Should zinc be used for COVID-19 prophylaxis or treatment? A rapid review version 1; peer review: awaiting peer review
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Wellcome Open Research 2020, 5:188 Last updated: 18 JAN 2021
SYSTEMATIC REVIEW
Should zinc be used for COVID-19 prophylaxis or treatment? A
rapid review [version 1; peer review: awaiting peer review]
Oghenekome A. Gbinigie 1, Ralph K. Akyea 2
1Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, OX2 6GG, UK
2Primary Care Stratified Medicine Research Group, University of Nottingham, Nottingham, NG7 2RD, UK
v1 First published: 07 Aug 2020, 5:188 Open Peer Review
https://doi.org/10.12688/wellcomeopenres.16173.1
Latest published: 07 Aug 2020, 5:188
https://doi.org/10.12688/wellcomeopenres.16173.1 Reviewer Status AWAITING PEER REVIEW
Any reports and responses or comments on the
Abstract article can be found at the end of the article.
Background: There have been intensive efforts worldwide to
establish effective treatments for coronavirus disease 2019 (COVID-
19), with recent interest in the use of zinc as a potential therapeutic
agent. The aim of this rapid review was therefore to critically appraise
and evaluate the evidence for using zinc as prophylaxis and/or
treatment for COVID-19.
Methods: We conducted electronic searches on 20th and 21st May
2020 of PubMed, TRIP, EPPI COVID Living Map, MedRxiv, Google
Scholar and Google. All searches were updated on 11th July 2020 to
check for new relevant studies. We included in vivo studies assessing
the safety and effectiveness of zinc, alone or combined with other
interventions, as treatment or prophylaxis for COVID-19. Studies
assessing the activity of zinc against SARS-CoV-2 in vitro were also
included.
Results: We identified one observational study with a high risk of bias
that was suitable for inclusion. The study authors found that
treatment with a combination of zinc, azithromycin and
hydroxychloroquine in patients hospitalised with COVID-19 resulted in
increased odds of being discharged home (adjusted odds ratio (OR)
1.53; 95% CI 1.12 to 2.09; p = 0.008) and reduced odds of death or
being transferred to a hospice (adjusted OR 0.559; 95% CI 0.385 to
0.811; p = 0.002), compared with treatment with hydroxychloroquine
and azithromycin.
Conclusions: We identified extremely limited evidence from a study
with methodological problems of an association between
improvement in certain outcomes when COVID-19 patients are
treated with a combination of zinc, hydroxychloroquine and
azithromycin, compared with treatment with hydroxychloroquine and
azithromycin. The results of randomised clinical trials in this area
should provide robust evidence of the effectiveness of zinc as
treatment/prophylaxis for COVID-19.
Keywords
COVID-19, coronavirus, zinc
Page 1 of 9Wellcome Open Research 2020, 5:188 Last updated: 18 JAN 2021
This article is included in the Coronavirus
(COVID-19) collection.
Corresponding author: Oghenekome A. Gbinigie (oghenekome.gbinigie@phc.ox.ac.uk)
Author roles: Gbinigie OA: Conceptualization, Formal Analysis, Funding Acquisition, Investigation, Methodology, Project Administration,
Supervision, Validation, Visualization, Writing – Original Draft Preparation, Writing – Review & Editing; Akyea RK: Formal Analysis,
Funding Acquisition, Investigation, Methodology, Project Administration, Validation, Visualization, Writing – Review & Editing
Competing interests: OAG is in receipt of funding from the Wellcome Trust. RKA is in receipt of funding from the National Institute for
Health Research School for Primary Care Research (NIHR SPCR).
Grant information: This work was supported by the Wellcome Trust through a Clinical PhD Fellowship to OAG [203921]. RKA is funded
by a National Institute for Health Research School for Primary Care Research (NIHR SPCR) PhD Studentship award. The views expressed
are those of the authors and not necessarily those of the NIHR, the NHS, or the Department of Health.
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Copyright: © 2020 Gbinigie OA and Akyea RK. This is an open access article distributed under the terms of the Creative Commons
Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly
cited.
How to cite this article: Gbinigie OA and Akyea RK. Should zinc be used for COVID-19 prophylaxis or treatment? A rapid review
[version 1; peer review: awaiting peer review] Wellcome Open Research 2020, 5:188
https://doi.org/10.12688/wellcomeopenres.16173.1
First published: 07 Aug 2020, 5:188 https://doi.org/10.12688/wellcomeopenres.16173.1
Page 2 of 9Wellcome Open Research 2020, 5:188 Last updated: 18 JAN 2021
Introduction 2020. Additional searches were conducted in Google and
Whilst efforts to develop novel treatments for coronavirus Google Scholar on 21st May 2020 (see extended data for link to
disease 2019 (COVID-19). are ongoing, a number of existing search strategy14). All of the searches were re-run on 11th
treatments have been re-purposed to try to treat this disease1,2. July 2020. We stopped searching Google and Google Scholar
One such candidate treatment is zinc. when we reached a page with no results relevant to this
review. Searches were limited to studies published from 2019
Zinc is a micronutrient primarily obtained through dietary con- onwards. The authors performed title and abstract screening and
sumption. Rich sources of zinc include oysters, red meat, poultry, full text screening independently for separate sets of databases.
beans, nuts and fortified cereals3. It is estimated that 20% The authors independently determined studies that were suit-
of the population worldwide are at risk of zinc deficiency4. able for inclusion in the review, with disagreements resolved by
Zinc has a number of functions including helping to maintain discussion.
proper functioning of the immune system5.
We included in vitro studies assessing the activity of zinc, alone
or combined with other treatments, against SARS-CoV-2. We
There is evidence that treatment with zinc may improve outcomes
included in vivo studies assessing the safety and effectiveness
in some viral infections. In a meta-analysis of 12 studies
of treatment or prophylaxis with zinc, alone or combined with
of children aged under five years, the authors found that zinc
other interventions, for COVID-19. We included studies that
supplementation for at least three months resulted in an 8%
provided data to allow comparisons to be made between
reduction in the incidence rate of respiratory illness compared
patients who did, and did not, receive zinc. We included par-
with placebo (pooled rate ratio 0.92; 95% CI 0.85 to 0.99)6.
ticipants of all ages and genders. No study setting or language
When the results of eight trials of high dose zinc supplementa-
restrictions were imposed. For inclusion, studies needed to
tion (greater than 75 mg zinc per day) were pooled in a systematic
report clinical and/or laboratory outcome data, such as time to
review by Hemila, there was a significant reduction in the
recovery and viral load. Systematic reviews were used as a
duration of common colds, compared with placebo7.
source of reference.
The mechanism by which zinc might inhibit severe acute respi- Forward citation and reference screening were performed on
ratory syndrome coronavirus 2 (SARS-CoV-2) activity is uncer- the included study. Both authors independently extracted data
tain. In an in vitro study, Te Velthuis and colleagues assessed from the included study and performed a risk of bias assessment
the activity of SARS-CoV in Vero-E6 cells, when the cells using the GRADE criteria15, with disagreements resolved
were treated with zinc and pyrithione8. Pyrithione is a zinc through discussion.
ionophore, facilitating zinc ion transport across cell membranes
into the intracellular space. The authors found that there was Results
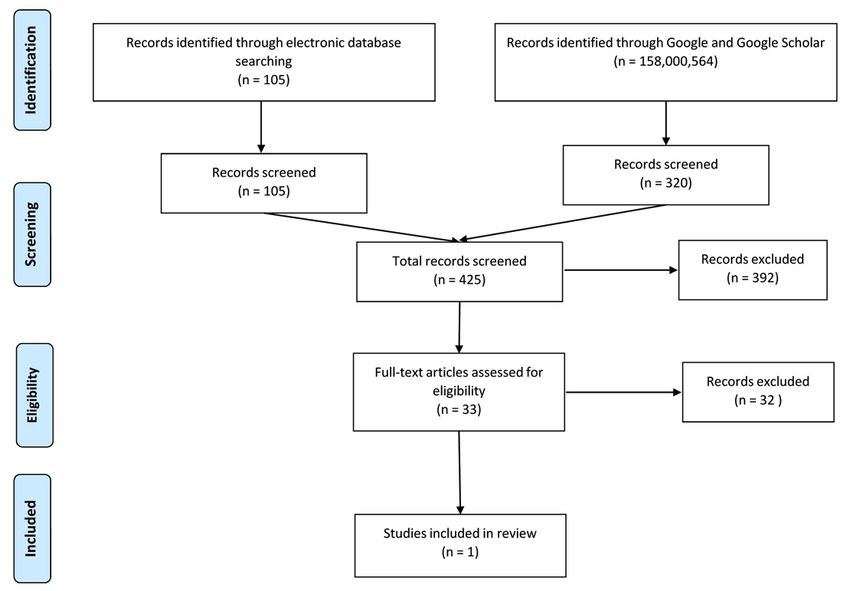
an additive inhibitory effect on SARS-CoV replication when Electronic database searches on 20th May 2020 identi-
Vero-E6 cells were treated with zinc combined with pyrithione, fied 105 studies. The first seven pages (70 links) of Google
compared with treatment with either zinc or pyrithione alone. Scholar were searched, and the first 25 pages of Google
Furthermore, the authors found that treatment of isolated were searched (250 links). After title and abstract screen-
SARS-CoV RNA-dependent RNA polymerase with zinc inhib- ing, 33 eligible studies were identified. Of these, one study was
ited viral RNA synthesis in a dose-dependent fashion. Given suitable for inclusion in this review16. All searches were re-run
that there is 79% genomic homology between SARS-CoV and on 11th July 2020, and no further studies suitable for inclusion
SARS-CoV-29, it is possible that zinc may have a similar effect on were identified (see Figure 1 - flow diagram for study inclu-
SARS-CoV-2. sion). The included study was rated as very low quality according
to the GRADE criteria (see Table 1).
In vitro studies have shown that zinc deficiency is linked to an
increase in levels of certain pro-inflammatory cytokines such The study, conducted by Carlucci and colleagues, was a retro-
as TNF-alpha and IL-810,11. It is, therefore, possible that zinc spective observational study assessing the clinical outcomes
deficiency could exacerbate the cytokine storm seen in some of patients hospitalised with COVID-19 in four New York
cases of COVID-19, which can in turn trigger acute respiratory hospitals16 (see Table 2). On 25th March 2020, clinicians in
distress syndrome. these hospitals added zinc to their usual treatment regime
of hydroxychloroquine (HCQ) and azithromycin (AZT) for
There are reports of clinicians using zinc as a treatment, com- COVID-19 patients. The authors compared the outcomes of
bined with other drugs, for COVID-1912. Donald Trump has 411 patients receiving a combination of HCQ (400 mg OD
also reported taking zinc as part of a COVID-19 prophylaxis followed by 200 mg BD orally for five days), AZT (500 mg
regime13. In light of this, it is important to establish whether there OD orally, duration not reported) and zinc (220 mg BD orally
is evidence to support this approach. The aim of this review is to for five days), with 521 patients receiving HCQ and AZT
evaluate the evidence for the safety and effectiveness of zinc for without zinc. The authors excluded patients who were addition-
COVID-19 treatment and/or prophylaxis. ally receiving other experimental COVID-19 treatments, such as
lopinavir/ritonavir.
Methods
Electronic database searches were conducted in PubMed, After adjusting their analyses for patient admission after 25th
TRIP, MedRxiv and EPPI COVID Living Map on 20th May March 2020, the authors found that the addition of zinc to
Page 3 of 9Wellcome Open Research 2020, 5:188 Last updated: 18 JAN 2021
Figure 1. Flow diagram showing the process for identification of study suitable for inclusion.
Table 1. GRADE evidence profile for the included study.
Quality assessment of evidence
Review authors’ judgements
↓ Inconsistency in some p-value estimates in the baseline table of the study.
Inconsistency
For instance, comparing respiratory rates and white blood cell count in of the included study.
Indirectness ↔ No limitation
↓ Relatively few events for some outcomes to establish an association e.g. number expired/transferred
Imprecision
to a hospice, numbers needing intensive care, and numbers needing mechanical ventilation.
↓ High – failure to adjust for possible confounders that were different between the groups such as
Risk of Bias
respiratory rate, baseline systolic blood pressure and lymphocyte count.
Quality grading Very low
GRADE: Grades of Recommendation Assessment, Development and Evaluation
↓ -downgraded; ↔ -neither upgraded nor downgraded
HCQ and AZT resulted in significantly increased odds of transferred to a hospice (adjusted OR 0.559; 95% CI 0.385 to
being discharged home (adjusted odds ratio (OR) 1.53; 95% 0.811; p = 0.002). However, they found that the addition of
CI 1.12 to 2.09; p = 0.008) and reduced odds of death or being zinc did not significantly reduce the need for intensive care
Page 4 of 9Wellcome Open Research 2020, 5:188 Last updated: 18 JAN 2021
Table 2. Characteristics of included study.
Authors (Year) Carlucci et al., 2020
Country USA
Setting NYU Langone Health hospitals
Number of
932; with zinc (n=411); without zinc (n=521)
participants
Mean age (SD) With zinc (63.19 ± 15.18); without zinc (61.83 ± 15.97)
Sex, Females With zinc (n=147, 35.7%); without zinc (n=201, 38.6%)
Patients who were admitted to the hospital with at least one positive test for COVID-19,
Inclusion criteria received hydroxychloroquine and azithromycin, and were subsequently discharged
from the hospital, transitioned to a hospice, or died
Patients who were never admitted to hospital or receiving other investigational
Exclusion criteria
therapies for COVID-19
• H
ydroxychloroquine (400 mg once followed by 200 mg PO BID for five days) and
azithromycin (500mg once daily) plus zinc sulphate (220 mg PO BID for five days) or
Treatment
• Hydroxychloroquine (400 mg once followed by 200 mg PO BID for five days) and
azithromycin (500mg once daily)
Addition of zinc associated with:
• Increased odds of being discharged home
• Decreased odds of mortality/transfer to a hospice
Addition of zinc not associated with:
Findings • Length of hospitalisation
• Duration of mechanical ventilation
• Need for invasive ventilation
• ICU duration
• Need for ICU
Abbreviations: BID: bis in die; ICU: Intensive Care Unit; SD: standard deviation; USA: United States of America
(adjusted OR 0.733; 95% CI 0.471 to 1.14; p = 0.168) nor the some significant differences between the two groups that were
need for invasive ventilation (adjusted OR 0.804; 95% CI 0.487 not adjusted for in their analyses, including systolic blood
to 1.33; p = 0.396). The addition of zinc to HCQ and AZT was pressure, troponin and lymphocyte count. It is possible that
also not associated with a change in the length of hospitalisa- adjusting for these possible confounders may lead to differ-
tion, the duration of mechanical ventilation nor the duration of ent results. Propensity score matching of observational studies17
time spent in the intensive care unit (p values of 0.646, 0.667 and randomisation of clinical trials are means of ensuring that
and 0.504, respectively). The authors conclude that the addi- baseline characteristics between groups are similar. We did not
tion of zinc to HCQ and AZT may have some therapeutic benefit identify any clinical trials assessing the use of zinc as treatment
for COVID-19 patients. or prophylaxis for COVID-19 that were suitable for inclusion.
However, we have identified more than a dozen clinical tri-
There are, however, some important points that must be con- als registered to this purpose on the WHO International Clinical
sidered. The study design is observational; we cannot use Trials Registry Platform (ICTRP)18 (see Table 3).
these results to make causal inferences about the effect of zinc
on outcomes in COVID-19 patients. The observed associa- Discussion
tions provide some information about zinc when combined with We identified very limited evidence from a single observa-
HCQ and AZT, but do not provide information about zinc as a tional study with a high risk of bias of an association between
standalone treatment. The authors do not report baseline lev- treatment with a combination of zinc, HCQ and AZT in hos-
els of zinc in patients, hence, we cannot tell whether this might pitalised COVID-19 patients and increased odds of being
have influenced the observed associations. discharged home and reduced odds of death or being transferred
to a hospice, compared with treatment with a combination of
The authors adjusted their analyses for date of admission to HCQ and AZT. The study found no association between tri-
hospital. However, the baseline characteristics and hospi- ple treatment with zinc, HCQ and AZT and reduced need for
tal medications of the study participants show that there were intensive care or invasive ventilation, compared with HCQ
Page 5 of 9Wellcome Open Research 2020, 5:188 Last updated: 18 JAN 2021
Table 3. Registered COVID-19 zinc-related studies registered on the WHO International Clinical Trials Registry
Platform (ICTRP) – updated on 16th July 2020.
Recruitment
Trial ID Scientific title Status Countries
A prospective, single centre, randomized open labelled
comparative clinical study to evaluate the effectiveness
ACTRN12620000454976 of Siddha medicine, Kabasura kudineer and vitamin Not Recruiting Australia
c-zinc supplementation in the management of
asymptomatic COVID 19 patients.
A Randomised Controlled Trial of Early Intervention in
Patients HospItalised with COVID-19: Favipiravir verses
NCT04326725 Recruiting Turkey
HydroxycholorquiNe & Azithromycin & Zinc vErsEs
Standard CaRe - PIONEER
A randomized open labeled clinical study to compare
the effectiveness of Kabasura kudineer and Vitamin-C
NCT04351490 Not recruiting France
Zinc supplementation in the management of
asymptomatic SARS-CoV-2 patients
A Randomized Study Evaluating the Safety and Efficacy
of Hydroxychloroquine and Zinc in Combination With United
EUCTR2020-001449-38-GB Not recruiting
Either Azithromycin or Doxycycline for the Treatment of Kingdom
COVID-19 in the Outpatient Setting
A Randomized, Double-Blind, Placebo-Controlled Phase
NCT04377646 IIa Study of Hydroxychloroquine, Vitamin C, Vitamin D, Not recruiting Tunisia
and Zinc for the Prevention of COVID-19 Infection
A Study of Hydroxychloroquine and Zinc in the
Iran (Islamic
IRCT20180425039414N2 Prevention of COVID-19 Infection in Military Healthcare Recruiting
Republic of)
Workers (COVID-Milit)
A study on melatonin and Vitamin C and zinc efficacy
United
NCT04342728 in patients with COVID19 hospitalized in intensive care Recruiting
States
unit of Semnan Kowsar Hopsital
Coronavirus Disease 2019- Using Ascorbic Acid and
United
NCT04370782 Zinc Supplementation (COVIDAtoZ) Research Study A Recruiting
States
Randomized, Open Label Single Center Study
COVID-19 Prophylaxis With Hydroxychloroquine
NCT04384458 Associated With Zinc For High-Risk Healthcare Workers Not recruiting Brazil
Involved In Suspected, or Confirmed Cases of COVID-19.
COVID-19 Prophylaxis with hydroxychloroquine,
Vitamin D, and Zinc supplementation in Danish nursing Iran (Islamic
IRCT20151228025732N52 Not Recruiting
home residents - a randomized controlled trial - COVID- Republic of)
19 PREVENTION
Does Zinc Supplementation Enhance the Clinical
NCT04407572 Efficacy of Chloroquine/Hydroxychloroquine in Not recruiting Turkey
Treatment of COVID-19?
Effect of a Combination of Nitazoxanide, Ribavirin and
NCT04447534 Ivermectin Plus Zinc Supplement on the Clearance of Recruiting Egypt
COVID-19: a Pilot Sequential Clinical Trial
Efficacy and safety of Hydroxychloroquine,
Azythromycine and Zinc for the treatment of patients United
NCT04335084 Recruiting
with SARS-Cov2 infection in Senegal: a dose ranging States
randomised trial. COVID-19
Evaluating the immune boosting ability of a
homoeopathic therapeutic strategy involving a nosode
Tuberculinum 1M, followed by Zincum Metallicum
PACTR202005622389003 Not Recruiting Senegal
6C, Chininum Arsenicosum 6C and Calc Phos 6x in
asymptomatic novel corona virus disease (Covid-19
illness) vulnerable risk group.
Page 6 of 9Wellcome Open Research 2020, 5:188 Last updated: 18 JAN 2021
Recruitment
Trial ID Scientific title Status Countries
High-dose intravenous zinc (HDIVZn) as adjunctive
CTRI/2020/05/025215 therapy in COVID-19 positive critically ill patients: A pilot Not Recruiting India
randomized controlled trial
Impact of Zinc and Vitamin D3 Supplementation on the
CTRI/2020/07/026340 Survival of Institutionalized Aged Patients Infected With Not Recruiting India
COVID-19
Proflaxis for Healthcare Professionals Using
Hydroxychloroquine Plus Vitamin Combining Vitamins
NCT04468139 Recruiting Saudi Arabia
C, D and Zinc During COVID-19 Pandemia: An
Observational Study
Prospective study to assess therapeutic role of Zinc in
NCT04472585 Recruiting Pakistan
COVID-19 patients
Australia;
Sub-cutaneous Ivermectin in Combination With
United
and Without Oral Zinc and Nigella Sativa: a Placebo
ACTRN12620000557932 Not Recruiting States of
Randomized Control Trial on Mild to Moderate COVID-19
America;
Patients
Germany
The effect of zinc on the treatment and clinical course
NCT04392427 Not recruiting Egypt
of patients with SARS-cov2 (COVID-19)
The Study of Quadruple Therapy Zinc, Quercetin,
NCT04395768 Bromelain and Vitamin C on the Clinical Outcomes of Not recruiting Australia
Patients Infected With COVID-19
COVID-19 Prophylaxis with hydroxychloroquine,
Vitamin D, and Zinc supplementation in Danish nursing
EUCTR2020-001363-85-DK Not Recruiting Denmark
home residents – a randomized controlled trial -
COVID-19 PREVENTION
A randomized open labeled clinical study to compare the
effectiveness of Kabasura kudineer and Vitamin-C Zinc
CTRI/2020/06/025874 Not Recruiting India
supplementation in the management of asymptomatic
SARS-CoV-2 patients
Zinc Vitamin D and b12 Levels in the Covid-19 Positive
CTRI/2020/06/026045 Not Recruiting India
Pregnant Women
and AZT. Furthermore, there was no association with the treat- intra-cellular uptake of zinc when the A2780 cells were treated
ment regime including zinc and a change in the length of with zinc combined with chloroquine, compared with zinc
hospitalisation, the duration of mechanical ventilation nor the alone. Moreover, they found that chloroquine encouraged accu-
duration spent in intensive care. We did not identify any stud- mulation of zinc in certain intracellular organelles such as
ies evaluating the use of zinc as a standalone treatment for lysosomes. The authors also found that chloroquine combined
COVID-19, nor zinc (alone or in combination) as COVID-19 with zinc enhanced the ability of chloroquine to cause cell
prophylaxis. apoptosis, compared with chloroquine alone. These in vitro study
findings provide support for the purported synergy between
Comparison with existing literature chloroquine (and its derivatives) and zinc, as suggested by
There is some in vitro evidence that chloroquine and HCQ Carlucci et al16. However, in vitro studies cannot fully replicate
have anti-SARS-CoV-2 activity19–21. However, some believe conditions inside the human body and we cannot infer that these
that the primary function of these drugs in COVID-19 is to findings would be replicated in vivo.
act as a portal of entry for zinc into cells, allowing zinc to
inhibit SARS-CoV-2 activity22. Xue and colleagues report that In a pre-print, Derwand and colleagues24 report the results
chloroquine is a zinc ionophore in an in vitro study23. The authors of a retrospective case series of patients in the community in
added zinc alone, and zinc combined with chloroquine to the New York State who tested positive for COVID-19. In total,
extracellular medium of A2780 cells (human ovarian cancer 141 consecutive patients - who were aged over 60 years,
cell line). They found that there was significantly increased aged 60 years and below and experiencing breathlessness, or
Page 7 of 9Wellcome Open Research 2020, 5:188 Last updated: 18 JAN 2021
were aged 60 years and below, were symptomatic and had at Implications for clinical practice and research
least one co-morbidity - received triple therapy with zinc sulfate In light of the extremely limited evidence identified, and
220 mg once a day, HCQ 200 mg twice a day and AZT 500 mg the methodological flaws outlined above, there is insuffi-
once a day. The control group comprised independent public cient evidence to recommend that clinicians prescribe zinc for
reference data for 377 COVID-19 positive patients in the same COVID-19 treatment or prophylaxis outside of clinical trials.
community who received usual care. The authors found that tri- The included study used secondary care data, thus, we did
ple therapy was associated with significantly reduced odds of not identify any evidence for the use of zinc in primary care
hospitalization (OR 0.16; 95% CI 0.06 – 0.5; p < 0.001) and a settings. We are aware of 24 studies, mostly clinical trials,
non-significant reduction in all-cause mortality (OR 0.2; 95% which have been registered to investigate the effectiveness of
CI 0.03 – 1.5; p = 0.16). zinc as COVID-19 treatment/prophylaxis. Some of these stud-
ies are being conducted in primary care settings. The results of
However, no demographic data, clinical characteristics or well-conducted, randomised, adequately powered clinical trials
co-morbidities were available for the control group; it is should provide primary and secondary care clinicians with
therefore not possible to tell whether the treated group and definitive evidence for the effectiveness of zinc as a COVID-19
controls were comparable. Furthermore, the authors report that therapeutic/prophylactic agent. It is critically important that
triple therapy was ‘well tolerated,’ yet 21% of treated patients these clinical trials report safety data. Zinc supplementa-
(30/141) reported adverse events, including weakness, gas- tion can cause gastrointestinal side effects such as nausea and
trointestinal side effects and rashes. No safety data was vomiting, diarrhoea, gastritis, and dysgeusia26,27.
available for the control group. Of note, this study provides
some information about zinc in combination with HCQ and
Conclusion
AZT. It does not, however, provide information about zinc as
There is extremely limited evidence of poor quality that treat-
a standalone therapy, nor does it tell us whether the addition
ment of hospitalised COVID-19 patients with a combination
of zinc to HCQ and AZT has an additive benefit compared with
of zinc, HCQ and AZT is associated with increased odds of
dual treatment with HCQ and AZT.
being discharged home and reduced odds of death or being trans-
ferred to a hospice, compared with treatment with HCQ and
Strengths and limitations
AZT combined. We did not identify any evidence for the use of
We believe that there are considerable strengths to this rapid
zinc as prophylaxis for COVID-19, nor as a standalone treatment.
review. We conducted the review quickly to facilitate timely
The results of clinical trials including zinc in the intervention
dissemination of the findings, with less than a week between
regimens should provide definitive evidence of the effectiveness
the searches being updated and the review being submitted
and safety of this treatment in the context of COVID-19.
for publication. We used a broad search strategy to maximise
capture of relevant studies. We also searched pre-print servers
and Google/Google Scholar to increase our chances of capturing Data availability
grey literature. Underlying data
All data underlying the results are available as part of the article
However, we recognise the limitations of this rapid review. and no additional source data are required.
Given the rapid pace at which COVID-19 studies are being
published, it is possible that we may have missed studies rel- Extended data
evant to this review, particularly studies not published in Figshare: Search strategy - “Should zinc be used for COVID-19
English. We tried to minimise this risk by not applying any prophylaxis or treatment? A rapid review”. https://doi.org/10.6084/
language restrictions to our eligibility criteria. Furthermore, m9.figshare.12728432.v114
whilst we adhered closely to the methods used in a system-
atic review (see reporting guidelines for link to PRISMA This project contains the following extended data:
checklist25), we did not perform dual screening at the title and - A ppendix_1_zinc_search_strategy_Wellcome_Open_
abstract or full-text screening stages. Research.docx (Study search strategy)
We also recognise significant limitations of the identified
Reporting guidelines
evidence. We identified a single study, with high risk of bias,
Figshare: PRISMA checklist for ‘Should zinc be used for
assessing the use of zinc as a treatment in combination with
COVID-19 prophylaxis or treatment? A rapid review’ https://doi.
other interventions for COVID-19. We cannot use this data to
org/10.6084/m9.figshare.12730532.v125
make any assertions about zinc as a standalone treatment, nor
as prophylaxis for COVID-19. The study data came from four
hospitals in New York; we do not know whether the observed Data are available under the terms of the Creative Commons
associations are generalizable to other populations. The authors Zero “No rights reserved” data waiver (CC0 1.0 Public domain
did not report baseline levels of zinc. If zinc does have favour- dedication).
able effects in COVID-19, this benefit may be influenced by
the zinc status of the individual, with zinc replete patients
benefitting less from zinc supplementation. Finally, the Acknowledgments:
study was published as a pre-print and has not been formally We would like to thank Nia Roberts (Specialist Librarian) for
peer-reviewed. her help with search terms for the database searches.
Page 8 of 9Wellcome Open Research 2020, 5:188 Last updated: 18 JAN 2021
References
1. Gbinigie K, Frie K: Should chloroquine and hydroxychloroquine be used to 15. Guyatt GH, Oxman AD, Vist GE, et al.: GRADE: an emerging consensus on
treat COVID-19? A rapid review. BJGP Open. 2020; 4(2): bjgpopen20X101069. rating quality of evidence and strength of recommendations. BMJ. 2008;
PubMed Abstract | Publisher Full Text | Free Full Text 336(7650): 924–6.
2. Gbinigie K, Frie K: Should azithromycin be used to treat COVID-19? A rapid PubMed Abstract | Publisher Full Text | Free Full Text
review. BJGP Open. 2020. 4(2): bjgpopen20X101094. 16. Carlucci P, Ahuja T, Petrilli CM, et al.: Hydroxychloroquine and azithromycin
PubMed Abstract | Publisher Full Text | Free Full Text plus zinc vs hydroxychloroquine and azithromycin alone: outcomes in
3. National Institutes of Health Office of Dietary Supplements: Zinc Fact Sheet for hospitalized COVID-19 patients. medRxiv. 2020.
Health Professionals. 2020. Publisher Full Text
Reference Source 17. Austin PC: An introduction to propensity score methods for reducing the
4. Kumssa DB, Joy EJ, Ander EL, et al.: Dietary calcium and zinc deficiency risks effects of confounding in observational studies. Multivariate Behav Res. 2011;
are decreasing but remain prevalent. Sci Rep. 2015; 5: 10974. 46(3): 399–424.
PubMed Abstract | Publisher Full Text | Free Full Text PubMed Abstract | Publisher Full Text | Free Full Text
5. Wessels I, Maywald M, Rink L: Zinc as a gatekeeper of immune function. 18. World Health Organization: International Clinical Trials Registry Platform
Nutrients. 2017; 9(12): 1286. (ICTRP).
PubMed Abstract | Publisher Full Text | Free Full Text Reference Source
6. Aggarwal R, Sentz J, Miller MA: Role of zinc administration in prevention of 19. Yao X, Ye F, Zhang M, et al.: in vitro Antiviral Activity and Projection of
childhood diarrhea and respiratory illnesses: a meta-analysis. Pediatrics. Optimized Dosing Design of Hydroxychloroquine for the Treatment of
2007; 119(6): 1120–30. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin Infect
PubMed Abstract | Publisher Full Text Dis. 2020; 71(15): 732–739.
PubMed Abstract | Publisher Full Text | Free Full Text
7. Hemilä H: Zinc lozenges may shorten the duration of colds: a systematic
review. Open Respir Med J. 2011; 5: 51–8. 20. Liu J, Cao R, Xu M, et al.: Hydroxychloroquine, a less toxic derivative of
PubMed Abstract | Publisher Full Text | Free Full Text chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro. Cell
Discov. 2020; 6(1): 16.
8. Te Velthuis AJW, van den Worm SH, Sims AC, et al.: Zn2+ inhibits coronavirus
PubMed Abstract | Publisher Full Text | Free Full Text
and arterivirus RNA polymerase activity in vitro and zinc ionophores block
the replication of these viruses in cell culture. PLoS Pathog. 2010; 6(11): 21. Wang M, Cao R, Zhang L, et al.: Remdesivir and chloroquine effectively
e1001176. inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell
PubMed Abstract | Publisher Full Text | Free Full Text Res. 2020; 30(3): 269–71.
PubMed Abstract | Publisher Full Text | Free Full Text
9. Lu R, Zhao X, Li J, et al.: Genomic characterisation and epidemiology of 2019
novel coronavirus: implications for virus origins and receptor binding. 22. Derwand R, Scholz M: Does zinc supplementation enhance the clinical
Lancet. 2020; 395(10224): 565–74. efficacy of chloroquine/hydroxychloroquine to win todays battle against
PubMed Abstract | Publisher Full Text | Free Full Text COVID-19? Med Hypotheses. 2020; 142: 109815.
PubMed Abstract | Publisher Full Text | Free Full Text
10. Wessels I, Haase H, Engelhardt G, et al.: Zinc deficiency induces production
of the proinflammatory cytokines IL-1β and TNFα in promyeloid cells via 23. Xue J, Moyer A, Peng B, et al.: Chloroquine is a zinc ionophore. PLoS One. 2014;
epigenetic and redox-dependent mechanisms. J Nutr Biochem. 2013; 24(1): 9(10): e109180.
289–97. PubMed Abstract | Publisher Full Text | Free Full Text
PubMed Abstract | Publisher Full Text 24. Derwand R, Scholz M, Zelenko V: COVID-19 outpatients–early risk-stratified
11. Bao B, Prasad AS, Beck FW, et al.: Zinc modulates mRNA levels of cytokines. treatment with zinc plus low dose hydroxychloroquine and azithromycin: a
Am J Physiol Endocrinol Metab. 2003; 285(5): E1095–E102. retrospective case series study.
PubMed Abstract | Publisher Full Text Publisher Full Text
12. Gusoff C: Coronavirus Drug Exclusive: Meet The Doctor Behind The 25. Gbinigie O, Ralph A: PRISMA_checklist_zinc_for_COVID_ 19_Rapid_review.
Hydroxychloroquine Treatment, And What’s Next For Its Use. 2020. figshare. Figure. 2020.
Reference Source http://www.doi.org/10.6084/m9.figshare.12730532.v1
13. The Telegraph: Inside Donald Trump’s anti-coronavirus cocktail. 2020. 26. Singh M, Das RR: Zinc for the common cold. Cochrane Database Syst Rev. 2013;
Reference Source (6): CD001364.
14. Gbinigie O, Ralph A: Search strategy - “Should zinc be used for COVID-19 PubMed Abstract | Publisher Full Text
prophylaxis or treatment? A rapid review”. figshare. Figure. 27. British National Formulary: Zinc Sulfate: National Institute for Health and
2020. Care Excellence.
http://www.doi.org/10.6084/m9.figshare.12728432.v1 Reference Source
Page 9 of 9You can also read