Venue
(n=15) (n=10) (n=96) (n=1) (n=1) (n=1) (n=124)ii
Social gatherings at
53.3 70.0 68.8 100.0 0.0 100.0 66.4
home or visiting friends
ii
One respondent did not disclose his sexual orientation.
7Kingston upon Thames LGBT Needs Assessment
Lesbian Bisexual Gay Heterosexual MSM Not sure Total
Venue
(n=15) (n=10) (n=96) (n=1) (n=1) (n=1) (n=124)ii
General bars & clubs 46.7 60.0 64.6 100.0 100.0 100.0 62.4
LGBT exclusive bars &
66.7 60.0 55.2 100.0 0.0 100.0 56.8
clubs
Theatre / Cinema /
46.7 50.0 52.1 100.0 0.0 100.0 51.2
Restaurants
Visit family 20.0 30.0 38.5 100.0 0.0 0.0 35.2
Dating/hook up websites 6.7 30.0 40.6 0.0 0.0 0.0 34.4
Mobile dating apps 0.0 0.0 40.6 0.0 0.0 0.0 31.2
LGBT community
20.0 40.0 20.8 0.0 0.0 100.0 22.4
groups/social groups
LGBT online
26.7 50.0 18.8 0.0 0.0 0.0 21.6
communities
Sport clubs & groups 20.0 40.0 13.5 0.0 0.0 0.0 16.0
General online
6.7 30.0 11.5 0.0 0.0 0.0 12.0
communities
General community
0.0 30.0 9.4 100.0 0.0 100.0 11.2
groups/social groups
Prefer to stay at home 13.3 10.0 11.5 0.0 0.0 0.0 11.2
LGBT specific sport clubs
13.3 0.0 8.3 0.0 0.0 0.0 8.0
& groups
Outdoor groups 0.0 10.0 5.2 0.0 0.0 0.0 4.8
Table 4 Venue of preference and age groups (%)WLGMP
groups
Outdoor groups 0.0 4.5 6.5 4.8 7.1 0.0 5.0
tea shops and pubs 0.0 2.3 0.0 0.0 0.0 0.0 0.8
5.1.10 Disclosure of sexual/gender identity
Apart from one transvestite male and one female who both self-identified as bisexual, most
respondents said they had come out to at least one or some members of their family, friend,
colleague, employer and/or their GP/doctors. Table 5 displays whom they had come out to. It is
noted that a large percentage, 28.4% (n=35) chose not to disclose to their GP/doctor.
Table 5 Whom participants had come out/open about sexual/gender identity to
Yes No Some Not Applicable Total
Family 91 72.8% 15 12.0% 19 15.2% 0 0.0% 125
Friend 107 85.6% 3 2.4% 14 11.2% 1 0.8% 125
Colleague 76 61.8% 14 11.4% 26 21.1% 7 5.7% 123
Employer 83 68.0% 19 15.6% 9 7.4% 11 9.0% 122
GP/ Doctor 74 60.2% 35 28.5% 5 4.1% 9 7.3% 123
5.2 Health & Wellbeing
5.2.1 Mental wellbeing
80.8% (n=101) of the respondents claimed that they had experienced certain mental health issues.
The most common issues include: stress (67.2%, n=84), anxiety (56.8%, n=71) and depression
(54.4%, n=68). Following these, 29.6% (n=37) admitted that they had experienced suicidal thoughts.
Figure 5 demonstrates participants’ mental health issues across different age groups. Younger
respondents had also reported experiences with eating disorders and self-harming.
60-70 1 3 4
Anxiety
50-59 4 6 7 2
Depression
40-49 18 15 2 3 14 8
Eating Disorder
30-39 18 18 6 5 21 8
Self Harm
20-29 26 22 6 8 33 15 StressKingston upon Thames LGBT Needs Assessment
5.2.2 Substance use
5.2.2.1 Smoking
28.8% (n=36) said they smoke, all of whom were under 50 with a median age of 28. Among them,
16% (n=20) stated that they were smoking more than 10 cigarettes a day. This result is much higher
than the national data which reports that the smoking prevalence in England was 20% in 2010 and it
is decreasing3.
5.2.2.2 Alcohol
Respondents were asked how often they drank to levels exceeding the amount that the government
recommends for occasional alcohol consumptioniv. 19.2% (n=24) never drank beyond the
recommended amount. The majority of respondents claimed that they did so on a monthly basis
(24.8%, n=31) or less than monthly (31.2%, n=39). 15.2% (n=19) drank at levels which exceeded
recommended advice every week and 9.6% (n=12) almost daily. This data suggest that more than
24% of the respondents binge drink on at least one day in the week, which is much higher than the
national finding where the same measurement among male and female were 19% and 12%
respectively4.
5.2.2.3 Drugs
A considerable percentage of respondents (39.2%, n=49) said that they used non-prescription drugs
as part of their social or home life. The 2011/12 CSEW national survey estimated one in three
adults (36.5%) had ever taken an illicit drug in their lifetime and 8.9% had used an illicit drug in the
last year5. Finding from this needs assessment suggests noticeably higher rate of drug misuse
among the LGBT community.
The most commonly used drugs include: Amyl nitrate (poppers), Cannabis (grass, spliff), Cocaine,
Viagra or equivalent and Ecstasy. Table 6 lists the details.
Table 6 Non-prescription drug and Sexual orientation
Drug Bisexual Gay Lesbian Heterosexual Total
Amyl nitrate (poppers) 3 34 1 38
Cannabis (grass, spliff) 4 8 3 15
iv
NHS recommends not drinking more than 8 units of alcohol for men (equivalent to 3 pints of strong beer)
and 6 units of alcohol for women (equivalent to 2 pints of strong beer) on one occasion.
10WLGMP
Drug Bisexual Gay Lesbian Heterosexual Total
Cocaine 1 11 1 13
Viagra or equivalent 2 10 12
Ecstasy 2 9 1 12
Mephedrone (meow meow) 6 6
Amphetamines (speed) 3 2 5
Crystal Meth 3 3
Ketamine 3 3
Tranquillisers 2 1 3
5.2.3 Sexual behaviour
5.2.3.1 Sexual partners
34.7% (n=43) had 2 to 4 sexual partners in the past 6 months. 33.1% (n=41) had one sexual partner.
26.4% (n=33) had more than 5 sexual partners (12 among them had more than 11 sexual partners),
of which one participant was a bisexual male and all others were gay males.
100%
0
80%
1
60%
2-4
40%
20% 5-10
0% 11+
Figure 6 Numbers of sex partners in the past 6 months and sexual orientation
As shown in Table 7, some respondents who self-identified as homosexual have sex with partners
of the opposite gender, indicating higher behaviourally bisexual practice.
Table 7 Gender of sexual partner and sexual identity
Not
Partner Gender Bisexual Gay Heterosexual Lesbian MSM N/A Total
sure
All men 2 91 1 1 1 96
All women 1 1 14 16
Equally men and
4 1 5
women
Mostly men 2 3 5
11Kingston upon Thames LGBT Needs Assessment
Not
Partner Gender Bisexual Gay Heterosexual Lesbian MSM N/A Total
sure
Not applicable 1 2 3
Total 10 96 1 15 1 1 1 125
5.2.3.2 Factors affecting safer sex choice
Respondents were given a list of factors that might potentially affect their choice of safer sex
behaviour, i.e. using condoms and/or having less casual sexual partners.
With each of the given factors, the majority of respondents believed that there was no effect at all on
their sexual behaviour. Of those who did note an effect on their sexual behaviour, the top chosen
negative influencing factors, i.e. those which promoted unsafe sexual practices, were: alcohol
(41.6%, n=52), drugs (24%, n=30) and loneliness (22.4%, n=28). Conversely, the top chosen
positive influencing factors, i.e. factors which encouraged participants to practice safer sex, were:
different HIV status of partners (36.8%, n=46), unknown HIV status of partners (30.4%, n=38) and
same HIV status of partners (16%, n=20). Details are displayed in Figure 7.
Alcohol
Drugs
100 Depression
Loneliness
My body image
Partner same HIV status as me
Partner different HIV status to me
Unknown HIV status of partner
Pornography I read/watch
Attractiveness of partner
10 What I want during sex
What my partner wants during sex
Where we are having sex
1
Much less safe Slightly less safe No affect Slightly safer Much safer
Figure 7 Effect on Safer sex choice
12WLGMP
5.3 Sexual Health Services
Respondents were asked how often they used sexual health services provided inside the borough
of Kingston within the past 12 months. 30.4% (n=38) said they never used any of the sexual health
service inside Kingston, 7 of whom never used any sexual health service outside the borough either.
Table 8 displays their answers. According to the responses, the most popular sexual health service
providers for male respondents are: K2 clinic, GUM clinic(s) and Wolverton Centre’s sexual health
service; the most popular sexual health service providers for female respondents are: GPs, family
planning clinics and GUM clinic(s). In addition, three respondents mentioned they had received
sexual health services from Kingston Community Matron HIV, all of whom were HIV positive gay
males.
Table 8 Use of sexual health services inside Kingston
More than 4 Once in Over a
Sexual Health services inside 2-4 times in the
times in the the last year Never
RBKv last year
last year year ago
Genital Urinary Medicine (GUM)
6 15 8 14 72
Clinic
Sexual health service from a GP 1 2 7 6 96
KU19 Young People’s Clinic 3 107
Information and Advice on
1 6 5 102
HIV/AIDS (RBK council HIV team)
Pharmacy Emergency
1 1 3 108
Contraception Scheme
Family Planning Clinics 2 4 106
General services @ Wolverton
Centre for Sexual Health (Kingston 6 12 12 9 77
Hospital)
K2 Gay and Bisexual Men's Clinic
6 25 17 9 62
@ Wolverton Centre
The Point @ Wolverton Centre 2 1 1 109
LARC Contraception Clinic @
2 1 109
Wolverton Centre
The reasons for not using the sexual health services are given below, in order of preference:
I don’t think I need it
I use services outside the borough
Their opening time is not convenient for me
v
The listed services were identified according to the information provided online.
13Kingston upon Thames LGBT Needs Assessment
I don’t know where to go
Their locations are not convenient for me
I am too afraid to go
Just moved into the area
They don’t provide the service I needvi
Many female respondents (50%, n=11) believed that they didn’t need the service. 4 out of the 5
respondents thought there was no in-borough provider for their sexual health needs as a female.
When asked how often they used any sexual health services outside the borough in the past 12
months, the most popular services are STI screening/treatment (44.8%, n=56), HIV
screening/treatment (43.2%, n=54), free condoms (and lube) (38.4%, n=48) and information/support
(23.2%, n=29). Figure 8 demonstrates the overall choice of the respondents.
Over a year ago 60
Once in the last year
2-4 times in the last year 50
More than 4 times in the last year
40
30
20
10
0
Figure 8 Use of sexual health services inside/outside Kingston
vi
Only one respondent detailed the service lacking, which is sexual health physiotherapy for Vestibulodynia
(vulval pain).
14WLGMP
5.4 LGBT Community Services
Only slightly more than a quarter of the respondents (n=32) used the listed LGBT services/groups
provided inside Kingston, which include Kingston University LGBT Society, Kingston LGBT Forum,
Kingston LGBT Support (Mind in Kingston) and Community HIV Matron.
Compared with the above, more responses were gained when asking how often the respondents
used LGBT services/groups outside Kingston. Only 19 (15.2%) claimed they never used any LGBT
services from outside Kingston; 11 of them (8.8%) never used those from inside Kingston either.
Social groups, community groups and condom (and lube) services are slightly more commonly used
than others.
45
40
35
30
25
20
15
10
5
0
Over a year ago
Once in the last year
2-4 times in the last year
More than 4 times in the last year
Figure 9 Use of LGBT services/groups inside/outside Kingston
From those who did not use LGBT services, reasons were given below in order of preference:
I don’t think I need any LGBT specific service/group
I don’t know where to go
The location is not convenient for me
The opening time is not convenient for me
I am afraid to expose my sexual orientation
I don’t want to be seen in the LGBT specific venue
Not interested
Nearly 10% (n=21) said they didn’t know where to seek LGBT services, especially those inside the
borough.
15Kingston upon Thames LGBT Needs Assessment
I've lived in RBK for 40 years and was totally unaware that there are LGBT
services here now! How can this be? What's gone wrong?
5.5 Experience
42.4% (n=53) hadn’t come out to their GP/doctor. 7 out of 9 (77.8%) respondents with transgender
identities hadn’t been given relevant information by a healthcare professional. A large proportion of
respondents (56.8%, n=71) didn’t think that their needs were fully understood by the health staff.
Table 9 lists the details.
Table 9 Occurrence of issues in the last 5 years
Occurrence Yes No Not Sure
Come out to your GP/doctor 49 39.2% 53 42.4% 7 5.6%
Been given information by a healthcare professional
2 1.6% 7 5.6%
relevant to your gender identity?*
Been given information by a healthcare professional
63 50.4% 44 35.2% 5 4.0%
relevant to your sexual orientation?
Felt that your needs weren’t fully understood by the
31 24.8% 71 56.8% 8 6.4%
health staff
Felt that the service you received was negatively
15 12.0% 87 69.6% 7 5.6%
impacted by your sexual orientation or gender identity?
Experienced homophobia from healthcare services? 17 13.6% 90 72.0% 4 3.2%
Experienced transphobia from healthcare services? * 1 0.8% 7 5.6% 2 1.6%
* Answers from respondents identifying with transgender history only.
Questions around experiences with specific problems (e.g. discrimination, negative attitudes) from
listed health care services because of sexual orientation or gender identity were asked. Most of the
respondents (76%, n=95) didn’t have such problems. However, 8.8% (n=11) had some problems
with GP/local health practices and 7.2% (n=9) with NHS hospitals. Some respondents kindly shared
their experiences with us.
After becoming aware of my sexuality, they immediately assumed I was
sexually promiscuous and then started talking about HIV.
I underwent a dental procedure at a local dentist. When I identified that I
was HIV+ the dentist decided to wear three pairs of gloves and was
immensely rude stating: “It may be better if I found another dentist".
I find that when I mention my sexuality it is either not relevant to the issue
being discussed, or just isn't talked about whatsoever. Although I've not
16WLGMP
had a bad experience I find that some doctors have a hard time talking
about it, especially the more mature ones.
More details were given by lesbian respondents:
Assumption of a heterosexual relationship. Staff visibly uncomfortable
when discussing homosexual sexual relationship. Unaware of possible
different needs of a lesbian relationship. Leaflets and information for
heterosexual relationships only.
My sexuality was questioned by a nurse as I was admitted to Kingston
Hospital for surgery. As I was being admitted she questioned a) why I had
a girlfriend and b) why I wanted her to be my ‘in case of emergency’
contact.
Sexual health services not being very helpful/knowledgeable about lesbian
sex health issues, GPs not being understanding/reacting badly about me
being young and gay a few years back, suggesting I might need
counselling.
On the other hand, good experiences were also shared:
Access and support from Dean Thompson Community Nurse with
Medication and other life issues. Easy to contact and approachable. As a
full time worker I use Kingston Aid evening group which is once a month
on a Tuesday evening. Access to support and information when I need it.
Every time I visit here (K2 at Wolverton Centre) it's been great service and
very informative.
Community HIV Nurses very supportive and culturally aware, able to be
very supportive to my specific needs and questions.
Evening drop in service once a month run in Surbiton provides access to
advice and support locally to home without taking time off from work.
Roland and Dean provide support and advice for living and working with
HIV.
17Kingston upon Thames LGBT Needs Assessment
GP has good understanding of my HIV status and no breaches of
confidentiality
My general practitioner is absolutely excellent. She confided with me that
she was not familiar with HIV medicine but would do everything to help.
She also has been great in securing services and as a general support
resource.
Staff at K2 are welcoming, polite and understanding
The (West London) Gay Men’s Project 24's (condom service) and the West
Middlesex Hospital GUM clinic have excellent staff
5.6 Needs
Respondents were asked how important the given criteria were when choosing a service. The most
important consideration is confidentiality and opening time; both were chosen by 91.2% (n=114) of
the respondents. Comprehensive sexual health screening and location were also very important
and were both chosen by 88.8% (n=111) of respondents. Table 10 displays the full list of results.
Table 10 Criteria for choosing a service
Very Not so Doesn’t
Important
important important matter at all
Confidentiality 94 75.2% 20 16.0% 5 4.0% 4 3.2%
Opening time 77 61.6% 37 29.6% 8 6.4% 1 0.8%
Comprehensive sexual health
77 61.6% 34 27.2% 9 7.2% 3 2.4%
screening
Location 68 54.4% 43 34.4% 8 6.4% 2 1.6%
Environment & Atmosphere 59 47.2% 48 38.4% 13 10.4% 3 2.4%
Accessibility 75 60.0% 25 20.0% 15 12.0% 8 6.4%
Visibly welcoming to LGBT people 48 38.4% 42 33.6% 18 14.4% 12 9.6%
Specialised Services 43 34.4% 38 30.4% 31 24.8% 7 5.6%
LGBT specific 31 24.8% 37 29.6% 37 29.6% 15 12.0%
Staff who are LGBT 25 20.0% 29 23.2% 43 34.4% 23 18.4%
Respondents were given a comprehensive list of services at the end of the questionnaire, and
asked to select the ones that they would use if provided in the borough of Kingston upon Thames.
Here is the result arranged in order of preference.
18WLGMP
Table 11 Interested in accessing particular service
Services Number selected %
Social Groups 47 37.6%
Local LGBT groups 44 35.2%
Café Space 44 35.2%
Counselling 42 33.6%
Drop In 39 31.2%
Outdoor activities i.e. walking groups 30 24.0%
Health services 29 23.2%
Drama / Theatre / Music 28 22.4%
Volunteering opportunities 26 20.8%
Safe Meeting Space 25 20.0%
Befriending 25 20.0%
Groups for older people I.e. Over 40, Over 60 25 20.0%
Sporting Activities 23 18.4%
Mental Health Specific Programme or events 22 17.6%
Carers Support / Advice 21 16.8%
Homophobic / Transphobic Crime Support 20 16.0%
Creative Art Projects 19 15.2%
Housing Advice 19 15.2%
Remote Police Reporting to report homophobic incidents 17 13.6%
Self Help Groups (alcohol, disability, weight etc) 17 13.6%
Health Related Workshops 16 12.8%
Alcohol Free Social Space 14 11.2%
Alcohol Education Awareness / Programmes 14 11.2%
Health outreach 14 11.2%
Youth Groups / Age specific Groups 12 9.6%
Internet access 12 9.6%
Lesbian & Bisexual Women’s Health 12 9.6%
Spiritual and/or religious group / support 11 8.8%
Support into work 11 8.8%
Erectile dysfunction clinic 8 6.4%
Immigration/ asylum service 8 6.4%
Ethnic Minority Interest 8 6.4%
Adult Literacy 8 6.4%
Smoking cessation groups 8 6.4%
Dealing with Domestic Abuse 8 6.4%
Advocacy 7 5.6%
Adult Numeracy 7 5.6%
Substance Misuse Awareness / Programmes 7 5.6%
19Kingston upon Thames LGBT Needs Assessment
Services Number selected %
Transgender Health 5 4.0%
Others 4 3.2%
5.7 Focus group
5.7.1 Issues facing LGBT people
The discussion fell into 3 areas: emotional, physical and sexual. More issues were raised when
discussing emotional issues facing LGBT people, which included:
Bullying in schools
Assault and physical threat
Family acceptance / marriage
Coming out at college / to family / workplace (fear of rejection)
Facing prejudice and a lack of understanding
Guilt when living up to family expectations
Parenthood issues
Hurt dealing with homophobia
Battle with religion
Physical issues were discussed around body image and peer pressure to look a certain way and
assault and physical threat.
As is confirmed in Kingston’s 2008 sexual health needs assessment1, the survey found there might
have been a general assumption in the field of sexual health that there has already been plenty of
STI and HIV education; however our participants still expressed concerns about a lack of
appropriate information and unclear answers to certain questions regarding HIV/AIDS stereotypes.
The group agreed to the increasing risk of STI transmission and valued the importance of
awareness of diseases that are specific to LGBT people and the relevant support needed for them.
The discrimination and segregation of LGBT people at clinics, and feeling uncomfortable to discuss
issues with health care professionals were also some of the presenting issues.
5.7.2 The best and worst designed clinics for LGBT people
The suggestions were given as follows:
Best
20WLGMP
Free healthcare including antibiotics
Integrating testing into society (saunas, clubs, coffee shops)
Social, friendly space
Walk-in/ drop-in counselling (no waiting list)
Give results quicker, e.g. lab on site
Home testing/sampling kits more freely available
24/7 clinics
HIV specialist always on site to offer advice and Post-exposure prophylaxis (PEP) / Pre-
exposure prophylaxis (PrEP)
More HIV clinics
PEP/PrEP easily available (only for high risk if no other choices)
Worst
Non person-centred (hidden agendas – e.g. targets)
No website
No drop-in
Judgemental/ blaming staff
Hetero-centric magazines
Difficult to access
Aligning HIV and gay all the time (there’s more to being LGBT than sexual health)
Charging for healthcare
Homophobic / not-aware staff
Assumptions about genders and relationships
Non-trans friendly toilets
Poor confidentiality, not discrete
Just offering one type of condom – no dental dams or lube
Limited opening hours
Badly groomed staff
Dirty/smelly setting
Bad customer service
No outreach
No specific nights
21Kingston upon Thames LGBT Needs Assessment
5.7.3 Experiences of sexual health services
The experiences shared in the group discussion echoed the responses from the questionnaires.
Lacking LGBT awareness is still a common phenomenon among health care services, especially for
lesbians; and homophobia is still experienced.
Both lesbian participants had experienced staff at GPs not being sensitive to the fact that they are
lesbian (with GPs notes reflecting this) and still being asked questions about the possibility of being
pregnant and being recommended contraceptive medication and devices. One woman said that it is
very difficult to find a clinic specifically for lesbians.
One gay man was treated rudely with unhelpful comments from staff after he disclosed his sexual
orientation. Another gay man was told he should attend the clinic on an alternative night specifically
for MSM and was refused entry.
3 people experienced poor confidentiality in the clinic reception areas: being asked their name, date
of birth and sexuality in public.
One man reported when registering with a local GP service that when he spoke of his partner he
was asked his wife’s name. Participants also found it difficult to put down a member of the same sex
as next of kin on medical forms as it is often questioned since it implies not a relative.
22WLGMP 6 Conclusion and Recommendations This report aims to convey the health and well-being needs of a sample of the local LGBT population and establish whether existing health and other services are meeting identified needs, and to make recommendations on how current service provision could be improved and/or enhanced. It must be acknowledged that, due to the small numbers of respondents, this assessment only provides a snap-shot of evidence, which the following conclusions and recommendations are based on. 6.1 Conclusion There was under representation of the bisexual population as the national data suggests that the bisexual population is over half of the gay and lesbian population6. The Lesbian population might have been underrepresented with a ratio of 12%. However, it is generally acknowledged to be difficult to predict the size of this group and the proportion of it. The proportion of respondents with a transgender history was also small, reflecting the lack of visibility of this population. Black, Asian and Minority ethnic LGBT people (7.2% in total) are underrepresented; however this reflects the general ethnic composition of Kingston. There might be a lack representation of White British and a slight over representation of White European groups as the latest national census data suggests 63% of the Kingston population is White British7. The needs assessment highlighted the need to work closely with the current services i.e. GUM clinics, GP and family planning services, in addressing concerns expressed by LGBT service users. The main concern was that the health needs of LGBT people is not fulfilled within the current service structure and clinical pathways. Due to the defined remit and limited amount of time available no data was collected from service providers in this study. Most LGBT respondents were ‘out’ to their friends and fewer individuals were ‘out’ to their GPs or health care professionals. There is a general assumption that gay and bisexual men have already received HIV education, however there were still 8% of gay, bisexual male and MSM respondents who had never tested for HIV before. More than 80% of LGBT respondents had experienced mental health issues. There is strong evidence of a need to support mental well-being amongst this community. 23
Kingston upon Thames LGBT Needs Assessment
The findings regarding high rates of smoking; binge drinking and drug use support the findings in
similar research8. However, given the small size of the sample of the survey it is not possible to
interpret the data in any further depth.
The needs assessment highlights that the majority of LGBT people within Kingston have not heard
of many of the services available, despite many of them being sure of the type of services they
require.
Most LGBT people within this study clearly wanted a higher profile of services. However it is worth
noting that the majority of respondents had previously made use of at least one of the services, with
many respondents indicating that they had used a number of services.
Heteronormativity (presumption of heterosexuality) seemed to be a common negative experience
for service users. Such assumptions/reactions were further highlighted with some experiences from
lesbian respondents. Service providers should re-visit diversity training to be able to better identify
issues that affect LGBT people as required by the Equality Act 2010.
LGBT people socialise in a variety of settings where direct client contact work could be done
successfully, for example bars, clubs and social groups. There is a strong need for services to offer
confidential and comfortable environments for LGBT clients to discuss health issues and
experiences. The respondents raised the importance and value on simply meeting and talking to
each other, gaining support and confidence from others through sharing their experiences.
Use of local LGBT specific services was low with evidence suggesting that people did not want to
engage with LGBT specific services as they did not want to be treated differently. However, low
levels of awareness do suggest a gap in the profile of local services.
Some respondents raised concerns about access to services. It was clear that services needed to
be accessible outside normal working hours i.e. 9am-5pm, particularly sexual health services and
support services. Offering services outside these times will help to increase accessibility for some
potential clients.
There is the possibility that the discrimination in health services not only reduces the control people
have over their own lives; it also reduces access to services and compromises the effectiveness of
services. It is important to remember that no matter how free of prejudice professionals may be, it
may still be rational for LGBT clients to have expectations of inequitable treatment because of a
history of such treatment9.
24WLGMP
6.2 Recommendations
The following recommendations were derived from the findings:
GP and Primary Care
It is essential to improve accessibility and appropriateness of mainstream services.
Mainstream health care providers should revisit diversity training to ensure that it raises
awareness of how to effectively meet the needs of LGBT people, given that 42% of
respondents had not disclosed their sexual identity to their doctor, and 78% of transgender
respondents were offered no relevant information, with 57% saying their needs were not fully
understood.
Health and social care staff should be equipped with the skills to work more sensitively with
their LGBT patients, and adopt a standard of care to ensure that all LGBT people are treated
fairly , appropriately and respectfully. Health and social care professionals should be trained
to focus on the health issues that specifically relate to LGBT people.
Mainstream health care providers should review EVERYTHING YOU ALWAYS WANTED TO KNOW
ABOUT SEXUAL ORIENTATION MONITORING... BUT WERE AFRAID TO ASK, a practice guide to
monitoring sexual orientation commissioned by NHS North West, aimed at the public sector
carrying out monitoring of staff and service users.
Mental health and well-being
Services need to target LGBT people specifically for lifestyle issues, i.e. smoking; alcohol and
drug use. Treating service users holistically will ensure appropriate and effective signposting
and service delivery with better health outcomes for individuals. An assessment of lifestyle
issues at the time of other assessments for risk taking behaviours, e.g. sexual risk taking,
should be integrated into pathways.
Increase access and availability to mental health (i.e. counselling) support. Promotion should
target positive mental well-being across LGBT communities given that 80% of respondents
experienced mental health issues, with 29% having suicidal thoughts. Assessments of
clients’ mental health needs could usefully be integrated into any assessment of their sexual
health need, with robust signposting and referrals pathways identified.
Younger LGBT respondents report higher levels of eating disorders and self harm and
identification of these additional issues need to be worked into individual risk assessments
25Kingston upon Thames LGBT Needs Assessment
when working with this group.
To combat bullying and heteronormactivity, integrate awareness of LGBT rights and health
and well-being issues into school education. This can be delivered by including LGBT specific
resources and signposting and including an LGBT element into general health and well-being
literature.
Sexual Health
With 26% of MSM having 5+ sexual partners in the last 6 months, and 35% having 2 to 4
sexual partners, and 12% of MSM HIV positive there are is clear evidence of sexual health
risk taking behaviour. A one to one behaviour change intervention for high risk MSM,
designed along NICE guidelines for effective interventions could benefit this group.
Sexual Health Promotion needs to be targeted at lesbian and bisexual women as well as gay
men, recognising that they may attend different services to MSM. Service providers should
develop practical strategies that narrow the gap between an understanding of safer sex and
actual practices. It is important to identify, develop and disseminate sexual health information
aimed at lesbian and bisexual women as well as for MSM
Targeted work with the 40% of MSM who use hook up websites or apps to meet other MSM.
This could be via online outreach (Netreach).
Local LGBT specific services are perceived to be very limited. LGBT specific health
promotion in popular venues where LGBT people socialise can raise the profile of the local
LGBT groups and services, and also increase awareness of LGBT health and well-being.
Integration of HIV testing availability into general activities such as saunas, clubs and groups,
and faster test results offered.
Condoms and lubricant are sought outside the borough currently but could be made more
readily available to Kingston residents via sexual health services and 24s condom scheme,
both of which were praised by respondents.
Raise awareness of local LGBT groups and services with LGBT people and other
mainstream services; develop and strengthen service networks in-between. This can be
achieved through many different methods including allowing general health promotion with
LGBT representation and distribution into mainstream outlets/services.
Service Access and integration
26You can also read