SOUTH AFRICA - Real-Time Assessment (RTA) of UNICEF's Ongoing Response to COVID-19 in Eastern and Southern Africa
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Real-Time Assessment (RTA) of
UNICEF’s Ongoing Response to
COVID-19 in Eastern and
Southern Africa
Case Study:
SOUTH
AFRICA
Key highlights from a real-time
assessment based on qualitative data Photo credit: UNICEF/2020/Simons Meyer
Kandi Shejavali
January 2021
RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
Preface
UNICEF’s Eastern and Southern Africa Regional Office (UNICEF ESARO) commissioned
Oxford Policy Management (OPM) to carry out a Real-Time Assessment (RTA) of UNICEF’s
response to COVID-19 in countries in the region.
This report outlines the findings from the South Africa country case study, drawing on the
qualitative data gathered during the course of interviews with key informants. In line with the
‘light-touch’ nature of the overall RTA and respecting the maximum length of 3,600–4,000
words, the report provides an overview of the findings, emerging themes, and lessons to be
learned. The report format follows the outline provided by UNICEF ESARO for regional
reports, adapted for a country-level analysis.
The RTA team includes the following members: Jayne Webster (Team Leader), Rashid
Zaman (Project Manager), Elizabeth Harrop (Adviser – Gender and Social Protection),
Georgina Rawle (Adviser – Education), Bilal Hakeem (RTA Coordinator), Kandi Shejavali
(Monitoring and Evaluation (M&E) Expert), Deogardius Medardi (M&E Expert), Lauren
Mueenuddin (M&E Expert), Denis Tiren (M&E Expert), and Nicola Wiafe (Research Analyst).
Kandi Shejavali drafted this report, which was then reviewed by members of the project
leadership.
We are grateful to UNICEF ESARO’s evaluation section, specifically to Urs Nagel, Bikul
Tulachan, and Yasmin Almeida, for their invaluable collaboration and guidance on the
conceptualisation, design, and technical delivery of the RTA work. In addition, UNICEF
consultant Karen Hickson provided useful inputs.
Furthermore, for the specific purposes of this case study:
• The invaluable support of UNICEF South Africa colleagues cannot go unmentioned.
Without the persistent efforts of Fulufhedzani Ravele, with the active support of Ben-
Albert Smith, Janine Simon Meyer, and other members of the team under the
leadership of Muriel Mafico, data collection for the case study would have been
impossible to complete within Phase I of the RTA. We also thank Kgaugelo Flora
Mojapelo for making available the images that bring visual life to this report.
• Most crucially, we thank the key informants for their time, for sharing their
perspectives and insights with such earnestness and passion, and for their work,
which seeks to make a meaningful, positive difference in the lives of South African
residents, notably those who are most vulnerable and most excluded. That such
important work is being carried out by individuals with such dedication to what they do
is heart-warming.
ii
RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
Executive summary
Introduction
This case study of the UNICEF response to COVID-19 in South Africa, where 1,004,413
COVID-19 cases and 26,735 deaths have been recorded as at 27 December 2020,1
The study forms part of a broader real time analysis (RTA) of UNICEF’s COVID-19 response
in eastern and southern Africa. The RTA was ‘light touch’, with a tight timeline. Due to this,
only a small sample of stakeholders were interviewed, and it was not possible to include
beneficiaries. The broad sectoral focus also precluded in-depth analysis. The research was
undertaken in December 2020.
Qualitative data collection, in the form of 16 key informant interviews (KIIs), was undertaken
was undertaken alongside a limited review of documentation and a survey of wider UNICEF
Country Office staff. The research aimed at answering four overarching questions: (i) how
has the UNICEF South Africa Country Office (SACO) adapted to the COVID-19 pandemic
and to evolving needs?; (ii) how can the implementation and quality of the Country Office’s
(CO’s) COVID-19 response be characterised?; (iii) what are the emerging themes?; and (iv)
what are the early lessons?
Themes emerging from the findings
Notable positives include the following:
• Adaptation in the COVID-19 response: the adoption of new methods to assess and
meet community needs; establishing a brand-new Water, Sanitation, and Hygiene
(WASH) programme; recognition of the importance of re-establishing SACO’s
Communication for Development (C4D) capacity; the CO expanding its geographic
footprint to meet expanded needs; the establishment of new partnerships, including
strategic public–private partnerships; the strengthening and acceleration of social
protection/social development efforts; and strong internal coordination.
• Implementation of the COVID-19 response: UNICEF SACO contributed to offsetting
the negative effects of the pandemic on access to basic services across all programme
areas. There has been successful coordination and programme delivery in the education
sector; and establishment of trust-based relationships with partners. The CO has also
been successful in reaching some pockets of the most vulnerable segments of the
population, ensuring gender equity and ownership in the process; and adherence to
programming standards and protocols. Furthermore, there has been upholding of the
spirit of community engagement/ Accountability to Affected People (AAP) - an approach
that was lauded by various respondents.
• Ability to assure quality in the COVID-19 response: Despite the challenges posed by
COVID-19, UNICEF SACO adhered to processes and verification systems used to
ensure quality.
Challenges encountered in the South Africa CO’s response to COVID-19:
• In terms of adaptation, there has been a lack of adequate resources to meet the need.
1Government of South Africa's COVID-19 Online Resource and News Portal, update of 27 December 2020,
available at https://sacoronavirus.co.za/2020/12/27/update-on-covid-19-27th-december-2020/ (last accessed 28
December 2020).
iii
RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
• In terms of implementation: Some sub-groups of women and children in need went
unsupported; there was inadequate communication (on SACO’s part) with implementing
partners; and insufficient pre-existing preparedness and contingency planning.
• In terms of quality: UNICEF SACO arrived on the national scene late and was unable to
consistently ensure programme delivery on a timely basis.
In terms of which populations were particularly vulnerable in the medium to long term as
a result of COVID-19, respondents noted that COVID-19 has amplified the needs of the
same populations that have always been known to be vulnerable in the South African
context.
Lessons learned/ suggested action points
Based on their perspective of emerging challenges, and considering the broader objective of
the RTA, respondents offered the following suggestions to inform UNICEF South Africa’s
programming in the medium to long term:
• Support to catch-up campaigns for children will be necessary, particularly in terms of
schooling and immunisations.
• Support economic development – ‘because if parents aren’t working then children aren’t
eating’ – and efforts to address youth unemployment.
• Support learners at all educational levels, including ensuring that those with disabilities
are targeted.
• Continue to encourage behaviour change to limit COVID-19 transmission – there is ‘a lot
of work to be done there’.
• Integrate COVID-19 considerations into ongoing health programming (by, for example,
establishing guidelines for dispensing medication for chronic conditions to cover longer
periods and thus limiting the need to visit health facilities).
• Integrate health messaging, specifically nutrition messages, into settings that go beyond
the health silo, such as in transportation hubs.
In addition, the following action points proposed by the RTA assessors might be considered:
OPERATIONS
1. UNICEF SACO should preposition itself and its partners for emergency situations. As
suggested by one respondent, the Emergency Preparedness Platform (EPP) should be
simulated at regular intervals and the CO should ensure that preparedness is in place.
2. UNICEF should consider revisiting its decision-making hierarchy and other internal
processes to ensure timely delivery of appropriate programming.
3. Consolidate and maintain partnerships, particularly innovative public–private partnerships
and institutional frameworks for coordination and continued engagement.
4. Deepen communication with partners to ensure transparency and for the sake of
coordination and the building of trust.
PROGRAMMING
5. Re-establish WASH and Communication for Development (C4D) as a permanent part of
the SACO programme and strengthen and accelerate related interventions, particularly
messaging on prevention.
iv
RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
6. Maintain and advance innovative ‘edutainment’ (education in the form of entertainment)
approaches in messaging.
7. Cement multi-dimensional/-sectoral/-faceted, empowerment-based approaches across
programming, especially in the area of social development. Partners and frontline
workers believe that this type of holistic community engagement ‘creates not just hope
but a sustainable future’.
8. Produce learning materials in indigenous languages to facilitate continued learning for all.
v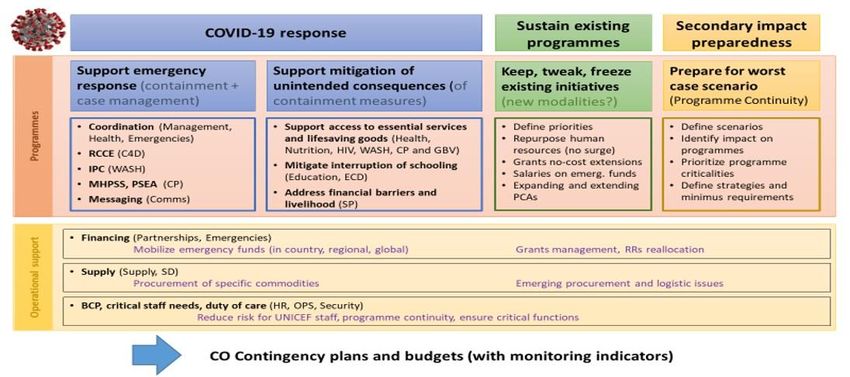
RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
List of abbreviations
AAP Accountability to Affected People
C4D Communication for Development
CO Country Office
EPP Emergency Preparedness Platform
ESA Eastern and Southern Africa
ESAR Eastern and Southern Africa Region
ESARO Eastern and Southern Africa Regional Office (of UNICEF)
GBV Gender-Based Violence
KII Key Informant Interview
M&E Monitoring and Evaluation
OPM Oxford Policy Management
PMTCT Prevention of Mother-to-Child Transmission
PPE Personal Protective Equipment
RCCE Risk Communication and Community Engagement
RTA Real-Time Assessment
SACO South Africa Country Office (of UNICEF)
SSOP Simplified Standard Operating Procedures
WASH Water, Sanitation, and Hygiene
WHO World Health Organization
vi
RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
Table of contents
1 Introduction.............................................................................................................1
1.1 Background ...................................................................................................1
1.2 Case study scope, approach, and methods ...................................................1
1.3 Regional context in relation to the COVID-19 epidemic .................................2
1.4 Summary of the impact of COVID-19 in South Africa ....................................2
2 Findings ..................................................................................................................3
ADAPTATION .............................................................................................................4
2.1 How UNICEF SACO has adapted....................................................................4
IMPLEMENTATION ....................................................................................................5
2.2 Effectiveness of UNICEF’s response to COVID-19 in South Africa ............5
2.2.1 Offsetting the negative effects of COVID-19 on access to basic services 5
2.2.2 Reaching the most vulnerable and ensuring equity 6
2.2.3 Meeting programming standards and protocols 7
2.2.4 Ensiring and sustaining community engagement/ AAP mechanisms 7
2.3 How UNICEF SACO has utilised preparedness and contingency planning ...8
2.4 What is known about needs and how UNICEF determined these .................8
QUALITY ..................................................................................................................9
2.5 What we know about the quality of the UNICEF response to COVID-19..........9
2.5.1 Effects of the crisis on UNICEF’s ability to deliver quality 9
2.5.2 Timeliness of UNICEF response to COVID-19 10
2.5.3 How UNICEF South Africa ensured the quality of the response 10
3 Emerging themes/ conclusions ...........................................................................11
3.1 Emerging positives from UNICEF South Africa’s performance in the COVID-
19 response ................................................................................................11
3.2 Challenges encountered in UNICEF South Africa’s implementation of the
COVID-19 response ....................................................................................12
3.3 Medium- to long-term implications for vulnerable children and communities 13
3.4 (Re)focusing UNICEF’s programming to reach vulnerable children .............14
4 Lessons learned/ suggested action points .........................................................16
Annexes
A.1 Countries in eastern and southern Africa with UNICEF COs .......................17
A.2 UNICEF response to COVID-19 in ESAR ....................................................18
A.3 Interviewees South Africa ……………………………………………………….21
A.4 RAG Rating: South Africa ............................................................................21
B.1 KII Guide for UNICEF Country Offices.........................................................24
B.2 KII Guide for UNICEF Partners....................................................................26
B.3 KII Guide for Frontline Workers ...................................................................28
B.4 Standard introduction and consent (all interviews).......................................30
vii
RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
1 Introduction
1.1 Background
Global context: Following evidence of rapid and widespread transmission of COVID-19, the
World Health Organization (WHO) declared the disease a global pandemic on 11 March 2020.
COVID-19 is ‘an unprecedented global crisis, causing high mortality, morbidity, social disruption,
and economic [hardship]’.2 As at 28 December 2020, the worldwide total of confirmed cases was
almost 80 million, with over 1.75 million deaths.3
Purpose: This case study of the UNICEF response to COVID-19 in South Africa forms part of a
broader RTA of UNICEF’s COVID-19 response in ESA. The RTA aims to inform a forward-
looking reflection on UNICEF’s response to COVID-19 and thus support timely course correction
for follow-on work.
Audience: The primary users of the RTA findings are the COs in the region as well as UNICEF’s
regional and global offices, which will consider the findings as they plan ahead.
Timeline: The RTA is being undertaken in two phases from October 2020 to July 2021.
1.2 Case study scope, approach, and methods
Scope: The RTA has four overarching questions: (i) how has UNICEF South Africa adapted to
the COVID-19 pandemic and to evolving needs?; (ii) how can the implementation and quality of
the CO’s COVID-19 response be characterised?; (iii) what are the emerging themes?; and (iv)
what are the early lessons?
Approach: The approach is qualitative, which is pertinent given the broad and contextual nature
of the questions and the goal of obtaining illustrative and explanatory responses.4
Methods: Data collection involved remote KIIs conducted in December 2020 with 16 purposively
selected respondents: UNICEF CO management (four respondents), UNICEF partners (eight),
and frontline workers (four). Annex A.3 provides a breakdown of the respondents. The primary
qualitative data was supplemented with a review of secondary documents (where these were
available) provided by the ESARO evaluation team; and a survey of wider UNICEF Country
Office staff.
Limitations: The assessment was designed as a ‘light touch’ real-time analysis, with a tight
timeline and relatively small budget. Due to this, only a small sample of stakeholders were
interviewed, 5 and it was not possible to include beneficiaries. The broad sectoral focus also
precluded in-depth analysis. As the research was conducted at the end of the year, some key
informants were unavailable (due to the Christmas period).
2 OPM (2020) ‘Inception Report for the Real-Time Assessment (RTA) of UNICEF’s Ongoing Response to COVID-19 in
Eastern and Southern Africa’, OPM, Oxford.
3 WHO Coronavirus Disease (COVID-19) Dashboard, available at https://covid19.who.int/ (last accessed 28 December
2020).
4 The primary qualitative data is supplemented to a limited extent by document review.
5 As agreed with UNICEF during the inception phase, the deep dive assessments involved key informant interviews
with 10-14 stakeholders in each of the deep dive countries. A purposive sampling approach was used to identify key
informants across key sectors involved in COVID-19 response. This sample was drawn from a list of potential key
informants provided by the UNICEF CO focal point, with a focus towards covering respondents from a diverse range of
organization types (UNICEF CO, NGOs, government, and UN agencies) and prioritizing sectors/areas which have
been key focus of COVID-19 response. Due to time and resource constraints, the assessment did not cover all sectors
or programme areas that were part of COVID-19 response.
1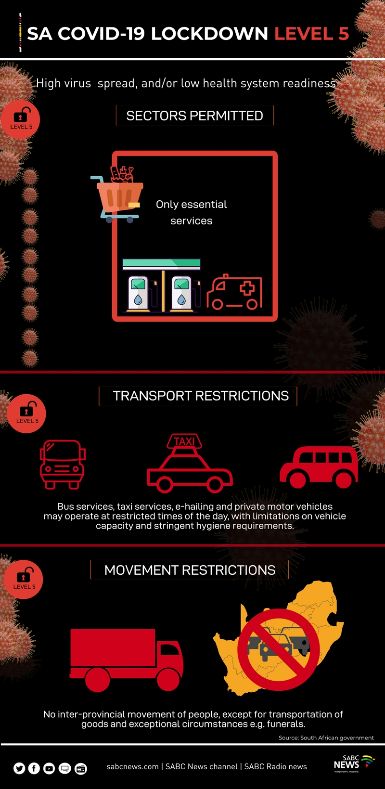
RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
1.3 Regional context in relation to the COVID-19 epidemic
Regional context: South Africa is one of the 21 countries with UNICEF offices overseen by
UNICEF ESARO (see Figure 1 in Annex A). South Africa’s relatively high level of socioeconomic
development and institutional strength is an exception in a region that includes countries that are
otherwise among the most vulnerable in the world. However, the delay in the pandemic’s onset in
the region (the first COVID-19 case in the region appeared in South Africa on 5 March 20206)
and proactive containment measures, appear to have enhanced the region’s ability to contain the
disease.7
1.4 Summary of the impact of COVID-19 in South Africa
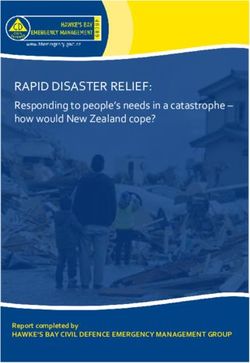
In South Africa, 1,004,413 COVID-19 cases and 26,735 deaths have been recorded as at 27
December 2020.8 The chart below illustrates the trend of new cases over time.
Figure 1: Trend of new COVID-19 cases in South Africa, as at 16 December 2020
(Source: Statista at https://www.statista.com/statistics/1107993/coronavirus-cases-in-south-africa/)
South Africa’s public health and social measures to limit the spread of COVID-19 have included
‘instituting response coordination mechanisms at all levels, setting up control interventions for all
critical pillars of response and imposing public health and social measures, including movement
restrictions, curfews, closure of businesses, schools and places of worship’. These efforts have
been commended by WHO9 and credited for delaying the peak of the pandemic.10
SACO is a partner in the government’s COVID-19 response, not only participating in the
related structures but also adapting its operations and programming. On the basis of the 16
KIIs, this report outlines how this is being done and presents emerging themes as well as the
lessons that can be drawn from SACO’s response to the COVID-19 pandemic.
6 Wikipedia (2020) ‘COVID-19 pandemic in Africa’, available at https://en.wikipedia.org/wiki/COVID-
19_pandemic_in_Africa (last accessed 27 December 2020).
7 Though it should be noted that those measures had unintended consequences in other respects.
8 Government of South Africa's COVID-19 Online Resource and News Portal, update of 27 December 2020, available
at https://sacoronavirus.co.za/2020/12/27/update-on-covid-19-27th-december-2020/ (last accessed 28 December
2020).
9 World Health Organization (2020) ‘WHO encouraged by South Africa’s declining COVID-19 trend (17 September
2020)’, available at www.afro.who.int/news/who-encouraged-south-africas-declining-covid-19-trend (last accessed 28
December 2020).
10 Salim S. Abdool Karim (2020) ‘The South African Response to the Pandemic’ (COVID-19 Notes Series, New
England Journal of Medicine, 29 May 2020), available at www.nejm.org/doi/full/10.1056/NEJMc2014960 (last
accessed 28 December 2020).
2
RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
2 Findings
Prior to COVID-19: UNICEF SACO’s programmatic focus areas in 201911 included:
• Health and nutrition, in which three key focus areas were prioritised: (i) strengthening health
systems for evidence-based planning and the monitoring of a comprehensive package of
health; (ii) strengthening paediatric HIV and the continuation of HIV/AIDS prevention,
specifically in the Prevention of Mother-to-Child Transmission (PMTCT) among young girls
and women; and (iii) improved maternal and child health services including nutrition services
for mothers and children;
• Education, geared toward strengthening the system for the delivery of holistic,
comprehensive, and equitable early childhood development and basic education in line with
the country’s National Development Plan and other sector policy blueprints; and
• Child protection and social policy, where UNICEF SACO advocated for increased
resources and a strengthened government response to ensure the safety of children and
women.
These programmatic areas were supported by related communications and partnerships.
Emergence of COVID-19: South Africa confirmed the ESA region’s
first COVID-19 case on 5 March 2020, with the president declaring a
state of disaster 10 days later, on 15 March 2020.12 From that point
onwards, a series of public health and social measures were put in
place to control the spread of the pandemic. The strictest level of
restrictions were imposed during an Alert Level 5 lockdown (see
graphic to the right) for 35 days, starting at midnight on 26 March
2020.13
A necessary shift: UNICEF SACO was forced to adapt, not only to
COVID-19 itself but also to related containment measures. This
raises certain questions:
• How did UNICEF SACO adapt its programming and
operations in the context of COVID-19 and related
containment measures?
• What did this mean for implementation?
• What were the implications of this adaptation in regard to
programme quality? © SABC News
11 This section draws directly from UNICEF South Africa’s Annual Report for 2019, available at
www.unicef.org/southafrica/media/4411/file/ZAF-Annual-report-2019.pdf (last accessed on 28 December 2020).
12 Government of South Africa's COVID-19 Online Resource and News Portal, ‘Academic Articles: Contextualizing
Lockdown (20 July 2020)’, available at https://sacoronavirus.co.za/2020/07/20/contextualizing-lockdown/ (last
accessed on 28 December 2020).
13 COVID-19 Content Centre, Lockdown Level 5, available at https://supportbusiness.co.za/lockdown/lockdown-level-5/
(last accessed on 28 December 2020); and SABC News, INFOGRAPHIC | South Africa’s lockdown level 5,4,3,2 and 1,
available at www.sabcnews.com/sabcnews/infographic-south-africas-lockdown-level-5432-and-1/ (last accessed on 28
December 2020).
3RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
ADAPTATION
2.1 How UNICEF SACO has adapted
UNICEF SACO adapted operationally and programmatically to support both the emergency
response, and mitigation of the unintended consequences of the public health and social
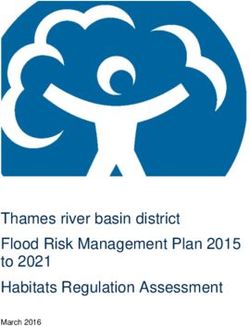
measures put in place to contain the disease. This was in line with UNICEF’s framework for the
COVID-19 response (see Figure 2).
Figure 2: Framework for UNICEF’s COVID-19 response
(Source: UNICEF ESARO)
Because UNICEF SACO staff were already partially working remotely, and thanks to South
Africa’s strong communications infrastructure, the CO’s most critical operational adaptations
were not related to undertaking an in-house shift to remote working modalities. Instead, they
related to scaling up support to new and existing partners, accelerating operations, increasing
fundraising efforts, and bringing WASH and C4D capacity on board. The operational adaptations
were often mentioned together with programmatic adaptations, including:
• Establishing a brand-new WASH programme.
• Reactivating the CO’s C4D component, to inform communities about COVID-19 and to
encourage the continued use of basic essential services. This was done via platforms and
means such as community radio and a mobile truck that would reach the most vulnerable,
including women and children.
• Adopting new methods to assess community needs. For example, by deploying a
team of young people to conduct needs assessments (thus simultaneously creating
employment and building skills) and by building on existing vulnerability mapping to
establish educational needs.
• Adjusting programme content and shifting to remote and digital modalities of
programme delivery. For example, shifting face-to-face sessions in an adolescent peer
mentor programme to using WhatsApp as a platform. This enabled continued exchange
and reorientation of nutrition messaging (in partnership with the National Department of
Health) to speak to nutrition in the context of COVID-19;
• Strengthening and accelerating social protection/social development efforts. This
included successful advocacy for an increase in the grant amount for children in poverty
(Figure 3) and supporting food provision efforts; and
4RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
Figure 3: Media coverage on the social grant increases
South
African
news
headlines
on the
increase
of social
grant
amounts
(Sources: The South African and The Conversation)
• Strengthening community engagement and enhancing partnerships with
government and other institutions (such as community-based organisations and
private enterprises). This could also be seen as an operational adaptation but had such a
significant programmatic impact that it is included here as well. For example, there was
increased frequency of meetings with partners; a public–private partnership was forged
that established WASH facilities in communities in need; and a new partnership was
forged with World Vision South Africa, which expanded SACO’s social development
efforts. SACO also activated a new partnership with the South African Red Cross Society
for risk communication and community engagement (RCCE) work.
IMPLEMENTATION
2.2 Effectiveness of UNICEF’s response to COVID-19 in South Africa
The effectiveness of UNICEF South Africa’s COVID-19 response is presented along four
dimensions: offsetting the negative effects of the pandemic on access to basic services; reaching
the most vulnerable and ensuring equity; meeting programming standards and protocols; and
ensuring community engagement.
2.2.1 Extent to which UNICEF has been able to contribute to offsetting the
negative effects of the pandemic on access to basic services (ensuring
coverage and scale-up)
Respondents struggled to provide an overall rating regarding the extent to which access to basic
essential services have been maintained. South Africa’s strict Alert Level 5 lockdown (35 days
from 26 March 2020),13 and initial messaging focused on urging social distancing, inadvertently
served to strongly discourage people from seeking basic services.
The SACO team and its partners saw evidence of ‘The beauty of this…has been the
steeply falling rates of access to some services, willingness from UNICEF to tap into
such as immunisation, sexual and reproductive unchartered waters… willingness to
healthcare services, antiretroviral medications, and stretch and do something different’
general and specialised medical care. Respondents
also spoke of empty hospital wards and of entire
healthcare facilities being shut down due to fear of COVID-19. This raised the alarm and
triggered a shift in messaging to highlight the importance of attending to basic essential needs,
alongside other interventions (such as catch-up campaigns for the abovementioned services).
This expanded beyond health and nutrition to encompass continuation of learning, child and
social development and protection, in what one respondent lauded as a ‘multifaceted’ approach.
It is worth mentioning that the messaging itself appears to have been multifaceted. It made use
of religious leaders, community activists, ‘hidden heroes’ (everyday community members who
modelled appropriate behaviour), talk shows, webinars, and locations such as taxi ranks (which
were not typically used for such messaging). Furthermore, the ‘look and feel’ of the messaging
5RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
went beyond the traditional. It also took gender equality into account by, for example, promoting
child medical appointments as a family responsibility (not a solely female role).
2.2.2 Extent to which UNICEF has been successful in reaching the most
vulnerable segments of the population and ensuring equity
UNICEF SACO’s partners and frontline workers’ ratings of the extent to which UNICEF support
helped them reach the most vulnerable and excluded varied widely. It varied according to
the sub-period taken into consideration (for example, different levels of lockdown) and the
respondent’s programmatic and geographic area of work. This may in itself reflect the vastness
and diversity of the South African context. Respondents also highlighted that has been a broad-
based effort; and found it difficult to give credit to a single agency.
Nonetheless, the KIIs revealed that UNICEF SACO undertook several important endeavours
aimed at reaching the most vulnerable segments of the population and ensuring equity. The
first step involved identifying who and where the vulnerable populations were and assessing their
needs. Then, to meet the identified needs (i.e. to be in a position to reach those populations), all
the adaptations listed in Section 2.1 came into play. As an example, the CO made appeals to
donors, including private sector funders, for support to enable the delivery of ‘buckets of care’ to
vulnerable families (Figure 4).
Figure 4: An appeal for support to reach vulnerable families
This graphic was
shared on social
media platforms and
sent to cooperating
partners as well as
pledge donors.
In addition, UNICEF
staff members
attached the design to
their email signatures.
(Source: UNICEF South Africa)
UNICEF SACO, along with others, also successfully advocated for an increase in social grants
benefiting children. This significant development contributed to ensuring that the most vulnerable
were reached.
Buckets of care’ hampers
Going beyond fundraising and advocacy, the CO also
established a strong presence on the ground in
certain zones. It deliberately extended its geographic
footprint and collaborated with community-based
organisations, which worked closely with target
communities to ensure that the interventions reached
the target beneficiaries. For example, related to the
appeal noted in the preceding graphic, UNICEF SACO
ensured that the ‘buckets of care’ were delivered to
families in need.
(Photo credit: © UNICEF/2020/Simons Meyer)
6RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
Additional examples of efforts to ensure reach to the vulnerable and excluded are home delivery
of supplies in cases where vulnerable families cannot reach central distribution points;
programming in local languages; and a UNICEF-supported mobile truck that is being deployed
to COVID-19 hotspots in rural areas to communicate health messages and engage communities.
Evidence-based prioritisation of geographic areas is helping target catch-up drives such as
those for child immunisations.
Despite the CO’s efforts, however, gaps have not been fully overcome. Respondents indicated
that refugee and migrant populations (‘the undocumented’) and those living in very rural areas
may be unreached. In addition, although attention is generally being paid to ensuring gender
equality, some respondents felt that more attention needs to be paid to men (a population
particularly poorly equipped to deal with the pandemic). One respondent said that when men are
vulnerable then women and children become vulnerable too, whether economically or as victims
of violence due to misdirected anger and frustration.
More broadly, CO key informants acknowledged that there were more needs than resources
allowed to address.
2.2.3 How UNICEF has been able to meet programming standards and protocols
Interestingly, SACO respondents’ perception that some needs are being unattended influenced
their ratings of the CO’s ability to meet programming standards and protocols. These ratings
ranged from 2 to 4 (on a scale of 1 to 5, where 5 is high). However, when focusing on individual
components of programming and protocols (e.g. maintaining rigour in reporting, ensuring that
partners were trained on the Prevention of Sexual Exploitation and Abuse by humanitarian
personnel, and conducting required oversight and verification) respondents expressed firm
confidence that they have been able to meet programming standards and protocols in the
COVID-19 context.
The CO’s assessment appears to be confirmed by implementing partners and frontline workers
especially. They indicated that continuous feedback, reporting, supervision, and other monitoring
and tracking activities were ways in which UNICEF SACO ensured that programming was taking
place as intended and was of good quality.
The SACO respondents indicated that guidance from UNICEF global and from UNICEF
ESARO was effective in informing COVID-19-era programming, not only for the CO but also for
its partners.
2.2.4 UNICEF’s ability to ensure and sustain community engagement/ AAP
mechanisms
Feedback from UNICEF SACO’s partners and frontline
workers revealed the strong sentiment that the CO’s ‘We wanted ownership
collaboration and support was a significant influence on their and accountability’
way of working with communities. This related specifically to
orienting them toward listening to communities rather than telling communities what they
should do. Indeed, in line with the quote to the right, this was intentional on SACO’s part, and it
appears to have had a major positive impact.
Going beyond engaging communities to understand their needs and concerns, one partner also
saw the freedom of choice given to beneficiaries (who received nutrition support through
UNICEF-supported food vouchers, versus food parcels) as further evidence of empowering
communities.
Thus, though the term ‘AAP’ was little cited in the KIIs, it appears that the spirit of AAP was
brought to life in the overall framework of SACO’s approach.
7RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
2.3 How UNICEF SACO has utilised preparedness and contingency
planning during the COVID-19 response, and how has it revised
COVID-19 response plans based on the evolving needs of the
population
Respondents were nearly unanimous in the view that
‘We were just so gob-smacked’
South Africa was ill prepared for COVID-19, both as a
country and at the various institutional levels. Unlike
other countries in the region that are experienced in public health crises and extreme natural
disasters, South Africa has been relatively untouched by widescale emergencies, with the
exception of HIV/Aids. However, one respondent nuanced this view by noting that the country
was prepared in terms of quality (e.g. the country was on high alert for Ebola), but not in terms of
quantity (i.e. for the sheer number of cases that COVID-19 caused). Another respondent
perceived that the country’s management of the pandemic was supported by the early
identification of South Africa as a potential COVID-19 hotspot, and strict containment measures.
At the UNICEF CO level, information in the previous cycle of SACO’s EPP had not been finalised
and the CO’s emergency action plan was oriented toward events such as droughts and
xenophobic violence. This suggests that the CO did not think it would be facing a crisis of
COVID-19’s nature and magnitude.
However, the data from the KIIs indicate that the CO responded well in terms of keeping up with
the evolving needs of the population in light of COVID-19. Close and continuous community
engagement, along with close and continuous scrutiny and interpretation of data, have ensured
knowledge of the realities on the ground. The KIIs further suggested that response plans are
being (or will be) adapted accordingly.
2.4 What is known about needs in South Africa and how UNICEF
has determined and verified those needs?
South Africa’s vast size and diversity present challenges for fully determining, understanding and
verifying its needs. However, according to one respondent, the country’s ‘strong social welfare
system’, based on measures of vulnerability, have been important in providing a ready-made
mapping of needs.
Furthermore, classifications of the country’s provinces, and data on urban areas within those
provinces, help to guide targeting. In the education sector, schools are divided into
socioeconomic quintiles and that categorisation, along with statistics on high school pass rates,
further shed light on needs. This is supported by reliable public health data (from various public,
private, and academic institutions) on rates of HIV infection, foetal alcohol syndrome, gender-
based violence (GBV), and other conditions. In terms of WASH, respondents mentioned data
that helped to identify areas where water and sanitation was lacking.
UNICEF SACO appears to have relied on all these sources to determine and understand
population needs. Data were further verified in some cases, most notably for WASH where lists
were compared against the WASH consultant’s findings to ensure that the CO was targeting the
most vulnerable. SACO also collated newspaper reports on GBV to identify hotspots for
intervention.
In addition, UNICEF supported primary data collection, such as U-Report surveys, community
needs assessments, and other studies. One such assessment employed youth as data
collectors, thus addressing youth unemployment and building skills all while generating needed
data. Hotlines, notably Childline (Figure 6), served as another source of information on needs,
particularly child protection needs.
8RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
Figure 5: Encouraging the reporting of child abuse
Graphics such
as this one
were shared
on UNICEF’s
social media
platforms.
(Source: UNICEF South Africa)
Lastly, community engagement and direct observation informed the CO’s identification and
verification of population needs. One respondent explained: ‘UNICEF SACO made more
attempts to be in the field and to work with implementing partners, international NGOs, … to be
side-by-side’.
‘[Gathering and disaggregating data is] not a
The KIIs indicated that, with the exception problem at all. … The proof of the pudding will
of the education sector, the statistics were be… what we do with that data…, how do we
generally perceived to be adequately readjust our programmes, how we adjust
disaggregated. Instead (as the quote to the [whom we talk with], who we work with, to
right suggests), issues arose in regard to address the issues that the data will uncover’
what is done with the data.
Respondents also mentioned the importance of being sensitive to communities’ broader realities
in responding to their needs. For example, messaging about social distancing in urban COVID-
19 hotspots must consider how practical it is for people living in impoverished, overcrowded
conditions to comply with that message.
QUALITY
2.5 What we know about the quality of the UNICEF response to
COVID-19
The quality of the UNICEF response to COVID-19 in South Africa can be analysed through three
lenses: the effects of the crisis and related containment on quality; timeliness of the UNICEF
response; and efforts made by the CO to ensure quality.
2.5.1 The effects of the crisis and related constraints on lockdown and
movement upon UNICEF’s ability to deliver quality
Unlike many other COs in the region and around the world, UNICEF SACO did not feel the
impact of COVID-19 on its procurement of skills and supplies, as such skills and supplies are
available in the domestic market. Due to this, SACO did not have to compete for resources in the
international market. SACO’s interventions were, however, heavily constrained during South
Africa’s Alert Level 5 lockdown, which is among the strictest in the world, according to one
respondent. During this period, very few interventions were able to reach beneficiaries.
However, even after the lifting of the 35-day lockdown, key informants suggested that UNICEF
SACO was absent from national meetings during the early part of the pandemic. Partners noted
that the UNICEF CO ‘came late’, but when it came in it was effective.
9RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
The latter remark referred to UNICEF SACO’s efforts to determine and verify population needs
and adapt programming and service delivery modalities, which helped ensure the relevance
and effectiveness of its actions. However, at least two respondents noted that UNICEF SACO
funding did not reach them even after programme implementation was supposed to be
underway. In one case, the project was completed before the promised UNICEF funds came
through.
2.5.2 Timeliness of UNICEF response to COVID-19
The KIIs suggested that UNICEF SACO’s overall COVID-19
response was not timely. With little exception, partners ‘Better late than never,
noted that UNICEF was late to contribute, and several though’
respondents specifically mention delays in receipt of
UNICEF funding.
On the plus side, the CO seems to be aware of this deficiency. One respondent noted that ‘it took
us a little bit of time to get our act together, but then when we were there, it was appreciated’.
2.5.3 How UNICEF South Africa ensured the quality of the response, and the
processes and verification systems used to ensure quality
Once UNICEF SACO’s COVID-19 interventions were underway, they were perceived to meet
high expectations in terms of quality. Partners and frontline workers spoke of the the CO’s efforts
to ensure quality. One respondent noted that SACO’s rigour helped them improve their data
quality and strengthen reporting, and also helped the partner to reflect on their use of resources,
and thus helped them to develop valuable skills.
10RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
3 Emerging themes/ conclusions
3.1 Emerging positives from UNICEF South Africa’s performance in
the COVID-19 response
The following key positive conclusions can be drawn from UNICEF South Africa’s performance in
the COVID-19 response:
POSITIVES IN ADAPTATION
• The CO was able to adopt new methods to assess and meet community needs.
• The CO succeeded in establishing a brand-new WASH programme to respond to the needs
presented by COVID-19.
Figure 6: WASH facilities installed at schools and in communities
(Photo credits: © UNICEF/2020/Smulders for photo on the left; © UNICEF/UNI324165/Spatari/AFP-Services for photo on the right)
• The CO also recognised the importance of re-establishing its C4D capacity, and of bold but
measured external communication work that integrates advocacy, fundraising and RCCE for
maximum impact.
• UNICEF SACO expanded its geographic footprint to meet expanded needs.
• UNICEF SACO was successful in establishing new partnerships, including forging strategic
public–private partnerships that were lauded by partners.
• The CO strengthened and accelerated social protection/social development efforts.
• Internally, regular programme coordination meetings and related tools, with ‘deep dives’ on
specific topics, enabled SACO to track progress and plan ahead for necessary adaptations.
POSITIVES IN IMPLEMENTATION
• UNICEF SACO contributed significantly to offsetting the negative effects of the pandemic on
access to basic services across all programme areas.
11RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
• Successful coordination and programme delivery in the education sector was highlighted by
respondents, though lack of participation from government partners in education means that
the KIIs did not provide an entirely holistic perspective.
Figure 7: A class in session in South Africa in the era of COVID-19
(Photo credit: © UNICEF/2020/Schermbrucker)
• UNICEF SACO’s partners expressed ‘UNICEF didn’t come [in] from a place
appreciation for the level of trust that the CO of superiority, they came from a place
placed in them to do what they do best. of learning…and I must say we
learned a lot from them, too’
• The CO has been successful in reaching some
pockets of the most vulnerable segments of
the population, ensuring gender equity and ownership in the process.
• Even in the COVID-19 context, UNICEF South Africa met programming standards and
protocols.
• SACO firmly upheld the spirit of community engagement/AAP, an approach that was lauded
repeatedly by various respondents.
‘For people in areas where they are reliant on social grants… that tells them that their
lives matter. What UNICEF has done has really changed people's lives’
POSITIVES IN QUALITY ASSURANCE
Despite the challenges posed by COVID-19, UNICEF SACO adhered to processes and
verification systems used to ensure quality.
3.2 Challenges encountered in UNICEF South Africa’s
implementation of the COVID-19 response
The challenges encountered in SACO’s response to COVID-19 can be summarised along the
same three dimensions (adaptation, implementation, and quality) as follows:
12RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
CHALLENGES IN ADAPTATION
• There was a lack of adequate resources to meet the need.
CHALLENGES IN IMPLEMENTATION
• The point above translated into a situation where some sub-groups of women and
children in need were not reached and went without support. Examples of sub-groups
that were not reached include those on the far side of the digital divide, those in need of
learning materials in indigenous languages, the undocumented, and the urban poor living
in informal settlements.
• Inadequate levels of communication (on SACO’s part) with partners seemed to have led
to some concerns; for example, government not being fully aware of UNICEF activities
and at least one partner wondering whether their UNICEF focal point was facing internal
pressures.
• UNICEF SACO had insufficient pre-existing preparedness and contingency planning in
place to support the response; thus, it was caught off-guard, with inadequate structures in
place to respond effectively and in a timely fashion.
CHALLENGES IN ASSURING QUALITY
• Following on from the preceding point, UNICEF SACO was late in participating in the
national effort and was unable to consistently ensure programme delivery on a timely
basis, despite seemingly making use of simplified standard operating procedures
(SSOPs).
3.3 Medium- to long-term implications for vulnerable children and
their communities in South Africa, and implications for
UNICEF’s strategy and action in the medium to long term
Respondents participating in the South Africa case study were nearly unanimous in their
impression that the COVID-19 pandemic had only served to highlight the plight of those
who had been vulnerable prior to the outbreak. Most notably these are the poor, unemployed
youth, those living in informal urban settlements as well as those in remote areas; those
participating in the informal economy, those suffering from mental health issues, those with
physical disabilities, and learners leaving school with inadequate achievement levels. Those in
the middle class were also perceived as somewhat worse off due to COVID-19. Put differently:
‘COVID-19 just showed where the gaps are that we knew before’ and ‘existing vulnerabilities
became amplified’.
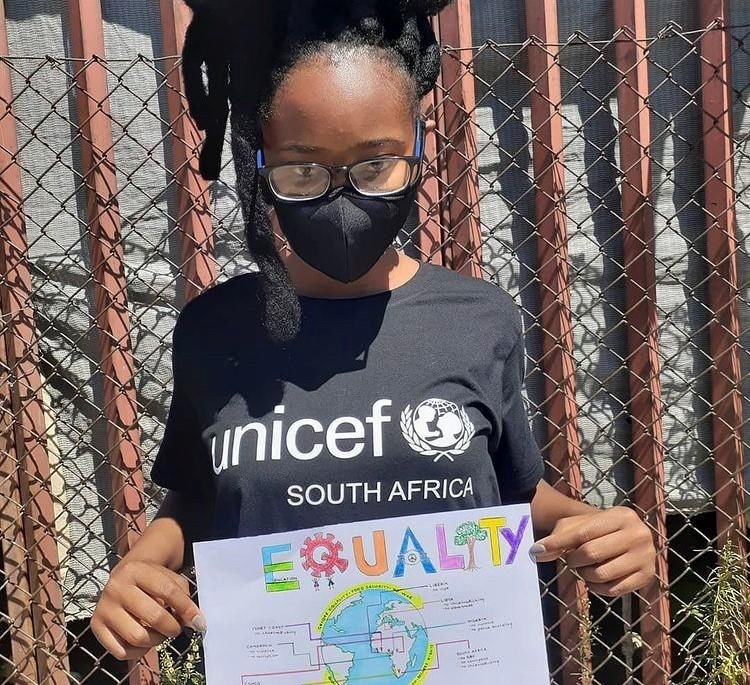
Interestingly, the plight of men was mentioned several times in the course of the KIIs. , One
respondent noted that men are least equipped to deal with the impact of COVID-19, which puts
women and children at risk of GBV. Another respondent remarked that the phrasing of the KII
question (on the most vulnerable sub-groups of women and children) further entrenches gender
inequalities. Respondents felt that programming that speaks to men and boy children is
needed.
13RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
Figure 8: An adolescent holds a handmade poster calling for equality
(Photo credit: © UNICEF/complete credit not provided)
3.4 (Re)focusing UNICEF’s programming to reach vulnerable
children in the medium to long term
Based on their perspective of emerging challenges and considering the broader objective of the
RTA, respondents participating in this case study offered the following suggestions to inform
SACO’s programming in the medium to long term:
• Support for catch-up campaigns for children will be necessary, ‘All the warning
particularly in the health (including nutrition) and education sectors. signs are there
that children
• Support economic development – ‘because if parents aren’t are at risk’
working then children aren’t eating’ – and efforts to address youth
unemployment.
• Support learners at all educational levels, including ensuring that those with disabilities are
targeted.
• Continue to encourage behaviour change to reduce COVID-19 transmission rates – there is
‘a lot of work to be done there’.
• Integrate COVID-19 considerations into ongoing health programming (by, for example,
establishing guidelines for dispensing medication for chronic conditions to cover longer
periods and thus limiting the need to visit health facilities).
• Integrate health messaging, specifically nutrition messages, into settings that go beyond the
health silo, such as in transportation hubs.
14RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
15RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
4 Lessons learned/Suggested action points
The major lessons and suggestions for SACO moving forward are presented in Section 3
(above). In this section, we highlight action points that are particularly important or that have not
yet been articulated, which may be useful for consideration in UNICEF’s programming (in South
Africa and beyond).
OPERATIONS
1. UNICEF SACO should preposition itself and its partners for emergency situations. As
suggested by one respondent, the EPP should be simulated at regular intervals and the CO
should ensure that preparedness is in place.
2. UNICEF should consider revisiting its decision-making hierarchy and other internal processes
to ensure timely delivery of appropriate programming.
3. Consolidate and maintain partnerships, particularly innovative public–private partnerships
and institutional frameworks for coordination and continued engagement.
4. Deepen communication with partners to ensure transparency and for the sake of coordination
and the building of trust.
PROGRAMMING
5. Re-establish WASH and C4D as a permanent part of the SACO programme and strengthen
and accelerate related interventions, particularly messaging on prevention.
6. Maintain and advance innovative edutainment (education in entertainment form) approaches
in messaging.
7. Cement multi-dimensional/-sectoral/-faceted, empowerment-based approaches across
programming, especially in the area of social development. Partners and frontline workers
believe that this type of holistic community engagement ‘creates not just hope but a
sustainable future’.
8. Produce learning materials in indigenous languages to facilitate continued learning for all.
16RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
Annex A Regional context
A.1 Countries in eastern and southern Africa with UNICEF COs
The map below shows the countries with UNICEF COs that fall under the purview of UNICEF
ESARO.
Figure 1 Countries in ESAR with UNICEF offices
17RTA of UNICEF’s Ongoing Response to COVID-19: South Africa
A.2 UNICEF response to COVID-19 in ESAR
Excerpted from OPM’s Inception Report14
Soon after the pandemic was declared by the World Health Organization (WHO) the UNICEF
country offices and regional office in ESAR began working with the governments and the
development partners in the region to respond to the pandemic with the aim to reduce
transmission and mitigate the impacts of COVID-19. The region received nearly US$350 million,
which is approximately 18% of UNICEF’s global Humanitarian Action for Children (HAC) to
respond to COVID-19.
UNICEF is responding to COVID-19 in the Eastern and Southern Africa Region (ESAR) mainly
through two distinct but complementary pathways, namely, programmatic response and
operational response. [As part of the programmatic response], UNICEF is…working to ensure
the continuity of ongoing basic essential services15 in the region. Further details on these
responses based on the information included in the ToRs of the RTA is outlined below.
Programmatic response
The programmatic response to COVID-19 in ESAR is aimed to minimise the impact of the
pandemic on women and children by ensuring the continuity of basic essential services and
adapting the services to incorporate safety measures and COVID-19 transmission prevention
activities, more specifically:
• Ensuring access to essential health and nutrition services, including sexual, reproductive,
maternal, newborn, child and adolescent health (SRMNCAH) and HIV;
• Supporting government to provide distance and home learning through eLearning
platforms and take-home packages, and promoting and supporting the early and safe re-
opening of schools;
• Ensuring availability of water and other lifesaving commodities;
• Identifying and protecting children and adolescents in the most vulnerable households
and circumstances, such as children with disabilities, children deprived of their liberty,
refugee, internally displaced, migrant and returnee children, and girls who face increased
risk to e.g. child marriage as a result of the pandemic;
• Providing support to caregivers on how to talk to children about COVID-19, managing
their children’s mental health and well-being and; supporting the continuity of learning
whilst schools and centres are closed;
• Adapting and refining standard COVID-19 response measures to support children and
families living in challenging settings such as refugee camps, informal settlements, rural
areas and densely populated urban and peri-urban areas;
• Expanding sustainable social protection programmes (including cash top ups to existing
beneficiaries and identifying new beneficiaries including the borderline poor), including
gender-sensitive measures such as cash transfers to support girls’ re-entry to school;
• Helping finance ministries access international funding opportunities to invest in health,
WASH, social protection systems and social welfare services;
14 OPM, Inception Report for the Real-Time Assessment (RTA) of UNICEF’s Ongoing Response to COVID-19 in
Eastern and Southern Africa, 10 November 2020.
15 Basic essential services comprise health services (including sexual, reproductive, maternal, newborn, child and
adolescent health); nutrition; social welfare, child protection and gender-based violence; access to and retention and
performance in education and learning; WASH, including in schools (including menstrual hygiene management),
health facilities, households and communities; social protection; HIV.
18You can also read