Sagittal Band Injuries - Gayle Severance MS, OT/L, CHT Good Shepherd Penn Partners
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Sagittal Band Injuries
Gayle Severance MS, OT/L, CHT
Good Shepherd Penn Partners
Philadelphia Hand Meeting
March 2019
Extensor System https://plasticsurgerykey.com/extensor-tendon-injuries/
MCP Joint
Bielefeld T and Neumann DA (2018). Clavero (2003)
❖Shallow joint - Large convex MC head with smaller concaved P1
P1
MC
❖Peri-articular tissue affords joint stability and supports arches of
hand
❖Joint capsule
❖Collateral ligaments
❖Palmer plate
❖Extensor apparatus
❖Sagittal band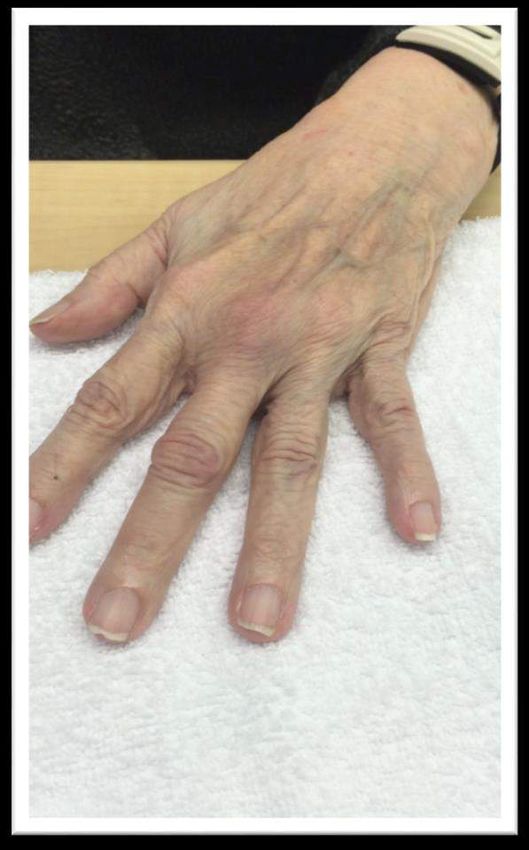
MCP Joint
Bielefeld T and Neumann DA (2018)
❖Motor:
❖FDS/FDP, EDC, lumbricals and interossei
❖Flexion/Ext, ABD/ADD, Pro/Sup, additional
passive joint play in axial plane
❖Function: Allows hand to span across and close
firmly around various size objects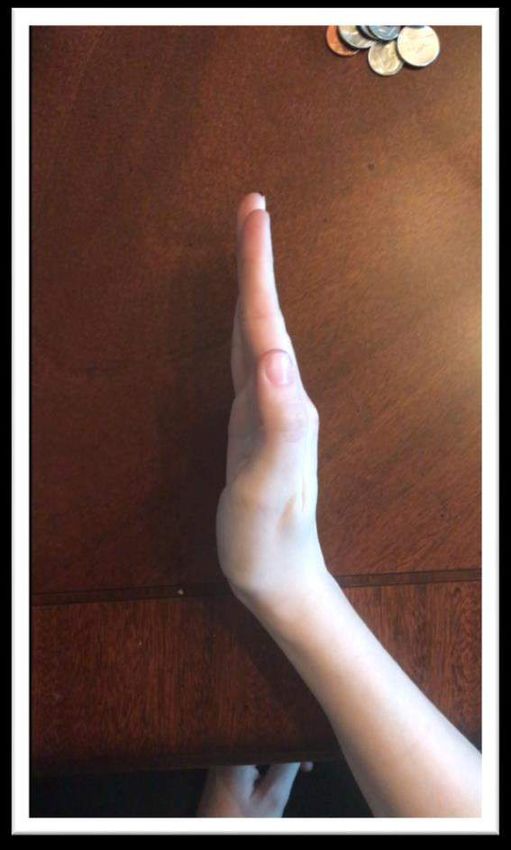
Extensor Digitorum Communis
Kichouh (2009), Kleinhenz (2015)
❖Primary: Extend MCP
❖Secondary: Contributes to wrist, PIP and DIP extension
❖Stabilized over the digit by complex reticular system of the
sagittal, transverse, and oblique bands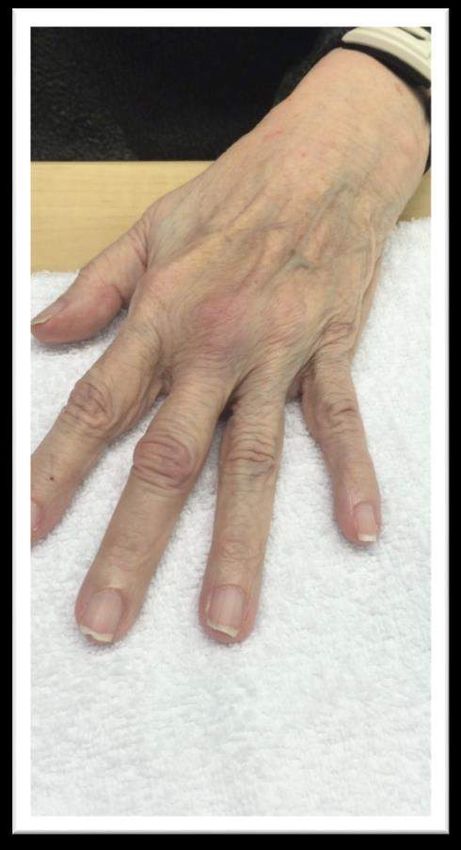
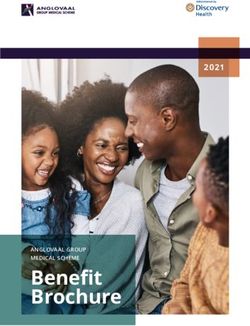
Sagittal Band Anatomy
Kichouch (2009) Castalano (2006), Young (2000), Kleinhenz (2015) Clavero (2003)
❖ Closed cylindrical tube surrounding the MC head and joint and insert palmerly into
the volar plate and deep transverse MC ligament.
❖ Dorsally - the EDC travels through a tunnel made up of a thin superficial layer and a
thick deep layer
❖ A dynamic structure - fibers orient perpendicular to extensor tendons but migrates
proximal to distal along with EDC when the MCP joint is in motion
Purpose of Sagittal Band
❖ Kleinhenz (2015), Kichouh (2009)
❖ Centralize and stabilize EDC tendons over
MCP Head
❖ Resists UD of the tendon especially when the
MCPJ is in flexion
❖ Contributes to digit extension
❖ Prevents tendon bowstringing when the MCP
hyperextends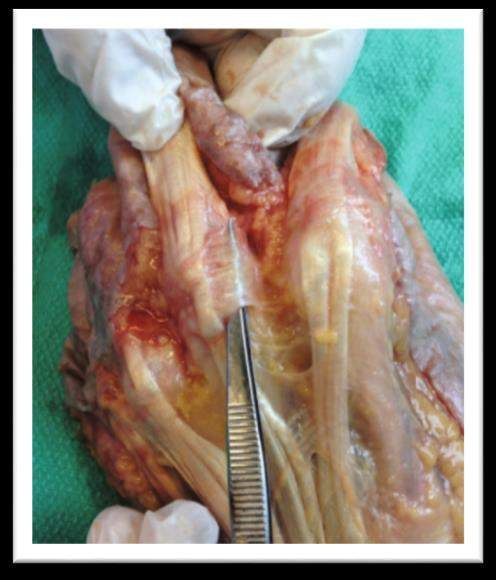
Pathomechanics
Young and Rayan (2000) Farrar (2012)
Ulnar sagittal band Radial sagittal band
• Partial or complete • Distal sectioning - NO
sectioning – NO extensor tendon instability
extensor tendon • >50% Sectioning of
dislocation proximal band – tendon
subluxation
• Unless the JT also
• Complete sectioning -
sectioned tendon dislocation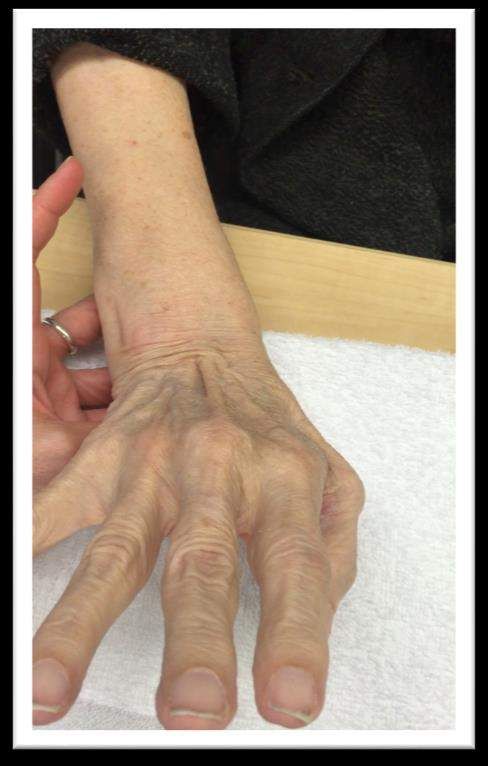
Pathomechanics
Rayan and Murray (1994), Young and Rayan (2000)
✴ Injury – D3>D5>D2>D4
✴BUT
✴ Tendon Instability central > boarder
digits
✴ D3 – least stable
✴ D5 – most stable (due to Junctura
Tendinae) but may develop
abduction deformities
Mechanism of Injury
Stracher (2002) Kleinman (2015)
Acute trauma
✴ Direct impact over dorsal MCP with
clenched fist
✴ Forced finger flexion with wrist flexed
and ulnar deviated
✴ Spontaneous Injury (flicking finger,
crossing finger)Mechanism of Injury
Oversen (1997), Castalano (2006), Kleinhenz (2015) Chinchalkar (2004) Barker 2015)
❖ Chronic attenuation with no trauma
❖ Rheumatoid Arthritis, CTD
❖ Can lead to sequela of events:
Extensor Quadriga
Intrinsic Tightness
Swan Neck DeformitySymptoms
Kleinhenz (2015)
❖Pain, tenderness, swelling over dorsal MPC
❖Pain with MCP motion w/ or w/o resistance
❖Ulnar deviation of digit at MCP joint
❖Tendon snapping with MPC motion
❖Tendon subluxation into intermetacarpal recess
❖Difficulty or inability to initiate digit extension but can
maintain extension
❖ vs EDC laceration - unable to maintain extDifferential Diagnosis
Kleinhenz (2015) Farrar (2012)
Boathouse Row
❖ MCPJ collateral ligament injury – lateral stress to digit, Xray
❖ EDC tendon rupture – inability to initiate AND maintain extension of digit
❖ Trigger finger – palpable mass on flexor tendon
❖ Juncturae tendinum disruption - rare. With USB injury may result in radial
subluxation
❖ MCP joint arthritis – X-ray, pain w/ compression, varus and valgus stress of jointImaging
Kleinhenz (2015)
❖Dx typically through history and physical exam
❖Radiographs
❖stress view to rule out collateral ligament injury
❖Brewerton view
❖Ultrasound (dynamic)
❖When swelling obscures the physical exam
❖MRI
❖may show underlying etiology e.g. synovitis in rheumatoid
arthritisClose SB Injury Classification
Rayan and Murray (1997)
❖ Type I – contusion without tears of SB,
pain, but No extensor tendon instability
❖ Type II – injury with tendon subluxation,
snapping within its borders - tendon
stays in contact with MC condyle
❖ Type III – Injury with tendon dislocation
into the groove between the 2 MC headsIndependence Hall Treatment
Non-Op Treatment (Traumatic)
Castalano (2006) Peelman (2015) Kleinhenz (2015) Merritt (2014)
❖ Type 1
❖ Buddy strap x 4 weeks
❖ Type 2 and 3
❖ Static hand based orthosis
❖ involved MCP 0-30° flexion
❖ RMEO
❖ 15°- 30° (stable)
❖ Combination
❖ Duration: 4-10 weeksNon-Op Treatment
(Nontraumatic/RA)
Chinchalkar SJ and Pitts S (2006) Porter BJ and Brittain A (2012) Bielefeld T and Neumann DA (2005)
Design should consider:
❖All joint deformities and function
❖ wrist, MPs, PIPs, DIPs
❖Deforming forces on lax system
❖ Stress from adjacent digits
❖ Volar subluxation P1 (flex/pulley)
❖ MCP Ulnar drift
❖ Intrinsic tightness
❖ Swan neck and BoutonniereConservative Treatment
Peelman (2015)
❖ 10 yr retrospective review
❖ 92 patients / 101 fingers
❖ 68 Traumatic 24 Atraumatic
❖ Acute >3 weeks (45 patients)
❖ Subacute 3-6 weeks (18 patients)
❖ Chronic wean 2-4 weeks (tx range 3-16 weeks)Conservative Treatment
Peelman (2015)
❖94% success rate for acute and subacute pt (6 weeks from onset)
❖Persistent subluxation occurred in atraumatic > traumatic
❖Increased with chronicity
Conservative tx may be warranted with sign of active collagen turnover
(inflammation)Surgical Options
Kleinhenz (2015)Post op Early Active Program
RMEO
Merritt (2014)
❖ Increasing use of RMO in hand tx
❖ Wear duration: 0-3 days post op to 6 wks
❖ AROM in confines of orthosis
❖ >6 wk - Wean to buddy strapping PRN
❖ Relatively little therapy neededPost Op Treatment
“Protective”
❖ Immediate post op:
❖ Cast or Orthosis; blocking MCP 30
❖ AROM of IP joints
❖ 3-4 weeks
❖ MCP blocking orthosis
❖ Isolated MCP flexion (Table top)
❖ Scar and edema mgmt
❖ 6 weeks
❖ Wean from orthosis
❖ Full fist
❖ No composite wrist/digit flexionCase 1: Post op Rehab ❖22 yo male collegiate baseball player torqued non-dom MF sliding into base ❖Surgical repair using slip of the EDC ❖POD 2: ❖RMEO (day), HB static MCP ext (night), ROM w/in RMEO ❖POD 12: ❖orthosis adjustment, scar mgmt ❖Minimal edema, full IP ROM, pain 3/10 ❖Week 6: Buddy strapping MF/IF ❖MCP: Hyper 5/55, pain 1/10 ❖Issued all TGE ❖Week 8: Abd/Add, FMC, light isometrics ❖MCP: H5/75, pain 1/10 ❖Pt did not return after 4th visit (Moved)
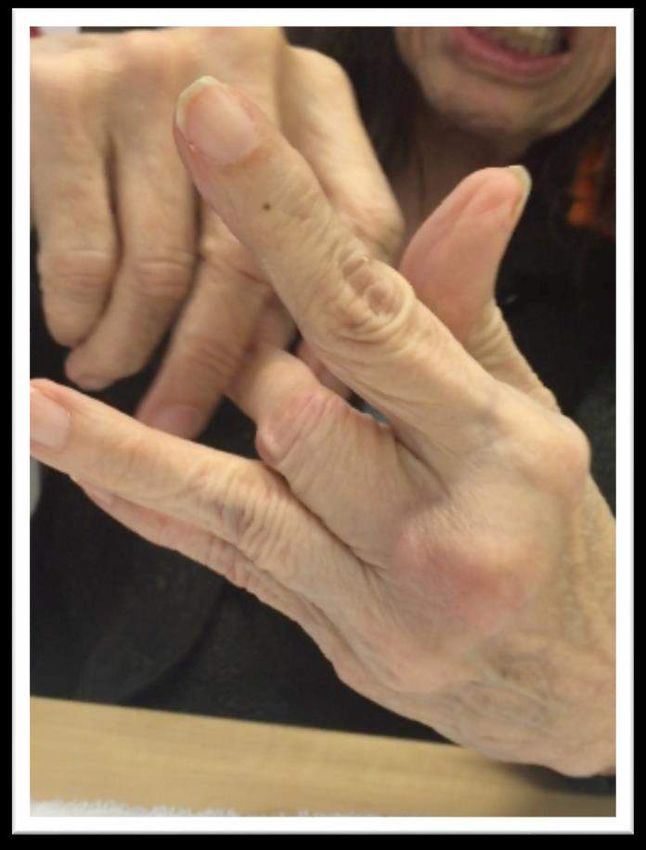
Case 2: Non-op ❖ 70 y.o. female ❖PMI: significant for Parkinson's (no RA) ❖Fx: assistance from caregivers, w/c, walker short distances, grab-bars ❖Treated by OT for general ADL deficits related to Parkinsons ❖New Rx from PCP for “trigger finger and hand contracture” ❖Orthosis: ❖ night - resting hand (MCP flexion, IP ext) ❖ day - PIP blocking orthosis
Case 2
Summary • Sagittal Band disruptions are uncommon but can be painful and functionally limiting • RSB results in subluxation > USB • Positive results with conservative treatment, especially in acute • Conservative and post-operative treatment guidelines are similar • Growing popularity and successful results with RMEO, caution use with RA, RA like conditions/deformities • Require little therapy unless there are secondary complications like extensor quadriga and intrinsic tightness
Thank you!
References
• Chinchalkar SJ. Pitts S. Dynamic assisted splinting for the attenuated sagittal bands in the rheumatoid hand. Techniques in Hand and Upper Extremity Surgery.
2006; 10(4)206-2011.
• Porter BJ. Brittain A. Splinting and hand exercises for there common hand deformities in rheumatoid arthritis: a clinical perspective. Curr Opin Rheumatol. 2012;
24:215-221.
• Bielefeld T. Neumann DA. The unstable metacarpalphalangeal joint in rheumatoid arthritis: Anatomy, pathomechanics, and physical rehabilitation considerations.
J Ortho Sport Phys Ther. 2005; 35(8):502-520.
• Kleinhenz BP. Adams B. Closed sagittal band injuries of the metacarpophalangeal joint. J Am Acad Ortho Surg. 2015; 23(7): 415-423.
• Castalano LW. Et. al. Closed treatment of the nonrheumatoid of extensor tendon dislocations of the metacarpophalangeal joint. J of Hand Surg (Am). 2005: 31(2)
242-245.
• Peelman, J., Markiewitz, A., Kiefhaber, T., & Stern, P. Splintage in the treatment of sagittal band incompetence and extensor tendon subluxation. J Hand Surgery
(Euro). 2015; 40(3), 287–290.
• Rayan GM. Murray D. et. al. The extensor retinacular system at the metacarpophalangeal joint: an anatomical and histalogical study. J Hand Surg (Br). 1997; 22(5):
585-590.
• Chichalkar SJ, Gan BS. McFarlane RM et. al. Extensor quadrigia: pathomechanics and treatment. Canadian Journal of Plastic Surgery. 2004: 12: 174-177.
• Young CM. et. al. Sagittal Band. Anatomical and biomechanical study. J Hand Surg. 2000; 25(6): 107-1113.
• Kichouh M. et. al. Functional anatomy of the dorsal hood of the hand: correlation of ultrasound and MRI findings in cadaveric dissections. 2009; 9(8): 1849-1856.
• Stracher M. Posner M. Boxer’s Knuckle. Tech Hand and UE Surg. 2002; 6(4): 196-199.
• Farrar NG. Kundra A. ISRN Orthopaedics. Role of juncturae tendinum in preventing radial subluxation after ulnar sagittal band rupture: a cadaveric study. 2012.
• Merritt WH. Relative motion splinting after extensor tendon injury and repair. J Hand Surg. 2014; 39(6); 1187-1194.
• Clavero JA et. al. Extensor mechanism of the fingers: MR imaging-anatomical correlation.Radiographics. 2003 May-June:23(3): 593-611.You can also read