Safe use of opioids at Capital & Coast District Health Board (CCDHB) - Caroline Tilah Director (Operations) Quality Improvement and Patient Safety ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
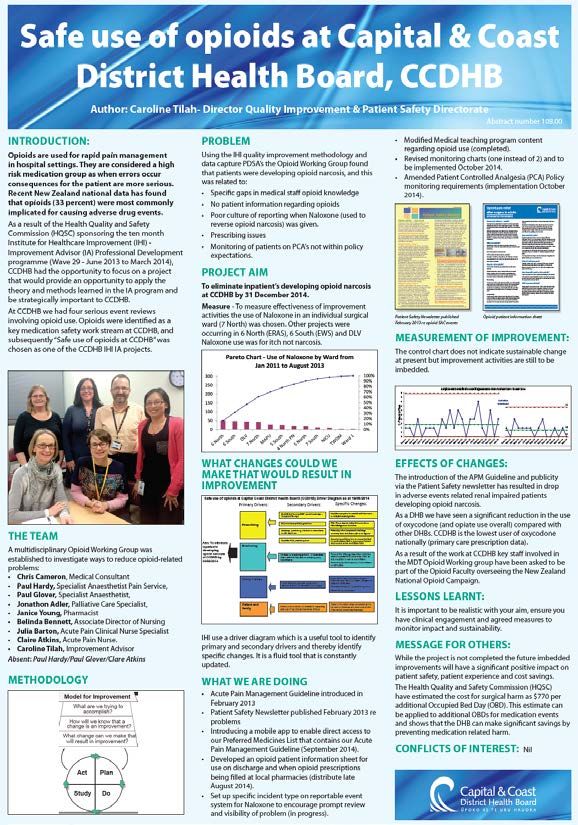
Safe use of opioids at Capital & Coast District Health Board (CCDHB) Caroline Tilah Director (Operations) Quality Improvement and Patient Safety (QIPS) Directorate CCDHB 10/10/2014 Medication Safety Forum
Background
Opioids are used for rapid pain management in hospital settings and
are considered a high risk medication group as when errors are
made there is more likely to be harm, and patient consequences
more serious.
Common opioid medications:
Mild: Codeine/Dihydrocodeine, Tramadol
Stronger: Morphine, Oxycodone, Methadone, Fentanyl
Recent national data has found that opioids (33 percent) were most
commonly implicated for causing adverse drug events.
As such opioids have been identified as a key medication safety
work stream at CCDHB (as well as now nationally).
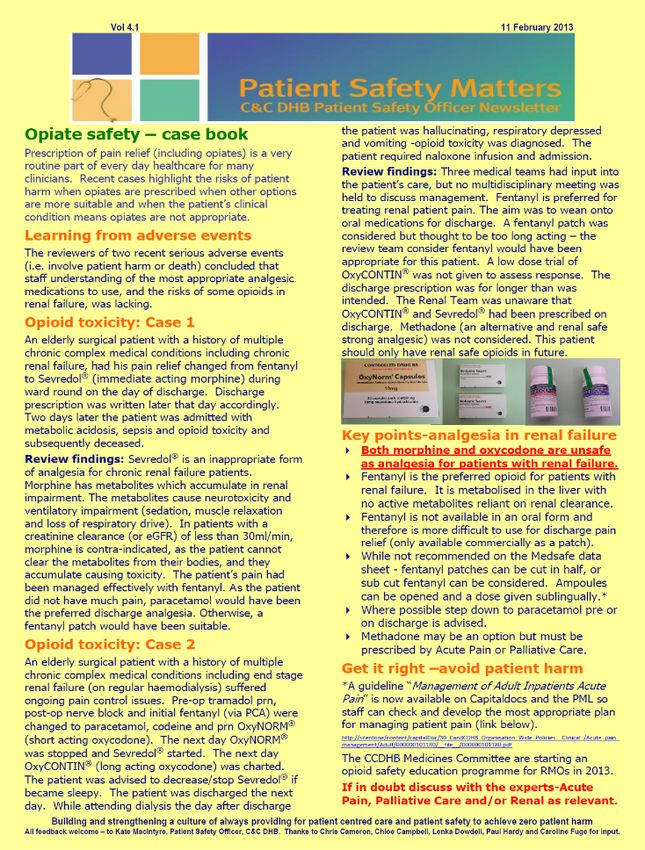
Actions in place at CCDHB early 2013: Patient Safety Opioid newsletter released February 2013 (2 recent SAC2 opioid toxicity events involving patients with renal failure who were not given fentanyl). The release of the “Management of Adult Inpatients Acute Pain” Guideline on PML & Capitaldocs February 2013. The CCDHB Medicine Review Committee starting an opioid safety education programme for RMOs’ 2013.

Opioid MDT Working Group
A MDT working group was established
in August 2013:
• Chris Cameron, Medical Consultant
• Paul Hardy, Specialist Anaesthetist
Pain Service,
• Paul Glover, Specialist Anaesthetist
• Jonathon Adler Palliative Care
Specialist
• Janice Young, Medication Safety
Pharmacist
• Belinda Bennett, Associate
Director of Nursing SWC
• Julia Barton, Acute Pain Clinical
Nurse Specialist
• Claire Atkins, Acute Pain Nurse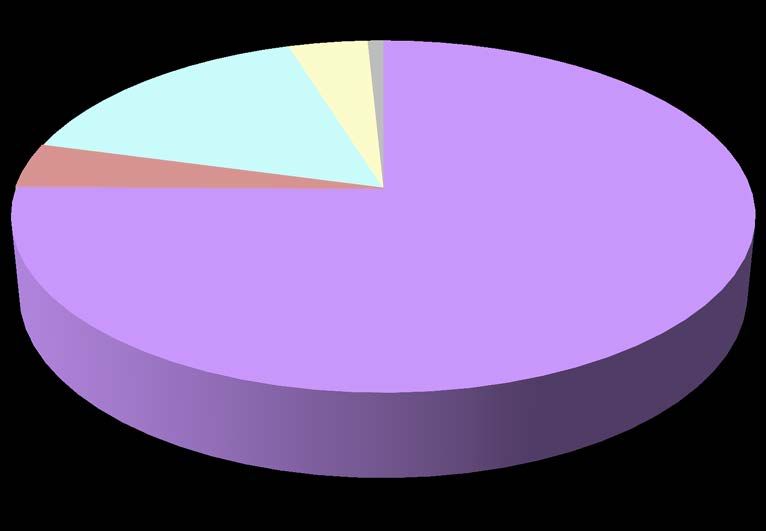
Initial data Plan Do Study Act findings: • Specific gaps in opioid knowledge base by HSO & RMO’s • No patient information regarding opioids given on discharge or by Pharmacies • Had introduced Acute Pain Management Guideline but access via Capitaldocs (More accessible tools available?) • Patents given naloxone for opioid narcosis did not have event routinely documented on discharge summary or a reportable event completed for review • Prescribing - 18% prescriptions did not have an appropriate dose in light of eGFR, multiple opiate use was seen for about 50% of patients prescribed prn opiates, tramadol prn was often prescribed with opiates • Poor monitoring of patient on Patient controlled analgesia (PCA’s) and duplication with monitoring forms • Increased doses of morphine given in the first 24 hours post PACU/Ward
How will we know that any change results in an
improvement?
We had assessed PYXIS naloxone data as the most reliable data source of measurement
data.
Goal To eliminate naloxone use (used to treat
opioid narcosis) on a general surgical
ward (target ward).
Measure Monthly the number of inpatients requiring
naloxone on 7 North.Progress to date: • A mobile app for direct access to our PML • Set up specific incident type on the reportable event system for naloxone. • Modified RMO/HSO teaching programme • Revised EWS to include minimum pain monitoring • Updated separate prescription chart “DO NOT PRESCRIBE PCA MORPHINE IN PATIENTS WITH RENAL IMPAIRMENT”. • Revised minimum requirement for PCA monitoring • Developed a Patient Opioid information sheet (discharge and by the community pharmacy when the script filled).
C Chart showing naloxone use on target ward Feb 11 to September 14 (Baseline for improvements)
Focus for the 3DHB opioid MDT working group for the national opioid collaborative CCDHB prescribing policy states... - All of the medications that a patient is taking at discharge must be documented on the discharge summary. This is so that the GP can reconcile them with his/her list. - Any changes made to the admission list should be specified, with the reason for the change. - A written analgesia plan should be included in the discharge summary for the patient and the GP. - This must be discussed with the patient. Document number: ID 1.1644 Issue Date: 11 April 2013 Review Date: 11 April 2015
Discharge controlled drug prescription audit
• A discharge controlled drug prescription audit was completed by
Emma Henderson (Pharmacy Intern) in July 2014.
• This audit was focussed on the the quality and type of information
documented on the patient’s discharge summary when they receive
a prescription for opiates on discharge.
• Audit was of 107 Discharge Controlled Drug prescriptions issued
over February, 2014 (excluded codeine).
• Data Gathered
– Opiate or concomitant sedating medication before admission,
– Mention of opiate in discharge summary,
– Co-prescribing of potentially sedating medications,
– Opiate-related ED presentation or hospital admission since
dischargeAudit findings • 13% of discharge summaries audited contained no mention of opiate prescribed on discharge • There was a lot of co-prescribing of sedative medications – hard to say if it was clinically inappropriate • Tramadol was the most common sedating medication co-prescribed
Breakdown of opiates prescribed
on discharge over February 2014.
1%
4%
16%
Morphine
4%
Methadone
Fentanyl
75% Oxycodone
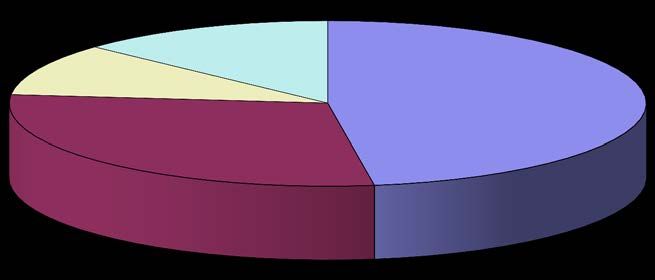
PethidineWhere was the opiate information
mentioned in the discharge
summaries? Mentioned in
Discharge
Medicines List
Mentioned in
13% Discharge
10% 48% Medicines List and
Body of Text
29% Mentioned in Body
of Text only
No Mention
anywhereYou can also read